
Abstract
Quantitative studies in marketing are dominated by variance-based approaches. These have limitations for understanding macromarketing outcomes that often derive from different combinations of causal conditions, and where factors productive of the same outcome may be different from those impeding it. In this paper we draw on set-theoretic theory and propose qualitative comparative analysis (QCA) as an analytical method able to complement and extend macromarketing research programs. Fuzzy-set QCA is used to explore combinations of conditions influencing COVID vaccine adoption, with readers provided with detailed guidance through the process and current best practices. We consider a number of important but often neglected issues in fuzzy-set QCA; outlining how to conduct robustness checks, appropriateness of a two-step approach, identifying individual cases with specific conditions for further analysis, and examining the problems and opportunities provided by irrelevant cases and contradictions. A summary of macromarketing issues that may benefit from QCA, and recommended practices for conducting a QCA, are provided.
Keywords
Introduction
As marketing problems become increasingly complex, diversity in research methods produces a more robust understanding of marketing phenomena (Tellis, Chandy, and Ackerman 1999). However, the marketing discipline is repeatedly criticized for the limited diversity of its research methods (Davis et al. 2013), which circumscribes research and other scientific inquiry (Hunt 2002). This paper contends that qualitative comparative analysis (QCA) (Ragin 1987, 2008) holds much potential for future macromarketing research, and provides an overview of the approach, best practices and an empirical application. QCA enables investigation of combinations of conditions or characteristics leading to an outcome and its negation, rather than net-effects; allows for complex interactions and several alternatives to achieve the same end, and is able to complement and extend research programs (Roig-Tierno, Gonzalez-Cruz, and Llopis-Martinez 2017).
Macromarketing is concerned with the intersections between society and marketing, and often involves complex stakeholder relationships and the need to consider many variables simultaneously. Quantitative studies in the field can produce contradictory results (e.g., Abrahamse et al. 2005; Waechter, Sütterlin, and Siegrist 2015). Chatzidakis and Lee (2012) argue that there are important differences between phenomena of negation (reasons against) and affirmation (reasons for) consumption. Asking consumers what matters also may not reflect what they choose (Mueller, Lockshin, and Louviere 2010). QCA can accommodate and address these issues, and consequently our understanding of many macromarketing phenomena could benefit from such an approach. Despite its appeal, QCA is at an early stage of adoption in business and management (Berger 2016), with a search of past issues of the Journal of Macromarketing highlighting an absence of articles using the QCA methodology.
The study had three major objectives. First, to illustrate how macromarketing research can benefit from QCA, and to provide an overview of the method. Second, to provide an original application in a macromarketing context, here focusing on identifying optimal combinations of conditions influencing COVID vaccine acceptance; to highlight the recommended process for conducting and reporting the QCA; common problems and solutions, and recent methodological developments. Third, to call attention to areas of macromarketing that would be highly suitable for QCA. The paper intends to act as a reference for macromarketing researchers who want to conduct a QCA. To support this goal, a summary of recommended practices for conducting a QCA is provided in the Appendix to this paper.
This research responds to calls for macromarketers to further develop their analytic skills with which to explore macromarketing phenomena (Fisk 2006); applications of the method in marketing in general (Berger 2016; Pappas and Woodside 2021) and in macromarketing specifically (Brychkov, Domegan, and McHugh 2022). While there are recent tutorials providing excellent guidelines for performing QCA (Pappas and Woodside 2021; Russo and Confente 2019), these authors neglect a number of critical issues and developments important for good practice. These include conditions influencing the non-outcome (Schneider and Wagemann 2012), advances in robustness testing (Wu et al. 2021), contradictions, irrelevant cases and false positives (Rubinson 2013; Schwellnus 2013); the two-step QCA approach, and how identification of individual cases exhibiting specific conditions delineating an outcome can be used for segmentation, communications and public policy development.
An overview of the QCA method and its three variants, conditions supporting its use, and relevant applications in marketing follow. The study context, research design and method is then presented, followed by a step-by-step process for conducting QCA, using COVID vaccine intentions, focusing on key decisions to be made and results presentation. The paper concludes with explanations and interpretations of the findings, some theoretical and methodological contributions, managerial and practical implications, future research directions and some limitations.
Set Theory and Qualitative Comparative Analysis
QCA is an asymmetric data analysis technique that transcends some of the limitations of conventional quantitative and qualitative research. This is achieved by combining the rationale of qualitative approaches that are rich in contextual information, with quantitative methods that deal with large numbers of cases and are more generalizable (Pappas and Woodside 2021; Ragin 1987). QCA extends and elaborates set-theoretic principles of social research. Set-theoretic analysis contrasts with conventional quantitative analysis through its focus on calibration versus measurement, configurations of conditions versus ‘independent’ variables, set-theoretic versus correlational connections, and the analysis of causal complexity rather than net effects (Ragin 2008). Set relations in social research involve causal or other integral connections linking social phenomena, are asymmetric (and thus should not be reformulated as correlational arguments), and can be very strong despite relatively modest correlations (Ragin 2008).
QCA is based on two assumptions: (1) change is often the result of a combination of factors, as opposed to any one individual factor; and (2) different combinations of factors can produce similar changes (Ragin 1984). Conventional quantitative techniques are often symmetrical in nature, therefore failing to consider the effects of complex interactions among independent variables. In traditional quantitative analysis, independent variables are seen as analytically separable causes of the outcome, with each variable having an autonomous or independent capacity to influence the level, intensity, or probability of the dependent variable. Effects of the independent variables are both linear and additive, thus the impact of a given independent variable on the dependent variable is assumed to be the same, regardless of the values of the other independent variables. The assumptions of additivity and linearity in regression analysis allow the estimation of outcomes regardless of whether there are cases existing that have the values of the independent variables. The net-effects approach of regression analysis addresses the problem of limited diversity by assuming that a linear relationship can be extrapolated beyond an observed range of values and is dependent upon model specification, with the estimate of an independent variable's effect highly determined by its correlations with competing variables.
A set-theoretic approach differs from conventional quantitative variable-based methods in that it does not disaggregate cases into independent, analytically separate aspects but instead treats configurations as different types of cases (Fiss 2011). This calls for modifications to the level of analysis and aggregation of data from the micro-level of individual cases to the macro-level, thus allowing quantitative data to be analyzed with a more case-based approach. Testing for contrarian cases, and examining cases in the sample that are not explained by the main effects, is typically absent in traditional quantitative analyses. However, QCA enables the analysis of complex causation, in which an outcome may follow from several different combinations of causal conditions, the principle of equifinality (Ragin 2008). The disaggregated subset relations provide important information about how social phenomena are connected, in particular in macromarketing studies where the conditions that are impediments to a particular outcome are often not the same as the conditions that are productive of that same outcome (Chatzidakis and Lee 2012). The asymmetry of set-theoretic analysis thus makes it possible, in this study, to examine whether different configurations of causally relevant conditions influenced COVID vaccine adoption and non-adoption.
QCA has three main variations: crisp set QCA (csQCA), multi-value QCA (mvQCA) and fuzzy-set QCA (fsQCA). While csQCA requires binary variables and mvQCA treats variables as multi-valued rather than dichotomous (Cronqvist 2004), fsQCA is considered more useful for marketing research applications due to its ability to better capture the complexity in cases that naturally vary by level or degree and are thus measured utilizing ordinal or interval scales (Ragin 2000; Rihoux and Ragin 2009). fsQCA is typically considered preferable to mvQCA (Cronqvist 2004) because multivalue sets tend to exacerbate the problem of limited diversity (see Rihoux and Ragin 2009).
Fuzzy set QCA makes set-theoretic analysis possible, while retaining fine-grained empirical generalizations. Since some variables will be inherently categorical in nature, another advantage of fsQCA is its ability to incorporate both crisp-set causal conditions along with fuzzy-set causal conditions, thus providing further flexibility of analytical techniques. The fsQCA procedure provides a bridge between fuzzy sets and conventional truth table analysis by constructing a Boolean truth table summarizing the results of multiple fuzzy-set analyses. Fuzzy membership scores (i.e., the varying degree to which cases belong to sets) combine qualitative and quantitative assessments. It is preferable to utilize fuzzy sets to calibrate degree of membership in sets and thereby avert what may be arbitrary choices when researchers are required in csQCA to specify breakpoints when dichotomizing interval and ratio-scaled variables, avoiding lost information and allowing a more nuanced analysis.
With fuzzy sets, it is mathematically possible for a causal condition or causal combination to be a subset of both an outcome (e.g., adopting COVID vaccination) and the negation of the outcome (e.g., not adopting COVID vaccination). No mathematical reason exists to expect consistency scores calculated for the negation of an outcome to be perfectly negatively correlated with consistency scores for the original outcome, as they are in crisp-set analyses (Ragin 2008). fsQCA also provides a higher standard of set-theoretic consistency than csQCA does. It is therefore strongly recommended that the use of crisp-sets be reserved only for phenomena that are categorical in nature (Ragin 2008).
Fuzzy-set QCA has been used in contexts as diverse as green buying behavior (Gonçalves, Ferreira, and Silva 2016), climate change strategies (Llopis-Albert, Palacios-Marqués, and Simón-Moya 2021), policy and practice divergence (Crilly, Zollo, and Hansen 2021), strategic typologies (Fiss 2011), educational poverty (Glaesser 2021) and health care practices (Thygeson et al. 2012). While QCA can complement variance-based approaches (Pappas and Woodside 2021), fsQCA has been found to offer richer insights and stronger explanatory power than cluster analysis, which also fails to reveal complex trade-offs (Ordanini, Parasuraman, and Rubera 2014), detect associations and identify relationships that regression analysis has been unable to do (Thygeson et al. 2012), and is considered to perform better than chi-squared automatic interaction detection (CHAID) in identifying causal configurations (Woodside 2015). In addition, fsQCA is employable on different sample sizes ranging from very small (e.g., fewer than fifty cases) to very large (e.g., thousands of cases) and is not sensitive to outliers (Pappas and Woodside 2021). QCA provides explanations without dismissing ‘exceptions’ or ‘outliers,’ which often shed light on the understanding of specific processes (Berg-Schlosser et al. 2009).
A Macromarketing Application of QCA: COVID Vaccine Acceptance
Studies conducted in the field of macromarketing consider the interaction between markets, marketing and society. This is ideally suited for understanding the complex issue of vaccine uptake. Akaka et al. (2023) argue that tackling social problems requires a macro approach that considers the multifaceted interactions of individual and collective perspectives. They position vaccine uptake having implications across multiple systems, including vaccine administration and distribution through to sociocultural and political imperatives. While this paper focuses specifically on vaccine uptake, it is within the larger field of social issues aimed at improving human wellbeing and fairness, part of the new era of macromarketing (Hunt, Hass, and Manis 2021).
The Study Context
This study examines COVID vaccine intentions in the United States. Reduction of the impact of COVID-19 depends on the actions of individuals to engage in socially responsible behaviors, including the uptake of vaccines which is the most important and effective tool for limiting the spread of the virus (DeRoo, Pudalov, and Fu 2020). Vaccines have been one of the most successful public health measures in history, resulting in the decline and even elimination of a number of infectious diseases (Delany, Rappuoli, and De Gregorio 2014). To be successful, vaccine programs need a high level of involvement across societies, offering direct protection to those vaccinated and indirectly protecting the unvaccinated through herd immunity (Fine, Eames, and Heymann 2011). While they have been a successful public health measure, demonstrated in the huge drops in incidence of diseases such as measles and polio across most of the world, a lack of confidence or belief in vaccines among some members of society represents a sizable threat to the future success of these programs (Omer et al. 2009; WHO 2020). Vaccine hesitancy is identified by the World Health Organization as one of the greatest threats to global heath, with immunization coverage to fight communicable diseases critical to the United Nations sustainable development goal of good health and well-being.
Factors Influencing Vaccine Intentions
Extant theory, and where possible in-depth knowledge of the cases, should be used to determine which factors (also termed ‘conditions’) are the most important and should be considered. Configuration theory implies that multiple factors combine to explain a result, and there should be an inherent logic or cohesiveness between the conditions (Miller 1987). QCA examines all possible combinations of factors, with each additional factor increasing the number of combinations exponentially. Using a large number of factors is not desirable (Misangyi et al. 2017), with a QCA involving more than 8-10 factors likely to be intractable (Greckhamer, Misangyi, and Fiss 2013) and exacerbate the problem of limited diversity.
We draw upon the work of Van Bavel et al. (2020), which argues that a social and behavioral science perspective is required to support the efforts of medical experts to ensure vaccine uptake. Their paper focuses on the importance of managing threat and risk perceptions, understanding the role of trust in government and belief in science communication, and incorporating the social context, including social norms, in-group influences and culture. The framework developed by Van Bavel et al. (2020) informed this research by focusing on conditions that may not have been extensively researched in relation to vaccines but which have been more broadly considered in social marketing, in relation to issues such as climate change, drink driving, smoking and opioid use (Lee and Kotler 2019; Lefebvre 2013). Our research specifically investigates the impact of pandemic severity perceptions, belief in science, trust in government, communal orientation, psychological reactance, religiosity and personal knowledge.
Pandemic Severity. Pandemic severity refers to the negative consequences an individual associates with an event or outcome. At the beginning of the pandemic, it was unknown how severe or contagious the COVID-19 virus would be. When people calculate the potential impact a virus could have on them, they consider the level of risk, disease transmissibility and severity (Smith 2006). Fear of the unknown, especially regarding a pandemic, can be a powerful motivator as it works to magnify the perceived severity of a threat (Rogers 1983).
Risk perceptions are key considerations when assessing people's health behavior (Ferrer and Klein 2015). In the Health Belief Model, severity is an example of negative utility and valence which influences the uptake of prevention strategies (Hochbaum 1958). Perceived severity is part of the threat perceptions in the Protection Motivation Theory and Extended Parallel Process Model. Meta-analysis supports the role of risk propensity in health behavior change, with increased worry and risk perceptions related to greater use of preventative behavior strategies (Hay, McCaul, and Magnan 2006; Sheeran, Harris, and Epton 2014).
While risk perceptions are found often to have a positive impact on preventative behavior, research on negative social behaviors, such as drinking and smoking, suggests that in some cases when people weigh up a health risk, particularly the severity of outcomes, they can be optimistically biased in their calculations (Klein and Weinstein 1997; Wolburg 2009). People can evaluate the chance of contracting a disease, for example, to be higher for others than for themselves, which increases their propensity to ignore or misinterpret information, underestimate the risk and not take appropriate action to protect themselves (Sharot 2011).
Belief in Science. Vaccine uptake requires an acceptance of public health initiatives and the science behind it. When an issue is complex, people tend to make decisions based on heuristics as opposed to investigating the evidence (Lewandowsky, Gignac, and Vaughan 2013). A belief in science is stronger when the source is seen as trustworthy and there is perceived consensus among scientists (Hornsey et al. 2016). Research has found that the most effective way to increase vaccination rates is through the recommendations of medical professionals (Sabin-Aspen Vaccine Science and Policy Group 2020) as Americans have a high level of trust in medical scientists (Funk et al. 2019) and they are seen as the most trusted source of information on COVID-19 vaccines (Machingaidze and Wiysonge 2021). Opinion polling conducted in November 2020 by Pew Research, just prior to data collection for this study, indicated that eighty-five percent of Americans had at least a fair amount of trust in medical scientists (Kennedy, Tyson, and Funk 2022). However, over the course of the pandemic these numbers have dropped by about ten percent (Kennedy, Tyson, and Funk 2022; Tyson and Funk 2022), this being partly attributed to changing medical guidance on how to limit the spread of the virus.
Skepticism toward science can have a negative impact on peoples’ assessment of the perceived value of public health initiatives. Skepticism has been found to determine peoples’ lack of compliance with COVID initiatives, as skeptics are less likely than others to accept the motivation behind science-based public policies (Brzezinski et al. 2020) and are less likely than others to engage with scientific information that contradicts their existing beliefs (Lewandowsky, Gignac, and Oberauer 2013) – which are often informed by less information and/or selective information seeking (Pennycook et al. 2020; Uscinski et al. 2020). Skepticism has been found to have negative impacts on COVID stay-at-home orders (Brzezinski et al. 2020), and vaccine uptake (Jolley and Douglas 2014).
Distrust in science is also not simply an issue of education (Uscinski et al. 2020) as often the most highly educated in a social group are the most skeptical (Gauchat 2012). Larson (2020) argues that simply giving more or better information will not be enough in a climate of misinformation and distrust. Understanding people's perceptions of science will help determine the most appropriate source of information (Brzezinski et al. 2020) and the strategies needed to rebut misinformation (Schmid and Betsch 2019).
Trust in Government. Trust in government officials is necessary for them to advocate effectively for pandemic measures, and for people to comply. Greater social trust and confidence in the government's motivations and their competence leads to a higher propensity for people to cooperate (Twyman, Harvey, and Harries 2008). Greater trust in government is associated with more positive vaccine intentions amongst their constituents (Larson et al. 2018). Trust is delicate and, once damaged, can be hard to repair, which is why the level of trust in government can differ depending on race, age and institution type (Jamison, Quinn, and Freimuth 2019). Distrust in elites and fears of being controlled by the government during a pandemic can drive vaccine dissent (Larson 2020). Low levels of trust in public officials in the United Kingdom was found to be associated with low COVID-19 vaccination rates, especially among minority groups (Chaudhuri et al. 2022). One explanation is that a lack of trust in authorities can result in people reinterpreting vaccine information (Yaqub et al. 2014). Evaluations of US government local and state officials’ effectiveness have decreased throughout the pandemic (Tyson and Funk 2022). Trust in the federal government is at near historic lows, with only about one quarter of Americans saying they trust the government in Washington to do what is right ‘just about always’ or ‘most of the time’ (Pew Research 2022).
Communal Orientation. Successful vaccination programs require a significant proportion of the population to participate, which necessitates a willingness for people to get vaccinated for both their own protection and the benefit of others (Fine, Eames, and Heymann 2011). People with a high communal orientation have a desire to assist others, with people putting the needs of others first without an expectation of equal return (Hepburn and Enns 2013). Within a communal orientation Cannon and Rucker (2020) identify two distinct motivations – the need to nurture or care for others and the desire to maintain connections and relationships.
In neoliberal economies, people are perceived as individuals acting in their own self-interest. America is highly individualistic (Hofstede Insights 2022), and reporting on the pandemic has often focused on individuals engaged in competitive and selfish behavior, such as panic buying. However, previous research into mass panic during a crisis has found this type of behavior to be rare, and if it does occur, it is often short-lived or demonstrated by only a small number of individuals (Jones et al. 2006). When a disaster happens, overwhelmingly, the research finds that people are much more likely to co-operate than to compete. Evidence suggests that supportive behaviors are widespread; helping being the most observed behavior (Grimm et al. 2014). Drury (2018) argues that the shared experience of a crisis leads to a shared social identity resulting in subsequent concern for others. Support for this type of behavior is found in social communication campaigns that emphasize ‘us’ as a collective and the impact individual behavior has on others (Van Bavel et al. 2020).
Psychological Reactance. Psychological reactance is caused by the notion that people value freedom, choice and autonomy. Reactance occurs whenever individuals no longer feel free “to hold their particular attitudes, to change their attitudes, or to avoid committing to any position” (Silvia 2006, p. 673). Psychological reactance theory posits that any attempt to change or control someone's current attitude or behavior may be perceived as a threat and may arouse motivation to avoid exposure to the effort altogether, to reject the advocacy, or result in a boomerang effect (e.g., refusing a COVID vaccination after exposure to pro vaccination messaging) (Brehm 1966; Dillard and Shen 2005). Restoration of threatened and lost freedom can occur indirectly by discrediting the message source (LaVoie et al. 2017) and evoke counterproductive psychological responses in people for whom the threatening messages are personally relevant (Bartikowski, Laroche, and Richard 2019) such as rejecting existence of the threat (e.g., by denying that COVID is a significant problem). Studies of this phenomenon demonstrate consistently that high threat situations cause reactance and subsequently reduce persuasion (Rains 2013) and that individuals are also likely to vary in their trait propensity to experience reactance (Shen and Dillard 2005).
There are numerous applications of psychological reactance theory in health communication (see Reynolds-Tylus 2019 for a review). Psychological reactance is often considered a contributing factor when public health campaigns and behavioral change strategies fail to produce the desired effect (e.g., Hunter et al. 2013; Wilde 1993) or produce results directly at odds with their intent (e.g., Pham, Mandel, and Morales 2016; Sieverding, Specht, and Agines 2019). Perceptions of limiting freedoms or control may induce non-adherence with prescribed treatments (Fogarty and Youngs 2000; Moore, Sellwood, and Stirling 2000) with various recommendations to obtain a COVID vaccination having the potential to elicit reactance and leading individuals to fail to comply with medical and other advice to get vaccinated.
Religiosity. Seventy-two percent of American adults consider religion ‘very’ or ‘somewhat’ important in their life (Pew Research 2021), and it is considered one of the most deep rooted of human behaviors (Bentzen 2021). Agarwala, Mishra, and Singh (2018) highlight a substantial literature that finds religiosity significantly impacts attitudes, values and actions. Religiosity plays a crucial role in lowering people's acceptance of opinions and values opposed to theirs, and for followers who truly and literally believe in the absolutes of their religion, it would be difficult to accept something that challenges it. Religious consumers are widely considered to be risk-averse, and religiosity is inversely related to positive attitudes toward innovation, new ideas and technologies (e.g., Mansori, Sambasivan, and Md-Sidin 2015).
Individuals with a tendency toward greater religiosity are often found to be more open to following recommendations (Guéguen, Bougeard-Delfosse, and Jacob 2015; Torgler 2006), and report stronger behavioral intentions toward following COVID-19 guidelines (Everett et al. 2020). Religion as an institution promotes social integration through community activities and rituals (Ellison, Burr, and McCall 1997) and involved group members display higher interdependence and collectivistic tendencies (Vandello and Cohen 1999). Religiosity places emphasis on having a greater sense of individual responsibility (Guiso, Sapienza, and Zingales 2003), and many religions value restraint (Lastovicka et al. 1999) and conformity (Ellison 1994). The care and wellbeing of others is important in many religions as emphasized by the teachings of the ‘Good Samaritan’ parable in Christianity and the practice of Ehsan in Islam (Albin Shaikh, Purchase, and Brush 2019).
Religion may also be associated with negative health outcomes and the inappropriate use of health services due to fanaticism, asceticism, mortifications or oppressive traditionalism (Alves et al. 2010; Van Ness 1999). Some religious communities have defied social distancing recommendations and continued to have mass gatherings. In the United States, metropolitan areas with a higher religious density (number of congregations per capita) exhibit less adherence to lockdown directives (DeFranza et al. 2021), and funerals, choir practices and church services have led to superspreader incidents (Aschwanden 2020). When religiosity increases, people perceive greater support from the divine, which can reduce compliance with recommendations from secular authorities (Wu and Cutright 2018). The majority of Americans with religious faith believe to some extent that God will protect them from being infected by COVID (AP-NORC Center for Public Affairs Research 2020).
Personal Knowledge. Individuals change their beliefs in response to experiences (Hogarth and Einhorn 1992). Direct experience affects attitude-formation processes by altering the ways in which available information is processed (Fazio, Zanna, and Cooper 1978). When people have personal knowledge of someone who has contracted COVID-19, they may rely on the availability heuristic to assess the risk of their own exposure (Tversky and Kahneman 1974). Support for vaccination and a belief that vaccines will prevent the illness is increased when people have personal knowledge of the dangers of a disease (Bureau of Sociological Research 2014).
While there is insufficient theory to deductively propose a priori the causal configurations (solutions) here, it is expected that high scores on pandemic severity, belief in science and communal orientation, low scores on psychological reactance, and having personal knowledge of someone with COVID, will be important (core conditions) in many of the solutions found that explain intentions to adopt the COVID vaccine. It also is likely that trust in government and religiosity may be either present or absent (negated) in explaining intentions to vaccinate depending upon how they combine with the other factors.
The use of fsQCA in this study allows for exploration of all possible solutions, comprising the selected conditions, that explain intentions to be vaccinated (or not) for COVID. While specific propositions could be developed regarding exact combinations of the conditions examined, this was beyond the purpose of this study. QCA studies differ in their modes of reasoning and the method is often employed to inductively or exploratively “help the researcher generate some new insights, which may then be taken as a basis for a further theoretical development or for re-examination of existing theories” (Berg-Schlosser et al. 2009, p. 16). Specifying a priori causally complex predictions presents a challenge given marketing's inclination toward a ‘general linear reality’ and net-effects oriented propositions (Delbridge and Fiss 2013). Our final acceptance and hesitancy QCA models included no assumptions about the presence or absence of conditions. We also conducted a necessity analysis beforehand to ensure that there were no necessary conditions for the outcome.
It is considered that solutions are likely to include combinations of the various conditions, including threat perceptions, social context, science communication, individual and collective interests, trust, leadership and coping mechanisms. Causal asymmetry is also expected. For example, since religiosity has equivocal effects on individual behavior, intentions to vaccinate might be achieved for those with high and low religiosity depending on how this factor combines with the other conditions. This gives rise to the following two general propositions:
Development of Study Measures
Multi-item scales are utilized to measure the conditions of interest, with the exception of the single-item vaccine intention measure and dichotomous personal knowledge variable. 1 Religiosity (the degree to which beliefs in specific religious values and ideals are held and practiced by an individual, e.g., Delener 1990) is used rather than religion (religious affiliation or membership) as it is claimed to be a stronger predictor of attitudes and behavior when compared to religious affiliation (see review by Agarwala, Mishra, and Singh 2018). The scales are derived from previous studies where they displayed appropriate psychometric properties. Survey items were pre-tested for interpretability and understanding with a small convenience sample of the target population group including those working in medicine and academia. Only minor changes to item wording were indicated. A full list of measures and their sources is provided in Web Appendix A (see supplementary materials).
Data Collection and Sample Characteristics
The study data are derived from an online survey of five hundred US residents aged 18 or older. Data collection was undertaken and actively managed by Qualtrics and their online panel partners from 9 December 2020 to 7 February 2021, with over 80 percent of responses received before 22 December. 2 Response time, pattern checks and directed queries were used in addition to the standard Qualtrics data quality processes. 3
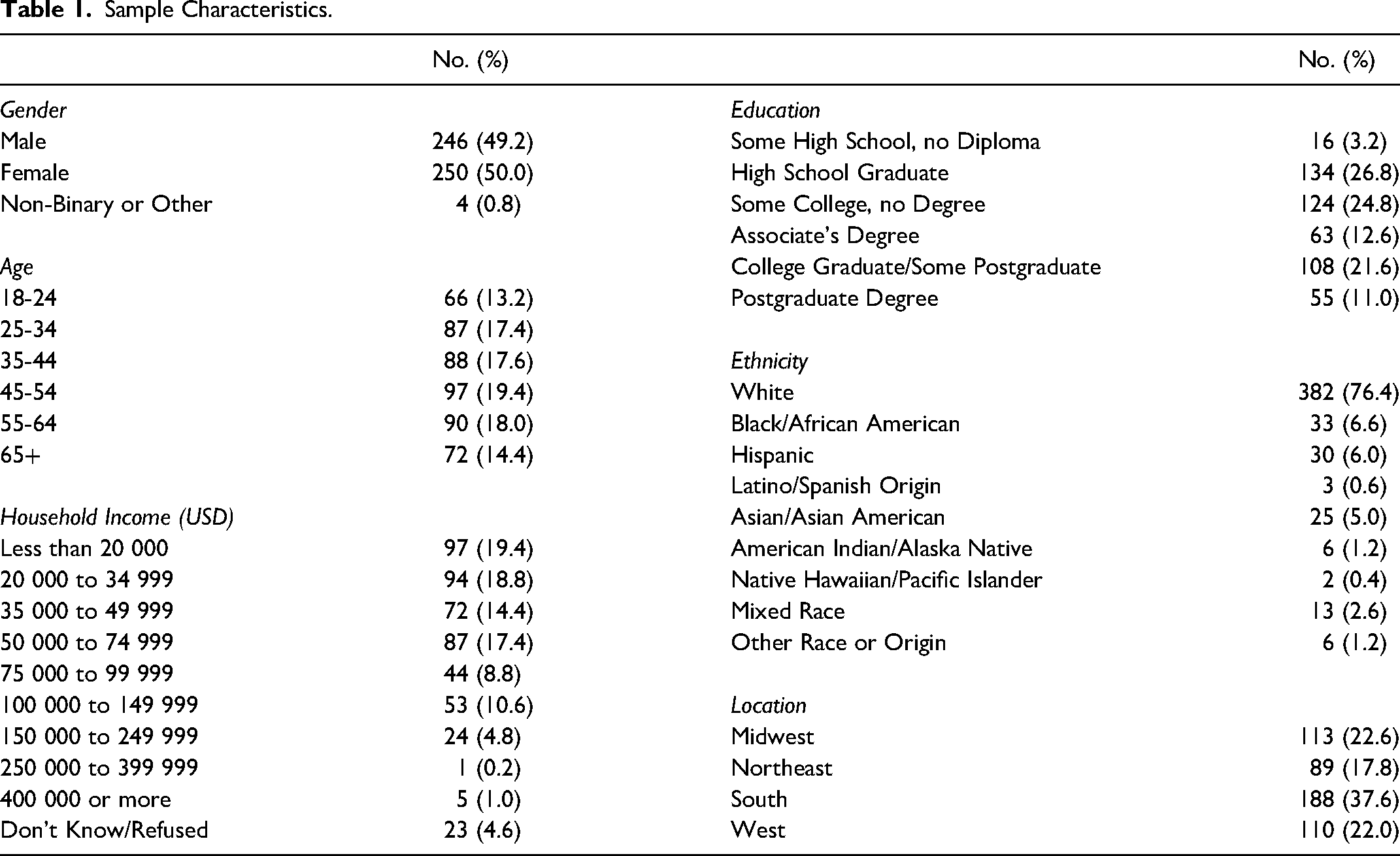
The final sample was nationally representative for gender, age and region. Forty percent of respondents indicated a household income less than USD 35 000, with a third between USD 35 000 and 75 000. Just over half of the sample had a high school diploma only, with forty-five percent holding a college degree. Respondents predominantly described themselves as white Americans (76.4 percent) with between five and seven percent considering themselves either African American, Hispanic or Asian.
Multiple approaches were used to test for common method bias, with findings suggesting this is not a problem here and that the data can be used with some confidence. A full reporting of the techniques used and test results are provided in Web Appendix B. Table 1 presents a breakdown of the sample demographics.
Sample Characteristics.
Measurement Evaluation and Refinement
Measurement development and estimation was performed using the LISREL 9.3 structural equation modeling program. For each of the multi-item scales a one-factor congeneric model was developed. The chi-square statistic, CFI, IFI and SRMR statistics were examined. Although the chi-square tests were significant, the sensitivity of this test to sample size is well known, and it is often recommended to examine other fit indices. The CFI and IFI indices all exceed 0.94, and all SRMRs are below 0.07. Although there is significant literature cautioning against the routine application of stringent cutoff criteria (e.g., Marsh, Hau, and Wen 2004), the discrepancy between the observed variance-covariance and the model implied variance-covariance matrix, and the average of the standardized residuals between the observed and the hypothesized covariance are relatively small, suggesting that the measurement models provide an acceptable description of the data (Tomarken and Waller 2003). Further, the ‘goodness of fit’ statistics of a congeneric model are a type of validity test, since, for the model to fit well, the items must all represent the same latent trait. Further testing indicated the constructs demonstrated acceptable composite and convergent reliability, and discriminant validity. 4 Summated scores from the multi-item scales were used in the QCA. Table 2 provides the correlation matrix and descriptive statistics.
Descriptive Statistics and Correlation Matrix of Study Variables.
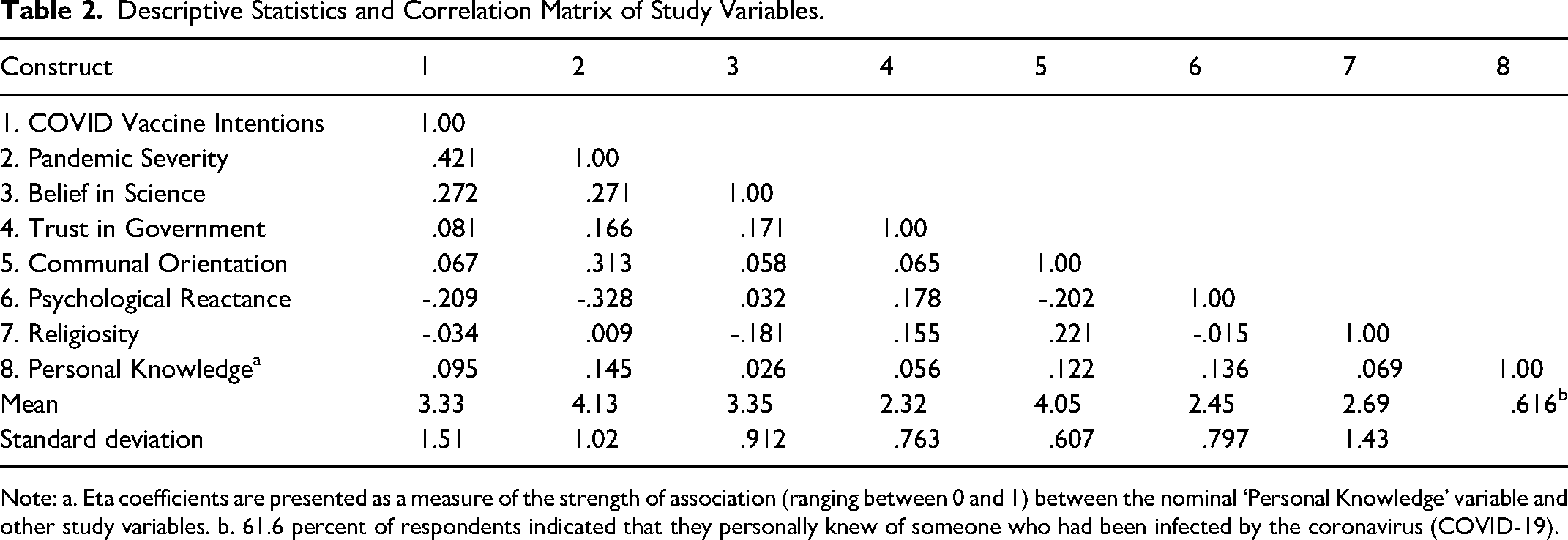
Note: a. Eta coefficients are presented as a measure of the strength of association (ranging between 0 and 1) between the nominal ‘Personal Knowledge’ variable and other study variables. b. 61.6 percent of respondents indicated that they personally knew of someone who had been infected by the coronavirus (COVID-19).
Pre-Analysis Considerations
Along with the standard tests for reliability, validity and common method bias there are a number of additional QCA specific issues that required attention before commencing the analysis. These include examination of contrarian cases, data calibration, choice of software and calibration function, whether to take an inductive, deductive, abductive or combined approach, choice of output solution, selecting raw consistency thresholds for necessity and sufficiency analysis, and the frequency threshold for sufficiency. While this work is more quantitative (with a large-N sample) in nature, a discussion of key issues in qualitative (or small-N) studies also is provided to highlight the versatility of QCA and offer guidance for these research situations
Contrarian Case Analysis. Contrarian case analysis considers the existence of cases that are not explained by the main effects in symmetric tests such as regression analysis (Pappas and Woodside 2021). An individual condition specified in a configuration can contribute positively or negatively to a specific outcome depending on the presence or absence of the other conditions in the configuration – the contrarian case tenet (Woodside 2016), which is especially important when the literature provides inconsistent evidence of the relationships between key variables. While we are not aware of any guidelines suggesting the percentage of contrarian cases that would support a configurational analysis, the average proportion of contrarian cases found here (26.5%) compares well with other marketing applications of QCA (Pappas and Woodside 2021; Russo and Confente 2019). An extended discussion of the importance of testing for contrarian cases and examining the sample distribution prior to conducting the QCA, the common procedure for investigating the prevalence of contrary cases in a large-N study, and results for the study variables, are provided in Web Appendix C.
Data Calibration. Calibration of the data is considered the most important step in QCA (Pappas and Woodside 2021). All fuzzy sets must be calibrated; most types of data can be used, with fsQCA being able to accommodate dichotomous and Likert-type responses. Generally the means of multi-item scales are used to derive a single value for each case on each condition, although alternatives such as factor or Rasch scores could also be used and may have advantages in being able to better account for the individual effects of each item on the construct itself (Brush and Soutar 2022; DiStefano, Zhu, and Mindrila 2009).
The researcher needs to transform the raw numerical data into degrees of membership in the target set. While the fsQCA software can mechanistically transform and calibrate fuzzy sets it is highly advisable that direct calibration is undertaken and the choice of calibration thresholds are informed theoretically, especially as calibration decisions can impact significantly on the results. 5 Robustness checks consider the sensitivity of the results to different calibration thresholds and are highly recommended. Direct calibration requires the researcher to choose three qualitative breakpoints (also referred to as thresholds or anchors) that define the level of membership in the fuzzy set for each case: full inclusion in the set, full exclusion from the set, and the crossover point reflecting maximum ambiguity.
While researchers in areas where QCA studies are more numerous, such as political and social science, often have reference points when determining the membership criteria, this is rare in marketing research. When reference points are unavailable for the membership anchors, researchers must choose these values. The two most common approaches involve: (1) use of original values in the scale as the thresholds, or (2) calculation of percentiles that allow for calibration of any measure regardless of its original values. When original values of a seven-point Likert-scale are used, generally six, four and two (e.g., Ordanini, Parasuraman, and Rubera 2014) or seven, four or other measure of central tendency such as the median, and one, are specified as anchors (e.g., Russo and Confente 2019). For a five-point Likert-scale the thresholds four, three and two are suggested (Pappas and Woodside 2021).
The use of percentiles is also common, although no general standards appear to exist as to recommended anchors, at least not for normally distributed data. In practice these range from 0.95, 0.50 and 0.05 (e.g., Pappas and Woodside 2021) to 0.75, scale mean point and 0.25 (Fainshmidt et al. 2019). Nonetheless there is support for the use of percentile thresholds of 0.8, 0.5 and 0.2 when the data is non-normal (Pappas et al. 2017; Pappas and Woodside 2021; Woodside, Nagy, and Megehee 2018), which is the case in this study. 6 When the data are non-normal, selecting the three qualitative breakpoints on the survey scale (five-point Likert-scale in this study) can lead to less meaningful results (Pappas et al. 2017) and produce only one solution with all conditions identified as necessary (Plewa et al. 2016). In the current study, a single solution was provided only when we used a 0.95, 0.50 and 0.05 calibration, and also when using the original values of the scale, five, three and one, for the reverse outcome. Thus, in this study the 80th percentile is the full-set membership, the 50th percentile the crossover point and the 20th percentile is the full-set non-membership. 7 The thresholds are then set as follows: Vaccine Intentions 5.00–4.00–1.00; Pandemic Severity 5.00–4.20–3.60; Belief in Science 4.20–3.40–2.60; Trust in Government 3.00–2.33–1.67; Communal Orientation 4.60–4.00–3.80; Psychological Reactance 3.00–2.40–1.80; Religiosity 4.33–2.50–1.00. Personal knowledge was calibrated as a crisp-set causal condition given its qualitative-scale measurement. Based on these values, study participants who responded with a five on the Likert scale belong to full-set membership, indicating a very high level of intention to be vaccinated. Similarly, full-set membership requires a response of four or higher to all conditions with the exception of trust in government and psychological reactance where respondents provided lower values. Full-set membership for these two conditions requires moderate levels of agreement with most responses under the value of four on the five point Likert scale. This aligns with reports of very low levels of public trust in government at the time of the study (Pew Research 2022). While we could calibrate these two conditions differently, following Pappas et al. (2017) to be consistent we calibrate trust in government and psychological reactance the same as the other constructs.
Software and Calibration Function. There are a number of software options for QCA; we use the fsQCA software (version 3.0) developed by Ragin and Davey 2016 that is most frequently used in business and management (Berger 2016). 8 The fsQCA software uses the logistic function as the calibration function, which is appropriate here as the functions are monotonic, always increasing or always decreasing to a certain point. 9 However, there are situations where a non-monotonic function is required for calibration, such as when the focus is on political moderates where those with strong left-wing or right-wing ideologies should be excluded. Here the ‘bell-shaped’ function should be used and an alternative to fsQCA is required, such as R, as the logistic function is the only calibration function available in the fsQCA software. 10 There are also many other functions beyond the logistic and ‘bell-shape’ function (Thiem 2014). There is no empirical evidence suggesting that calibration functions dramatically alter the QCA results, using the same set of calibration thresholds (Duşa 2021).
Inductive, Deductive or Abductive Approach. QCA can be used for inductive theory generation and elaboration (Pappas and Woodside 2021), deductive theory testing (Fiss 2011) and abductive reasoning (Saridakis, Angelidou, and Woodside 2020). Researchers primarily use QCA in an inductive way, likely due to the challenges of developing specific a priori causally complex predictions in light of the overwhelming dominance in marketing research of net-effects oriented propositions and hypotheses. Nonetheless, it is possible to combine inductive and deductive reasoning by first identifying all possible causal configurations that explain the outcome then testing of specific propositions. 11 This linked approach can overcome the risk that explicit theorizing can ignore disconfirmatory evidence, and considers inductive explanations important for revising deductive theories, providing support for theoretical refinements and specification of scope conditions (Boswell and Brown 1999).
Output Solutions, Consistency, Coverage and Thresholds. QCA can distinguish core conditions from peripheral and irrelevant ones, where the difference is determined by the strength of the evidence relative to the outcome (Fiss 2011, p. 403). Fuzzy-set QCA software provides three solutions: complex, intermediate and parsimonious. The complex solution presents all of the possible combinations of conditions, but may result in a large number of identified configurations and include configurations with several terms, making the interpretation of the solutions somewhat difficult and often impractical (Pappas and Woodside 2021). The parsimonious solution is a simplified version of the complex solution presenting only the ‘decisive causal ingredients’ (Misangyi et al. 2017, p. 276) (generally termed core conditions) that cannot be left out from any solution, but excludes peripheral conditions. This solution requires simplifying assumptions about the logical remainder rows (truth table rows not populated with cases), and can incorporate solutions with limited cases without regard to their empirical plausibility (Schneider and Rohlfing 2016). Core conditions remain part of the solution when all simplifying assumptions (consistency with empirical and theoretical knowledge) are included. In the intermediate solution, conditions are added that are also present in the cases that consistently display the outcome but require difficult counterfactuals (consistent with empirical knowledge but not with theoretical knowledge) to be removed (Greckhamer et al. 2018; Ragin 2008). These are generally termed peripheral conditions. An intermediate solution (which is a subset of the parsimonious solution) including core and peripheral conditions is generally preferred as it can offer a more detailed and aggregated view of the findings (Fiss 2011). We focus on this solution in our study. 12
QCA solutions are evaluated primarily on the basis of their consistency and coverage. Consistency should always be assessed first, as if this is too low, the calculation of coverage is meaningless (Schneider and Wagemann 2012). The consistency measure is the proportion of consistent cases (i.e., the number of cases who are members of both a causal (solution) set and the outcome set, divided by the total number of cases who are members of that causal set (Ordanini, Parasuraman, and Rubera 2014)). Higher solution consistency can lead to more robust findings (Emmenegger, Schraff, and Walter 2014), and it is recommended to set this threshold at 0.80 (Fiss 2011; Pappas and Woodside 2021) in large-N studies. Proportional Reduction in Inconsistency (PRI consistency) is an alternate measure of the consistency of subset relations in fsQCA. PRI consistency is used to avoid simultaneous subset relations of configurations in both the outcome and the absence of the outcome (i.e., negation). PRI consistency scores should be high and close to raw consistency scores (e.g., 0.70), while configurations with PRI scores below 0.50 indicate significant inconsistency (Greckhamer et al. 2018).
Researchers are advised to consider necessary conditions. A necessary condition implies that the outcome is not present unless the condition is also present, and is identified when the condition exceeds the recommended 0.90 consistency threshold (Tóth et al. 2015). Other conditions cannot compensate for the absence of a single necessary condition. Even if the necessary condition is in place, the outcome is not guaranteed (Dul 2016). Schneider and Wagemann (2012) consider that conditions that pass the consistency test as a necessary condition should not be deemed to be relevant necessary conditions unless they also obtain a high value in the relevance (coverage) measure. 13 The fsQCA approach does not express degrees of membership when formulating the necessary condition, assuming that the necessity applies to the entire range of condition and outcome values.
Coverage is an assessment of the extent to which a subset (of the conditions) physically covers the target set (outcome), allowing for equifinality, which occurs when several effective combination routes can lead to the same result. There are three coverage metrics: raw coverage, unique coverage and solution coverage. Raw coverage measures the proportion of memberships in the outcome explained by each term of the solution, and provides the explanatory power of an individual configurational solution (Fiss 2011). However, any single observation might be explained by multiple configurations, and therefore a measure of each configuration's unique contribution to the solutions is provided in the form of unique coverage (Ragin 2008). Unique coverage shows how much of the overall coverage stems exclusively from the respective path, explaining the part of a configuration that does not overlap with others in explaining cases exhibiting the outcome (Fiss 2011). Ragin (2008) suggests that only solutions with a unique coverage of 0.01 or higher should be retained. Solution coverage measures the proportion of memberships in the outcome that is explained by the complete solution and is partially analogous to R-squared in regression. Coverage is generally used descriptively rather than diagnostically (Mendel and Ragin 2011). Tradeoffs are often required with consistency (Schneider and Wagemann 2012). The coverage scores for configurations can highlight the dominance of some paths over others to achieve the outcome. Solution coverage results in large-N QCA studies in management and marketing show considerable variation from 0.10 or lower to higher than 0.80 (cf. Misangyi and Acharya 2014; Pappas and Woodside 2021) with a focus often on configurations that might have low statistical relevance but offer important theoretical insights. The difference between these three coverage metrics is illustrated in Figure 1. Solution 1 is divided into parts a, b, c and d, and solution 2 into parts d, e and f.
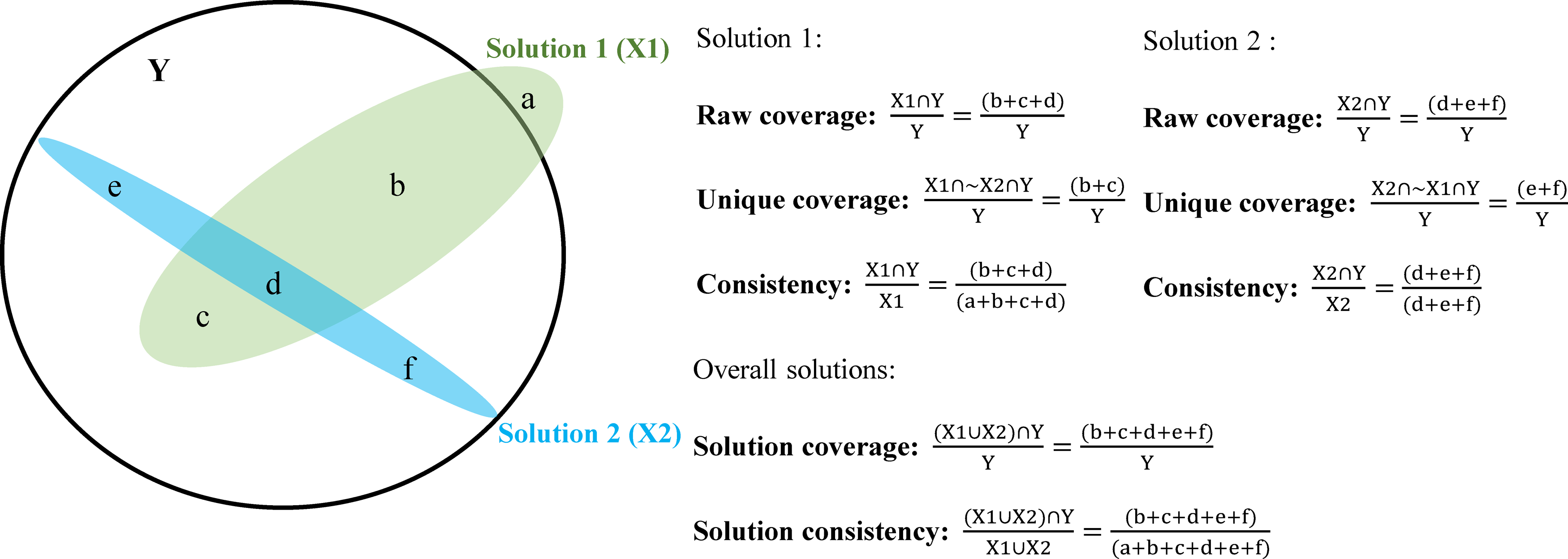
Understanding coverage and consistency metrics in QCA.
Before running the QCA, researchers must decide on a frequency threshold that is required to be met for configurations to be retained in the analysis. For larger samples (e.g., greater than 150 cases) this threshold may be set at three (or higher), while for smaller samples (e.g., less than 60 cases) the threshold may be set at one (Fiss 2011; Pappas and Woodside 2021).
QCA for Small-N Studies. While the focus of this paper is on an application of QCA with a large-N sample, it is a very versatile method and can be applied equally well as a research strategy and analytic technique in qualitative small-N studies. Web Appendix D provides a discussion of how researchers’ goals, assumptions and research processes often are different in small-N studies, factors that support the appropriateness and advantages of set-theoretic methods, and a summary of key differences between small/medium-N and large-N QCA regarding sample size, the ratio of cases to conditions, calibration procedures, frequency thresholds, consistency and coverage considerations, treatment of contradiction cases and within and cross-case analyses (or process tracing).
Results
fsQCA Findings for Vaccine Intentions
Table 3 presents the intermediate solution findings from the fsQCA output for vaccination adoption intentions. Following standard conventions, the presence of a condition, or core condition, is indicated by a large filled black circle (●); the negation, or absence, of a core condition with a large crossed-out circle (⨂). Smaller circles using the same nomenclature are used for peripheral conditions. Where there is a blank space this indicates that the condition is neither core or peripheral in the configuration, often termed a ‘don’t care’ condition. These latter conditions can be either present or absent and consequently do not play a role in the specific configuration (Pappas and Woodside 2021).
fsQCA Solutions for Vaccine Adoption Model.
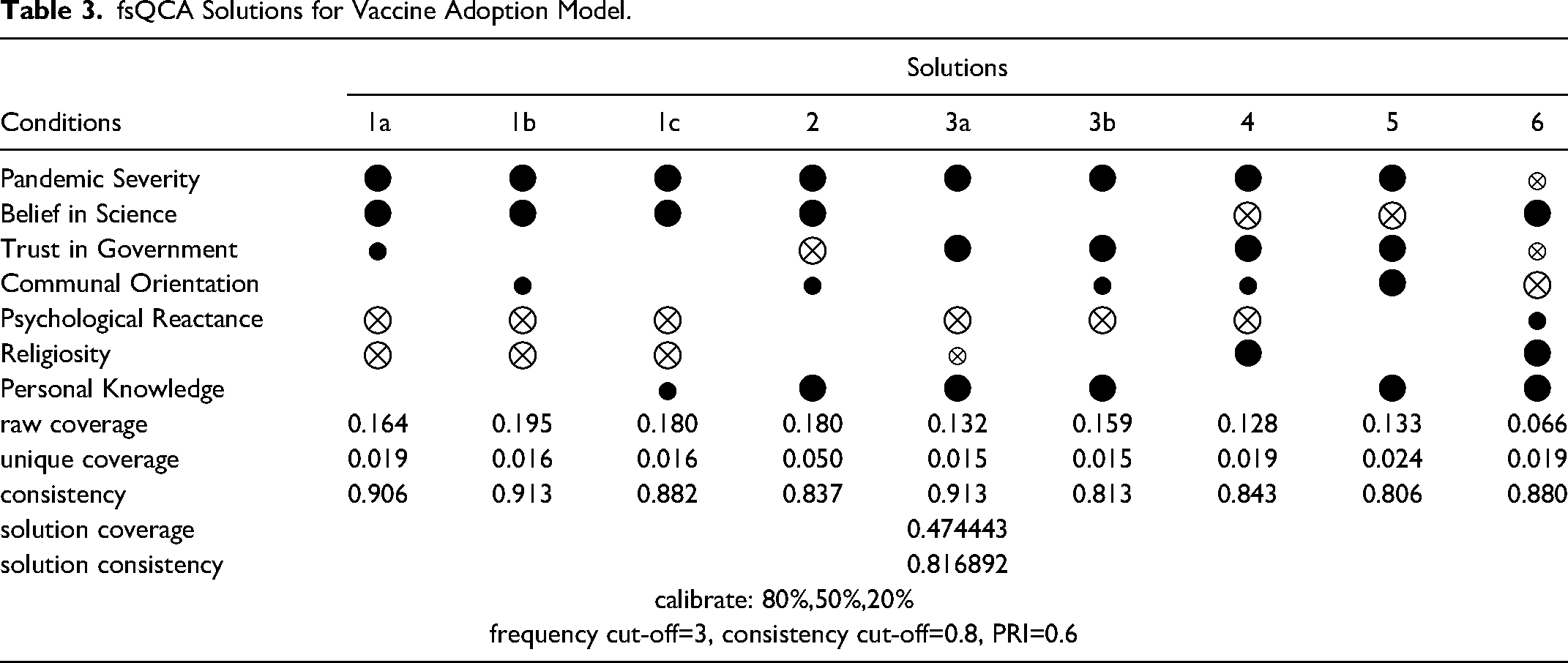
There are nine solutions identified with a solution consistency of 0.82 and overall solution coverage of 0.47. Paths numbered 1a, 1b and 1c have the same core conditions, with only the peripheral conditions being different. This is the case also for paths 3a and 3b. Solutions 1a-c show that a combination of high concern about the severity of the pandemic, a strong belief in science, and the absence of psychological reactance and religiosity lead to high vaccine adoption intentions. In the parsimonious solution (not shown here) the configuration solution with these core conditions had the highest raw (0.26) and unique (0.07) coverage. There is an additional peripheral condition in each of the solutions distinguishing these paths. In solution 1a this is trust in government, communal orientation in solution 1b, and personal knowledge in solution 1c. In solution 2 the presence of pandemic severity, belief in science and personal knowledge, and the absence of trust in government are core constructs, with communal orientation playing a peripheral role, and the presence or absence of reactance and religiosity irrelevant here. Solution 3 combines pandemic severity, trust in government, personal knowledge, and an absence of reactance. In solution 3a, the absence of religiosity is a peripheral condition; whereas in solution 3b communal orientation is a peripheral element. In solution 4 pandemic severity, trust in government and religiosity, and the absence of a belief in science and reactance play important (core) roles. Communal orientation has a weaker (peripheral) relationship with the outcome here. Pandemic severity, trust in government, communal orientation and personal knowledge, and the absence of belief in science are primary conditions in solution 5. In solution 6 a belief in science, religiosity and personal knowledge, and an absence of a communal orientation are core conditions; with low concerns about pandemic severity, low trust in government and the presence of reactance acting as peripheral conditions.
There were no conditions identified as necessary for the outcome, with all scores on the necessity condition tests clearly below the recommended 0.90 consistency threshold. Pandemic severity achieved the highest result with a consistency of 0.73 and coverage of 0.64, and it is present in eight of the nine solutions. Table 4 reports the necessary conditions analysis for the presence and absence of vaccine uptake intentions with respective consistency and (raw) coverage scores. The absence of psychological reactance is important in six of the solutions, with a belief in science and personal knowledge of someone with COVID core conditions in five solutions. Religiosity, trust in government, and even a belief in science can be either present or absent in explaining vaccination intentions depending on how they combine with the other conditions. Surprisingly, communal orientation is an important condition in only two solutions, with one of these requiring its absence (solution 6). Theoretical and practical implications of the results are provided in the ‘Discussion’ section.
Analysis of Necessary Conditions for Vaccine Adoption and Hesitancy Models.
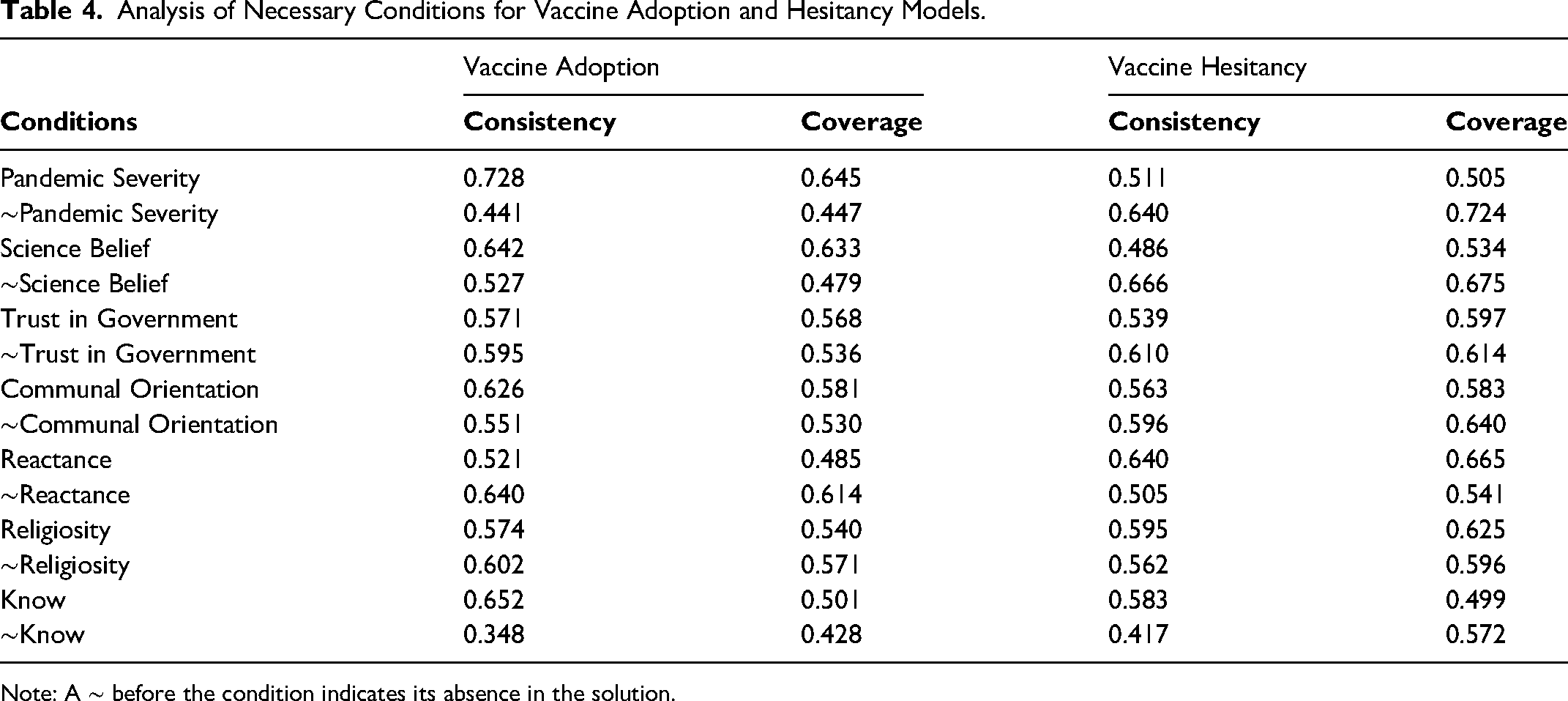
Note: A ∼ before the condition indicates its absence in the solution.
fsQCA Findings for Vaccine Hesitancy
The reverse, or negated, solution might not always be the inverse of the standard solution. It is important to consider the negated outcome, although this often is neglected in practice, as factors influencing positive responses may be different from those determining negative responses or avoidance behaviors. Table 5 presents the intermediate solution for vaccination hesitancy. The interpretation of the table is the same as for the standard solution. There are ten solutions identified, although solutions 6 and 10 should be excluded from analysis as these fail to meet the unique coverage threshold of 0.01. The solution consistency is 0.84 and overall solution coverage 0.47. The following discussion focuses on the retained solutions.
fsQCA Solutions for Vaccine Hesitancy (Reverse) Model.
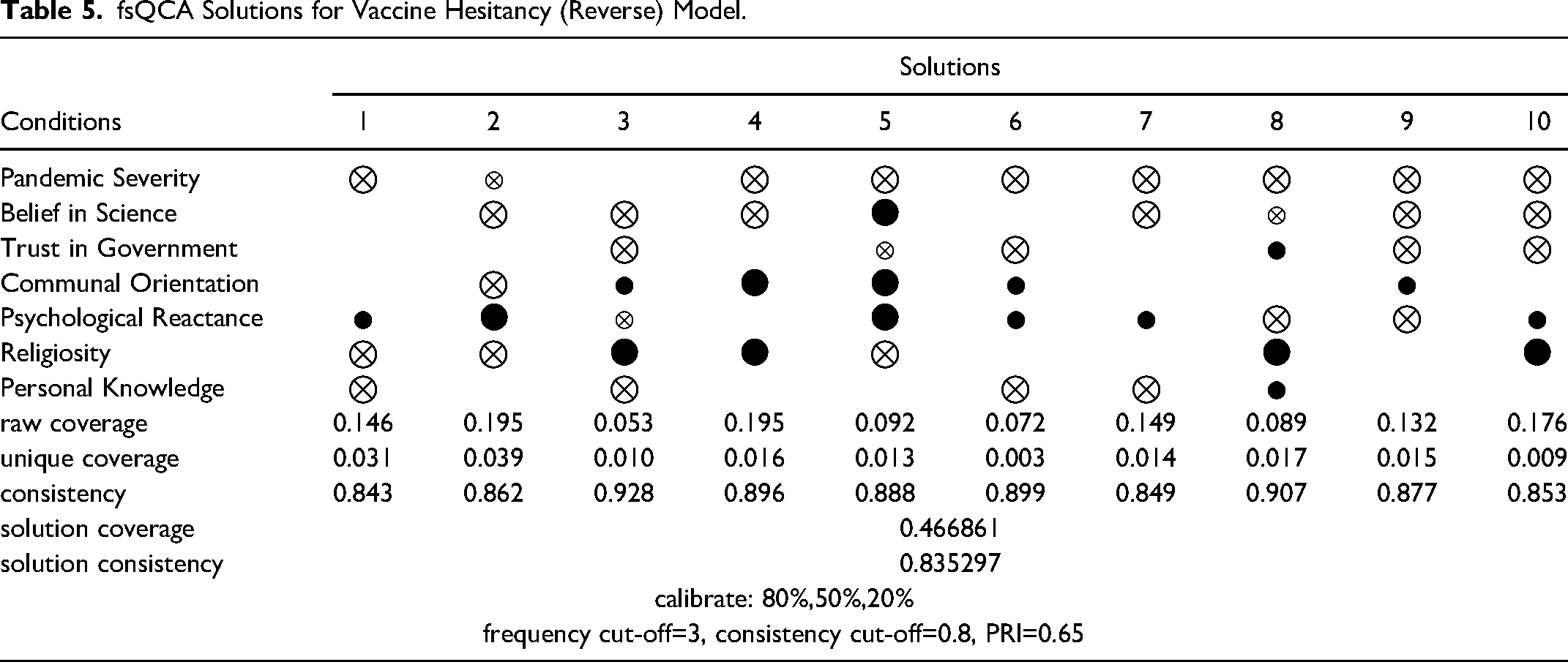
None of the causal conditions being examined are necessary for an individual to exhibit COVID vaccine hesitancy. The absence of a belief in science achieved the highest consistency score of 0.67, and the absence of pandemic severity concerns, the highest coverage of 0.72 (see Table 4). The absence of a high concern for the severity of the pandemic is a core condition in six of the eight retained solutions, with it also being a peripheral element in one other solution. Not personally knowing someone with COVID and an absence of a belief in science are core conditions in three and five solutions respectively. As found in the standard solution, religiosity can be either present or absent in explaining vaccine hesitancy, dependent on the presence or absence of other factors. These findings are to a large extent mirror images of those found in the standard solution. There also are differences, with vaccine hesitancy being explained with reactance both present and absent, and seemingly more dependent here on how it combines with other factors. For example, even though reactance is absent in solutions 8 and 9, in combination with an absence of a high concern about the severity of the pandemic, and little belief in science (as a peripheral element in solution 8 and core condition in solution 9), there is support for a vaccine hesitancy response. An absence of trust in government is a core condition in only two solutions explaining vaccine hesitancy, with its presence or absence being irrelevant for four of the eight retained solutions. Communal orientation can be either present or absent in explaining vaccine hesitancy, depending upon how it combines with other factors. Where its presence is a core condition it combines with an absence of a high concern for pandemic severity (solution 5) and in addition a low belief in science (solution 4) to explain vaccine hesitancy. That is, a high level of concern for others that could be expected to lead to increased vaccine adoption intentions appears to be overshadowed by perceptions of lower pandemic severity and also, for some, a limited belief in science.
The findings for vaccine adoption and hesitancy provide support for both propositions and indicate equifinality and causal asymmetry. More than one solution path exists that leads to a high (low) intention to receive a COVID vaccination (Proposition 1). The results also reveal configurations of high (low) intentions on which one condition may be either present or absent depending on its combination with other conditions (Proposition 2).
Testing for Predictive Validity
Predictive validity shows how well a model predicts the dependent variable in additional samples (Gigerenzer and Gaissmaier 2011; Pappas et al. 2016; Pappas and Woodside 2021). Following Woodside (2013) and Pappas and Woodside 2021 we undertook four steps to test the validity of our predictions. We first randomly split the data set into two equal-sized subsamples. Second, we obtained the solution for subsample 1 using the same process as outlined for the previous (original) vaccination adoption analysis. The frequency threshold was set at two to reflect the smaller subsample sizes. Third, to check whether the model derived from subsample 1 had predictive power for subsample 2, we used the subsample 2 data from the fuzzy plots of the first three of the solution paths to test the results from subsample 1 and to verify whether the consistency was greater than 0.80. Figure 2 provides the fuzzy-plot for model 1. 14 Fourth, we reversed the process and repeated steps two and three for subsample 2, using models 4-6, to test the predictive power of subsample 2. The consistency of both subsamples was greater than 0.80, indicating good predictive validity (see Table 6 for a summary of results). 15
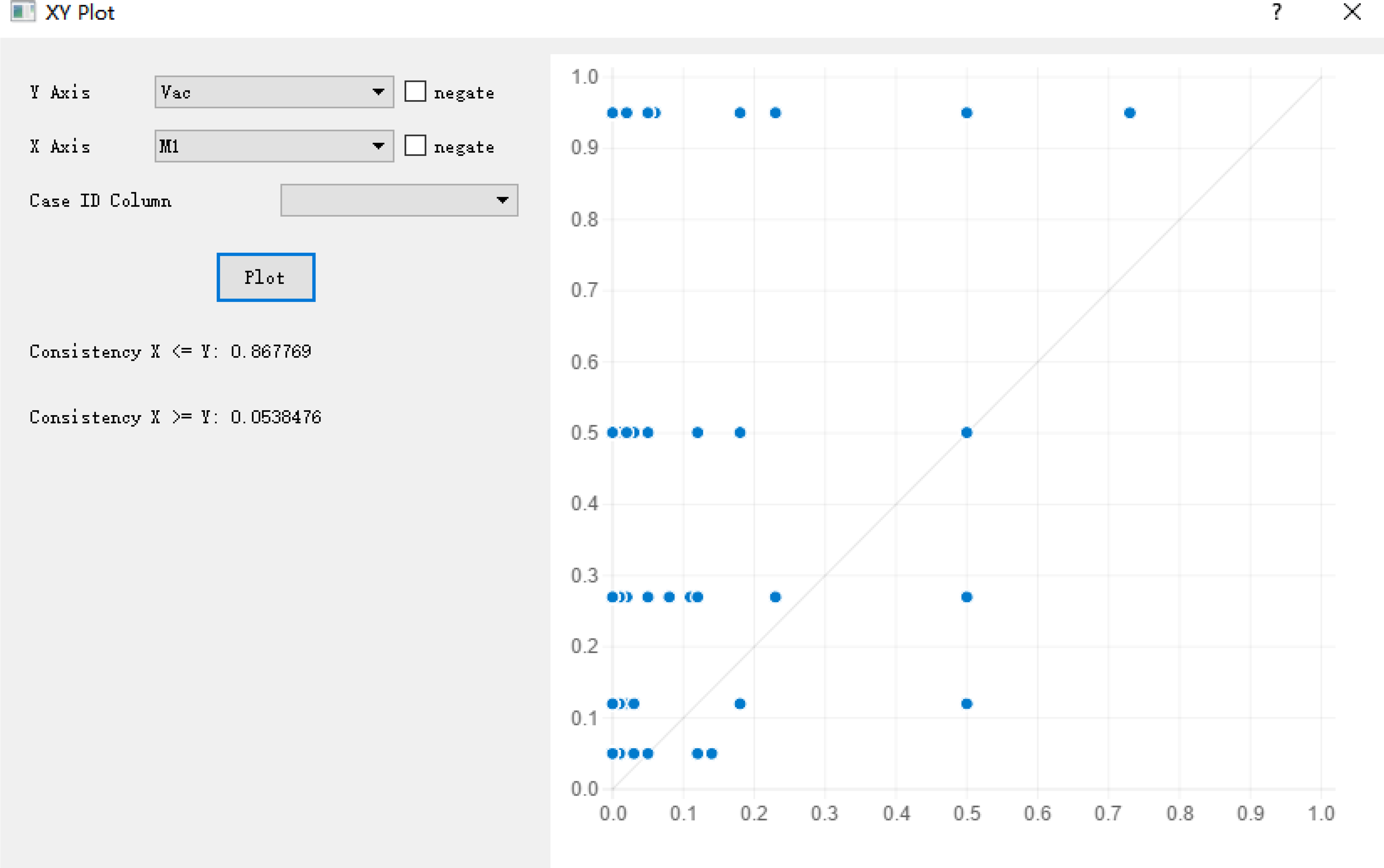
Fuzzy plot of model 1.
Predictive Validity Test Results.
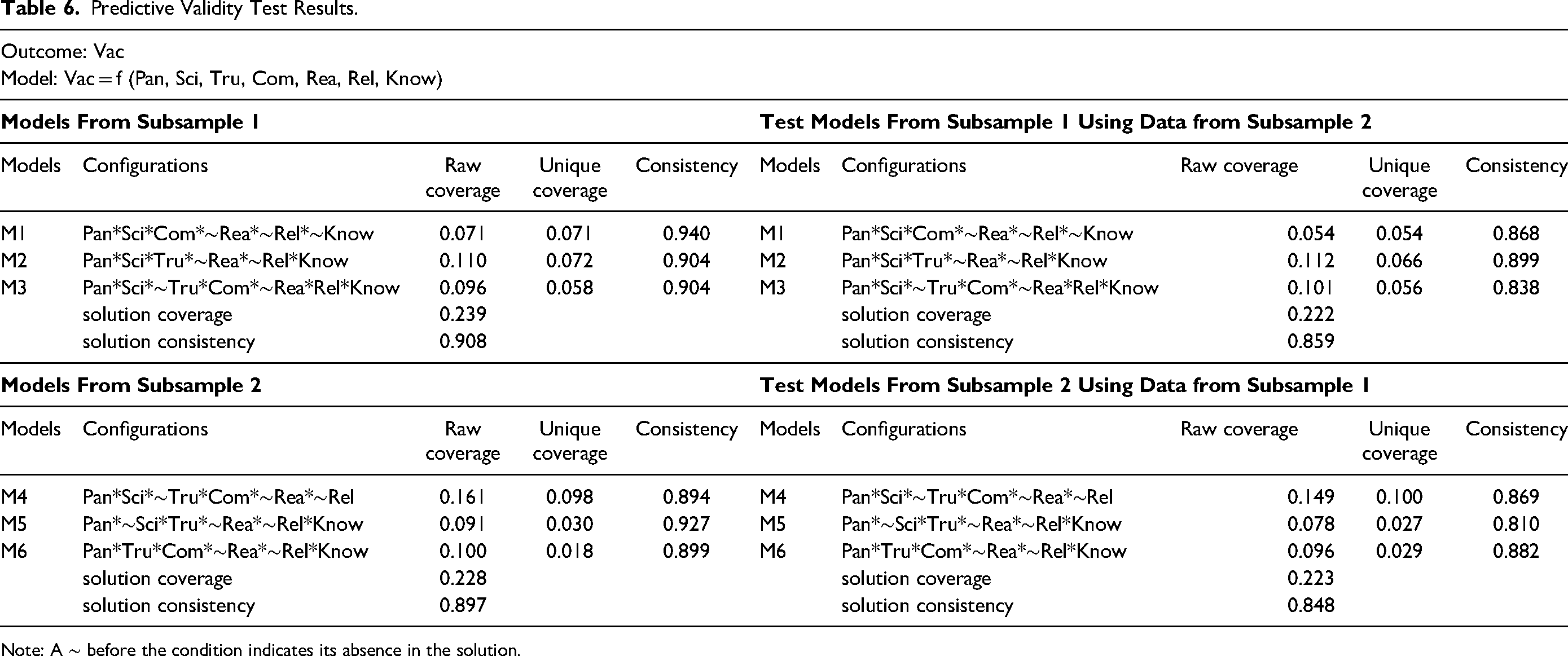
Note: A ∼ before the condition indicates its absence in the solution.
Robustness Tests
Following the recommendations from previous fsQCA studies (e.g., Schneider and Wagemann 2012; Wu et al. 2021) we varied the consistency thresholds, frequency thresholds and calibration strategies to investigate the robustness of our results for high and low vaccine intentions (see Table 7). We first considered the implications of setting a higher (0.85) or lower (0.75) consistency threshold for our high vaccine intention baseline model in fsQCA. At the higher consistency threshold, the overall solution consistency increased, the coverage decreased, and five configurations were eliminated from the baseline model. Use of the lower consistency threshold generated solutions identical to the baseline solutions, as no new configurations in the truth table were included for analysis. Second, we recalibrated the anchors by changing the full membership criterion by adding five percent (from 80 percent to 85 percent) and the full non-membership criterion by subtracting five percent (from 20 percent to 15 percent). These changes decreased solution coverage marginally and increased consistency. All solutions were logical subsets of the baseline solutions with one configuration eliminated. We further recalibrated the anchors by changing the full membership criterion by subtracting five percent (from 80 to 75 percent) and the full non-membership criterion by adding five percent (from 20 to 25 percent). Solutions were again logical subsets of the baseline solutions, although five configurations were eliminated. Third, to assess whether our results were robust to changes to the frequency thresholds, we reset these to four and two (baseline was three). At a threshold of four, solution coverage decreased, consistency increased, while solutions remained logical subsets of the baseline solutions. Two new configurations emerged when setting the frequency threshold to two.
Summary of Robustness Tests.
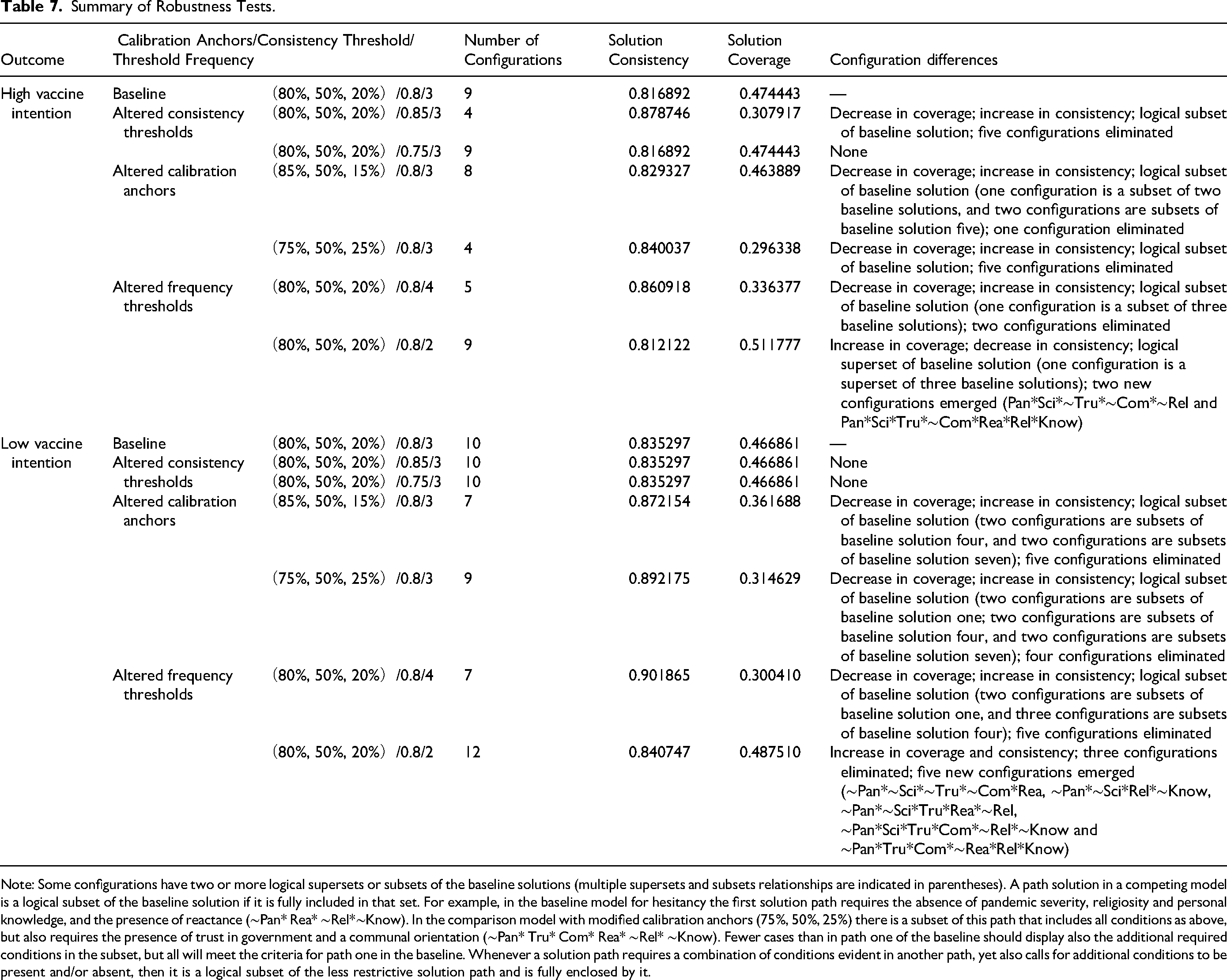
Note: Some configurations have two or more logical supersets or subsets of the baseline solutions (multiple supersets and subsets relationships are indicated in parentheses). A path solution in a competing model is a logical subset of the baseline solution if it is fully included in that set. For example, in the baseline model for hesitancy the first solution path requires the absence of pandemic severity, religiosity and personal knowledge, and the presence of reactance (∼Pan* Rea* ∼Rel*∼Know). In the comparison model with modified calibration anchors (75%, 50%, 25%) there is a subset of this path that includes all conditions as above, but also requires the presence of trust in government and a communal orientation (∼Pan* Tru* Com* Rea* ∼Rel* ∼Know). Fewer cases than in path one of the baseline should display also the additional required conditions in the subset, but all will meet the criteria for path one in the baseline. Whenever a solution path requires a combination of conditions evident in another path, yet also calls for additional conditions to be present and/or absent, then it is a logical subset of the less restrictive solution path and is fully enclosed by it.
Robustness checks for the low vaccine intention baseline model indicated no differences in the solutions when changes were made to the consistency thresholds. When modifications were made to the calibration anchors the results diverged. When setting the full membership criterion at 85 percent and full non-membership at 15 percent, the overall solution coverage decreased and consistency increased. The solutions were logical subsets of the baseline solutions, with five configurations eliminated. In addition, when setting the full membership criterion to 75 percent and the full non-membership criterion to 25 percent, while the solutions were logical subsets of the baseline solution, four configurations were eliminated. Finally, the frequency thresholds were again reset to four and two. When specifying the higher frequency, the configurations became a logical subset of the baseline solutions with five being eliminated. Five new configurations emerged when the lower frequency threshold was specified, although three configurations from the baseline were eliminated. The use of a higher frequency threshold resulted in a higher consistency but lower coverage than the baseline solution. The lower frequency model showed a marginally higher consistency and coverage than the baseline.
Schneider and Wagemann (2012) consider there are two set-theoretic-method specific dimensions indicating that results are not robust: (1) if different choices of calibration anchors and consistency and frequency thresholds lead to differences in the fit parameters large enough to require a meaningfully different substantive interpretation, and (2) if different choices lead to solution terms that are not in a subset relation with one another. Solution consistency in the robustness tests here are similar to the baseline model. However, by increasing the raw consistency and frequency thresholds, fewer truth table rows are used for logical minimization and as a consequence the new solutions can show less coverage (the reverse is less evident). The robustness test solutions are generally logical subsets of the baseline solution. There was little substantive deviation in the interpretation of the results with mainly new neutral permutations evident, and the same core elements observed and primary interpretation of the solutions persisted. Overall, none of the robustness tests showed substantial deviation from the baseline solutions, with all meeting one or both criteria, indicating that our reported findings are robust. However, it was evident that even small changes can affect the final fsQCA solution configurations (Gonçalves, Ferreira, and Silva 2016; Wu et al. 2021). Schneider and Wagemann (2012, p. 286) state that “If, however, there is a clear subset relation between different solution terms, then results can be interpreted as robust, even if these solution terms look quite different on the surface.”
Identification of Irrelevant Cases
When the consistency and coverage measures are applied in fuzzy-set analysis, cases with low membership in the condition or outcome count positively for consistency and coverage, thus creating the possibility that QCA solutions are driven by irrelevant cases. This is a significant problem as the existence of irrelevant cases can produce solution terms with high consistency and at least considerable coverage without supporting empirical evidence. Schwellnus (2013) proposes a resolution using the XY-plot for the solution terms to reveal the unrelated cases. However, using the XY-plot directly to detect irrelevant cases and present the results is less suitable for large-N samples.
In order to investigate for the existence of irrelevant cases in our analysis we first performed a preliminary check to determine whether our vaccination adoption results were driven by these cases. To do this we conducted an additional csQCA with a dichotomized dataset and compared the results with our original fuzzy-set analysis. Crisp-set comparison analysis was used here as it can alert the researcher to a possible problem and can help prevent false inferences. If a solution term showed considerably higher consistency and coverage under fuzzy-set than under crisp-set conditions (or did not qualify as a sufficiently consistent solution term under crisp-set conditions), then the fuzzy-set solution term was investigated as ‘suspect’ possibly due to irrelevant cases. Three such solution paths were identified: Pan*Tru*Com*∼Rea*Know (Path 3b), Pan*∼Sci*Tru*Com*∼Rea*Rel (Path 4) and Pan*∼Sci*Tru*Com*Know (Path 5). Second, we calculated the respective contributions of related and unrelated cases to the consistency of each solution, according to the preliminary comparison of the csQCA and fsQCA results. Third, we used the Schwellnus (2013) formula to exclude irrelevant cases when evaluating the consistency or coverage of our results. 16 The revised solution (with irrelevant cases removed) is provided in Table 8 with the solution terms renamed as new models M1a–M6 corresponding to our original solution. 17
Revised Solution with Irrelevant Cases Removed.
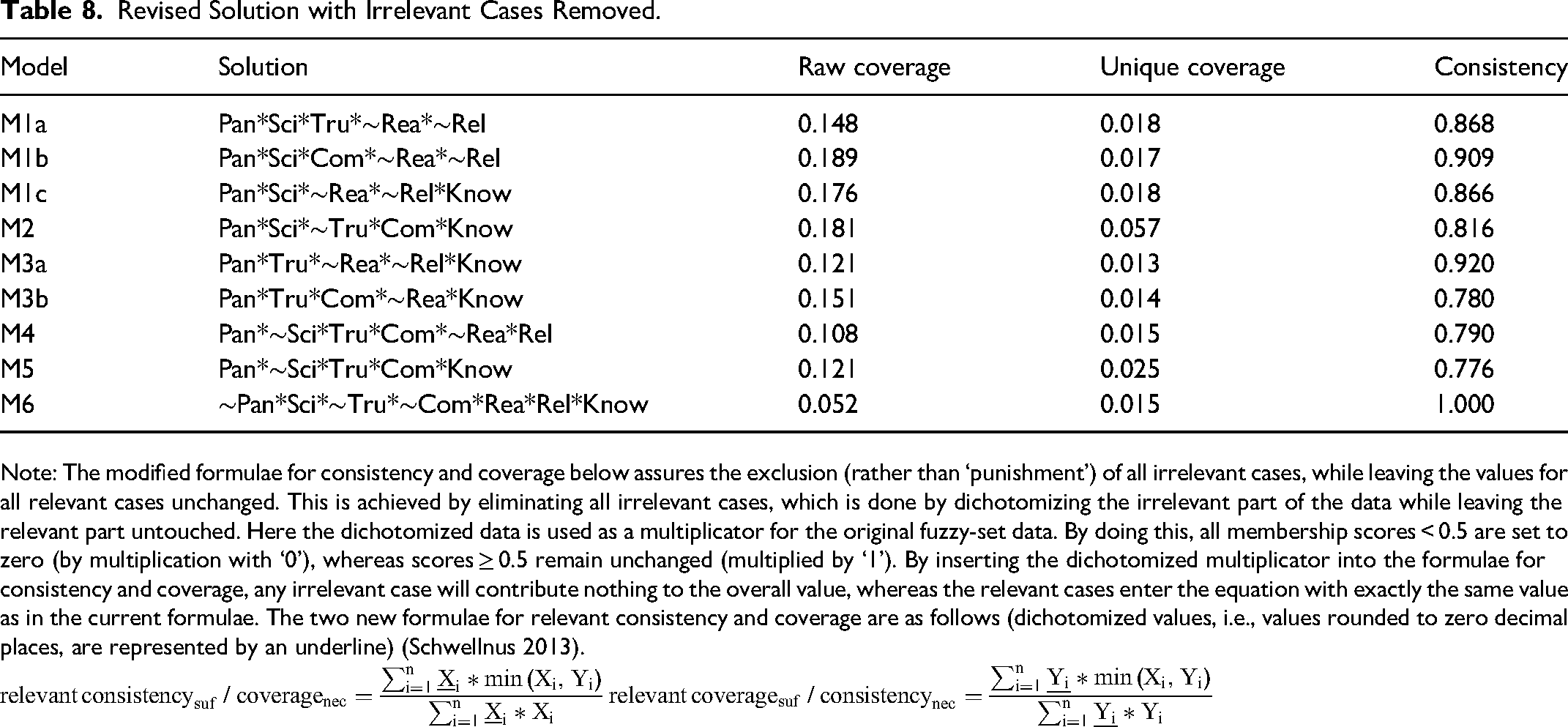
Note: The modified formulae for consistency and coverage below assures the exclusion (rather than ‘punishment’) of all irrelevant cases, while leaving the values for all relevant cases unchanged. This is achieved by eliminating all irrelevant cases, which is done by dichotomizing the irrelevant part of the data while leaving the relevant part untouched. Here the dichotomized data is used as a multiplicator for the original fuzzy-set data. By doing this, all membership scores < 0.5 are set to zero (by multiplication with ‘0’), whereas scores ≥ 0.5 remain unchanged (multiplied by ‘1’). By inserting the dichotomized multiplicator into the formulae for consistency and coverage, any irrelevant case will contribute nothing to the overall value, whereas the relevant cases enter the equation with exactly the same value as in the current formulae. The two new formulae for relevant consistency and coverage are as follows (dichotomized values, i.e., values rounded to zero decimal places, are represented by an underline) (Schwellnus 2013).
Taking into account the different weights in the consistency formula according to set membership, the weight coefficients of unrelated cases in M1a, M1b, M3a and M4 were greater than those of the related cases (factors ranged from 1.044 to 1.771); thus, these solution terms may be predominantly determined by irrelevant cases. However, when only accounting for relevant cases, M1a, M1b and M3a each exhibited sufficiently high consistency (greater than 0.80) indicating the solution terms were valid. In contrast, the consistency of M4 was now marginally less than 0.80. In M1c, M2, M3b and M5 the weight values of related cases were greater than for unrelated cases (factors ranged from 0.879 to 0.612). When exclusively considering relevant cases, M1c and M2 each provided sufficiently high consistency and their solutions appeared valid. In contrast, the consistency of M3b was slightly less than 0.80 with the same being true for M5. Irrelevant cases greatly outweighed relevant cases in M6 (by a factor of 9.6). The fsQCA result for this configuration thus appeared to be driven by irrelevant cases and therefore would be regarded as a ‘false positive’ and excluded from the overall solution. However, sufficiently high consistency was evident when taking into account only the relevant cases. In our analysis, the high ‘perfect’ consistency (consistency = 1) of M6 may seem coincidental, but it is reasonably present in our analysis, although perhaps infrequently encountered. Three relevant cases
18
were found in the M6 path, and after excluding the irrelevant cases using the revised consistency formula
Contradictions in fsQCA
A contradiction (or contradictory row), is a row of a truth table in which some cases exhibit the outcome and others do not (Rubinson 2013, p. 2855). The prevalence of the data-set to include both consistent and inconsistent observations tends to increase with sample size, particularly for individual-level data. Truth tables in fuzzy-sets do not produce contradictions as in crisp-set QCA (see Ragin 1987). This is a limitation of fsQCA for inductive analysis, and Rubinson 2013 describes how to extend fsQCA to incorporate the identification of contradictions and introduces a new measure, the consistency proportion threshold, which operationalizes contradictions as a ratio of consistent to inconsistent observations. Contradictory cases should be examined further as these challenge the basic model and could provide guidance on omitted conditions that may strengthen and refine theory.
To identify contradictions we first filtered the data in our truth table analysis using a consistency threshold of 0.80, proportional reduction in inconsistency (PRI) 0.60 and a frequency threshold of three. From this we obtained 75 truth table rows, which were then analyzed for contradictions. Of the 75 truth rows in our results there were 18 with high intentions to vaccinate outcomes, of which six were true and twelve were contradictions. 21 We determined whether there was a contradiction by calculating the proportion of consistent and inconsistent cases for each of the 75 truth rows. For example, in truth row one (which specifies membership scores greater than 0.50 for pandemic severity, trust in government, communal orientation, religiosity and personal knowledge; and non-membership scores less than 0.50 on belief in science and reactance) the proportion of consistent cases was 0.56 (9 of 16 cases) and the proportion of inconsistent cases 0.44 (7 of 16 cases), both falling below the specified consistency proportion threshold of 0.80. Thus, the vector space corner would be categorized as contradictory (Rubinson 2013). If we were to incorporate contradictions in our fsQCA we would need to further investigate the twelve truth rows that had contradictions, by returning to the cases covered by each of these truth rows to investigate which ones were causing the inconsistencies. Extending Rubinson 2013, we also identified the total number of contradictions in our configuration paths, and through this can identify which contradictions exist in the truth rows that make up each path. A specific path of the baseline model is obtained by the Boolean algebra simplifying calculation from the truth rows, so we can manually identify which truth rows forming a specific path are in contradiction. To do this we use the counts of the intermediate solutions, as the parsimonious solution also considers all of the truth rows with frequency numbers below three. 22 Researchers using fsQCA generally accept high consistency as sufficient, and neglect to undertake more holistic and complex investigations of cases that show nonoccurrence and inconsistency (Rubinson 2013). Further investigation of contradictions encourages researchers to return to their data and to revisit their cases, deepening their understanding of the social phenomena under study from both confirmatory and contradictory perspectives.
Evaluating a Two-Step QCA Approach
The two-step approach was developed by Schneider and Wagemann (2006) to address the phenomenon of limited diversity and complexity of results. This is especially an issue for small and medium-size N studies. When it is considered essential that a larger set of conditions are examined in a small-N study, there may be value in considering a two-step QCA approach. The two-step approach also can integrate a temporal dimension into conventional QCA and is considered a technique for better differentiating between conditions located at different distances from the outcome (Schneider and Wagemann 2012). Two-step QCA can be used with crisp, multi-value and fuzzy sets. Web Appendix E provides a summary of the key motivations for undertaking a two-step approach, an overview of the common procedure for the two-step method and an application using the study conditions.
Exploring Differences Across Solution Paths
To explore the existence of differences amongst the cases following two mutually exclusive paths with high vaccination intention outcomes, we manually calculated the raw coverage for solution paths one and five, as the fs/QCA software did not cover all cases for each specific path, only showing up to twenty representative cases per path. Univariate analyses (chi-square and t-tests, see Table 9) were then undertaken to investigate whether any demographic differences were apparent. While, due to low sample sizes, none of the differences tested in the chi-square tests were significant statistically, there were some interesting directional trends. In particular, Path 1 had a slight female skew and these cases were more likely to be characterized as being over the age of 55 years and to be white in ethnicity. Conversely, those in Path 5 were more likely to be male, to earn a medium-level annual income (USD35 000 −74 999) and to have a college degree. An independent samples t-test reveals that those in Path 1 were more likely to be Democrat leaning in their political views than those in Path 5 (t = - 4.14, p < 0.05). Those in Path 1 were also more likely to be located in the US South.
Univariate Analysis of Differences between Path 1 and Path 5.
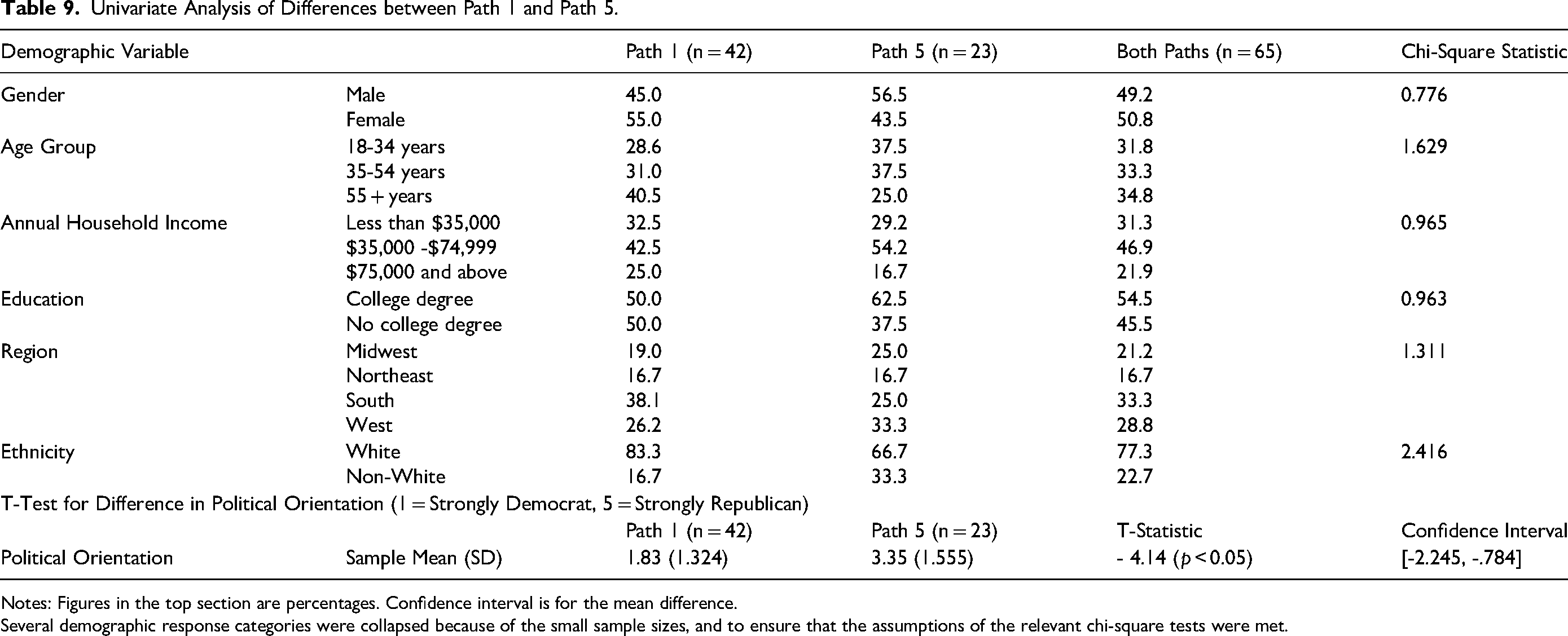
Notes: Figures in the top section are percentages. Confidence interval is for the mean difference.
Several demographic response categories were collapsed because of the small sample sizes, and to ensure that the assumptions of the relevant chi-square tests were met.
Alternative Model Configurations
As pandemic severity and personal knowledge conditions feature in most of the solutions that indicated the presence or absence of vaccine uptake intentions, an additional analysis was run without them to investigate the co-occurrence of the other conditions. Also, a further analysis was conducted where only personal knowledge was excluded. The intermediate solution findings and a discussion of results is provided in Web Appendix F.
Discussion
Vaccine hesitancy was already a growing concern before the COVID-19 pandemic (World Health Organization 2020). In the early part of the COVID-19 pandemic, it became increasingly critical to communicate the importance of vaccination as a tool to fight the virus. However, vaccine hesitancy is a complex phenomenon (Machingaidze and Wiysonge 2021). This study provides an alternative approach to additive variable-oriented models by utilizing QCA to understand and reveal the social complexity of vaccine uptake. Social complexity concerns the processes of ‘becoming’ (as opposed to ‘being’), characterized by the heterogeneity of cases and the variation in time- and place-bounded ‘causal recipes’ (Gerrits and Pagliarin 2021). This study demonstrates that QCA is a useful tool to address complex causality in vaccination uptake and provides a systematic approach to understanding the mechanisms at work in vaccine (non) uptake across contexts. An understanding of the more complex relationships underlying vaccination uptake (or lack thereof) allows social marketers and policy makers to design campaigns targeted toward specific segments, based on their combinations of causal factors, rather than a ‘one size fits all’ approach.
Implications for Theory, Social Marketing and Public Policy
While this research found that no singular condition was necessary, the perceived severity of the pandemic appeared to be the most important condition and was present in all but one of the solution paths for vaccine acceptance. An absence of belief in the severity of the pandemic was also evident in almost all paths to vaccine hesitancy. This has direct implications for the role of communications in raising awareness of the severity of the health crisis appropriately. In the one solution path where pandemic severity was absent, those who indicated vaccine acceptance intentions had personal knowledge of a person infected by the virus. Personal knowledge was present in over half of the solution paths for vaccine acceptance and largely absent in those who were vaccine hesitant. These findings support the importance of social marketing communications that can illustrate both the severity of the virus and personal stories of its impact (Nowak et al. 2015). This can be achieved through simulating familiarity (Weisbuch and Mackie 2009), such as using images and stories of trusted peers or public figures (Cartmell et al. 2019).
Belief in science was also an important condition in this study, and an absence of belief was evident in most solution paths for vaccine hesitancy. Americans’ belief in science is relatively high, with three quarters having at least a fair level of trust in scientists. High numbers of people believing in science has positive implications for increasing rates of vaccine acceptance, which is reflected in just over two-thirds of Americans being fully vaccinated, although only a little more than one-third have received a booster shot (World Health Organization 2023). These findings emphasize the need for messaging that maintains the perceived severity of the pandemic, but with pandemic fatigue setting in, arguments must also be supported by the robustness of the science behind them to ensure their credibility (Bodas et al. 2023). A lack of belief in science influenced vaccine hesitancy, which has implications – higher death rates are attributed to anti-scientific beliefs (Hotez 2021). Research suggests that anti-science beliefs are enhanced when the messenger lacks credibility; when people associate with a group that is anti-science or if the information challenges their core values (Philipp-Muller, Lee, and Petty 2022). This was reflected in our findings on religiosity, with the solutions in our study highlighting the presence of a belief in science generally accompanied by an absence of religiosity, and a lack of belief in science accompanied by higher religiosity. This is supported by previous research which has found that religiosity can weaken the credibility of science (Hoogeveen et al. 2022), with scientists perceived as exhibiting biases against Christian values (Philipp-Muller, Lee, and Petty 2022). Maintaining a societal belief in science and tackling misinformation and anti-scientific sentiments are important factors in ensuring vaccine acceptance.
An unexpected outcome of this research was that in nearly half of the paths for vaccine acceptance, belief in science was either absent or irrelevant (may be either present or absent), but trust in government was present. Trust in government played a larger part than we had initially anticipated, particularly in its role in mitigating a lack of belief in science. The trust of citizens in their governmental civil servants is a significant predictor of their confidence in a vaccine's safety, effectiveness and importance (Denemark, Harper, and Attwell 2022). A large study in the UK found that positive perceptions of public sector officials and the government led to a substantive increase in vaccine willingness, with negative attitudes among the most unwilling to be vaccinated (Chaudhuri et al. 2022). While there is a low level of trust in elected officials, the presence of trust in government in this research may be due to the higher levels of trust in public health officials, and Americans were particularly critical of elected officials who they felt interfered with the ability of public health officials to respond to COVID (Kennedy, Tyson, and Funk 2022). This demonstrates the importance of trust in government and of supporting the credibility of officials, especially when there is a lack of belief in science.
The prevalence of psychological reactance was consistent with what we had anticipated. It was absent in nearly all of the scenarios for vaccine acceptance and was present in half of the retained solution paths for vaccine hesitancy. A more unexpected finding from this research was that communal orientation had an equivocal impact on the findings, being present in most solution paths for intentions and hesitancy to adopt vaccinations. Disaster research suggests that communal orientation increases during public emergencies and is often used as a mental health buffer to cope with uncertainty (Afifi, Felix, and Afifi 2012), so it was anticipated that this would be present and would have a larger impact on adoption outcomes (and equally would be absent in hesitancy outcomes). Instead it was predominately a peripheral condition in regards to vaccine acceptance and was present in half of the solution paths for vaccine hesitancy. Evidence suggests that Americans are less communal and more exchange-based in their interpersonal relationships when compared to other countries (Van Yperen and Buunk 1991). This frequent presence of communal orientation in vaccine hesitancy solution paths indicates that people's social connections and networks could be having a detrimental impact for many. Research has found that the spread of health misinformation in online social communities is most often about vaccines (Suarez-Lledo and Alvarez-Galvez 2021). Combatting misinformation within social groups will continue to be an ongoing challenge for vaccine programs.
Implications for Research Practice
The findings of this study should interest market and social researchers, and industry managers. The reasons for behavioral outcomes in social and market research are often complex. However, methodological limitations of traditional quantitative techniques make it difficult to evaluate and organize marketing activities to maximize performance. Studies, such as this one, are important tools for increasing the awareness and application of alternative and, in many cases, superior analytical approaches. QCA is a valuable method for identifying and investigating interdependencies and causal complexity among causal factors, as was demonstrated in this study. Discussion with senior market research industry executives highlighted that they often utilize traditional quantitative analysis, where independent variables are seen as analytically separable causes of the outcome under investigation, and which do not enable examination of more complex causation, where an outcome may follow from several different combinations of causal conditions. QCA does not disaggregate cases into independent, analytically separate aspects but instead treats configurations as different types of cases (Fiss 2011). Thus, causal explanations are investigated as combinations of factors, among which different combinations might produce the same outcome of interest (Greckhamer et al. 2008), allowing better allocation of resources to achieve the same outcome. QCA addresses questions around why some interventions worked and not others, as it investigates how causal attributes function in particular combinations rather than in isolation. This is particularly useful for evaluations where market researchers are interested not only in the results of a project or program, but also in how and why those results were achieved. QCA assists decisions relating to whether and/or how projects or programs could be scaled up or replicated (Baptist and Befani 2015).
QCA offers health service providers an analytical approach to consider the range of issues impacting on people's behavioral intentions. Vaccine uptake is a complicated issue that requires clear public health communication to counter ongoing criticism and hesitancy toward these types of medical measures (Schoch-Spana et al. 2021). For interventions to be effective, it is necessary to understand the different combinations of factors that can lead to a successful outcome to be able to develop a range of communication responses. QCA also would benefit future health and social marketing interventions, such as in respect of climate change, by helping to inform the creation of campaigns that focus on essential messages and avoid topics that are not relevant or may even undermine the key messaging. Understanding who to target and how is especially relevant in an era of misinformation and increasing polarization of social issues (Loomba et al. 2021; Puri et al. 2020).
Due to its robustness to small sample sizes, QCA also is a useful tool for researchers faced with sample sizes too small for the application of conventional linear statistical methods, but at the same time too large for the in-depth qualitative analysis generally utilized for very small numbers of cases (Ragin 1987; Ragin 2000). Such situations can often arise with particular subsamples of the population for which the incidence rate is too low to collect a large enough sample for many traditional quantitative analysis techniques, as is often the case in B2B research, and research among senior management and contexts where the cases are companies rather than individuals (Greckhamer et al. 2008).
Applications in Macromarketing
Macromarketing studies complex phenomena and this paper demonstrates how QCA can be applied to understand the interaction of multiple factors on systemic issues. Through researching vaccine intentions, we have demonstrated that acceptance and hesitancy are different states and that the factors impacting them can be independent or unrelated. There are a number of contemporary issues in macromarketing where a QCA methodology could enhance theory and improve practice. In the context of the natural environment, macromarketing has a unique part to play in addressing climate change by arguing for specific practices and policies that support environmental stewardship (Klein and Laczniak 2021; Shapiro et al. 2021), and QCA could assist in moving these concepts beyond the theoretical into practice. This approach could also be applied to systemic social and quality of life issues, such as social justice, human wellbeing and sustainable communities (Francis 2021; Layton and Grossbart 2006; Sheth and Parvatiyar 2021). For example, there is an opportunity to explore conditions that positively influence consumer wellbeing and quality of life, through understanding the interaction of factors that are objective and subjective (Sirgy and Lee 2006). QCA could be utilized also to understand the metrics of vulnerable consumers, whether it is those grappling with the challenges of disaster relief, to consumers who are susceptible to exploitation (DeQuero-Navarro, Stanton, and Klein 2021). For topics where choice is often between competing forces, such as in Klein and Laczniak's (2021) work that challenges the ethical efficacy vs. economic efficiency argument, QCA could help unpack the complex interactions and assist in developing system thinking solutions that may enable more ethical, sustainable and just outcomes. Wooliscroft (2021) argues that macromarketing's focus on studying systems goes beyond the limitations of micromarketing and consequently needs systems-based research methodologies. QCA's ability to deal with complexity, competing perspectives and mixed findings offers potential as one of these methodologies. Macromarketing issues are complex and QCA provides a method that can consider the interaction of multiple conditions in a more authentic and systemic way.
Future Research Directions and Limitations
Our research investigates the impact of pandemic severity perceptions, belief in science, trust in government, religiosity, communal orientation and personal knowledge on vaccine uptake. In developing this research, we draw upon the work of Van Bavel et al. (2020), which argues that a social and behavioral science perspective is required to support the efforts of medical experts to ensure vaccine uptake. However, vaccination uptake is complex and there are a multitude of variables potentially influencing this. Our selection of causal factors was based on existing theory, balanced with the requirements of QCA, which performs best with a restricted number of causal conditions (usually 4-8) to avoid solutions that are too complex to provide meaningful explanation (Haesebrouck and Thomann 2021). Future research may wish to investigate additional variables of interest to see how these causal factors combine to influence vaccination uptake. For example, it would be beneficial to consider the interaction of these conditions with traditional demographic data. Black American and ethnic communities have a history of medical mistreatment and continue to experience discrimination and socio-economic inequities in their health care experiences (e.g., Bailey, Feldman, and Bassett 2021). Investigating the impact of ethnicity on vaccine intentions would offer valuable insights into racial divides. Democrats and Republicans differ in the trust they place in scientists (Kennedy, Tyson, and Funk 2022) so it would be interesting to examine the impact of political affiliation on vaccine intentions, especially given that members of both political parties expressed frustrations at the political disagreements and misinformation, and its negative impact on the pandemic response (Saks and Tyson 2022). The role and effectiveness of financial and other incentives in motivating vaccine acceptance could be investigated, especially in light of the equivocal findings (cf. Robertson et al. 2021; Thirumurthy et al. 2022). Research also has found that vaccine hesitancy is higher among women, younger age groups, lower socio-economic groups and educational levels (Razai et al. 2021). Further investigation incorporating these conditions should consider a two-step QCA approach that allows for a larger number of total conditions to be used and the ability to model these factors as remote conditions. The reasons for hesitancy might include issues of complacency, access and confidence (Dubé et al. 2013; MacDonald 2015). Further investigation is needed into the interaction of these factors and their contribution toward increasing rates of vaccine hesitancy (Schoch-Spana et al. 2021). People are increasingly choosing to make decisions on vaccines based on personal experience, and recommendations from close friends and family, over scientific evidence or the advice of medical professionals (Larson et al. 2018, Nowak et al. 2021). Understanding the role that others have on decision making, beyond communal orientation and religious sentiment, would provide useful insights into the complex interactions of factors impacting vaccine intentions.
This research, conducted in the United States, led to a number of interesting findings. However, one limitation is that results may be bound to the US population among which the study was undertaken. Future research may wish to carry out similar studies of this nature to understand how the results replicate in other populations. For example, this research unexpectedly found that communal orientation impacted both on intentions to accept vaccination, and on hesitancy, in the United States. In more individualistic cultures, such as the United States, there is lower communal containment of COVID-19 than in more collectivist cultures (Cao, Li, and Liu 2020). Thus, it would be interesting to see whether this finding, regarding communal orientation, replicates in other cultures. In addition, it would be interesting to see how the findings with respect to trust in government replicate in other nations. Integrated government response policies, underpinned by containment health measures and economic reliefs, are crucial to winning public trust and support (Liu, Shahab, and Hoque 2022). Lack of trust in government is pronounced in the United States. Furthermore, in the USA, the response to the COVID-19 pandemic has been politically polarized, increasing the divide between partisan groups (Chen and Karim 2022). Political partisanship has been linked to diverging attitudes toward the virus (Priniski and Holyoak 2022) and is likely to have contributed to lower trust in government in the United States.
The scales utilized to measure the conditions of interest in this study were derived from previous studies, where they displayed appropriate psychometric properties, and were pre-tested for interpretability and understanding. Multi-item scales were utilized, with the exception of the single-item vaccine intention measure and binary personal knowledge variable. The binary measure of personal knowledge demonstrates the flexibility of the QCA technique in handling both categorical and continuous variables in the understanding of a phenomenon (often very important in social and market research). However, it is noted that the measure of personal knowledge as binary (i.e., ‘know someone infected by COVID-19’ versus do not), could represent a somewhat oversimplified measure of the construct. Other research has utilized multiple item scales for personal knowledge, and separated measures of personal knowledge into direct and indirect experience (e.g., Savadori and Lauriola 2022). While the development of a scale to measure personal knowledge was beyond the scope of this study, future research may consider utilizing more complex measures to unveil greater complexity of this construct.
FsQCA uses calibrated measures, as raw numerical data are transformed into degrees of membership in the target set. Calibration is common in areas where QCA studies are more numerous and researchers have reference points when determining the membership criteria, which is rare in marketing research (Russo and Confente 2019). As a result, this research utilizes an empirical approach to calibration. While our approach demonstrates the (often necessary) application of the empirical approach to calibration, future research should consider how theoretical knowledge could be used to inform these decisions, as to date there is little guidance here. Greckhamer et al. (2018) suggest that expert panels could be relied upon. Hodson and Roscigno (2004) provide an example of how external standards can be used to calibrate qualitative data. In the absence of theoretically informed calibration it is especially important to conduct robustness checks to investigate the sensitivity of the study results to these decisions.
Supplemental Material
sj-docx-1-jmk-10.1177_02761467231182300 - Supplemental material for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA
Supplemental material, sj-docx-1-jmk-10.1177_02761467231182300 for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA by Gregory J. Brush, Xiaoling Guo, Amabel Hunting, and Catherine Frethey-Bentham in Journal of Macromarketing
Supplemental Material
sj-docx-2-jmk-10.1177_02761467231182300 - Supplemental material for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA
Supplemental material, sj-docx-2-jmk-10.1177_02761467231182300 for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA by Gregory J. Brush, Xiaoling Guo, Amabel Hunting, and Catherine Frethey-Bentham in Journal of Macromarketing
Supplemental Material
sj-docx-3-jmk-10.1177_02761467231182300 - Supplemental material for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA
Supplemental material, sj-docx-3-jmk-10.1177_02761467231182300 for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA by Gregory J. Brush, Xiaoling Guo, Amabel Hunting, and Catherine Frethey-Bentham in Journal of Macromarketing
Supplemental Material
sj-docx-4-jmk-10.1177_02761467231182300 - Supplemental material for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA
Supplemental material, sj-docx-4-jmk-10.1177_02761467231182300 for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA by Gregory J. Brush, Xiaoling Guo, Amabel Hunting, and Catherine Frethey-Bentham in Journal of Macromarketing
Supplemental Material
sj-docx-5-jmk-10.1177_02761467231182300 - Supplemental material for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA
Supplemental material, sj-docx-5-jmk-10.1177_02761467231182300 for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA by Gregory J. Brush, Xiaoling Guo, Amabel Hunting, and Catherine Frethey-Bentham in Journal of Macromarketing
Supplemental Material
sj-docx-6-jmk-10.1177_02761467231182300 - Supplemental material for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA
Supplemental material, sj-docx-6-jmk-10.1177_02761467231182300 for Using Qualitative Comparative Analysis to Identify Complex Solutions and Optimal Combinations of Conditions Influencing COVID Vaccine Acceptance: A Primer for QCA by Gregory J. Brush, Xiaoling Guo, Amabel Hunting, and Catherine Frethey-Bentham in Journal of Macromarketing
Footnotes
Acknowledgments
The authors gratefully acknowledge the editor and reviewers for their extremely constructive feedback and guidance, and Helga Arlington for copy-editing assistance.
Associate Editor
Ben Wooliscroft.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplemental material for this article is available online.
Notes
Correction (November 2023):
Table 3 and Table 5 have been corrected to include the correct formatting of the peripheral absent condition circles.
Author Biographies
Recommended Practices for Conducting a Qualitative Comparative Analysis
Research Design
The study needs to include cases where the outcome is both present and absent, as a condition that is always present in the data has no explanatory power as it is necessary for both the presence and absence of the outcome.
A sufficient number of cases for each condition is required with special consideration needed for minority groups and contexts with low incidence rates. These situations may require a purposive sampling approach.
QCA does not rest on an assumption that the data are drawn from a given probability distribution.
QCA can test deductive explanations derived from extant theory and provide inductive theoretical revision.
Conditions need to have strong psychometric properties. Standard tests for reliability, validity and common method bias need to be used before applying QCA.
Sample Size
QCA can be applied successfully with small (10-50 cases) and large (thousands of cases) samples.
Fewer than ten conditions should be used, and the sample size should exceed the number of ideal types and combinations that are logically possible (2k ideal types are possible, where k is number of conditions). The more complex the model, the greater the number of unusual combinations of variables for which cases could not exist.
Calibration
Calibration should be informed by theory, with the anchors used and assumptions made provided.
Output Solution Selection
While the intermediate solution is commonly used to present fuzzy-set QCA findings there is recent evidence that the use of the parsimonious solution is preferred for crisp-set QCA (Baumgartner and Thiem 2020).
Necessary and Sufficient Conditions
It is important to consider whether any conditions are necessary or sufficient for the outcome. A necessary condition implies that the outcome is not present unless the condition is also present (e.g., when you observe the outcome, you will always observe the condition). However, when you observe the condition, you may or may not observe the outcome. A sufficient condition implies that the outcome will be present whenever the condition is present. When the condition is absent, the outcome can still be present.
Analysis and Interpretation
A consistency threshold of at least 0.80 is strongly recommended. Higher thresholds are desirable for macrolevel data and use of a lower threshold requires justification.
While there is no recommended guidance on acceptable solution coverage, a low score indicates there are many instances of the outcome that are not explained by the model. The solution coverage score is generally considered to be comparable with the R-squared reported on regression-based methods.
Reverse (negation) Outcome
QCA is asymmetric and it is important to examine the conditions influencing the absence or negation of the outcome separately. Macromarketing theory (e.g., Chatzidakis and Lee 2012) and QCA findings in related settings (e.g., Mellewigt, Hoetker and Lutkewitte 2018) highlight the conditions supporting the anti-outcome are not necessarily the logical opposite of those for the outcome.
Robustness of Results and Contradictions
Examination of predictive validity and robustness of the results to threshold variations is required.
Contradictions (identical combinations of causal factors with both positive and negative outcomes) should be examined, as these can provide further insights for theory development.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.