
Abstract
Introduction
Fisherfolk communities in sub-Saharan Africa carry a high HIV burden. In Uganda, HIV prevalence among fisherfolk is 3–5 times higher than the general population prevalence of 5.8% among individuals aged 15–49,1,2 in part due to poor healthcare access, including to HIV services. Healthcare barriers include a relative absence of nearby full-service facilities combined with poor transport infrastructure.3,4 Fisherfolk’s high mobility (following fish migrations and traveling to markets) and irregular work schedules mean that they are frequently far from healthcare, not consistently near the same facility, and unavailable during facility hours.3,5–8
Oral Pre-Exposure Prophylaxis (PrEP), the use of antiretroviral medications for HIV prevention, has shown efficacy in sub-Saharan Africa across multiple clinical trials, including in general populations of heterosexual men and women, heterosexual sero-discordant couples, and men and transgender women who have sex with men.9–12 Some research suggests high acceptability of PrEP, but low retention, among fisherfolk.13–16 Individual-level barriers to PrEP use among fisherfolk and other key populations in sub-Saharan Africa have included low educational attainment, low perceived risk, side effect concerns, mobility, competing needs for work, anticipated stigma (because PrEP medications are also used for HIV treatment), and fear of partner conflict.7,16–21
A review concluded that the knowledge base is thin regarding what HIV prevention interventions work for fisherfolk. 1 We conducted qualitative research to identify feasible strategies to improve PrEP implementation and social marketing messages to encourage PrEP use in Ugandan fisherfolk communities.
Materials and Methods
Setting
Study procedures were conducted at healthcare outreach events in the Nakiwogo and Kigungu fishing community landing sites (Wakiso District, Lake Victoria, Uganda). At outreach events, healthcare workers and community leaders mobilized fisherfolk (e.g., with bullhorns), and healthcare workers (including study team members) provided HIV testing, prevention, and treatment services, including oral PrEP, in temporary community venues or local healthcare facilities. During this study, PrEP was available for key and priority populations in Uganda (including fisherfolk).
Participants
We conducted ∼1-h in-person semi-structured interviews in Luganda or English with 35 HIV testing clients and 10 key stakeholders from August 14 to December 11, 2020. Fisherfolk were eligible if they were aged 18 or older and tested HIV-negative at an outreach event in Nakiwogo or Kigungu. We used purposive sampling to interview similar numbers of men and women across fishing-related occupations. The sample size was in accordance with recommendations for reaching saturation. 22
Fisherfolk Participant Characteristics (n = 35).
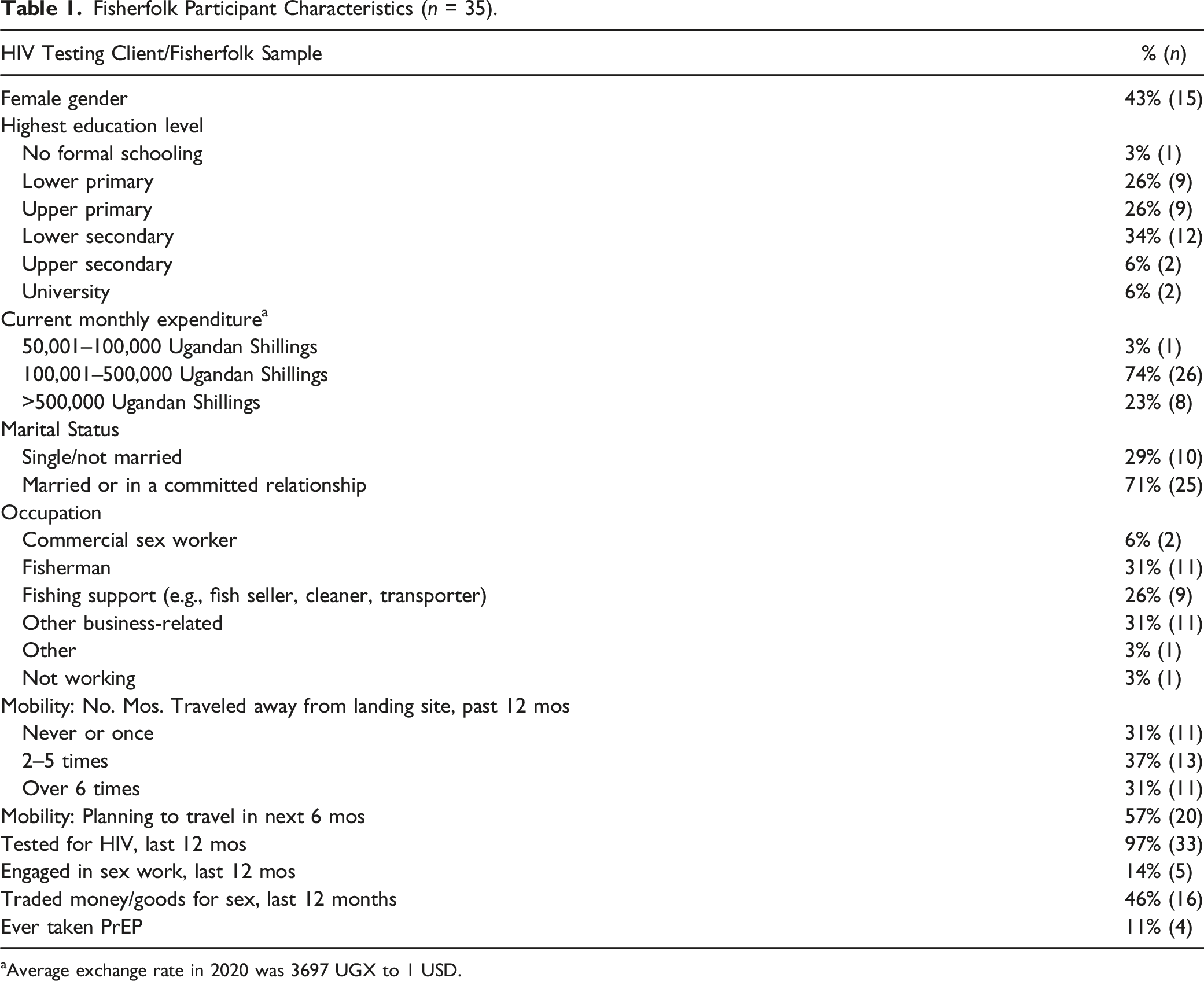
aAverage exchange rate in 2020 was 3697 UGX to 1 USD.
Procedures
During post-test counseling in outreach events, healthcare providers asked testing clients who screened HIV-negative and as eligible for PrEP (as a member of a key or priority population) if they would be interested in participating. If so, they were referred to the study coordinator [Ugandan male, MPH], who conducted interviews at a private space at the landing site. Stakeholders were identified and approached by team members who knew them through their work with fisherfolk. Interviews were conducted in a private space (e.g., workplace). Interviews were audio-recorded, transcribed, and translated. Participants provided written informed consent and received 20,000 Ugandan Shillings (∼$5USD) as compensation. All procedures were approved by institutional review boards in the U.S. as well as Uganda, including: the RAND Human Subjects Protection Committee (HSPC 2019–0571), the Makerere University School of Public Health Higher Degrees, Research, and Ethics Committee (HDREC 755), and the Ugandan National Council of Science and Technology (HS 2748).
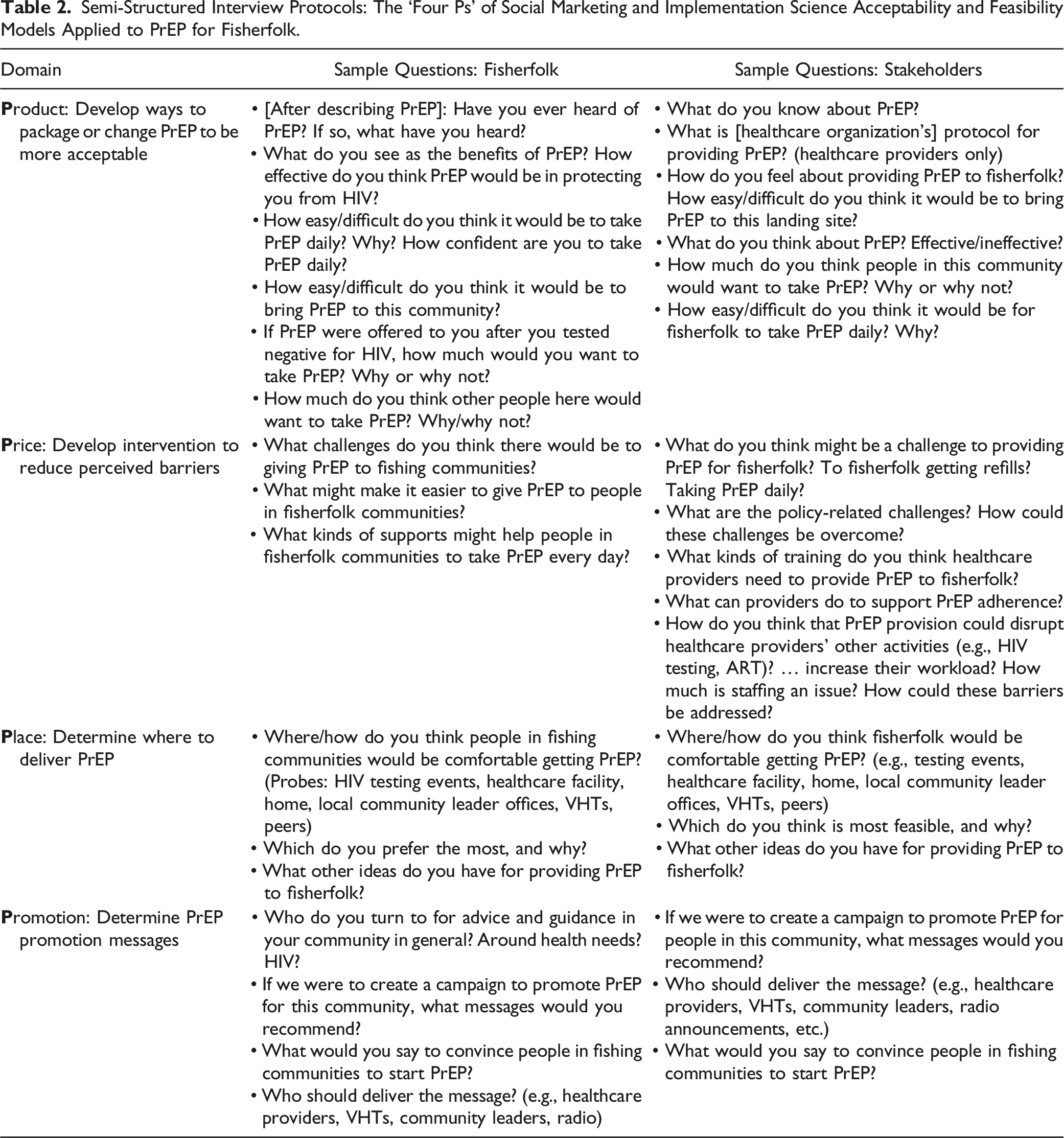
Interview Guide
Semi-Structured Interview Protocols: The ‘Four Ps’ of Social Marketing and Implementation Science Acceptability and Feasibility Models Applied to PrEP for Fisherfolk.
Analysis
Barriers to PrEP Implementation in Fisherfolk Communities by Social Marketing (‘Four Ps’) Theme.
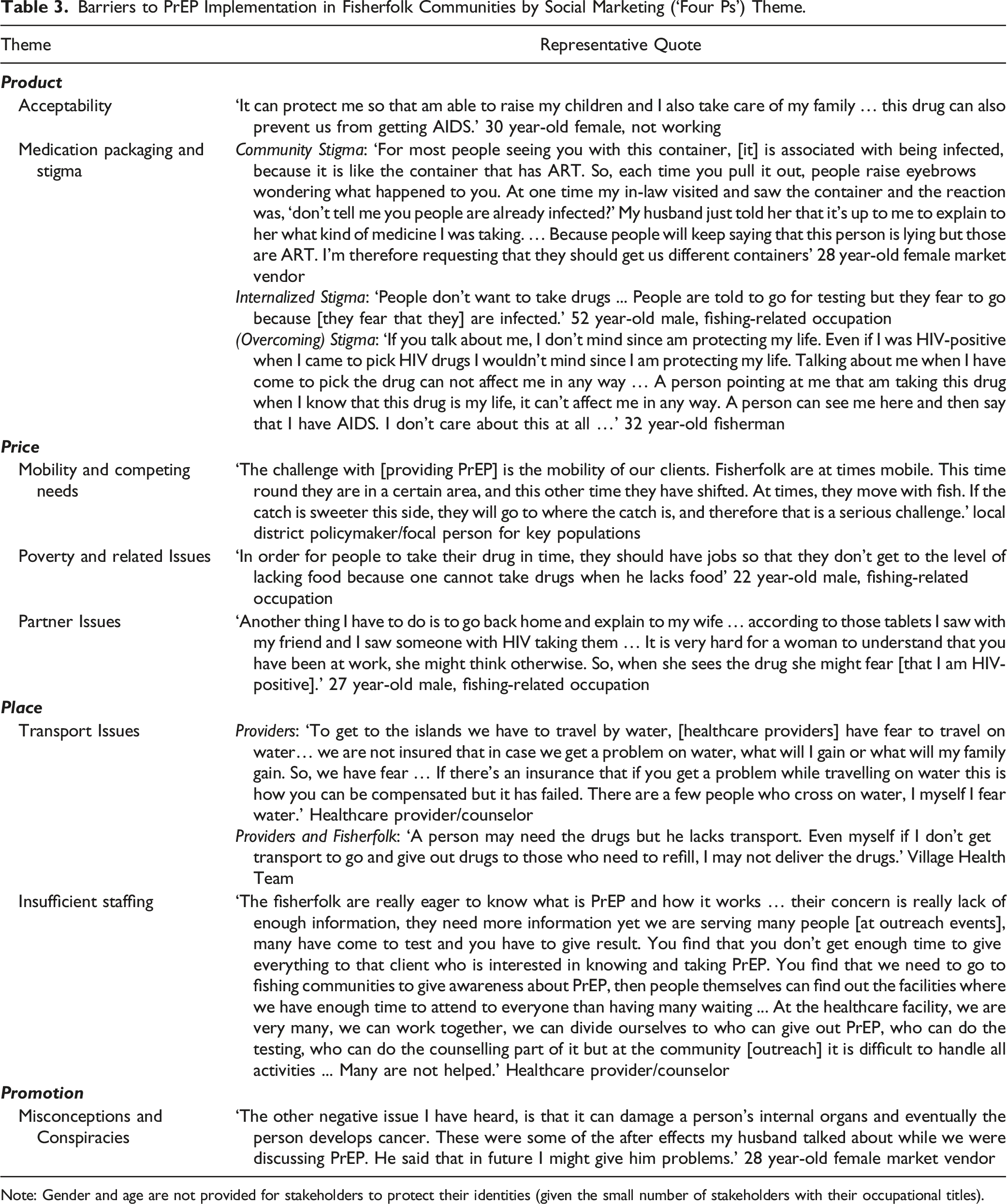
Note: Gender and age are not provided for stakeholders to protect their identities (given the small number of stakeholders with their occupational titles).
Results
Pre-Exposure Prophylaxis Barriers and Acceptability
Table 3 shows the themes and associated quotes for PrEP barriers and acceotability using the four Ps framework.
Product
Product refers to perceptions of PrEP itself and included positive attitudes about PrEP as well as PrEP-related stigma.
Overall Acceptability. Fisherfolk and stakeholders showed great enthusiasm and perceived need for PrEP, given high HIV rates in fisherfolk communities. Participants said that PrEP allows them to live healthy lives for their families and themselves, and reduces their stress and worry about HIV. Another advantage mentioned was that PrEP is not life-long, in contrast to HIV treatment. Several mentioned wanting to take PrEP because they love their life. Women mentioned being able to stay healthy and alive to raise their children, if their partner had multiple partners; men mentioned that PrEP allows for freedom to have multiple partners and keep themselves and their spouse safe.
Medication, Packaging, and Stigma Concerns. Across interviews, participants said that many fisherfolk thought that PrEP was for HIV treatment (and not prevention), because of the similar packaging of medications for PrEP and HIV treatment. Some fisherfolk also associated PrEP with stigmatized risk behaviours (e.g., sex work, multiple partners). Thus, people who took PrEP were at risk of being stigmatized. Fisherfolk referenced internalized stigma as discouraging people from HIV testing (and thus PrEP initiation) due to fear of discovering that they are HIV-positive. Some fisherfolk emphasized that stigma did not deter them from wanting to take (or actually taking) PrEP, because it was important to protect themselves.
Overall, fisherfolk who recently started (or who had previously taken) PrEP referenced similar barriers to PrEP use; some also discussed having side effects (e.g., bloating) or difficulty swallowing pills. Nevertheless, they remained willing to continue taking PrEP.
Price
We expanded the social marketing concept of price to include a range of barriers to getting and using PrEP (not only financial barriers).
Mobility and Competing Needs, combined with high alcohol use, were discussed across participants as challenges for traveling to get refills and for daily adherence. Some fisherfolk traveled far from designated PrEP refill pick-up locations. Fisherfolk said that inflexible or irregular ferry schedules, as well as weather-related issues, could impede them from reaching refill outreach events at designated times.
Among fishermen and related occupations, competing needs for work arose from the busy schedule of fishing and related activities (e.g., fish offloading and selling). Among women with families, competing needs manifested as daily shopping and childcare chores, and among female sex workers, competing needs meant being available when fishermen completed their daily work.
Poverty and Related Issues such as food insecurity were discussed as potentially contributing to nonadherence. Fisherfolk discussed not being able to take medications on an empty stomach or without access to clean water. Moreover, fisherfolk may not be able to afford transport costs to get refills.
Partner Issues included fear of conflict from partners suspecting infidelity or HIV-positive serostatus. Men and women discussed the potential for partner discord if their PrEP use were discovered, although more women seemed to have this concern.
Place
Place refers to where PrEP is provided.
Transport Issues contributed to Insufficient Healthcare Staffing. Healthcare providers, like fisherfolk, had difficulties with transport, including a lack of travel support (no insurance, hazard pay, life jackets, or funds for boat transport, which could be unsafe). In addition, local providers (such as VHTs) were not typically trained on PrEP and so could not answer PrEP users’ questions in between refills. These barriers contributed to an insufficient number of staff willing to travel to fisherfolk communities to explain and provide PrEP. Nevertheless, healthcare providers felt that PrEP’s benefits outweighed the challenges of delivering PrEP to fisherfolk communities, because managing ART for a patient who is HIV-positive is more challenging than administering PrEP.
Promotion
Promotion refers to education about PrEP with social marketing.
Misconceptions and Conspiracies. Although all fisherfolk had heard of PrEP, many, including those prescribed PrEP, were unclear about PrEP’s purpose, how and whether it works, and how it is intended to be taken, including when it can be discontinued. Misconceptions included that PrEP’s side effects are severe, PrEP is treatment for HIV, PrEP is experimental, PrEP can be stopped after 6 months, and PrEP is expensive. Many believed that PrEP should not be taken with alcohol. Conspiracy beliefs included that one can get cancer or HIV from PrEP. Fisherfolk felt social pressure not to take PrEP, due to such beliefs in their social networks. Among stakeholders, lack of awareness and misconceptions were viewed to be at least partially a result of PrEP not being explained adequately by healthcare providers.
Recommendations
The ‘Four Ps’ of Social Marketing Applied to Recommendations for PrEP Implementation for Fisherfolk.
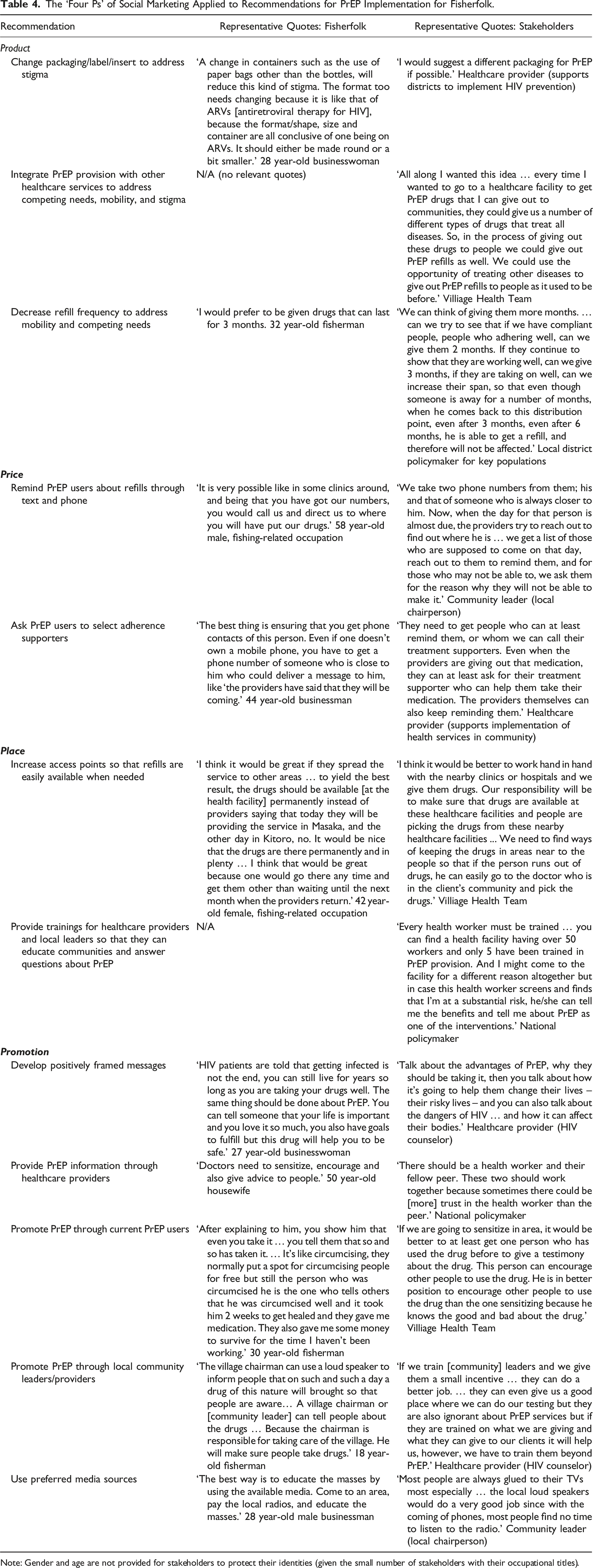
Note: Gender and age are not provided for stakeholders to protect their identities (given the small number of stakeholders with their occupational titles).
Product
To address stigma concerns around the association of PrEP to HIV, a major recommendation across interviews was to change PrEP medication packaging and use clear labels indicating that the medicine is for HIV prevention and not treatment. Furthermore, stakeholders suggested integrating PrEP and HIV testing services with other types of health-related services (e.g., immunization, family planning, sexually transmitted infection testing and treatment). In addition to addressing stigma concerns, such integration would help to address barriers related to mobility, transportation, and competing needs, given fisherfolk’s limited time and resources to visit healthcare. In addition, barriers about PrEP implementation could be addressed by decreasing PrEP refill frequency (e.g., monthly to every 3 months).
Price
To address barriers to getting refills and adhering to PrEP, participants suggested adapting strategies that are already used for community ART delivery and HIV treatment adherence. Fisherfolk suggested that healthcare providers could obtain the phone numbers of people on PrEP as well as their close contacts, such as a selected adherence supporter, so that they could text or call about the next refill date and place. For adherence, fisherfolk suggested counseling PrEP users to set a phone reminder or alarm, or ask a close friend or family member, such as an adherence supporter, to do so.
Suggestions also were made in terms of supplying transportation funds, a risk allowance, travel insurance, and lifejackets to providers, so that they could travel to islands safely to dispense PrEP. Transportation incentives for providers were seen as a better option than transportation incentives for PrEP users, as both stakeholders and fisherfolk said that getting transport funds did not guarantee that PrEP users would take the medications and may not be sustainable.
Place
An overall theme for PrEP implementation is that fisherfolk want multiple options and cannot have a one-size-fits-all approach. A key sentiment was that PrEP and refills need to be provided close to fisherfolk communities, to meet them where they work and live. Thus, local providers need to be trained to provide PrEP so that fisherfolk can obtain refills at additional places when they are traveling. Different acceptable options for PrEP implementation included getting refills at healthcare facilities, the local hospital, and/or healthcare outreach events. Fisherfolk were split on whether delivery directly (e.g., to homes or boats) would be acceptable. Some expressed stigma and privacy concerns, whereas others said that home delivery reduced the stigma of being seen at a healthcare facility or outreach event.
Promotion
Across interviews, participants suggested that the benefits of PrEP as preventing HIV need to be conveyed clearly and accurately. Fisherfolk suggested using positively framed messages that emphasize PrEP’s benefits beyond its efficacy, including that PrEP allows one to live a long healthy life with peace of mind, without worrying about HIV; using PrEP shows that you love your life; PrEP helps to protect you, your family and your community; and PrEP can be discontinued, but HIV and taking ART is life-long. Suggested media sources included radio and television advertisements, loudspeakers, edutainment, and DJs at outreach events, and posters with positively framed PrEP messages pinned at healthcare facility entrances and waiting areas, as well as in non-healthcare community locations. Fisherfolk felt that the likelihood of partner conflict around PrEP could be reduced if there were sufficient sensitization in fisherfolk communities, so that PrEP would be more understood and viewed positively—and thus less stigmatized.
Above all others, fisherfolk said that only trained healthcare workers (especially doctors) could be trusted to supply accurate information about PrEP. However, trainings for healthcare providers need to be tailored around unique issues in fisherfolk communities that might affect PrEP adherence and refill pick-ups, and include education about relevant subgroups and occupations (e.g., fishermen, fish sellers, sex workers), generally low literacy levels, risk factors (e.g., substance use, gender-based violence), and how to handle difficult and potentially unsafe situations (e.g., intoxication, violence, water travel).
Some fisherfolk said that they would trust VHTs and local leaders to mobilize communities for outreach events, if such individuals were sufficiently educated about PrEP. Fisherfolk and stakeholders suggested asking peer PrEP users (e.g., PrEP champions) to give testimonials about their experiences, to demonstrate that they have not suffered ill consequences or severe side effects. Such testimonials could help to reduce stigma.
Discussion
This qualitative study found high acceptability and anticipated feasibility of implementing oral PrEP in hyperendemic fishing communities in Uganda among multiple levels of stakeholders, including policymakers, healthcare providers, and community leaders, as well as potential and actual PrEP users themselves. We extended prior qualitative and quantitative research in Uganda fisherfolk communities, which has similarly found high PrEP acceptability and low knowledge. Prior research also has identified some of the same themes that emerged in the present study regarding anticipated barriers (e.g., stigma concerns, mobility, transportation, competing needs, partner conflict, and food insecurity among fisherfolk; understaffing among healthcare providers) and facilitators (perceived risk, closeness of services).7,19 Many of these barriers may affect PrEP adherence and continuation as well as, or perhaps more than, uptake—which may be why prior research on community-based ART delivery has found high PrEP acceptance yet high discontinuation. 28
The interview guide and analysis were structured around implementation science and social marketing frameworks. Thus, in addition to eliciting factors that impede or facilitate implementation, we heard recommendations for improved implementation strategies and specific key messages to use in PrEP public health campaigns. Our results provide a roadmap for PrEP implementation with interventions at multiple levels. At the policy level, changing PrEP packaging and labeling to indicate that pills are for HIV prevention (and not treatment) would be a major advance toward reducing stigma. Although not mentioned as a key theme in the interviews, as injectable PrEP becomes more widespread (along with less frequent healthcare visits), stigma as well as other barriers to adherence and refill receipt, such as mobility, may decrease. In addition, refills could be provided as part of general healthcare outreach events that are not specific to HIV services. However, such changes would not reduce community HIV stigma, but would allow PrEP users to be shielded from HIV stigma and the assumption by others that they are HIV-positive. To truly address stigma, as suggested by participants, community campaigns and discussions around PrEP, including PrEP user testimonials that normalize PrEP use, would be needed in tandem with packaging changes.
Our results suggest further intervention at the healthcare level to address fisherfolk’s mobility and competing needs: PrEP can be provided in multiple settings (in local healthcare facilities as well as outreach events), if local healthcare providers receive adequate training. In addition, as has also been recommended in prior research, 7 text and telephone reminders can be used to facilitate PrEP continuation as can adherence supporters; and at the community level, current PrEP users can provide credible advice, testimonials, and peer support around adherence. Such strategies have been effectively used to promote HIV treatment adherence29,30 and can be applied to PrEP as well.
Participants preferred positive framing for PrEP messages that promote PrEP as a way for themselves and their loved ones to live long and healthy lives without the stress of HIV. Prior research in sub-Saharan Africa and the U.S. has similarly indicated that PrEP is perceived to have mental health benefits.31,32 Such a positive perspective and will to live contrasts with prior research suggesting that fatalism contributes to fisherfolk’s HIV risk. 33 In the present study, participants tended to emphasize structural barriers related to work, poverty, and healthcare as contributing to PrEP acceptance and feasibility, more than individual-level barriers such as fatalism.
A limitation of the present study is the focus on two fishing villages on the shores of Lake Victoria in Uganda, both of which received PrEP through healthcare outreach events. Results may not generalize to other fisherfolk communities, such as islands, that are further from healthcare facilities that provide PrEP. Nevertheless, the sample showed high mobility, and many likely traveled to island communities throughout the year. Moreover, this study was conducted relatively early in the implementation of oral PrEP for fisherfolk communities in Uganda, at a time when only key and priority populations had access to PrEP. Misconceptions, stigma, and other barriers may decrease over time as PrEP is scaled up across the region, and when injectable PrEP becomes available. Overall, our findings can inform policymakers and healthcare organizations who strive to overcome barriers to PrEP and reduce HIV incidence in most at-risk populations.
Footnotes
Author’s Note
Bogart and Musoke are sharing first authorship, and Mukasa and Wanyenze are sharing senior authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health (P30MH058107, R34 MH119924).