
Abstract
Capsular warning syndrome is a neurologic emergency marked by recurrent, stereotyped lacunar transient ischaemic attacks with a high risk of early infarction. We report a case of a 72-year-old male who presented with three episodes of left-sided weakness within 24 h, consistent with classical capsular warning syndrome, culminating in a right internal capsule infarct. He received timely thrombolysis, followed by dual antiplatelet therapy and atorvastatin. Early transfer to inpatient rehabilitation enabled targeted upper and lower limb recovery using validated protocols, including the Graded Repetitive Arm Supplementary Programme protocol and proprioceptive balance training. The patient achieved near-complete functional independence by discharge. This case highlights the importance of integrating acute stroke management with structured multidisciplinary rehabilitation to optimise outcomes in capsular warning syndrome.
Keywords
Introduction
Capsular warning syndrome (CWS) represents a neurologically urgent form of lacunar transient ischaemic attack (TIA), often preceding a small deep infarct. 1 Classical diagnostic criteria include three or more stereotyped episodes of transient, unilateral motor or sensory symptoms without cortical involvement, occurring within 24–72 h. 2 Although relatively rare, with a prospective population-based study reporting an incidence of only 1.5% among patients with TIA, CWS carries a high risk of early stroke progression, with up to 71.2% of patients subsequently developing an ischaemic infarct.3,4 While the literature primarily focuses on acute management, the role of structured rehabilitation remains underreported.2,5 This case highlights the crucial role of early multidisciplinary rehabilitation in supporting recovery from an internal capsule stroke, likely resulting from probable CWS. This article complies with the Case Reports (CARE) reporting checklist. 6
Case presentation
A 72-year-old male with a medical history of hypertension, asthma, appendicectomy, left hip replacement and transurethral resection of the prostate presented to the emergency department (ED) of a local hospital on the evening of 5 March 2025 following a collapse. His regular medications included olmesartan 20 mg daily and Pavtide (fluticasone/salmeterol) 250/50 μg, one inhalation daily. Before this event, he was functionally independent in all activities of daily living, with a modified Rankin Scale of 0 and a Barthel Index of 100/100.
At approximately 8:00 pm, he experienced sudden light-headedness while walking to the bathroom, followed by an acute onset of left upper and lower limb weakness, resulting in a fall. He denied head trauma or loss of consciousness. On ED arrival at 10:00 pm, his symptoms had resolved, and neurological examination was unremarkable. He was discharged after observation at 3:00 am on 6 March.
At 8:00 am the same day, he experienced a second episode of transient left facial droop and hemiparesis while preparing breakfast. The symptoms resolved within 20 min. Planning to see his general practitioner, he later experienced a third episode at 12:45 pm while parking his car. He could not exit the vehicle and was transported to Liverpool Hospital ED.
On arrival, examination revealed left facial droop and hemiparesis (Medical Research Council grade 3/5) with preserved sensation. The National Institutes of Health Stroke Scale score was 7. His motor symptoms partially improved while in the ED. Nevertheless, intravenous thrombolysis (alteplase) was administered at 3:00 pm, approximately 2 h after symptom onset. He was admitted to the stroke unit. Magnetic resonance imaging of the brain demonstrated an acute infarct in the posterior limb of the right internal capsule (Figure 1). Transthoracic echocardiography and cardiac investigations were unremarkable.
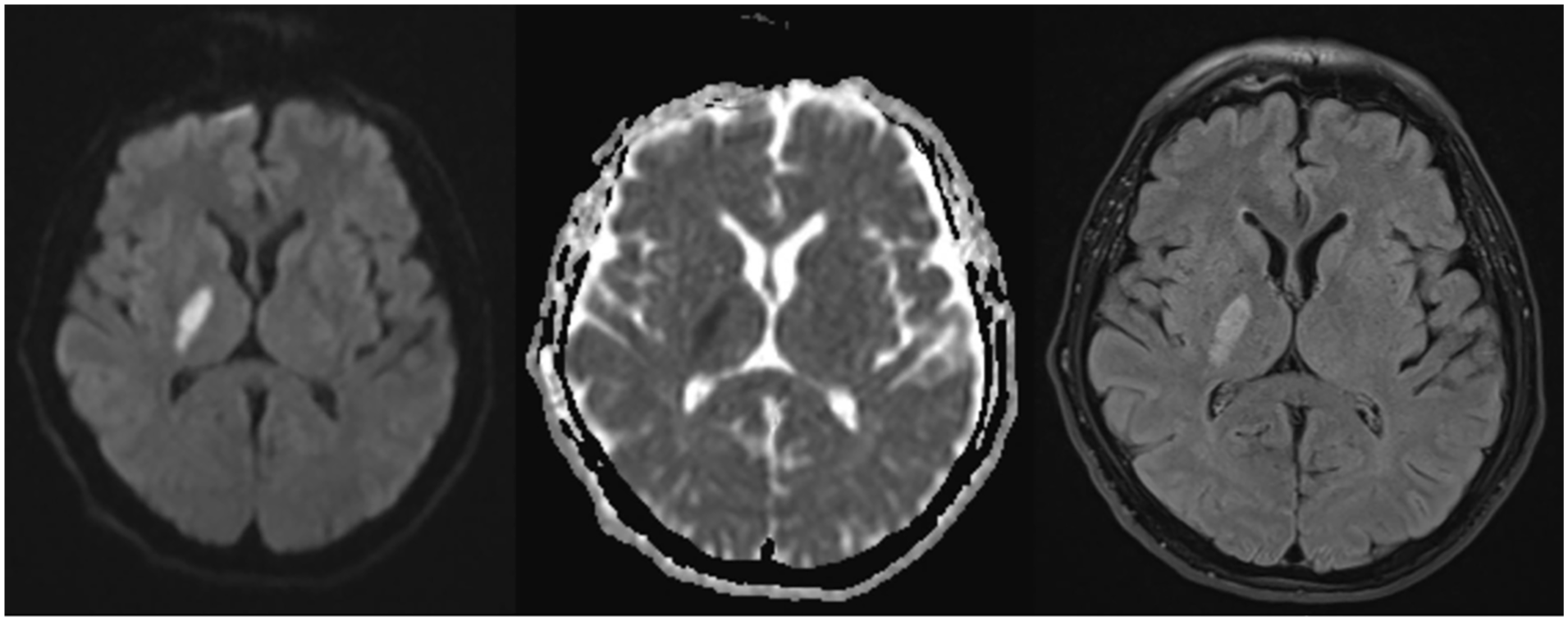
Axial magnetic resonance imaging brain images showing a small acute infarct in the posterior limb of the right internal capsule. From left to right: diffusion-weighted imaging (DWI), apparent diffusion coefficient (ADC), and fluid-attenuated inversion recovery (FLAIR) sequences.
On 8 March, the patient commenced dual antiplatelet therapy (DAPT) with aspirin and clopidogrel, which continued for 21 days. Clopidogrel was discontinued on 28 March, and aspirin was maintained. Atorvastatin 40 mg nocte was also initiated for secondary prevention.
The patient was transferred to inpatient rehabilitation on 8 March to address persistent left-sided weakness and functional deficits. A multidisciplinary programme was implemented, including occupational therapy, physiotherapy and speech pathology, with goals focused on restoring mobility and independence in daily activities.
Occupational therapy utilised the Graded Repetitive Arm Supplementary Programme (GRASP) Level 2 protocol to target upper limb recovery. Gross motor skills were trained using the Box and Block Test, while fine motor skills were addressed using the Nine-Hole Peg Test and object manipulation tasks (e.g. coins, pegs, nuts and bolts, weighted object transfer). Exercises were designed to enhance pincer grasp, release control and bilateral coordination.
Physiotherapy focused on gait re-training, progressive lower limb strengthening and dynamic balance tasks. Functional re-training simulated real-world activities such as navigating uneven surfaces and carrying household objects to promote mobility confidence and fall prevention.
The patient demonstrated progressive improvement throughout his rehabilitation. By discharge, he had regained independent ambulation and self-care capacity, with only minor residual fine motor deficits requiring outpatient follow-up. The integrated rehabilitation approach was instrumental in facilitating his recovery and restoring a high level of post-stroke functional independence.
Discussion
This case illustrates the typical form of CWS, with recurrent stereotyped, transient motor episodes without cortical features, culminating in an internal capsule infarct. 1 The pathophysiology of CWS remains unclear, but it is thought to involve penetrating artery disease due to small vessel lipohyalinosis, intermittent microembolism or haemodynamic compromise within the internal capsule. 5 Given the high risk of early infarction, treatment focuses on rapid symptom recognition and intervention. Evidence supports the use of intravenous thrombolysis in eligible patients, and short-term DAPT has been proposed to reduce recurrence and stroke risk.2,5,7–10 Blood pressure optimisation and statin therapy also play key roles in secondary prevention. 2 While acute interventions were central to this patient’s initial stabilisation, comprehensive rehabilitation was critical to restoring functional independence. Despite the small volume of infarction, the lesion’s location in the posterior internal capsule resulted in significant hemiparesis, underlining the strategic vulnerability of this region. Early transfer to inpatient rehabilitation enabled timely motor re-training and functional restoration.
A tailored rehabilitation programme was implemented, targeting both upper and lower limb deficits through structured, evidence-based approaches. The GRASP Level 2 was employed to enhance paretic arm function. The GRASP protocol has been validated for stroke-related upper limb rehabilitation. In a multi-site randomised controlled trial (RCT) of subacute stroke inpatients, those performing daily GRASP exercises showed significantly greater improvement in functional arm use compared to controls, with gains maintained at 5 months post-stroke. 11 GRASP participants also had better grip strength and increased use of the paretic arm in daily activities, highlighting the efficacy of repetitive task-oriented arm training. 11 This was evident in our patient, who regained substantial fine motor control through structured daily therapy.
The patient also engaged in targeted fine motor re-training using the Nine-Hole Peg Test and object manipulation tasks. Such fine motor training has been shown to enhance hand function beyond conventional therapy. The Nine-Hole Peg Test is a widely used measure of finger dexterity in stroke rehabilitation, and studies have confirmed its effectiveness in tracking and guiding fine motor recovery in patients recovering from an acute stroke. 12 These findings support the incorporation of repetitive fine motor task practice to improve coordination and hand function after stroke.
Lower limb rehabilitation focused on progressive resistance training, task-specific gait re-training and balance re-education. These approaches are supported by Cochrane reviews and meta-analyses of 21 RCTs demonstrating their safety and effectiveness in improving strength, walking speed, endurance and balance.13,14 Task-specific gait training is an effective method for improving walking ability after a stroke. A Cochrane review concluded that physical rehabilitation significantly improves walking capacity and balance in stroke survivors compared to no rehabilitation. 13 Providing sufficient gait practice intensity, such as more than 2.5 h per week of therapy, further enhances walking outcomes. 13 To mitigate the risk of falls and restore safe mobility, the patient participated in dynamic balance exercises that incorporated proprioceptive training and postural control strategies derived from Motor Relearning Programmes. Clinical studies have demonstrated that incorporating proprioceptive balance training yields superior post-stroke balance recovery compared to standard therapy alone. 15
Conclusion
CWS is a neurologically urgent condition with a high risk of progressing to a stroke, particularly internal capsule infarction. This case emphasises recognising the classical CWS presentation – recurrent, transient motor deficits without cortical features – and requires prompt, evidence-based interventions. Intravenous thrombolysis and short-course DAPT stabilise symptoms and prevent further neurological decline. Early multidisciplinary rehabilitation, with established recovery protocols for upper and lower limbs, is crucial for restoring independence. Upon admission to rehabilitation, the patient had moderate hemiparesis and mobility issues. After interventions such as the GRASP protocol, fine motor re-training, gait re-education and proprioceptive balance training, the patient showed significant improvement, achieving independent ambulation and self-care by discharge, with minor residual fine motor deficits. This case highlights the importance of integrating acute medical management with structured rehabilitation to optimise outcomes for CWS patients. Further research is needed to establish standardised treatment protocols for this high-risk syndrome.
Footnotes
Acknowledgements
The authors would like to thank the patient for giving his consent and cooperation in relation to the writing of this case report.
Ethical Considerations
No ethical approval is required for case report in our institution.
Consent to Participate
Informed consent was obtained from the patient in order to publish this care report.
Author Contributions
Quoc Dung Nguyen: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. Jim Xu: Conceptualisation, Methodology, Supervision, Validation, Writing – review & editing. Friedbert Kohler: Conceptualisation, Supervision, Validation, Writing – review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.