
Abstract
Argentina and Australia endured among the most severe COVID-19 lockdowns globally. This study examined which artistic creative activities (ACAs) Argentinians in the Buenos Aries region used to support their mental health and wellbeing and compared these findings with existing data for Australians (primarily from Victoria) across a similar period. Adult Argentinians (N = 86) responded to an online survey regarding 27 listed ACAs, as well as ratings of anxiety, depression, and loneliness. While “watching films and television” was the most commonly reported ACA, it was not rated as effective in supporting mental health and wellbeing. Conversely, musical ACAs were ranked highest. We consider evidence from Australia, North America, and South America that musical ACAs (especially music listening) have been most effective at supporting mental health and wellbeing during the COVID-19 pandemic by way of avoidance-based emotion regulation. We also conclude from the data that Argentinians tended to place greater importance on music-based ACAs than Australians.
Keywords
To date, both Argentina and Australia have experienced some of the longest periods of continuous lockdown worldwide due to rising infections of COVID-19. On March 20, 2020, the Argentinian government implemented a compulsory countrywide lockdown in an effort to “flatten the curve” of infections (Badellino et al., 2021; Lucuix et al., 2021). In some provinces, the lockdown was lifted by August 2020, whereas other provinces experienced intermittent periods of additional lockdown throughout the latter half of the year. The greater region of Buenos Aires, however, experienced the most intense restrictions, which amounted to a record 234 days in continuous lockdown from March to November (Boaz, 2021; Elisondo, 2021). This was the longest continuous lockdown anywhere in the world up to this point, and was only later surpassed by lockdowns in Melbourne, Australia, during 2021 (Boaz, 2021). In Australia, the majority of lockdowns during 2020 took place in Victoria, with the city of Melbourne receiving the most severe restrictions. Residents of Melbourne experienced an initial lockdown period of 43 days, between March and May 2020, followed by a second lockdown of 111 days between July and October 2020. These Victorian lockdown periods continued until October 2021 (Boaz, 2021).
Despite the necessity of such measures for public health and safety, there is a wealth of literature indicating the significant detrimental impact that lockdowns around the world have had on global mental health and wellbeing, such as increased reports of anxiety, depression, and thoughts of suicide (see, e.g., Czeisler et al., 2021; Howlin & Hansen, forthcoming; Salari et al., 2020). Consequently, many studies have examined ratings of mental health and wellbeing for various subpopulations, focusing on predictors such as age and gender (Ausín et al., 2021; Bu et al., 2020; Fisher et al., 2020; Torrente et al., 2021; Torrente et al., 2022; Zhang et al., 2020), household size (Badellino et al., 2021; López Steinmetz et al., 2020; Oh & Neal, 2021), and occupational area and status (Cag et al., 2021; Smallwood et al., 2021; Sunjaya et al., 2021). Yet, overall, less research focus has been given to examinations of how mental health and wellbeing can best be maintained during pandemic crises (Drake et al., 2022).
Research into such protective factors for mental health and wellbeing have focused on aspects such as time spent working at a screen (Mata et al., 2021), whether or not people attend psychological counseling (Kumari & Singh, 2021), time spent in nature (Ribeiro et al., 2021), and time spent in online social interaction (Moore & March, 2022; Pandey et al., 2021; Stuart et al., 2021). Furthermore, a growing body of research has indicated that increased exercise can be a robust method for offsetting detriments to mental health (e.g., Chmiel et al., 2022; Colley et al., 2020; Coyle et al., 2021; Faulkner et al., 2021). Yet in the present work, we focus on the relationship between engagement in artistic creative activities (ACAs) and mental health and wellbeing while in periods of COVID-19-related lockdown.
ACAs refer to creative activities that specifically involve the arts, as defined by Fancourt et al. (2019). This includes fine art activities—such as those relating to music, theatre, dance, poetry, literature, and the like—but also extends to other activities which can incorporate artistic elements and lead to creative outputs, such as cooking, gardening, and crafting or textile work, as a non-exhaustive list. During periods of lockdown, many settings in which people can engage in ACAs as a group (e.g., live performances, rehearsals, classes, exhibitions, and so on) were required to be shut down for safety precautions. Despite this, various adapted forms of these ACAs still tended to emerge around the world as a means of social communication and expression, as evidenced through music-making between balconies in locked-down suburban areas (Ferreri et al., 2021; Granot et al., 2021; Gupta, 2020; Hansen et al., 2021; Howlin & Hansen, forthcoming).
Music and the arts have been shown to play an important role in regulating emotion in different contexts during the pandemic, helping individuals influence which emotions they have, and when and how they experience and express them (Martín et al., 2021; Steinberg et al., 2021). And, despite the various cultural differences between Australia and Argentina—and the different ways music and the arts may be embedded into everyday life in each country (Moore & Baker, 2009)—the pandemic has provided a unique opportunity to examine how people in these different cultural contexts use ACAs to respond to pandemic crisis, regulate emotion, and support their mental health and wellbeing during extended periods of lockdown. By gaining a better understanding of the potential benefits that ACAs can provide to mental health and wellbeing during lockdown periods, we aim to expand the evidence base that can inform policy and the development of future projects, so that they may better support public health in times of crisis. Furthermore, by tracking which ACAs were most undertaken and which were most ceased during the COVID-19 pandemic, we hope to provide additional insight as to which creative industries and fields may warrant greater support during future crises. Globally, the creative arts sector has seen unprecedented losses in jobs and revenue during the pandemic (see, e.g., Browne, 2020; Flore et al., 2021; Florida & Seman, 2020; Jeannotte, 2021), making this an area of urgent need.
Existing Research on ACAs in Australia During the Pandemic
Relatively few studies have examined the role that ACAs have played in supporting Australian mental health and wellbeing during the COVID-19 pandemic. Most notably, a study by Kiernan, Chmiel, Garrido et al. (2021) examined which ACAs were undertaken and which were ceased using data collected in 2020, as well as measures of mental health and wellbeing. While watching films and television was the most frequently undertaken ACA, it was not deemed effective at making participants feel better during the pandemic. The most effective ACAs at making Australians feel better were listening to music, singing, and dancing, although singing and dancing both ranked as two of the three most commonly ceased ACAs during lockdown, meaning that the ACAs of greatest benefit were often those that participants could not (or did not) do. Kiernan, Chmiel, Garrido et al. (2021) also examined the ways ACAs provided a medium for different emotion regulation strategies using the Emotion Regulation Strategies for Artistic Creative Activities scale (ERS-ACA scale; see Fancourt et al., 2019) as well as different modes of music engagement reported by participants using the music engagement questionnaire (MusEQ scale; Vanstone et al., 2016).
They found that Australians were more likely to use ACAs for avoidance-based emotion regulation (e.g., as a distraction or escape from reality) as opposed to approach-based (e.g., problem-solving) or self-development-based (e.g., enhancing self-identity) emotion regulation. These findings also indicated that Australians were more likely to engage in musical activities for the purpose of emotion regulation than for any other reason (e.g., rather than to express a musical identity or to scaffold daily activities). Importantly, the findings of Kiernan, Chmiel, Garrido et al. (2021)concerning the popularity and effectiveness of music listening and the underlying avoidance-based emotion regulation strategies used during the lockdowns in Australia were corroborated by a study based primarily on respondents from the USA (Drake et al., 2022). Granot et al. (2021) observed similar results across parts of South and Central America, Asia, Europe, the UK, and the USA, although they discuss “diversion from the crisis” as a wellbeing goal rather than avoidance-based emotion regulation explicitly. Together, these findings suggest that despite significant cultural differences, commonalities remain in the ways music supports people around the world during times of pandemic crisis.
Additionally, a qualitative study by Kiernan and Davidson (2023) used in-depth interviews to examine how music helped participants cope with experiences of social isolation during lockdown in Australia and described the findings in terms of five key themes (perceived control, dynamic connection, identity, mobility, and presence). A repeated measures study by Krause et al. (2021) also surveyed Australian undergraduates every 2 weeks between April and June 2020, with participants being asked to indicate their life satisfaction, as well as their engagement with four specific types of media: listening to music; video/computer gaming; watching films, television, or any other video streaming; and on social media. Music listening was associated with positive life satisfaction, whereas watching films and television was associated with negative life satisfaction. While we acknowledge that the number of ACAs examined by Krause et al. was limited, these findings highlight the potential benefits that certain ACAs can provide for mental health and wellbeing and suggest the need for further research into how and why people turn to some ACAs and not others during times of pandemic crisis. Further work by Vidas et al. (2021) asked Australian undergraduate students to rate the effectiveness of specific stress management strategies, taken from an existing list by Thayer et al. (1994). However, this list only contained one ACA (music listening), and so is of limited relevance here. Additionally, we note that while there were social distancing and non-essential workplace closures which certainly affected the student participants socially and economically, there were virtually no cases of COVID in the locations where these two student-based studies were conducted.
Existing Research on ACAs in Argentina During the Pandemic
As with Australia, there has been limited research focusing on the relationship between ACAs and Argentinian wellbeing during the COVID-19 pandemic. Prior work has largely been limited to two recent papers led by Romina Cecilia Elisondo (Elisondo, 2021; Elisondo & Melgar, 2021). The first of these studies (Elisondo, 2021) examined which ACAs Argentinians living in the province of Córdoba had undertaken during periods of lockdown in 2020 (although we note that Elisondo includes some activities that we do not consider ACAs, such as physical activity, cleaning/tidying the home, and children's homework). Elisondo (2021) reported the most frequently undertaken ACAs as (1) cooking; (2) painting and drawing; (3) reading; (4) sewing, embroidery, and weaving; and (5) photography. The second study (Elisondo & Melgar, 2021), which used a qualitative approach, again focused on the province of Córdoba (totaling 84% of participants in this case). In this second study, cooking was again the most frequently reported ACA, followed by crafting/textile work, visual arts (drawing, painting, photography, and so on), and music- and dance-related activities.
Despite providing a valuable insight, Elisondo's studies also contain several key limitations. First, data from these studies pertaining to engagement in ACAs were collected during the first few weeks of a lockdown that lasted up to 8 months (specifically referring to those living in the greater Buenos Aires region). While one study was longitudinal (Elisondo, 2021), the second phase of data collection involved qualitative interviews with a convenience subsample (n = 30) which “indicated that participants mentioned the same creative activities” (p. 120) but which focused on other issues such as life changes and emotions during lockdown. Thus, it is not sufficiently clear from this study if, or how, engagement in ACAs may have changed toward the end of 2020. This is a notable point considering that engagement with ACAs has been strongly linked to mental health and wellbeing (e.g., Fancourt et al., 2019; Garrido & Schubert, 2011a, 2011b; Gupta, 2020; Kapoor & Kaufman, 2020; Krause et al., 2021; Leckey, 2011; Martínez-Castilla et al., 2021). When coupled with the fact that several studies have indicated that Argentinian mental health progressively declined over the lockdown period (Etchevers et al., 2021; López Steinmetz et al., 2020; Torrente et al., 2022), it is reasonable to assume that as the lockdown progressed, the most frequently undertaken ACAs may have changed. Therefore, further detailed investigation during the latter months of the 2020 lockdown is warranted.
Second, it is worth noting that almost 92% of participants across the combined studies by Elisondo resided in the province of Córdoba, whereas less than 4% resided in the Buenos Aires area (which received far greater lockdown restrictions). As such, Elisondo's findings are not representative of people residing in the greater Buenos Aires region, which is where close to 40% of the Argentinian population resides (Bolay, 2020). To best understand how ACAs supported Argentinians during the lockdown periods, we propose that Buenos Aires provides the ideal area to focus study. Third, while both of Elisondo's studies examined which ACAs were most frequently undertaken during the lockdown period, neither study reported which ACA participants had ceased during the lockdown. This is an important aspect for policy makers to better understand as it may provide insight into the feasibility of specific activities in such contexts, as well as identifying which ACAs warrant further support during times of crisis.
Finally, while Elisondo's studies broadly examined emotions and subjective wellbeing in relation to engagement in ACAs, they used general and open-ended questions rather than standardized measures pertaining to mental health and wellbeing. ACAs can provide a medium for specific emotion regulation strategies (Fancourt et al., 2019), and while other studies suggest that these strategies have played an important role in supporting mental health and wellbeing during the pandemic (e.g., Chmiel et al., 2022; Kapoor & Kaufman, 2020; Kiernan, Chmiel, Garrido et al., 2021), this aspect was not explored in Elisondo's research.
Aims
The two aims of this study were (1) to investigate the role of ACAs in regulating emotion and supporting the mental health and wellbeing of Argentinians during the COVID-19 pandemic and (2) to identify and examine any potential similarities and differences in the ways Argentinians and Australians used ACAs to support their mental health and wellbeing during the pandemic. To enable this comparison, data collected during 2020 were used for this study. The following five research questions (RQs) were developed:
Methods
The method was modeled on that used by Kiernan, Chmiel, Garrido et al. (2021), to enable the best possible comparison. Therefore, this study examined which ACAs were undertaken and which were ceased during periods of lockdown, and accompanying ratings were collected for mental health and wellbeing and for engagement with ACAs. Data were gathered via an anonymous online survey made available to the general public of Argentina who were aged 18 or older. The survey questions used by Kiernan, Chmiel, Garrido et al. (2021) were transcribed to Spanish by a native Argentinian (author HR), to ensure accuracy. While anyone within Argentina was able to take part in the survey, we targeted people living in the greater Buenos Aires region due to the extreme lockdown measures in this area. Responses were collected between October 7, 2020, and December 10, 2020, inclusive. This time period aligned with the final 2 months of the Buenos Aires lockdown of 2020 and coincided with what was at the time a record number of cases within the country (Ritchie et al., 2020).
ACAs, Emotion Regulation, and Music Engagement
To collect data about ACAs undertaken and/or ceased during the pandemic a list of 26, ACAs were developed (see Table 1), based on that used by Fancourt et al. (2019) and Kiernan, Chmiel, Garrido et al. (2021). Participants could also add up to four unlisted ACAs via “Other” options that were accompanied by open-ended response boxes. As the “Other” responses were provided in Spanish, these responses were individually validated by author HR. While activities such as music listening or watching TV or films are sometimes not regarded as ACAs, Kiernan, Chmiel, Garrido et al. (2021) included these based on the fact that domestic media consumption typically increases the longer people stay at home (Mikos, 2020) and because receptive engagement with artistic media can be considered “creative” on account of its capacity to generate new perspectives on what is already familiar (Chan, 2016). Additionally, because “the cinematic” is an aesthetic concept increasingly used to describe the artistry of big-budget television shows (such as AMC's Breaking Bad, which ran from 2008 to 2013, and many others since then; see Restivo, 2019) and because film and television scholarship often considers the two in relation to one another under the umbrella of “screen media” (Stadler, 2020), the item “watching films or TV shows” was retained in the list of ACAs for the purposes of this study as per Kiernan, Chmiel, Garrido et al. (2021). We also suggest that the wording of “TV shows” in the item name and the accompanying contextual information provided to participants about the study's focus on ACAs indicated with sufficient clarity that this item did not refer to purely informative television broadcasts such as news or weather updates, but this potential ambiguity may be worthy of consideration in future studies.
ACAs Listed in the Survey, in Order of How Frequently Argentinian Participants Reported Undertaking Them During the COVID-19 Pandemic in 2020.
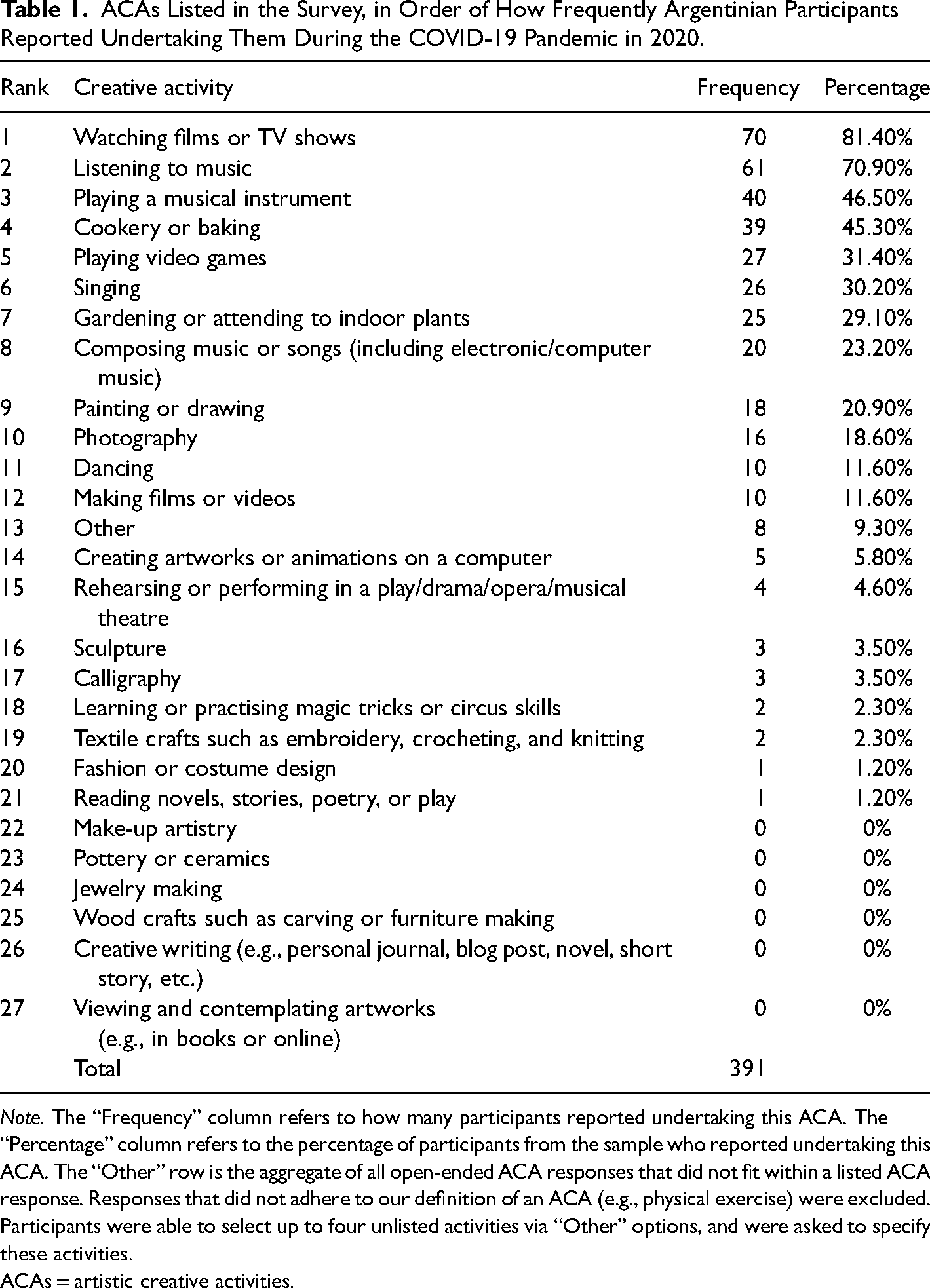
Note. The “Frequency” column refers to how many participants reported undertaking this ACA. The “Percentage” column refers to the percentage of participants from the sample who reported undertaking this ACA. The “Other” row is the aggregate of all open-ended ACA responses that did not fit within a listed ACA response. Responses that did not adhere to our definition of an ACA (e.g., physical exercise) were excluded. Participants were able to select up to four unlisted activities via “Other” options, and were asked to specify these activities.
ACAs = artistic creative activities.
Participants were asked to indicate which ACAs, if any, they had been undertaking since the COVID-19 pandemic began and also which ACAs, if any, they had ceased due to the COVID-19 pandemic. For any ACAs that the participant selected, they were asked to enter the average amount of weekly hours they would spend on that ACA during the pandemic. Participants were also asked to rank their selected ACAs in terms of their effectiveness in making them “feel better,” with rank 1 equating to the most effective. To examine which emotion regulation strategies participants were using while engaging with ACAs, all participants completed the ERS-ACA scale (Fancourt et al., 2019). This scale was completed only once, and in relation to the ACA that they rated as most effective at making them feel better. The ERS-ACA is made up of four subscales concerning “Avoidance” strategies (distraction or escapism from negative experiences), “Approach” strategies (active confrontation of negative experiences), “Self-development” strategies (those concerning reaffirmation of a sense of self), and an overall “General factor” that is the mean rating of all responses.
Additionally, participants who selected that they had been undertaking at least one music-based ACA were also presented the MusEQ scale (Vanstone et al., 2016), which measures engagement with music in everyday life. The MusEQ scale contains six separate subscales concerning music uses in routine life (“Daily” subscale), emotional and mood regulatory aspects of musical experience (“Emotion” subscale), social “performance” of a musical identity (“Perform” subscale), consumer choices for music (“Consume” subscale), responses made in synchrony with music being heard such as foot tapping or humming (“Respond” subscale), and aesthetic musical preferences (“Prefer” subscale). MusEQ was only completed once, regardless of how many music-based ACAs the participant had selected.
Wellbeing Scales and Demographic Aspects
Four measures pertaining to mental health and wellbeing were used. These mental health and wellbeing scales are typically used to identify anxiety, depression, or loneliness in participants; however, in this study, the scales are used to provide a general overview of participant mental health and wellbeing. Therefore, as detailed below, we inverted these four scales from their traditional scoring methods, such that in this work 0 equates to the worst a participant can feel and higher scores equate to the participant feeling better.
The GAD7 scale (Spitzer et al., 2006) was used to assess severity of anxiety symptoms ranging from 0 (most anxiety) to 21 (least anxiety), and the PHQ9 scale (Kroenke et al., 2001) was used to measure severity of depressive symptoms ranging from 0 (most depression) to 27 (least depression). Two separate scales were used to assess self-reported loneliness, based on the UCLA Loneliness Scale (Russell, 1996). The first loneliness scale asked for responses relating to “Before the COVID-19 pandemic began,” whereas the second loneliness scale asked for responses relating to “Since the COVID-19 pandemic began.” The two loneliness scales are henceforth referred to as “UCLA Before” and “UCLA Since,” with each ranging from 0 (most loneliness) to 6 (least loneliness). These four scales were intended to give a general overview of the mental health and wellbeing of participants during the COVID-19 pandemic, although the authors acknowledge that these scales do not cover the entire breadth of this area (Dodge et al., 2012).
The survey additionally collected the demographic and lifestyle variables of age, gender, household size, and the province the participant currently resides in. Participants were also asked to indicate how much exercise they were currently undertaking, in comparison to before COVID-19, with possible responses being “less,” “the same,” and “more.”
Ethics Approval
This study received approval from the Human Research Ethics Committee of the University of Melbourne (Ethics ID 2056873.1). Participation was voluntary, and the survey could be stopped at any point after commencement. Participants read a Participant Information Sheet prior to their agreement to take part, which indicated that the focus of the study was on engagement with ACAs during the COVID-19 lockdown periods. Upon completion of the survey, participants were able to opt in for the draw of a USD $150 gift voucher.
Results
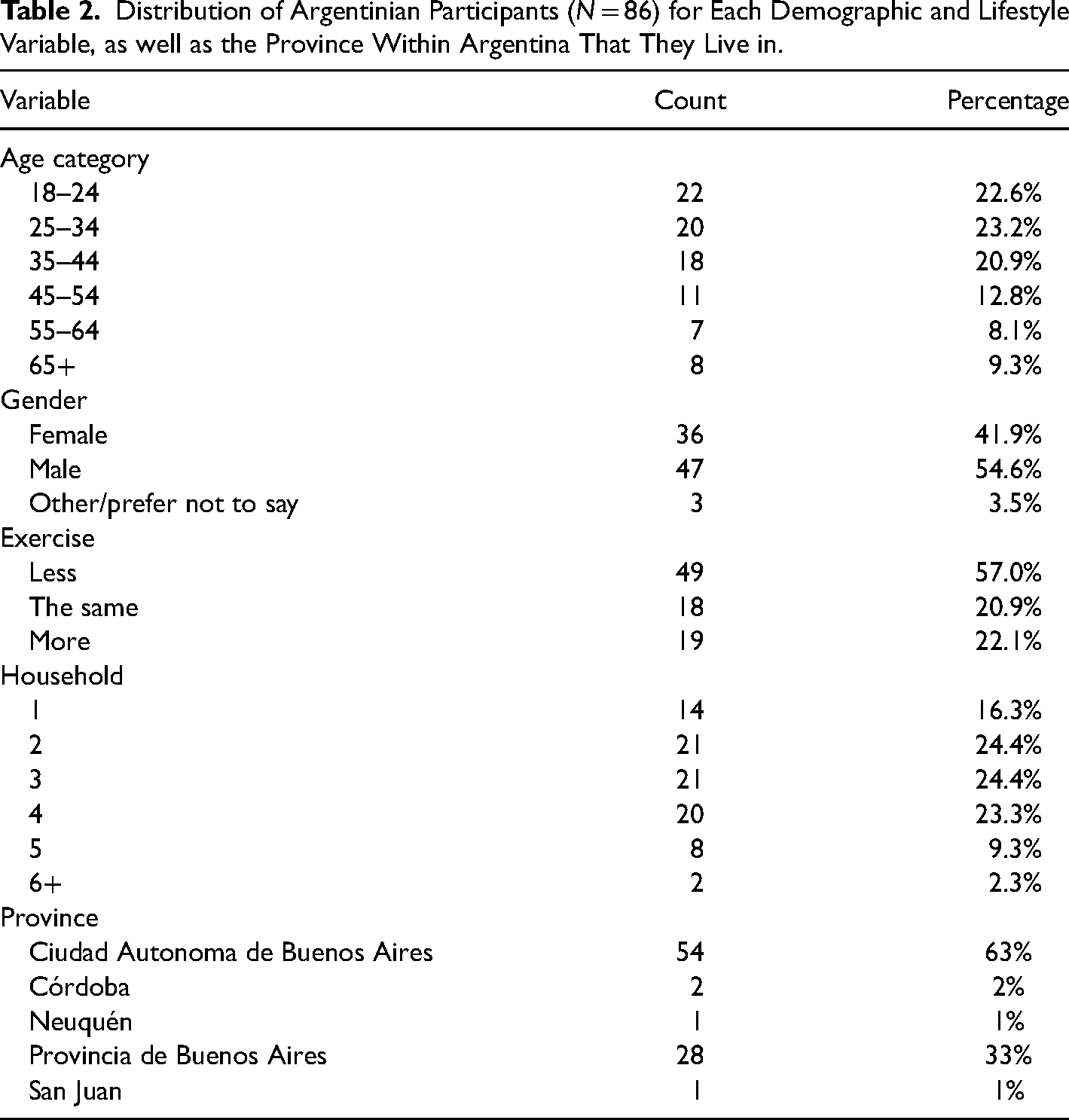
A total of 112 participants from the general Argentinian population responded to the online survey, although 26 responses (28%) were incomplete and so were removed from the data set. This left a usable sample of 86 responses. The distributions of age, gender, exercise, household size, and province for these 86 participants are reported in Table 2. As intended, 82 (95%) of participants were from the greater Buenos Aires area. Internal consistency of the four mental health and wellbeing scales for the 86 participants was measured with Cronbach's alpha. This score (α = 0.72) passed the suggested threshold for internal reliability (see Tavakol & Dennick, 2011). Descriptive statistics for these four scales were: GAD7 (M = 13.9, SD = 5.2), PHQ9 (M = 20.2, SD = 4.5), UCLA Before COVID-19 (M = 4.9, SD = 1.3), and UCLA Since COVID-19 (M = 4.2, SD = 1.8).
Distribution of Argentinian Participants (N = 86) for Each Demographic and Lifestyle Variable, as well as the Province Within Argentina That They Live in.
RQ1: ACAs Undertaken and Ceased During the COVID-19 Pandemic in 2020
Collectively the Argentinian participants reported spending on average 18.2 hours engaging with ACAs in a week (SD = 15.9). Additionally, the ACAs that these Argentinian participants undertook during the 2020 COVID-19 pandemic are reported in Table 1, listed in order of frequency. Watching films or TV shows was the most popular ACA, with listening to music ranking second. Playing a musical instrument and cookery or baking ranked third and fourth, respectively. ACAs ceased during the 2020 COVID-19 pandemic are reported in Table 3. The most stopped ACAs were rehearsing or performing in a play (or similar), dancing, playing a musical instrument, listening to music, and composing music or songs. Importantly, insofar as rehearsals/performances and dancing involved music, all five of these ceased ACAs contain music as a central component.
ACAs ceased by Argentinian participants during the COVID-19 pandemic in 2020.
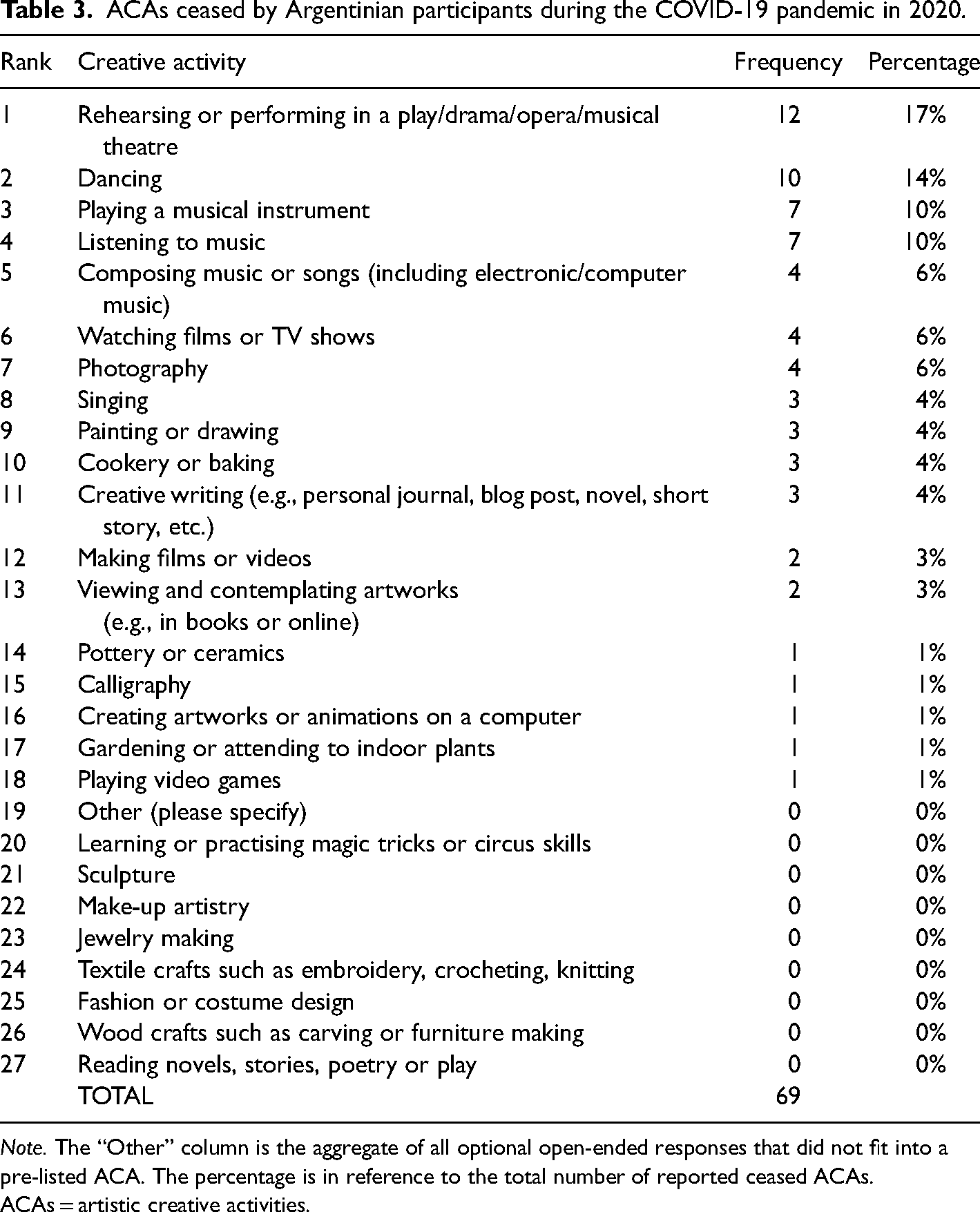
Note. The “Other” column is the aggregate of all optional open-ended responses that did not fit into a pre-listed ACA. The percentage is in reference to the total number of reported ceased ACAs.
ACAs = artistic creative activities.
RQ2: Most Effective ACAs at Making Participants “Feel Better”
Each participant ranked their undertaken ACAs from the most effective at making them feel better to the least effective. Table 4 reports these findings, ordered by the M of the ranking score (where rank 1 = most effective). The most effective ACA was composing music or songs, followed by rehearsing or performing in a play (or similar), followed by playing a musical instrument. The next most effective ACAs were listening to music, singing, and cookery or baking. Thus, the top 5 ranked ACAs for wellbeing contained music as a central component. This is reminiscent of the findings reported by Kiernan, Chmiel, Garrido et al. (2021), for which listening to music, singing, and dancing were ranked in the top 5 for making participants feel better. Also in line with Kiernan, Chmiel, Garrido et al. (2021) is the fact that despite watching films or TV shows being the most commonly undertaken ACA, this ACA ranked approximately halfway down the list in terms of making participants feel better.
ACAs Ranked as the Most Effective at Making Argentinian Participants “Feel Better” During the COVID-19 Pandemic in 2020.
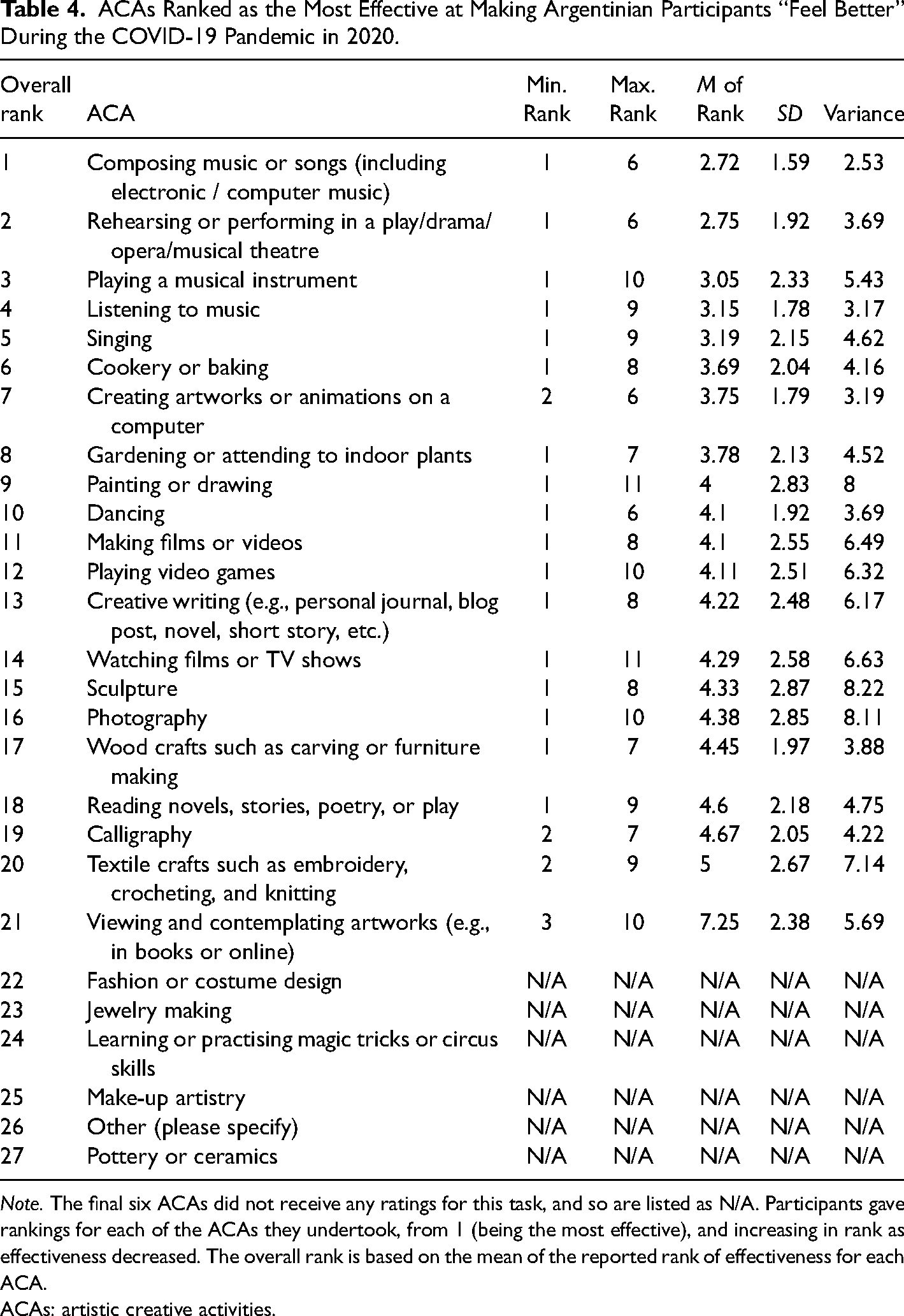
Note. The final six ACAs did not receive any ratings for this task, and so are listed as N/A. Participants gave rankings for each of the ACAs they undertook, from 1 (being the most effective), and increasing in rank as effectiveness decreased. The overall rank is based on the mean of the reported rank of effectiveness for each ACA.
ACAs: artistic creative activities.
RQ3: Emotional Regulation and Musical Engagement Strategies
Descriptive statistics for each ERS-ACA subscale and each MusEQ subscale are reported in Supplemental Table 1, within the Supplemental Material. A within-subject analysis of variance (ANOVA) was performed on the ERS-ACA data to compare the subscales, and a second within-subject ANOVA was performed on the MusEQ data to again compare the subscales. Both the ERS-ACA ANOVA (F(3,255) = 10.71, p < .001, ηp2 = .112) and the MusEQ ANOVA (F(3,225) = 10.71, p < .001, ηp2 = .118) were significant; the MusEQ ANOVA violated the assumption of sphericity and so used Greenhouse–Geisser correction. Šidák post hoc comparisons between the various subscales are reported in Supplemental Table 2. The ERS-ACA “Avoidance” subscale was significantly higher than all other ERS-ACA subscales, indicating that during the 2020 COVID-19 pandemic, the Argentinian participants were most commonly engaging with ACAs for avoidance or escapist purposes. For MusEQ, the “Emotion” subscale was significantly higher than all other subscales apart from the “Prefer” subscale. This indicates that these Argentinian participants were most likely to use music during the 2020 COVID-19 pandemic to regulate their emotions.
RQ4: Correlation Analysis
A correlation analysis was performed to examine relationships between (1) the four mental health and wellbeing scales, (2) engagement with ACAs (being the number of weekly hours spent on ACAs, and also the ERS-ACA and MusEQ subscale scores), and (3) demographics and lifestyle variables (age, household, and exercise). Kendall's tau-b correlation was used due to the mixture of continuous and ordinal variables. Coefficient and significance values are reported in Table 5.
Coefficients and Significance for Kendall's tau-b Correlation, Between the Four Wellbeing Scales, the Four ERS-ACA Subscales, the Six MusEQ Subscales, as well as Activity Hours, Age, Household, and Exercise.
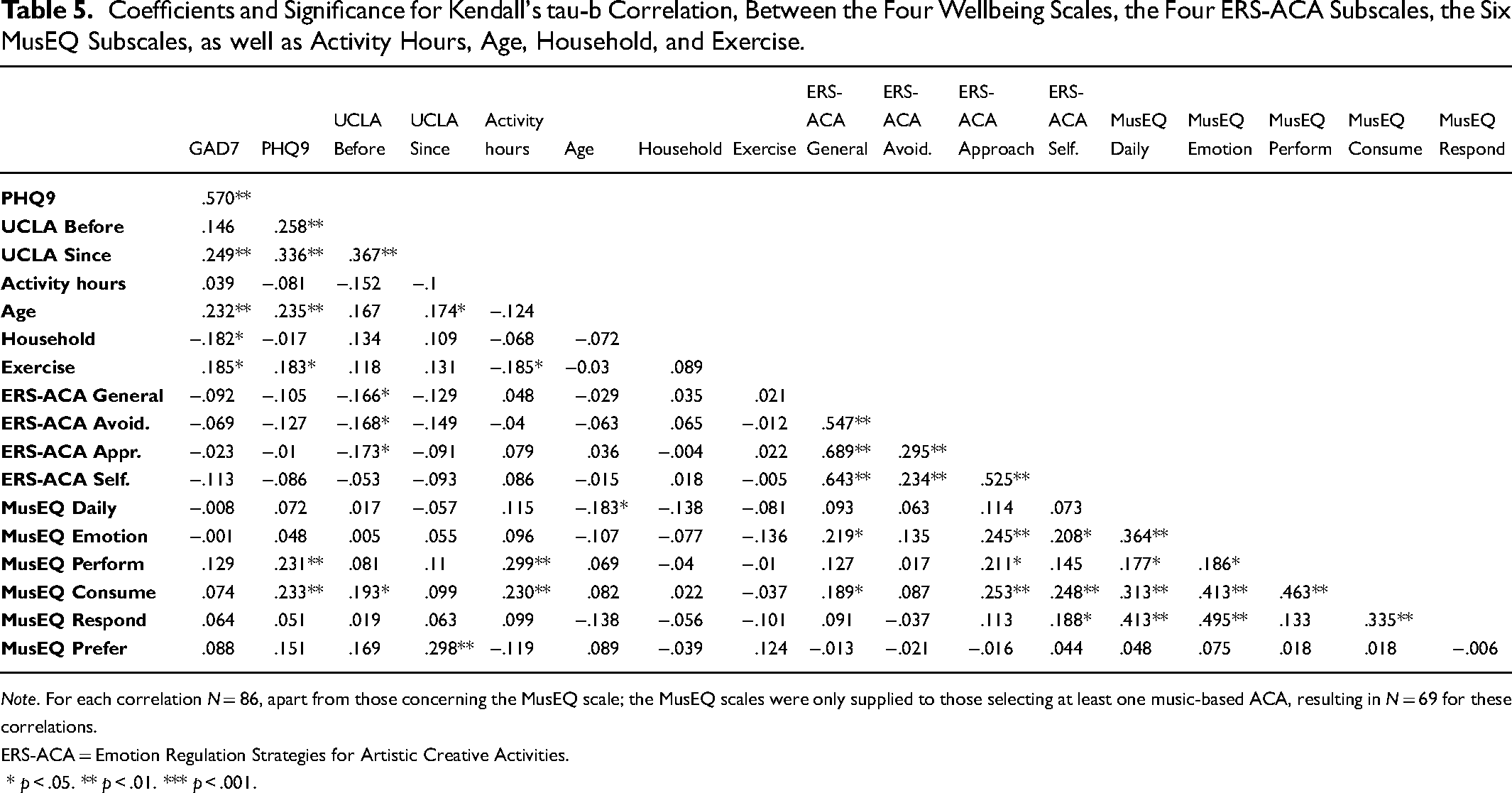
Note. For each correlation N = 86, apart from those concerning the MusEQ scale; the MusEQ scales were only supplied to those selecting at least one music-based ACA, resulting in N = 69 for these correlations.
ERS-ACA = Emotion Regulation Strategies for Artistic Creative Activities.
* p < .05. ** p < .01. *** p < .001.
As shown in Table 5, five of the six comparisons between the four mental health and wellbeing scales produced significant, positive relationships, with coefficients ranging from .249 to .570, and all of which were significant at p < .01. The only non-significant comparison between mental health and wellbeing scales occurred between the GAD7 and UCLA Before scales (r = .146, p > .05). This outcome indicates that overall, these four mental health and wellbeing scales were well-matched. Age produced a significant, positive relationship with three of the four mental health and wellbeing scales. This indicates that older participants were feeling less anxious, depressed, and lonely during COVID-19, in concert with the findings of Kiernan, Chmiel, Garrido et al. (2021) as well as numerous other studies around the world (e.g., Bu et al., 2020; Chmiel et al., 2022; Czeisler et al., 2021; Fisher et al., 2021; Rossell et al., 2021). There are several possible explanations for this, such as the likelihood of lower job security for younger participants, thereby leading to heightened concern, as well as younger participants placing greater importance on socialization (Leung et al., 2022). Additional mixed-method examination may help shed further light on this interaction. Moreover, as the UCLA Before scale was the only mental health and wellbeing scale that did not produce a significant relationship with age, this suggests that this interaction with age was less pronounced prior to the pandemic.
Household size produced one significant, negative coefficient, which occurred with GAD7. This indicates that those in larger households reported feeling more anxious than those in smaller households; although considering only one significant coefficient was observed, we suggest that household size is not a particularly useful predictive variable in this study. Additionally, exercise undertaken produced a significant, positive relationship with both GAD7 and PHQ9, indicating that those exercising more also reported less anxiety and depression. This finding is in line with other studies focusing on exercise and mental health (e.g., Chmiel et al., 2022; Colley et al., 2020; Coyle et al., 2021; Faulkner et al., 2021), as well as the findings of Kiernan, Chmiel, Garrido et al. (2021), although importantly, we cannot infer causality in this relationship. Exercise was also negatively correlated with Activity hours, showing that participants exercising more than they had before COVID-19 devoted less time to ACAs per week and similarly that those devoting more time to ACAs were exercising less than they had prior to COVID-19.
Activity hours was not significantly correlated with any of the mental health and wellbeing scales, and neither were the majority of the ERS-ACA subscales. The exception here was that three of the ERS-ACA subscales produced a significant negative relationship with the UCLA Before scale, with the Self-development subscale producing the only non-significant result. This suggests that before the COVID-19 pandemic, our participants were using Avoidance strategies (e.g., distraction, suppression, and detachment) and Approach strategies (e.g., acceptance, reappraisal, and problem-solving) significantly less than they were during COVID-19. Yet of 24 potential relationships between the mental health and wellbeing scales and the MusEQ subscales, only four were significant, with no clear pattern emerging between these.
RQ5: Comparison Between Argentinian and Australian Data
Finally, we compare responses for the ERS-ACA and MusEQ scales between the present Argentinian sample (N = 86) and the Australian sample (N = 653) reported by Kiernan, Chmiel, Garrido et al. (2021); as reported in Chmiel et al. (2022), the majority of these Australian participants (68.3%) were from Victoria, for which Melbourne is the most populous city. Bayesian modeling was chosen to analyze the data due to the substantial differences in sample sizes between the Argentinian and Australian participants. Bayesian modeling was performed using the brms package for R (Bürkner, 2017). For each model, a separate ERS-ACA or MusEQ subscale was used as the dependent variable, and country was used as the independent variable. Bayesian modeling produces an evidence ratio; given that no directional hypotheses were attached to RQ5, we consider an evidence ratio greater than 39 to be strong, which is loosely analogous to a two-tailed p-value below .05 (Makowski et al., 2019). We provide additional information and references for interpreting Bayesian evidence ratios within the Supplemental Material.
Ratings for each ERS-ACA and MusEQ scale, split by country, are plotted in Supplemental Figures 1 and 2, respectively. Additionally, evidence ratios for each Bayesian model are reported in Supplemental Table 3. All four of the ERS-ACA Bayesian models produced strong evidence (evidence ratio > 39) that Australian and Argentinian participants were rating their emotional regulation strategies at different levels to each other. Upon closer investigation of Supplemental Figure 1, Argentinian participants rated each ERS-ACA subscale lower than the Australian participants. As with the Australian data, the Argentinian participants rated Avoidance as the most prevalent, indicating that in both countries, ACAs were more likely to be used as an avoidance strategy (e.g., for distraction or escapism) rather than as an approach-based or self-development-based emotion regulation strategy. As noted above, these findings regarding the prevalence of Avoidance strategies during COVID-19 lockdown are in concert with findings reported by Drake et al. (2022), for which more than 90% of participants resided in the USA.
When comparing general trends of mean ERS-ACA values, both Australia and Argentina produced similar trends for the three subscales: General factor, Avoidance, and Approach subscales (see Supplemental Figure 1). However, the primary difference between the two countries was that Argentinian participants rated the Self-development subscale lower (relative to the other subscales) than Australian participants did. This finding suggests that Argentinians were less likely than Australians to engage in ACAs as a self-development strategy (e.g., as a way of reaffirming a sense of self) during the 2020 lockdown period.
When examining the Bayesian models for the six MusEQ subscales, five models showed little to no evidence of a difference in ratings between the Argentinian and Australian participants (as shown in Supplemental Table 3, evidence ratios ranged from 0.99 to 9.61; also depicted in Supplemental Figure 2). However, the model concerning the Perform subscale provided strong evidence (evidence ratio of 3999) that Argentinian participants rated this subscale higher than Australian participants did. Thus, the Argentinian participants were more likely to engage in musical activities which lead individuals to become known to others as a ‘musical’ person, or, in other words, which involve the performance of a musical identity. Broadly, this supports the earlier findings of Moore and Baker (2009), which showed how powerful music was in familial and broader social identity formation for Argentinians living within Australia.
Discussion and Conclusion
This paper examined the role of ACAs in regulating emotion and supporting the mental health and wellbeing of Argentinians during the 2020 COVID-19 lockdowns and investigated potential similarities and differences between Australian and Argentinian populations in this regard. Comparison with Australia was made by drawing on a similar, existing study (Kiernan, Chmiel, Garrido et al., 2021), with Australia chosen as a suitable country for comparison due to both countries experiencing extended periods of lockdown throughout 2020.
We observed clear similarities in the ways that Argentinians and Australians used ACAs for emotion regulation. Most notably, in both countries, ACAs were primarily used for avoidance-based emotion regulation rather than for self-development-based or approach-based emotion regulation. Similarly, in both countries, music was primarily used for the purpose of emotion regulation than for other purposes, and music-based ACAs tended to be frequently engaged in during the lockdown period. Indeed, when these findings are considered alongside those recently reported by Drake et al. (2022), an overarching commonality emerges regarding how people engaged in ACAs during the COVID-19 lockdown periods. That is, for these three studies occurring within periods of COVID-19 lockdown across targeted areas within three separate continents (South America, North America, and Australia), there was a tendency toward avoidance-based emotion regulation and a tendency for people to turn to music-based ACAs to maintain or improve their mental health and wellbeing. Given the similar findings reported by Granot et al. (2021) across the Americas, Asia, Europe, and the UK (albeit being termed as “diversion from the crisis”), music appears to be an important and somewhat universal tool for support in such times.
It is also worth noting that while the top 5 ACAs for helping Argentinians “feeling better” during the pandemic were all musical in nature (“composing music,” “rehearsing in plays/drama/opera/musicals,” “playing a musical instrument,” “listening to music,” and “singing”), the ACA “listening to music” was ranked fourth, while in Australia (Kiernan, Chmiel, Garrido et al., 2021) and the USA (Drake et al., 2022), music listening was ranked first. The current study builds on this previous research by providing evidence from a third continent (South America) of specifically musical ACAs, and music listening in particular, being ranked as highly effective at helping people “feel better” during a pandemic crisis, and that, as noted above, this process occurs by way of avoidance-based emotion regulation, regardless of cultural differences between participants in Australia, North America, and South America and seemingly also in other countries. These findings also support previous research which has shown that different types of situation can inform the type of emotion regulation strategy deployed, with low-intensity stimuli leading to a tendency toward reappraisal strategies on the one hand and high-intensity stimuli (such as a global pandemic) leading to a tendency toward distraction or avoidance-based strategies on the other hand (e.g., Sheppes et al., 2014).
In contrast to the music-based ACAs, both Argentinian and Australian participants listed “watching films or TV shows” approximately halfway down the list regarding ACAs that made them “feel better.” This reinforces the notion (see, e.g., Kiernan, Chmiel & Davidson, 2021) that this ACA was perhaps prevalent simply due to the ease of undertaking it at home and that many other ACAs (and especially music-based ACAs) are more beneficial in supporting overall wellbeing during a pandemic lockdown. These findings also further support age and exercise as robust predictors of mental health and wellbeing (e.g., Bu et al., 2020; Chmiel et al., 2022; Colley et al., 2020; Coyle et al., 2021; Rossell et al., 2021).
Participants in both Argentina and Australia listed “watching films or TV shows” as their most undertaken ACA and “listening to music” as their second most undertaken ACA, and “cookery or baking” remained in the top 5 for both countries. But while Australians were more likely to read, do gardening, or paint or draw, Argentinian participants were more likely to play a musical instrument, play video games, or sing. Moreover, Australian participants were far less likely than Argentinians to play a musical instrument or sing, listing these ACAs as the 11th and 13th most frequently undertaken ACAs during this time. This finding supports the above-suggested idea that Argentinians may have placed more cultural importance on active music-making than Australians did during the pandemic, which in turn sheds some cursory light on cultural differences in the pandemic response. It is also noteworthy that these findings contrast with those of Elisondo (2021) in which musical activities did not feature among the five most frequently undertaken ACAs by Argentinian participants, a difference that may perhaps be explained by the fact that participants in Elisondo's (2021) study were residents of the province of Córdoba, whereas the current study targeted people living in the greater Buenos Aires region. Further consideration of this difference would be warranted in future studies.
While this study also examined reported levels of loneliness as one indicator of mental health and wellbeing among study participants, future studies could dedicate greater attention to the question of how engagement in ACAs may specifically help to address loneliness. Associations between loneliness and poor mental and physical health outcomes are well established (Hawkley & Cacioppo, 2010), and the COVID-19 pandemic and its associated lockdowns have drawn attention to loneliness and social isolation as broader social and public health issues (Smith & Lim, 2020). Indeed, the prevalence of loneliness has itself been described as a “modern epidemic” (Jeste et al., 2020). Future studies would do well to build on the growing body of literature outlining the various ways that arts and music engagement have supported people during the socially isolating conditions of pandemic lockdown to explore how the arts and music may potentially support the mental and physical health of people experiencing loneliness and/or social isolation in everyday life.
These findings provide insights into the links between engagement with ACAs and mental health and wellbeing during times of crisis; however, it must be stated that these data were self-reported in a semi-reflective manner. That is, while participants were reporting on their own experiences while living in periods of lockdown, much of this was based on their memories of the past weeks, as distinct from a study in which longitudinal data were collected via consecutive surveys or activity diaries. This approach may have had an impact on the accuracy of data reported, and so future work should aim to track such reports across a period of weeks.
Additionally, despite the fact that the present study was able to replicate many of the findings of Kiernan, Chmiel, Garrido et al. (2021), the findings also suggest that the survey could have benefitted from increased clarity in the wording that was used. Argentinians ranked “listening to music” as both the most undertaken ACA as well as the fourth most ceased ACA. While “listening to music” was intended to encompass any kind of music listening (including on portable devices using headphones or home sound systems), it could have also been interpreted as meaning live music attendance specifically (although this was not the intention). The same cause may explain why “playing a musical instrument” was listed as both the third most undertaken and ceased ACA for Argentinians, many of whom may have been referring to stopping performances at shows (which was intended to be captured by a separate listed ACA). Similarly, while “watching films or TV shows” was the most prevalent ACA in both countries, this ACA also ranked in the top 6 ceased ACAs for both countries. It is therefore possible that this ACA unintentionally captured responses concerning public cinema-watching as well as the intended activity of in-home viewing. While the intention of this study was to capture engagement with cinematic television, it is also possible that some participants may have included non-cinematic television engagement (e.g., with news and weather updates) in their responses. Future studies should take these limitations into account and draw clearer distinctions between public and home-based ACAs, as well as cinematic and non-cinematic television.
We conclude that ACAs play an important role in supporting mental health and wellbeing for many people around the world in times of crisis and that, regardless of the myriad of social and cultural differences across continents, similarities do exist in the ways people have used music and the arts to respond to the pandemic. Namely, music—and especially music listening—has been identified in this case as consistently effective at helping people in Australia and Argentina to “feel better,” and avoidance-based emotion regulation has been identified as the most common emotion regulation strategy in each context. During 2020, Argentinians appear to have placed a particular emphasis on music-based ACAs such as composing music, rehearsing or performing in plays, dramas, and operas, playing musical instruments, listening to music, and singing. Given these results, it is crucial that future planners and policy makers in Argentina explore how these music-based ACAs can be adapted safely to suit extreme scenarios such as a pandemic in order to support mental health and wellbeing in such contexts.
Supplemental Material
sj-pdf-1-art-10.1177_02762374231196083 - Supplemental material for Musical Activity as Avoidance-Based Emotion Regulation During the COVID-19 Pandemic: Evidence Across Continents
Supplemental material, sj-pdf-1-art-10.1177_02762374231196083 for Musical Activity as Avoidance-Based Emotion Regulation During the COVID-19 Pandemic: Evidence Across Continents by Anthony Chmiel, Frederic Kiernan, Hernán D. Ramallo, and Jane W. Davidson in Empirical Studies of the Arts
Footnotes
Acknowledgments
The authors would like to acknowledge the important contribution of co-author Hernán D. Ramallo, who, sadly, passed away prior to the completion of this work. This research paper is dedicated to his memory.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Creativity and Wellbeing Hallmark Research Initiative at the University of Melbourne (Grant holder JD).
Data availability
The raw data supporting the conclusions of this article will be made available by the authors upon request, without undue reservation.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.