
Abstract
Objective
Little is known about the impact of cerebral microbleeds on cognitive function. This study investigated the distribution of cerebral microbleeds and their impact on cognitive function, in patients with lacunar infarct.
Methods
Patients with lacunar infarct were enrolled prospectively. Cerebral microbleeds were classified as absent, mild, moderate or severe, based on magnetic resonance imaging findings. Cognitive function was measured using the Montreal Cognitive Assessment (MoCA) questionnaire, with a total score of <26 indicating cognitive impairment.
Results
Of the 85 patients included in the study, 35 (41.2%) had cerebral microbleeds. They were more frequently observed in mixed and deep brain regions, but rarely in the cerebral lobes. Multiple logistic regression analysis demonstrated that presence of cerebral microbleeds (odds ratio [OR] 5.320), duration of education (OR 0.938) and age (OR 1.464) were independent predictors of cognitive impairment. There was a significant correlation between cerebral microbleed severity and MoCA score.
Conclusion
The number and location of cerebral microbleeds were both closely associated with cognitive impairment, in patients with lacunar infarct.
Introduction
Interest in cerebral microbleeds has increased with the widespread clinical use of magnetic resonance imaging (MRI). Cerebral microbleeds appear as small, round hypointense lesions on gradient-echo (GE) T2*-weighted MRI sequences and are characterized histologically by the presence of haemosiderin deposits around small blood vessels with a diameter <200 µm. 1 In general, histopathological analysis of cerebral microbleeds reveals two types of vascular pathological change: hypertensive vasculopathy and cerebral amyloid angiopathy.1–3 Cerebral microbleeds are often detected in patients with ischaemic stroke, Alzheimer’s disease or cerebral amyloid angiopathy, but are also found in healthy elderly individuals, although the prevalence and distribution differs among these groups. 1 Research has also indicated that cerebral microbleeds are associated with an increased risk of stroke recurrence and haemorrhagic transformation after ischaemic stroke.4,5
A relationship between cerebral microbleeds and cognition has been demonstrated in some patients with ischaemic stroke, 6 vascular cognitive impairment 7 or Alzheimer's disease, 8 but the impact of such bleeds on cognitive function in other patient populations has not been extensively described. Cerebral microbleeds may be associated with endothelial dysfunction and blood–brain barrier damage, which play significant roles in lacunar infarct, and may be damaging to neurons and nerve fibre function.1,9,10
Few studies have examined the relationship between cerebral microbleeds and cognitive function in patients with lacunar infarct. Using MRI, the present study prospectively investigated the regional distribution of cerebral microbleeds in the brains of Chinese patients with lacunar infarct, and examined the relationship between such bleeds and cognitive function, using the Montreal Cognitive Assessment (MoCA) questionnaire in these individuals.
Patients and methods
Study Population
Patients with ischaemic stroke associated with lacunar infarct, presenting at the Department of Neurology, Jinling Hospital, Nanjing University School of Medicine, Nanjing, Jiangsu, China, between July 2010 and September 2011, were recruited to this study. All patients were registered in the Nanjing Stroke Registry Programme. Lacunar infarct was defined as a clinical lacunar syndrome with a compatible lesion on MRI and computed tomography (CT) scans. All patients had routine investigations for stroke, including head MRI and CT scanning, electrocardiogram, cardiac ultrasonic contrast and Duplex ultrasound. Patients were eligible for study inclusion if they were of Chinese ethnicity, were aged ≥18 years, and if they had well-documented (clinical presentation and CT or MRI scan of the brain) first-ever acute ischaemic stroke within the previous 7 days. Exclusion criteria were: (i) carotid or vertebral artery stenosis of >50%, regardless of subcortical infarction or cortical infarction of any size; (ii) potential cardiac sources of embolism defined as high or moderate risk, based on the Trial of Org 10172 in Acute Stroke Treatment classification; 11 (iii) subcortical infarction >15 mm in diameter or cortical infarction; (iv) inability to undergo cerebral MRI; (v) history of neurological disorder or brain injury.
The study protocol was approved by the Institutional Review Board of Jinling Hospital and written informed consent was provided by patients or their legally authorized representatives.
Clinical Assessment
Demographic data and clinical histories of participating patients were collected from the Nanjing Stroke Registry Programme. Hypertension was defined as the combination of a self-reported high blood pressure and use of antihypertensive medications, or blood pressure ≥140/90 mmHg on three occasions. The presence of diabetes mellitus was defined as a fasting blood glucose level of ≥125 mg/dl or use of antidiabetic medication. Coronary artery disease was defined as a history of myocardial infarction, coronary artery bypass grafting, coronary angioplasty, stenting or angina pectoris. Hyperlipidaemia was defined as elevated fasting total cholesterol concentrations or use of statins prior to stroke.
MRI
Magnetic resonance imaging was performed with patients in the supine position using a 3.0 T system (MAGNETOM® Trio; Siemens, Erlangen, Germany) with a 12-channel head coil. Susceptibility-weighted images (SWI) were acquired with a long time-to-echo (TE), fully flow-compensated three-dimensional GE sequence with the following parameters: repetition time/TE, 28/20 ms; flip angle, 15°; rectangular field of view, 7/8; matrix size, 448 × 168; slice thickness, 2 mm; integrated parallel imaging technique factor, 2; acquisition time, 5 min. Images were obtained in the axial plane parallel to the bicommissural line. SWI sequences were reconstructed with the minimum intensity projection (minIP) algorithm and multiplanar reformation techniques to obtain images of 3–10 mm thickness, with positions comparable to those of routine sequences. The minIP algorithm enabled enhanced detection of images of veins while minimizing the signal from cerebral tissues.
Cerebral microbleeds were defined as homogeneous rounded areas of signal loss with a diameter <10 mm on SWI sequences. Hypointense lesions within the subarachnoid space, or those probably associated with calcification of the globus pallidum, traumatic brain injury or vascular degeneration, were excluded. Cerebral microbleeds were classified as absent, mild (1–2 microbleeds), moderate (3–10 microbleeds) or severe (>10 microbleeds), 12 and location was described as lobar (cortex/subcortex) or nonlobar (basal ganglia, thalamus and infratentorial area). 13 Leukoaraiosis on CT and MRI in all stroke patients was graded using the Fazekas scale, which has been correlated with pathological severity in a postmortem validation study, 14 modified to separate degrees of confluent leukoaraiosis, as previously described: 15 grade 0, no leukoaraiosis; grade 1, mild leukoaraiosis (>5 white-matter hyperintensities); grade 2, moderate confluent leukoaraiosis; grade 3, severe confluent leukoaraiosis.
Magnetic resonance images were evaluated by two experienced neurologists, blinded to clinical information.
MoCA questionnaire
A Chinese version of the MoCA questionnaire was used in this study (available at: http://www.mocatest.org). The MoCA questionnaire is a 30-point test covering seven cognitive domains: (i) visuospatial/executive; (ii) naming; (iii) memory; (iv) attention; (v) language; (vi) abstraction; (vii) orientation. Cognitive impairment is indicated by a total MoCA score of <26. A bonus point is given to individuals with <12 years’ education. 16
Statistical Analyses
All statistical analyses were performed using the SPSS® statistical package, version 11.0 (SPSS Inc., Chicago, IL, USA) for Windows®. The interobserver agreement was determined by κ statistics. Baseline characteristics and MRI findings were compared between patients with normal (≥26 points) or subnormal (<26 points) total MoCA scores, using the χ2-test and Mann–Whitney U-test. In addition to age and sex, clinical variables with a P-value of <0.10 in univariate logistic regression analysis were entered into a multiple logistic regression analysis, to determine the independent factors contributing to a low MoCA score. Comparisons of the total MoCA score and subscores between cerebral microbleed-positive and -negative patients were performed using the Student’s t-test. Spearman’s rank correlation coefficient test was used to evaluate the correlation between severity of cerebral microbleeds and MoCA score. A P-value <0.05 was considered statistically significant.
Results
A total of 85 patients (60 [70.6%] males) with lacunar infarcts were included in this study; patients had a mean age ± SD of 68.39 ± 11.37 years and a mean ± SD total MoCA score of 22.91 ± 2.94. Interobserver agreement on the presence of cerebral microbleeds was high (κ = 0.92). Cerebral microbleeds were detected in 35 (41.2%) patients, among whom 30 (85.7%) had multiple microbleeds (≥2 bleeds). In the 35 patients with cerebral microbleeds, these were classified as mild in five (14.3%), moderate in 17 (48.6%) and severe in 13 (37.1%). Microbleeds were observed more frequently in deep or mixed brain regions, and rarely in strictly lobar (cortex/subcortex) locations. The distribution was strictly lobar in four of the 35 patients (11.4%), nonlobar in 18/35 patients (51.4%; 12 patients with microbleeds in the basal ganglia and six patients with microbleeds in the infratentorial brain regions) and in mixed regions in 13/35 (37.1%) patients.
Demographic, clinical and magnetic resonance imaging characteristics of Chinese patients with lacunar infarcts (n = 85), stratified according to normal (≥26) or subnormal (<26) Montreal Cognitive Assessment (MoCA) score.
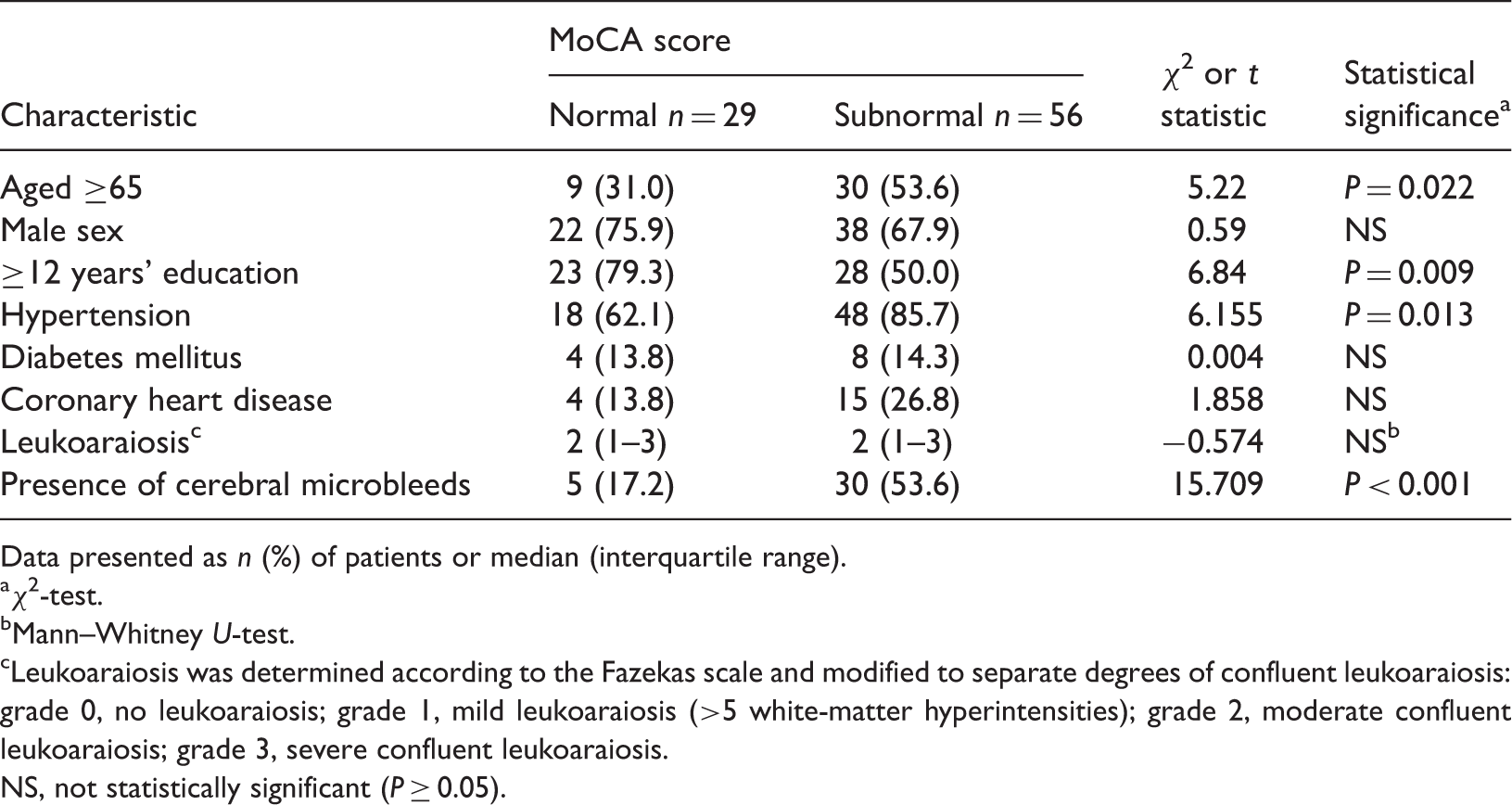
Data presented as n (%) of patients or median (interquartile range).
χ2-test.
Mann–Whitney U-test.
Leukoaraiosis was determined according to the Fazekas scale and modified to separate degrees of confluent leukoaraiosis: grade 0, no leukoaraiosis; grade 1, mild leukoaraiosis (>5 white-matter hyperintensities); grade 2, moderate confluent leukoaraiosis; grade 3, severe confluent leukoaraiosis.
NS, not statistically significant (P ≥ 0.05).
Multiple logistic regression analysis to determine independent factors associated with subnormal Montreal Cognitive Assessment scores (<26 points) in Chinese patients with lacunar infarct (n = 85; subnormal scores were obtained in 56 patients.

OR, odds ratio; CI, confidence interval.
Montreal Cognitive Assessment (MoCA) total score and subscores in Chinese patients with lacunar infarct (n = 85), stratified according to the presence (positive) or absence (negative) of cerebral microbleeds, as determined by magnetic resonance imagin.

Data presented as mean ± SD.
Student’s t-test.
NS, not statistically significant (P ≥ 0.05).
Relationship between location of cerebral microbleeds and Montreal Cognitive Assessment (MoCA) total and subscores in Chinese patients with lacunar infarct (n = 85), stratified according to the presence (positive group) or absence (negative group) of cerebral microbleeds, as determined by magnetic resonance imagin.
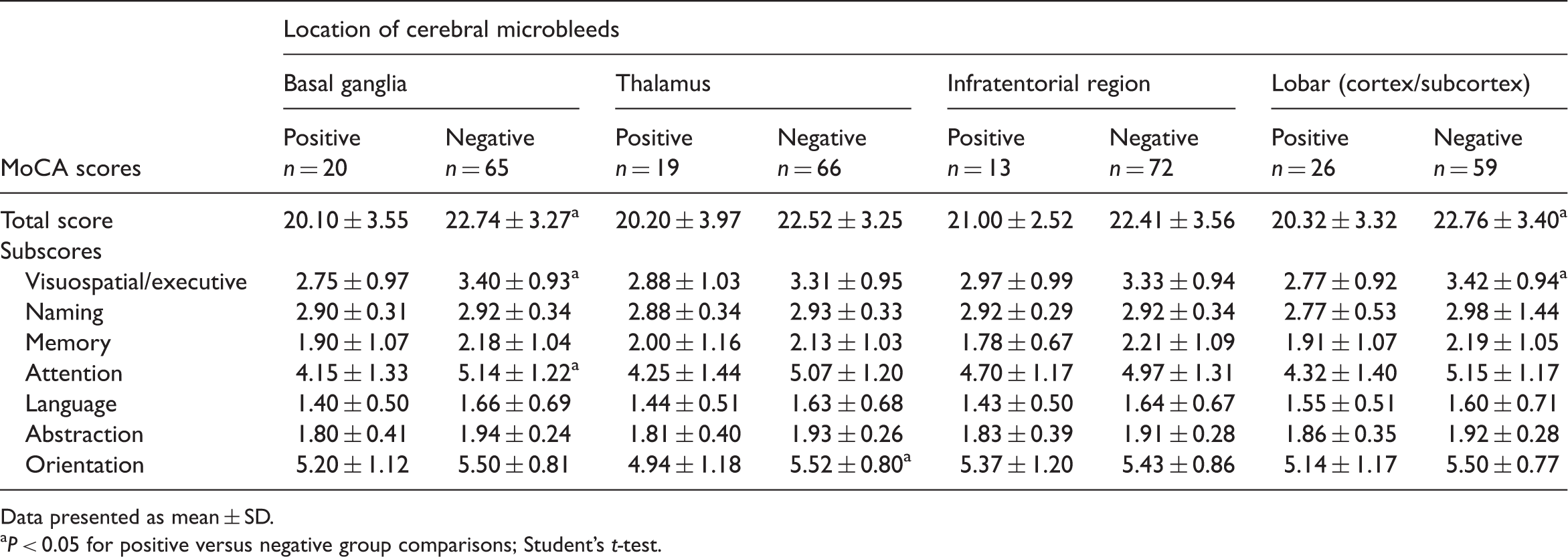
Data presented as mean ± SD.
P < 0.05 for positive versus negative group comparisons; Student’s t-test.
Discussion
In the present study, cerebral microbleeds were frequently observed in patients with lacunar infarcts, with nearly half of all patients having such bleeds (41.2%). The microbleeds appeared mainly in deep or mixed brain regions, but rarely occurred in strictly lobar (cortex/subcortex) locations. In addition, cerebral microbleeds were more often classified as moderate or severe, compared with mild. It has been postulated that the aetiology of microbleeds differs according to their location in the brain, with lobar microbleeds being caused by cerebral amyloid angiopathy, and nonlobar microbleeds (occurring in deep, infratentorial or mixed regions) resulting from arteriosclerosis.1,2 Cerebral microbleeds may be indicative of microangiopathy in the cerebrovascular systems of patients with lacunar infarct. In addition, the presence of microbleeds in deep or mixed lobar locations might also serve as a marker of severe cerebrovascular burden, or suggest the presence of hypertensive damage. 17 Hypertension and ageing have been shown to be important risk factors in the development of small-vessel disease.9,10
In the present study, a significant correlation was determined between cognitive dysfunction and the presence of cerebral microbleeds, in patients with lacunar infarcts. Traditionally, cerebral microbleeds have been considered to be clinically silent, but some studies have demonstrated that they are associated with clinical changes such as cognitive dysfunction,6,18 depression 19 or neurological deterioration, in patients with lacunar infarct. 20 Consistent with data from the present study, other research also suggests that cerebral microbleeds have an important effect on cognitive function, in patients with Alzheimer's disease 21 or ischaemic stroke.22,23 There are two possible explanations for the association of microbleeds with cognitive performance in patients with lacunar infarct. First, microbleeds are associated with the progression of microangiopathies. 1 Cerebral microbleeds in lacunar infarcts may reflect severe blood–brain barrier breakdown, which is important in blood extravasation. Blood breakdown products from microbleeds in the cerebrovascular system (including haemosiderin, iron and ferritin) may cause neuronal damage around the blood vessels and profound neuroinflammation, as demonstrated in a rat model. 24 Secondly, it has been suggested that the presence of cerebral microbleeds may indicate more severe disruption of the neural network between cortical and subcortical structures; 6 cerebral microbleeds could affect, for example, the frontal–subcortical circuits that have important visuospatial or executive functions. The frequent detection of cerebral microbleeds in multiple brain regions (including the cortex, basal ganglia and thalamus) in the present study may be consistent with this hypothesis.
Data from the present study indicate that that the distribution of cerebral microbleeds may be relevant in terms of the dysfunction of various cognitive domains; the presence of microbleeds in particular brain regions had detrimental effects on associated cognitive functions. For example, thalamic microbleeds were associated with a significant reduction in the MoCA orientation subscore, lobar (cortex/subcortex) microbleeds were associated with significantly reduced visuospatial/executive subscores, and basal ganglia microbleeds were associated with significantly reduced attention and visuospatial/executive subscores.
Older age, shorter duration of education and the severity of leukoaraiosis have all been shown to have important impact on cognitive function.25,26 Similarly, the current study demonstrated that age and education were significantly associated with cognitive dysfunction, but no association between the severity of leukoaraiosis and cognitive dysfunction could be determined in univariate logistic regression analysis. This may be because the prevalence of leukoaraiosis was high in patients with lacunar infarcts in the present study, such that there was no significant difference between patients with normal or subnormal MoCA scores.
In conclusion, the present study demonstrated that cerebral microbleeds had significant impact on cognitive dysfunction in Chinese patients with lacunar infarct, and that the severity of such microbleeds was significantly correlated with MoCA scores. Furthermore, the distribution of cerebral microbleeds was associated with the type of cognitive dysfunction experienced by the patient. This small study provides preliminary data to suggest that cerebral microbleeds are important factors in cognitive function, in patients with lacunar infarct. Further prospective studies with larger sample sizes are, however, required to confirm these initial findings.
Footnotes
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Natural Science Foundation of China (NSFC grant no. 81171099 to W.Z.) and the Science and Technology Programme Project in the Bao’an District, Shenzhen, Guangdong, China (grant no. 2010618).