
Abstract
Objective
To test the hypothesis that chemoresistance in pancreatic cancer is mediated via extracellular signal-regulated protein kinase (ERK) 1/2 overactivity.
Methods
The human pancreatic cancer cell lines BxPC3, PANC-1 and a stably gemcitabine-resistant subline, PANC1GemRes, were treated with combinations of gemcitabine and the ERK1/2 inhibitor, U0126. Phosphorylated (p)ERK1/2 was examined by Western blotting; cell proliferation and apoptosis were quantified. A nude mouse xenograft model was established with each cell line, and the therapeutic efficacy of gemcitabine and U0126 alone or in combination was examined.
Results
Gemcitabine treatment visibly increased pERK1/2 levels in BxPC-3 and PANC-1 cells. PANC-1GemRes constitutively produced high levels of pERK1/2. U0126 treatment reversed the gemcitabine-associated increase in cell proliferation and reduction in apoptosis, in all three cell lines. Combination treatment with U0126 and gemcitabine inhibited tumour growth and promoted apoptosis in xenograft tumours derived from all three cell lines.
Conclusions
ERK1/2 activity may protect pancreatic cancer cells from chemotherapy-induced apoptosis. The combined use of an ERK1/2 inhibitor (such as U0126) together with gemcitabine may result in synergistic therapeutic effects at tolerable gemcitabine doses.
Keywords
Introduction
Pancreatic cancer has the worst prognosis of all major cancers, with a 5-year overall survival rate of ∼5%. 1 The current standard treatment for advanced pancreatic cancer is gemcitabine, which is a cytotoxic nucleoside analogue. The benefits of gemcitabine are modest, with a tumour response rate of 12% and a median survival time of 5 months. 2 Data from a small number of studies suggest that a combination of targeted therapy and gemcitabine has statistically significant benefits. 3 The extracellular signal-regulated protein kinases (ERK) 1 and 2 are potential targets for combination therapy. 4
The ERK1/2 signalling pathway is involved in the control of diverse cellular processes such as proliferation, survival, differentiation and motility. 4 This pathway is often upregulated in human tumours5,6 and represents an attractive target for the development of anticancer drugs.7–10 The inhibitor of mitogen-activated protein kinase kinase 1/2 (MAP2K1/2), U0126, has been shown to inhibit ERK1/2 phosphorylation effectively, 11 and to enhance radiosensitivity of rhabdomyosarcoma cells. 12 ERK1/2 has been shown to be activated in pancreatic carcinoma, 5 but little is known regarding its role in chemoresistance.
This study investigated the effects of ERK1/2 inhibition by U0126 and gemcitabine, alone and in combination, on a pancreatic carcinoma model in vitro and in vivo.
Materials and methods
Cell culture
Human pancreatic adenocarcinoma PANC-1 and BxPC-3 cells were obtained from American Type Culture Collection (Shanghai, China) and maintained in Dulbecco’s modified Eagle’s medium (DMEM) containing 10% fetal bovine serum (Life Technologies, Gaithersburg, MD). Cells were incubated in 75-cm2 culture flasks in a humidified atmosphere at 37°C with 5% carbon dioxide in air, and passaged on reaching 60–80% confluence.
Development of PANC-1GemRes
The pancreatic adenocarcinoma cell line PANC-1 was used to develop a gemcitabine-resistant cell line, PANC-1GemRes, as described previously. 13 Briefly, PANC-1 cells were serially subcultured through incrementally increasing gemcitabine concentrations, starting at the 50% inhibitory drug concentration (IC50), over 3 months. Persistence of stable resistance was confirmed by subculture in gemcitabine-free DMEM containing 10% fetal bovine serum; PANC-1GemRes retained the capacity for proliferation when returned to medium containing 5 µM gemcitabine.
Determination of gemcitabine IC50
The IC50 of gemcitabine was determined in each cell line. BxPC-3, PANC-1 and PANC-1GemRes cells were seeded at 1 × 104 per well in 96-well plates, in 0.1 ml of culture medium and cultured overnight. The next day, the medium was supplemented with 0–100 µM gemcitabine (Sigma, St Louis, MO, USA) for 48 h at 37°C. The IC50 was determined using 2,3-bis(2-methoxy-4-nitro-5-sulphophenyl)-2H-tetrazolium-5-carboxanilide (XTT) assay (Roche Molecular Biochemicals, Indianapolis, IN, USA) according to the manufacturer’s instructions. Cell proliferation was quantified by measuring the absorbance at 450 nm, and the IC50 for each of the cell lines was estimated from the semilogarithmic dose–response curves, by linear interpolation.
Cell proliferation and apoptosis analysis
Cells (BxPC-3, PANC-1 or PANC-1GemRes) were seeded at 1 × 104 per well in 96-well plates in 0.1 ml of culture medium and allowed to grow overnight. The next day, the medium was supplemented with IC50 gemcitabine for 48 h at 37°C in the presence or absence of 25 µM U0126 (Sigma, St Louis, MO, USA) (added 1 h before gemcitabine), or treated with 25 µM U0126 alone. Cell proliferation was quantified by XTT assay as described above. Parallel cultures were immediately fixed in 37% formaldehyde at room temperature for 30 min and allowed to dry overnight. Apoptosis was determined using the terminal deoxynucleotidyl transferase-mediated dUTP-biotin nick end labelling (TUNEL) method (Roche in situ Apoptosis Detection System; Roche, Mannheim, Germany), according to the manufacturer's instructions. Cells were examined by light microscopy; apoptosis was quantified as the mean number of stained cells as a percentage of total cells in five random high-power fields (×100 magnification).
Western blotting
Cells (BxPC-3, PANC-1 or PANC-1GemRes) were seeded at 1 × 104 per well in 96-well plates, in 0.1 ml of culture medium, and allowed to grow overnight. The next day, the medium was supplemented with IC50 gemcitabine for 48 h at 37°C. Cells were rinsed once with cold phosphate buffered saline (PBS; 20 mM, pH 7.6) and lysed in radioimmunoprecipitation assay buffer (50 mM Tris-HCl, pH 8.0, 150 mM sodium chloride, 1% nonyl phenoxypolyethoxylethanol, 0.5% sodium deoxycholate, and 0.1% sodium dodecyl sulphate [SDS]), containing 0.3 mg/l protease inhibitor (Roche), for 15 min on ice. Cell lysates were centrifuged at 28 340
Mouse tumour model
Male athymic nu/nu mice (aged 5 weeks; weight 18–20 g; specific pathogen free) were obtained from the Laboratory Centre of Shandong University. Mice were housed in microisolator cages, with autoclaved bedding in a specific pathogen-free facility, with a 12-h light/dark cycle. Animals received water and food ad libitum and were observed for signs of tumour growth, activity, feeding and pain, in accordance with the guidelines of the Standing Committee on Animals, Shandong University. The study protocol was approved by the Ethics Committee of Jinan Central Hospital of Shandong University.
Xenograft tumours were established by subcutaneous injection of 1 × 106 BxPC-3, PANC-1 or PANC1GemRes cells in 20 µl of PBS (pH 7.6). When tumours were 50–100 mm3 in diameter (after 4 weeks) the mice were divided into four groups (n = 8 per group), to receive the following treatments by intraperitoneal injection, three times per week for 4 weeks (all injections were of identical volume): 250 µg/kg U0126 (in dimethyl sulphoxide; DMSO); 100 mg/kg gemcitabine (in 1% DMSO); 250 µg/kg U0126 and 100 mg/kg gemcitabine (in DMSO); and control group (1% DMSO). Tumour growth was monitored with calipers three times per week during the treatment period; tumour volume was calculated according to the formula (length × width2)/2. On completion of treatment, mice were sacrificed and the tumours were excised.
Ttissue samples were immediately snap-frozen in liquid nitrogen and stored at −80°C until used for analysis. Apoptosis was quantified in frozen sections of tumour tissue (4-µm thick) using TUNEL assay (Roche in situ Apoptosis Detection System), according to the manufacturer’s instructions, as previously described. 14 Sections were examined by light microscopy and the apoptosis index was determined by counting ≥1000 cells in 5 randomly selected high-power fields (×200 magnification).
Statistical analyses
All experiments were performed a minimum of three times. Data were presented as mean ± SD and compared using Student’s t-test. A P-value <0.05 was considered to be statistically significant. Statistical analyses were performed using SPSS® software, version 11.0 (SPSS Inc., Chicago, IL, USA) for Windows®.
Results
Effect of the extracellular signal-regulated protein kinase 1/2 inhibitor U0126 on the 50% inhibitory drug concentration (IC50) of gemcitabine in the human pancreatic adenocarcinoma cell lines BxPC-3 and PANC-1, and in a gemcitabine-resistant PANC-1 derived cell line, PANC-1GemRes.
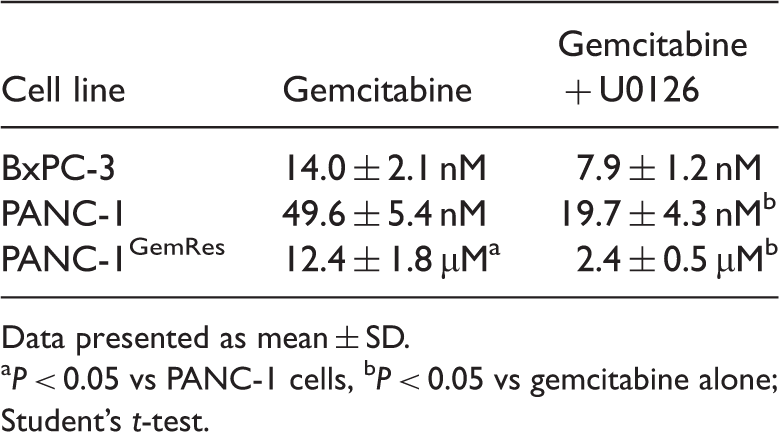
Data presented as mean ± SD.
P < 0.05 vs PANC-1 cells, bP < 0.05 vs gemcitabine alone; Student’s t-test.
Western blot analysis of pERK1/2 in PANC-1, BxPC-3 and PANC-1GemRes cells, after treatment with gemcitabine, is presented in Figure 1. BxPC-3 cells appeared to have no constitutive pERK1/2 (absence of protein at 0 h). Gemcitabine treatment resulted in visibly increased pERK1/2 levels in BxPC-3 and PANC-1 cells at 6 and 12 h after treatment, respectively. PANC-1GemRes cells constitutively produced relatively high levels of pERK1/2 that were unchanged by gemcitabine treatment.
Western blot analysis of phosphorylated signal regulated extracellular kinase (pERK)1/2 and β-actin in human pancreatic adenocarcinoma cell lines BxPC-3 and PANC-1, and a gemcitabine-resistant PANC-1 derived cell line, PANC-1GemRes. Cells were treated with their 50% inhibitory concentration of gemcitabine (14 nM, 49.6 nM and 12.4 µM, respectively) for 48 h.
Effect of treatment with U0126 and/or gemcitabine on apoptosis a in the human pancreatic adenocarcinoma cell lines BxPC-3 and PANC-1, and a gemcitabine-resistant PANC-1 derived cell line, PANC-1GemRes.

Data presented as mean ± SD.
mean percentage of apoptotic cells as a proportion of total cells in five random high power fields (× 100 magnification).
P < 0.05, **P < 0.01, ***P < 0.001 versus control; Student’s t-test.
Effect of treatment with U0126 and/or gemcitabine on tumour volume and apoptosis in mouse xenograft models of pancreatic carcinoma, derived from human pancreatic adenocarcinoma cell lines BxPC-3 and PANC-1, and a gemcitabine-resistant PANC-1 derived cell line, PANC-1GemRes.

Data presented as mean ± SD.
mean percentage of apoptotic cells as a proportion of total cells in five random high power fields (×200 magnification).
P < 0.05, **P < 0.01, ***P < 0.001 versus control; Student’s t-test.
In vivo, combination treatment with U0126 and gemcitabine resulted in significantly increased apoptosis compared with controls, in tumours derived from all three cell lines (P < 0.001 for each comparison; Table 3). Neither U0126 nor gemcitabine treatment alone had any effect on apoptosis in vivo.
Discussion
Human pancreatic cancer is characterized by high intrinsic (de novo) and acquired (therapy induced) resistance to traditional chemo- and radiation therapy. 15 Understanding the underlying mechanisms of drug resistance in pancreatic cancer is critical in order for new and effective treatments to be developed for this deadly disease. Gemcitabine is the standard chemotherapeutic agent for pancreatic cancer patients, but its clinical impact is limited by the high degree of inherent and acquired resistance. 15
Studies have found ERK1/2 to be involved in tumour chemoresistance,16,17 and increased ERK1/2 activity has been shown to correlate with inherent gemcitabine resistance in intrahepatic cholangiocarcinoma cells. 18 Levels of pERK1/2 appeared to be higher in PANC-1GemRes cells than in the gemcitabine-sensitive PANC-1 parental cell line in the present study, suggesting that gemcitabine resistance may be mediated via pERK1/2.
Inhibition of ERK1/2 activity by U0126 promoted gemcitabine-induced apoptosis in human pancreatic adenocarcinoma cell lines and reversed acquired gemcitabine resistance in PANC1GemRes in the present study. BxPC-3 cells, which were shown not to produce pERK1/2 constitutively in the present study, were sensitive to gemcitabine-induced apoptosis in vitro. These data suggest that inherent ERK1/2 activity may play an important role in gemcitabine resistance.
It has been suggested that the ERK1/2 pathway mediates apoptosis induced by various stimuli, including cisplatin. 19 This is supported by the finding that Nic-T24 cells (which have low ERK1/2 activity) tend to remain in G0/G1 phase rather than undergo apoptosis, in response to antitumour agents. 17
In conclusion, the findings of the present study suggest that high ERK1/2 activity protects tumour cells from chemotherapy-induced apoptosis, in pancreatic cancer. The combined use of an ERK1/2 inhibitor (such as U0126) and gemcitabine may result in synergistic therapeutic effects at tolerable gemcitabine doses. Further studies are required to elucidate the mechanism by which ERK1/2 inhibition enhances chemotherapeutic effects. The significance of pERK1/2 as a therapeutic marker in clinical specimens remains to be investigated.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.