
Abstract
A growing body of research has acknowledged the heterogeneity of subclinical social anxiety, identifying a subgroup of individuals who exhibit high levels of impulsivity. In a sample of Swedish early adolescents (N = 2,509, Mage = 13.64; 52.8% girls), we conducted latent transition analyses (LTA) to identify four classes of subclinical social anxiety-impulsivity across three time points. We identified a Low Social Anxiety-Low Impulsivity class, as well as a High Anxiety-High Impulsivity class for girls and boys, which had high levels of Time-4 internalizing problems. The latter class was less stable but larger for boys. There was also a more typical High Anxiety-Low Impulsivity class for both genders. Nevertheless, Low Anxiety-High Impulsivity girls and boys fared the worst in terms of both internalizing and externalizing problems later on. To our knowledge, this is the first study to adopt an LTA framework to investigate trajectories of early adolescent social anxiety-impulsivity over time.
Keywords
Subclinical social anxiety can be a problem for young people in their everyday lives, as it is related to social fears, worry and rumination about events, negative feelings, discomfort, and somatic symptoms such as trembling, blushing, and sweating before, during, and after social interactions (Heiser, Turner, Beidel, & Roberson-Nay, 2009). Typically speaking, the behaviors of shy, socially anxious individuals are characterized by inhibition and risk-avoidance (Lorian & Grisham, 2010). Nevertheless, a growing body of research has acknowledged the heterogeneity of social anxiety, identifying a small atypical subgroup of socially anxious individuals who also exhibit high levels of impulsive and novelty-seeking behaviors, alongside a large and more typical subgroup of socially anxious-inhibited individuals. This counterintuitive combination of high social anxiety and impulsivity has been identified in clinical populations of adults (Kashdan & McKnight, 2010; Kashdan, McKnight, Richey, & Hofmann, 2009; Mörtberg, Tillfors, van Zalk, & Kerr, 2014), as well as in subclinical populations of early adolescents (Tillfors, Van Zalk, & Kerr, 2013), young adults (Tillfors, Mörtberg, Van Zalk, & Kerr, 2013), and adults (Kashdan, Elhai, & Breen, 2008; Nicholls, Staiger, Williams, Richardson, & Kambouropoulos, 2014). One explanation for this link is that impulsive behaviors might be an atypical strategy for socially anxious individuals to regulate their emotions when feeling anxious.
Indeed, both inhibition and impulsivity might have a similar underlying function of avoiding negative effects in social situations. According to the limited self-regulatory resource theory (Baumeister, Gailliot, DeWall, & Oaten, 2006), not escaping an anxiety-provoking social situation costs a socially anxious person a great deal of self-control. Because self-control resources are limited, exhausting them is linked to an increase in automatic, impulsive behaviors. This notion has received some empirical support, as adults with high levels of both social anxiety and impulsivity show more problems with emotion regulation in fear-provoking social situations (Kashdan et al., 2008). Even if impulsive behaviors appear to be the opposite of inhibited behaviors, the underlying function might nevertheless be the same—that is, regulating negative inner experiences such as socially related negative thoughts and intense emotions.
In addition, compared to typically inhibited socially anxious individuals, those with the high social anxiety-impulsivity combination appear to have worse outcomes. Research on problem behaviors in clinical populations indicates that severity of substance use problems is greater in the impulsive subgroup compared to a low novelty-seeking group of socially anxious adults (Kashdan & Hofmann, 2008). High novelty-seeking, which is characterized by dislike of monotony and exploratory endeavors, is highly related to impulsivity (Kashdan & Hofmann, 2008). Studies on subclinical samples of socially anxious-impulsive adults show they have higher levels of risky behaviors such as aggression and drug use compared with adults low on novelty-seeking (Kashdan et al., 2008; Kashdan et al., 2009; Lipton, Weeks, Daruwala, & De Los Reyes, 2016). Undergraduates with elevated levels of social anxiety-impulsivity exhibit higher levels of coping-motivated drinking compared to those with low levels of impulsivity (Keough, Badawi, Nitka, O’Connor, & Stewart, 2016). Studies using adolescent and young adult samples are scarce, however. Higher levels of intoxication frequency and delinquency have been identified among socially anxious-impulsive boys (Tillfors, Van Zalk, & Kerr, 2013), whereas higher levels of depressive symptoms were identified among anxious-impulsive girls (Tillfors, Mörtberg, et al., 2013) compared to other social anxiety subgroups.
Early adolescence is a particular period of interest for studying the links between social anxiety and impulsivity. Symptoms of social anxiety typically emerge during early adolescence (Epkins & Heckler, 2011; Rapee & Spence, 2004; Spence & Rapee, 2016), with a number of studies showing increases in symptoms from childhood to adolescence (see Spence & Rapee, 2016, for a review of the current literature). Early onset of Social Anxiety Disorder (SAD; APA, 2013), of which social anxiety is a forerunner, typically emerges between 10 and 13 years and is related to later-life psychopathology to a higher degree compared to later onset SAD (Rapee & Spence, 2004). On a neurobiological level, a gap between the brain’s “break” and “gas” systems governing the ability to regulate emotions (based in the prefrontal cortex and the subcortical regions, respectively) is the largest during early adolescence compared to both childhood and adulthood, as early adolescents have an easier time to accelerate rather than slow down how they feel (Sommerville, Jones, & Casey, 2010; Tillfors & Van Zalk, 2015). The increased importance of peers and social interactions in young people’s lives, often paired with school transitions (Steinberg & Morris, 2001), also makes early adolescence a particularly sensitive period for those who are shy or socially fearful. In addition, problems with self-regulation or self-control, which can result in impulsivity, tend to appear early on in childhood. Children start to internalize social standards, inhibit actions they are not supposed to make, and start to monitor or regulate such actions as early as 3 to 4 years (Kopp, 1982). Nevertheless, early adolescence is typically accompanied by a rise in sensation-seeking, though causes of this might differ among adolescents—as individual differences in the equilibrium between cognitive executive function and impulsive tendencies likely distinguish those who become prone to risk (Romer et al., 2011). Because of the apparent rise of social anxiety and impulsivity during early adolescence, as well as previous work identifying a link between these two traits later on, more research is required for early adolescents in particular.
The majority of the studies focusing on identifying social anxiety subgroups have relied on cross-sectional data. There might be important subgroup fluctuations that are not captured at one point in time, but to our knowledge only two studies have examined the links between social anxiety and impulsivity using longitudinal samples of subclinical adolescents (Tillfors, Van Zalk, & Kerr, 2013) and early adults (Kashdan et al., 2008). None of these studies examined potential stability or changes in the heterogeneity of social anxiety, however, which requires moving beyond traditional cluster-analytic techniques. Individuals might transition from one problematic manifestation of social anxiety and impulsivity into another, making it important to adopt an approach that allows for capturing transitions as well as controlling for their stability over time. One such approach is latent transition analysis (LTA; Collins & Lanza, 2010), which allows for exploring changes in latent classes of individuals across time (Nylund, 2007). LTA is based on latent class analysis (LCA), which is a latent variable mixture model used as a measurement model to identify unique classes or subgroups of individuals at each separate time point in the analyses (Nylund, 2007). Overall, LTA allows for defining heterogeneous subgroups in a sample as well as modeling individual-level changes among the subgroups across time. It also allows for including distal outcomes related to the change process in transitions (Nylund, 2007). As such, LTA is preferable to commonly used cluster analytic approaches, which do not consider potential stability or change in subgroup membership nor links to later outcomes.
A significant factor to take into account regarding social anxiety-impulsivity concerns gender differences. First, girls tend to report higher mean levels of shyness/social anxiety during early and late childhood (Burgess, Wojslawowicz, Rubin, Rose-Krasnor, & Booth-LaForce, 2006; Crozier, 1995; Kim, Brody, & Murry, 2003; Lemerise, 1997) compared to boys. Nevertheless, boys likely have worse social consequences related to social fears due to gender stereotypes compared to girls (Kerr, 2000). That is, it is more acceptable for girls to exhibit shy, socially fearful behavior compared to boys. Second, gender differences regarding risk-taking, impulsive behaviors have also been reported, as boys tend to be more impulsive than girls, whereas girls exhibit higher levels of self-control compared to boys (Chapple & Johnson, 2007). Studies examining trajectories of social anxiety for girls and boys show that girls are more likely to be in classes characterized by moderate or high initial symptoms that subsequently decrease over time, whereas boys exhibit a more stable course of symptoms from middle to late adolescence (Ohannessian, Milan, & Vannucci, 2017). Thus, differences in both sizes and transitions of classes over time between the genders would be expected, though as far as we are aware this is yet to be tested for anxious-impulsive subgroups. Finally, previous findings indicate gender differences in outcomes for the atypical Anxious-Impulsive subgroup, as Anxious-Impulsive boys have reported higher levels of externalizing problems such as intoxication frequency compared to Anxious-Impulsive girls (Tillfors, Van Zalk, & Kerr, 2013). In a sample of Swedish young adults, however, Anxious-Impulsive as well as Anxious-Inhibited young women had higher levels of internalizing problems compared to Anxious-Impulsive young men (Tillfors, Mörtberg, et al., 2013). Because of these differences regarding both the effects and the consequences of social anxiety and impulsivity, we explored gender differences via separate analyses for girls and boys.
In this study, we conducted LTA to identify distinct subgroups based on subclinical social anxiety and impulsivity in a longitudinal sample of Swedish early adolescents. To start, we conducted separate LCAs for each time point separately for girls and boys, as we expected gender differences in class transitions as well as outcomes. The final class solutions from the separate LCAs were subsequently used to examine the longitudinal transitions between the classes in the final LTA models. Previous findings on Swedish adolescents using a standard clustering approach identified five subgroups of subclinical social anxiety and impulsivity for both boys and girls (Anxious-Inhibited, Impulsive, Anxious-Impulsive, No problems, and No problems/Low subgroups; Tillfors, Van Zalk, & Kerr, 2013). We therefore expected to identify similar patterns in the current data set. To examine long-term consequences of class transitions for girls and boys, we included internalizing and externalizing problems as distal outcomes (i.e., variables measured after the period of focus). Based on previously identified gender differences in mean levels as well as consequences of social anxiety and impulsivity, respectively, we expected Anxious-Impulsive girls to have high levels of internalizing problems, and Anxious-Impulsive boys to exhibit higher levels of externalizing problems over time.
Method
Participants
This study used data from the Three City Study, a longitudinal research program following adolescents from 18 public schools in three mid-sized communities in Sweden (supported by a grant from FORMAS, Swedish Research Council for Health, Working Life and Welfare, Swedish Research Council and Vinnova). The overarching aim of the project was to study adolescent risk and protective factors influencing later health. All of the data collections took place in schools with approximately 1 year between the time lags. The study included participants in seventh and eighth grade followed over time (who were subsequently in eighth and ninth grade at Time 2, in ninth grade and first grade of high school at Time 3, and in first and second grade of high school at Time 4). For this reason, there are variations across the time points in the number of participants (and available data), as changing to high school meant changing schools for the participants. Some participants left for high schools that were not participating in the Three City Study. The final analytical sample includes seventh to eighth graders at Time 1 (N = 2,509, Mage = 13.64; 52.8% girls), comprising 11.5% adolescents who were born outside of Sweden, and 71.4% who lived at home with both of their parents. This sample was followed up at Time 2 (N = 2,504, Mage = 14.80; 52.6% girls) and Time 3 (N = 1,875, Mage = 15.71; 53.5% girls). Those who were still taking part in the study at Time 4 provided information on distal outcomes (N = 1,382, Mage = 16.77; 53.3% girls). The percentage of missing values in the current data was computed using the “coverage” covariance matrix in MPlus (Muthén & Muthén, 1998-2012). The overall data coverage ranged for all study variables from .484 to .993 across all time points, indicating that there were between 48% and 99% of existing data for any given set of variables for the participants over time. We compared adolescents who did not participate at Time 2 (0.2%), Time 3 (44.7%), or Time 4 (45%) with those who remained throughout the study (45.6% across all time points) on all demographic and study variables. None of the variables predicted dropout at any subsequent time point.
Procedure
In order to participate in the study, adolescents had to provide active consent and their parents had to provide passive consent. At Time 1, parents of 3,336 pupils were sent a letter with information about the study. Of those, 122 (3.6%) returned a prepaid envelope with a signed form declining their child’s participation. The adolescents provided active consent before partaking in the study, after being informed that participation was voluntary. The combination of active participant and passive parent consent is common in developmental studies, as it helps reduce sampling bias (Shaw, Cross, Thomas, & Zubrick, 2015). A total of 446 adolescents (13.4%) either declined to participate or were absent on the day of the first data collection, resulting in a sample of 2,768 (83%) at Time 1 (a number higher than the final analytical sample for this study, as not all of those had viable data for the current project). For this study, we included seventh to eighth graders who had available data at Time 1 for variables of interest (N = 2,509, Mage = 13.64; 52.8% girls). The adolescents were told about the types of questions they would answer and the time it would take to finish the questionnaires. They were also informed that their participation was voluntary, that they could do something else instead if they chose to, and that their answers would never be shown to anyone if they chose to participate. The adolescents filled out the questionnaires administered by trained research assistants in classrooms, with no teachers present during the data collection. They were given 90 minutes and provided with snacks. Each class received 300 SEK (Swedish Krona) for taking part. The data collection procedure was the same for the remaining time points. All of the procedures and measures in the study were approved by the Regional Ethics Board in Uppsala (no. 2013/384). All measures were delivered in Swedish. Measures of social anxiety, delinquency, intoxication frequency, and drug use were originally written in Swedish. All of the other measures have been translated and validated in Swedish (as well as back-translated in English) during pilot testing prior to start of the study.
Measures
Social anxiety
Social anxiety was measured using the Social Phobia Screening Questionnaire (SPSQ; Furmark et al., 1999), adjusted for children and adolescents up to age 18 (the SPSQ-C, or the Social Phobia Screening Questionnaire for Children; Gren-Landell, Tillfors, et al., 2009). This instrument has shown a moderate test–retest reliability (r = .60) in a validation study (Gren-Landell, Björklind, et al., 2009). The measure comprises eight questions about how much fears the adolescents felt in various social situations, such as “speaking in front of the class,” “going to a party,” and “being with classmates during breaks.” The response items ranged from None (1), Some (2), to A lot (3). Cronbach’s αs were .73 for Time 1, .76 for Time 2, and .80 for Time 3.
Impulsivity
Impulsivity was measured with 11 items about urgency, which is a subscale from the UPPS impulsive behavior scale (Whiteside & Lynam, 2001). The original measure includes 12 items, but only 11 items were included in the current data collection due to human error (the item “I have trouble controlling my impulses” was excluded). Examples of items were “I have trouble resisting my cravings (e.g., for sweets),” “I often get involved in things I later wish I could get out of,” and “When I feel bad, I will often do things I later regret in order to make myself feel better.” The Urgency subscale has shown good reliability in previous research (Cronbach’s α = .89), as well as a high level of correspondence with other measures of impulsivity (Lynam, Hoyle, & Newman, 2006). The response items range from Don’t agree at all (1), Don’t particularly agree (2), Agree pretty well (3) to Agree completely (4). Cronbach’s αs for this study were .87 for Time 1, .87 for Time 2, and .88 for Time 3.
Distal outcomes
Several indicators of internalizing and externalizing problems were used as distal outcomes at Time 4 in the final LTA models. Mean scores of depressive symptoms and anxiety were used to indicate internalizing problems, whereas mean scores of delinquency, intoxication frequency, and drug use were used as indicators of externalizing problems.
Depressive symptoms
Depressive symptoms were measured using the 20-item Child Depression Scale from the Center for Epidemiological Studies (CESD; Radloff, 1977). This scale assesses depressive symptoms such as worry, sadness, hopelessness, lethargy, and poor appetite and has demonstrated good factorial validity (Cheng, Chan, & Fung, 2006). Participants were instructed to think about the past week. Examples of statements were as follows: During the past week, “I felt like I was too tired to do things,” “I didn’t feel like eating/I wasn’t very hungry,” and “I was more quiet than usual.” The response items ranged from Not at all (1), A little (2), Some (3), to A lot (4). Cronbach’s α was .92 for Time 4.
Anxiety
Anxiety was measured using five questions from the Overall Anxiety Severity and Impairment Scale (OASIS; Norman, Cissell, Means-Christensen, & Stein, 2006). This scale was originally developed for use in adult populations, with the language slightly adapted to fit adolescents. Examples of items were “In the past week, when you have felt anxious, how intense or severe was your anxiety,” “In the past week, how often did you avoid situations, places, objects, or activities because of anxiety or fear,” and “In the past week, how much did your anxiety interfere with your ability to do the things you needed to do at work, at school, or at home?” This measure has shown robust correlations with other global as well as disorder-specific measures of anxiety in a validation study (Campbell-Sills et al., 2009). The response items ranged from Not at all (1), Rarely (2), Now and then (3), Often (4) to A lot (5). Cronbach’s α was .90 for Time 4.
Delinquency
Delinquency was measured using seven items about norm-breaking behavior (updated in Kerr & Stattin, 2000; Magnusson, Dunér, & Zetterblom, 1975). The entire scale comprises items about norm-breaking and violence (including contact with the police), but the latter items were excluded as the focus for this study were more commonly occurring norm-breaking behaviors in early adolescence. The questions refer to the past 6 months. Examples of items were “Have you taken things from a store, stand, or shop without paying,” “Have you taken money from home that didn’t belong to you,” and “Have you taken part in threatening or forcing someone to do something that he or she didn’t want to do?” This measure has shown a robust correlation with parental measures of delinquency in previous research (r = .43; Kerr & Stattin, 2000). The response items ranged from No, never (1), Once (2), 2-3 times (3), 4-10 times (4), to More than 10 times (5). Cronbach’s α was .77 for Time 4.
Intoxication frequency
There was one item measuring intoxication frequency. The participants were asked whether they’d had so much beer, liquor, or wine that they got drunk—during the past 6 months (Koutakis, Stattin, & Kerr, 2008; Van, Zalk, Kerr, & Tilton-Weaver, 2011). This one-item indicator of intoxication has been used successfully in previous studies (Koutakis et al., 2008; Tillfors, Van Zalk, & Kerr, 2013; Van Zalk et al., 2011). The response items ranged from No, never (1), Once (2), 2-3 times (3), 4-10 times (4), to More than 10 times (5).
Drug use
The participants were asked whether they had used any drugs other than pot (marijuana, cannabis) during the past year. The response items ranged from No, never (1), Once (2), 2-3 times (3), 4-10 times (4), to More than 10 times (5).
Analytic Strategy
The data were analyzed using Mplus 7.0 and a combination of LCA and LTA, which allows for the operationalization of continuous variables into latent categorical variables (Collins & Lanza, 2010). This modeling procedure is according to previous recommendations about LTA (Collins & Lanza, 2010; Nylund, 2007). As a first step, LCA identified classes of social anxiety and impulsivity at three time points. As a second step, we used LTA, which is a longitudinal extension of LCA and helps identify mutually exclusive latent statuses of individuals in classes across time (Cleveland, Lanza, Ray, Turrisi, & Mallett, 2012; Collins & Lanza, 2010). Thus, LTA allows for stage-sequential testing of individual growth (Graham, Collins, Wugalter, Chung, & Hansen, 1991). What distinguishes LTA from other trajectory-based models is that classes (or statuses) identified are not assumed to be stable per se, although they might be. Individuals are therefore allowed to change class membership over time. For that reason, LTA lends itself well when examining changes from one state to another over time, such as for example transitioning into different levels of social anxiety and impulsivity. Full Information Maximum Likelihood (FIML) estimation was used for all models, which approximates information about missingness in the dataset via all available data (Enders, 2010; Little, 2013). By doing so, FIML provides less biased results than both pairwise and listwise deletion (Little, 2013).
Generally speaking, the LTA model comprises a measurement model for the latent class variables at each time point, as well as a structural model that links the latent class variables to each other (Collins & Lanza, 2010). In addition, the model estimates the latent class prevalence and the latent transitions while adjusting for measurement error (Collins & Lanza, 2010). In this article, the LTA model is based on a final chosen number of classes derived from LCAs conducted separately for girls and boys at each of the three time points. The final choice of classes per time point is described in more detail in the “Results” section. Models using distal outcomes at Time 4 (i.e., mean levels of internalizing and externalizing problems) were run as a final step in the analyses.
The FIML procedure calculates maximum likelihood parameter estimates and standard errors for any specified model by using all available information provided in the observed data (Enders & Bandalos, 2001). This technique is appropriate to use when the data are not missing completely at random or missing at random (MCAR or MAR; Schafer & Graham, 2002). Little’s MCAR test indicated that our data were not missing completely at random (χ2 = 387.37, df = 299, Sig. = .000), as would be expected due to the study design with participants changing schools from Time 2 to Time 3 and onward. Because both intoxication frequency and drug use were highly skewed (as would be expected for a sample of early adolescents), the maximum likelihood estimation parameter (MLR) was used in all analyses, which has been recommended when using variables with non-normal distributions (Muthén & Muthén, 1998-2012). Pairing FIML with maximum likelihood estimation (MLR) results in unbiased parameter estimates even with large amounts of missing data, missing time points in longitudinal studies, or under MAR assumptions (Enders & Bandalos, 2001).
Results
Descriptives
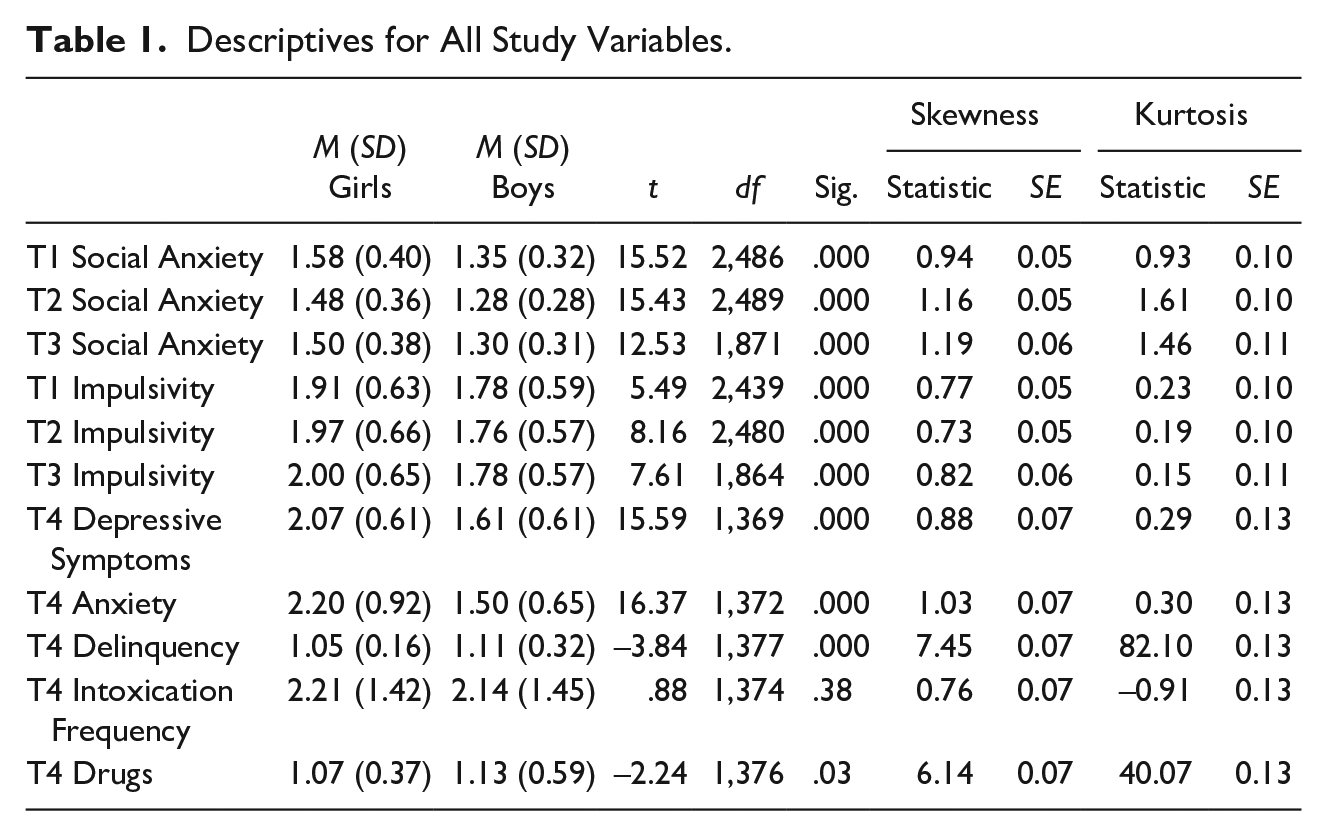
The descriptives and correlations for all study variables are shown in Tables 1 and 2, respectively. Compared to boys, girls had significantly higher levels of social anxiety, impulsivity, depressive symptoms, and anxiety over time. Higher levels of internalizing problems including social anxiety, anxiety, and depressive symptoms would be expected for girls from the current literature (Cummings, Caporino, & Kendall, 2014). Contrary to the previous literature (Chapple & Johnson, 2007), however, girls had higher levels of impulsivity compared to boys. According to expectations (e.g., Moffitt & Caspi, 2001), boys had higher levels of delinquency compared to girls. There were no significant differences between boys and girls on drinking and drug use. In addition, there were positive correlations between most study variables, whereas social anxiety was negatively correlated with delinquency, drinking, and drug use over time.
Descriptives for All Study Variables.
Correlations (N’s) Between All Study Variables.
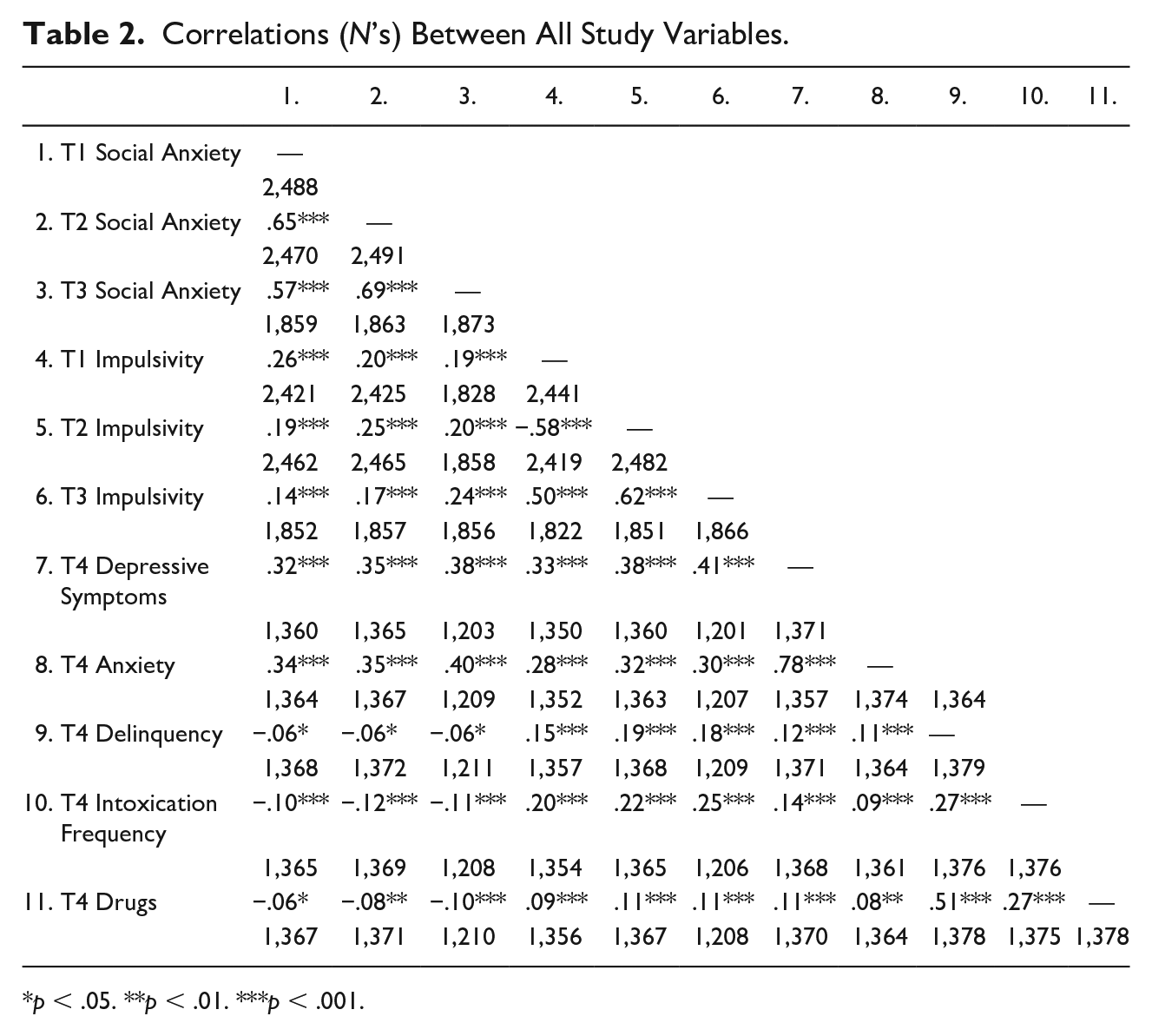
p < .05. **p < .01. ***p < .001.
Identifying Concurrent and Longitudinal Classes of Anxious-Impulsive Early Adolescents
First step: Cross-sectional LCAs
To explore social anxiety-impulsivity classes, a set of cross-sectional LCAs were estimated for each of the three time points and separately for boys and girls. Multiple starting values were employed, as previously recommended, to replicate the maximum likelihood value (Collins & Lanza, 2010). The number of classes were thus not determined a priori but were empirically derived from the data. Consequently, this approach warrants the most optimal fit of potential social anxiety-impulsivity subgroups to the current data.
Based on theoretical considerations and previous findings about social anxiety-impulsivity subgroups, we tested up to six class solutions for each time point. A number of criteria were used to determine the final number of latent classes (Muthén & Muthén, 2000; Nylund, Asparouhov, & Muthén, 2007). First, a decrease in the Bayesian Information Criterion (BIC; Schwarz, 1978) and the Akaike Information Criterion (AIC; Akaike, 1974) indicate an improvement in model fit comparing a solution with k classes to a solution with k − 1 classes. Second, the Vuong-Lo-Mendel Rubin likelihood ratio test (LMR LRT) should indicate a significant increase of fit compared to the previous class solution (Nylund et al., 2007). Third, the entropy values (ranging from 0 to 1) should be .70 or higher, to indicate good classification accuracy (Reinecke, 2006). Fourth, a more parsimonious model solution (k − 1 classes) should be favored, providing that a less parsimonious model poses a minor variation of an already identified class. Fifth, each class should preferably represent at least 5% of the sample so as to make the latent transition analyses viable (for more details, see Speece, 1994). And finally, the classes need to make theoretical sense and be interpretable. The final chosen class solutions that met the above criteria (except representing at least 5% of the sample) are presented in Table 3. As the table shows, a 4-class solution was superior to all others at all time points for both boys and girls—contradicting previous research identifying five classes (Tillfors, Van Zalk, & Kerr, 2013). The 4-class solution had lowered levels of BIC and AIC, significant increases in LMR MRT for almost all time points, entropy levels of over .70, and overall parsimoniousness. As the table shows, a class with high levels of social anxiety-impulsivity was identified at each time point for both boys and girls (marked in bold). However, this class was only 2% for girls at Time points 1 and 2 but increased to 6% at Time 3. For boys, this class was small at Time 1 (2%) but increased to 5% at Time 2 and 4% at Time 3. Previous research has shown this class to comprise 4% of girls and 2% of boys in a Swedish early adolescent sample, nevertheless (Tillfors, Van Zalk, & Kerr, 2013). Based on these criteria, the 4-class solution was found to be preferable and was used in the subsequent LTA analyses described below.
Descriptives for Final Class Solutions for Separate Gender LCAs at Time Points 1 to 3.
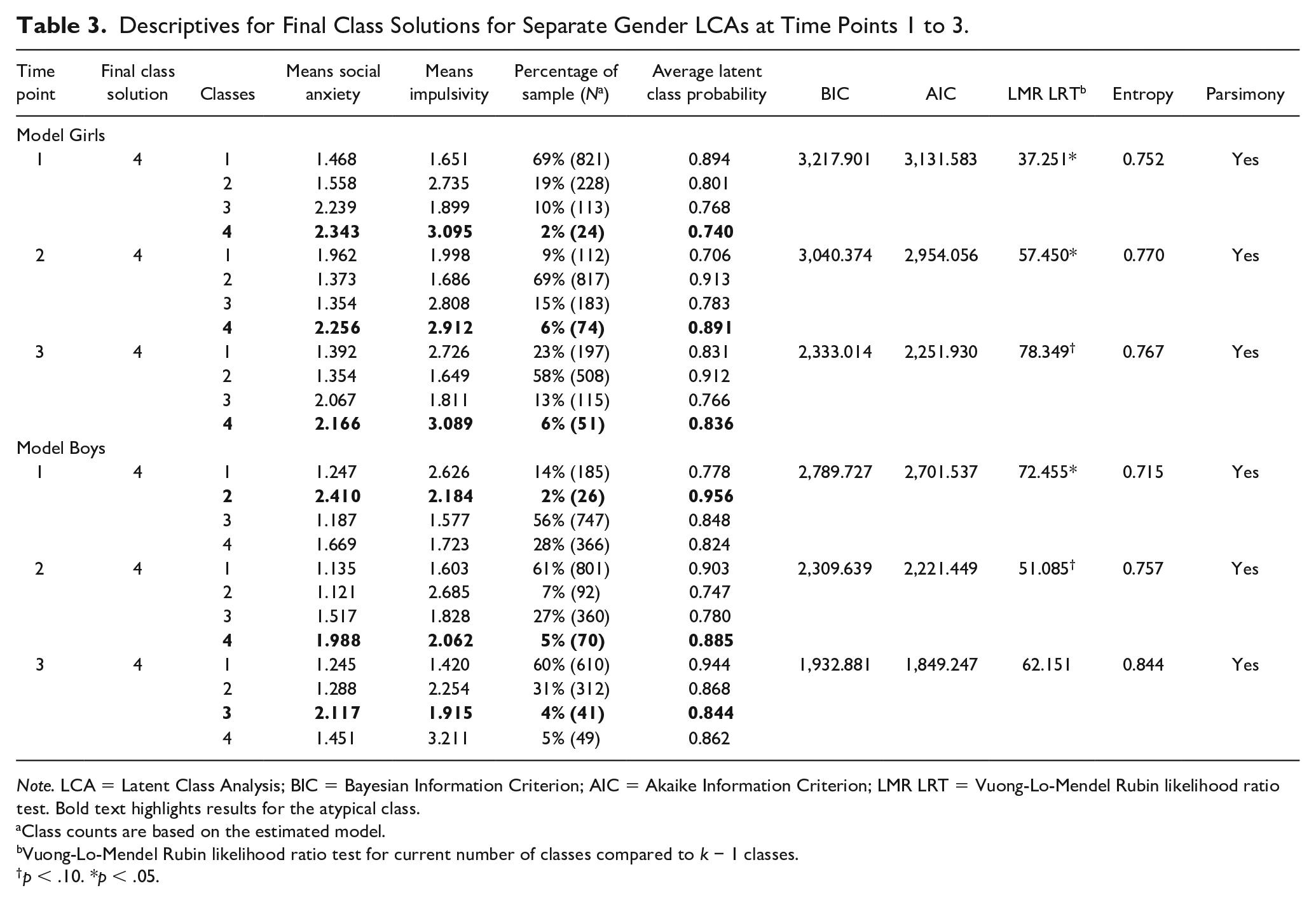
Note. LCA = Latent Class Analysis; BIC = Bayesian Information Criterion; AIC = Akaike Information Criterion; LMR LRT = Vuong-Lo-Mendel Rubin likelihood ratio test. Bold text highlights results for the atypical class.
Class counts are based on the estimated model.
Vuong-Lo-Mendel Rubin likelihood ratio test for current number of classes compared to k − 1 classes.
p < .10. *p < .05.
Second step: Longitudinal LTAs
Next, we used the specified numbers of classes obtained from the separate LCAs in initial LTAs without distal outcomes and separately for genders. This is a necessary step to specify a baseline model before adding outcome variables (Nylund, 2007). Because each Time 2 row of the latent class transition matrix is conditioned on Time 1 latent classes (the same principle applies for Times 2-3), the latent transition analyses represent changes in social anxiety and impulsivity over time. Again, multiple starting values were employed so as to replicate the Maximum Likelihood value (Collins & Lanza, 2010). These models replicated the ML values from the separate LCAs for girls and boys (Loglikelihoodgirls = −3,454.828; AICgirls = 7,023.65; BICgirls = 7,132.020; Loglikelihoodboys = −2,775.272; AICboys = 5,664.543; BICboys = 5,960.283).
Comparing Girls and Boys in the Different Classes on Internalizing and Externalizing Outcomes
We related the Time-4 distal outcomes (internalizing and externalizing problems) to the latent class membership at Time 3 in the girl and boy models, respectively (Loglikelihoodgirls = −4,553.574; AICgirls = 9,241.147; BICgirls = 9,581.340; Loglikelihoodboys = −3,938.840; AICboys = 8,011.679; BICboys = 8,359.303). Internalizing problems were based on a mean score of depressive symptoms and anxiety (Mgirls = 2.156 and Mboys = 1.552), whereas externalizing problems were based on a mean score of delinquency, intoxication frequency, and drug use (Mgirls = 1.465 and Mboys = 1.479). Mean scores were chosen over single variables or latent constructs on the basis of the typically very large degrees of freedom required by LTA models, as well as common non-identification problems (Collins & Lanza, 2010). The inclusion of distal outcomes changes the estimation of the LTA model parameters (Nylund, 2007). The descriptives for the final LTA classes with distal outcomes are shown in Table 4, whereas the latent class transition probabilities for the final LTAs with distal outcomes are shown in Table 5 for girls and Table 6 for boys, respectively. Class/subgroup names were derived from how they related to mean levels of social anxiety and impulsivity at each time point (i.e., low, average, or high). Wald test of parameter estimates was used to examine whether the means of internalizing and externalizing problems differed significantly among the classes (Nylund, 2007).
Descriptives for Girls’ and Boys’ LTA Classes for Three Time Points (for Final Model With Distal Outcomes).
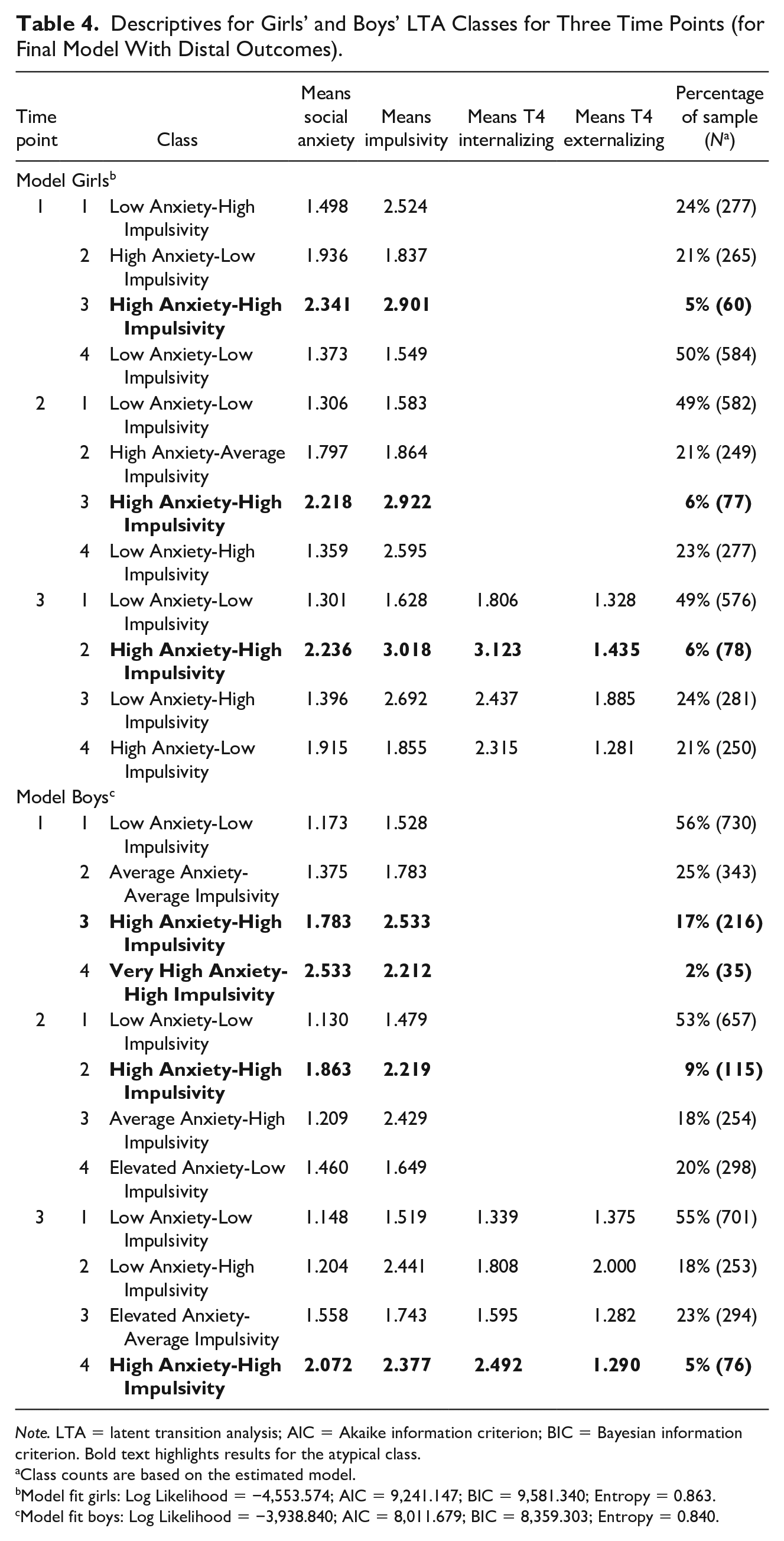
Note. LTA = latent transition analysis; AIC = Akaike information criterion; BIC = Bayesian information criterion. Bold text highlights results for the atypical class.
Class counts are based on the estimated model.
Model fit girls: Log Likelihood = −4,553.574; AIC = 9,241.147; BIC = 9,581.340; Entropy = 0.863.
Model fit boys: Log Likelihood = −3,938.840; AIC = 8,011.679; BIC = 8,359.303; Entropy = 0.840.
Girls’ Latent Transition Probabilities From Final Model With Internalizing and Externalizing Problems as Outcomes.
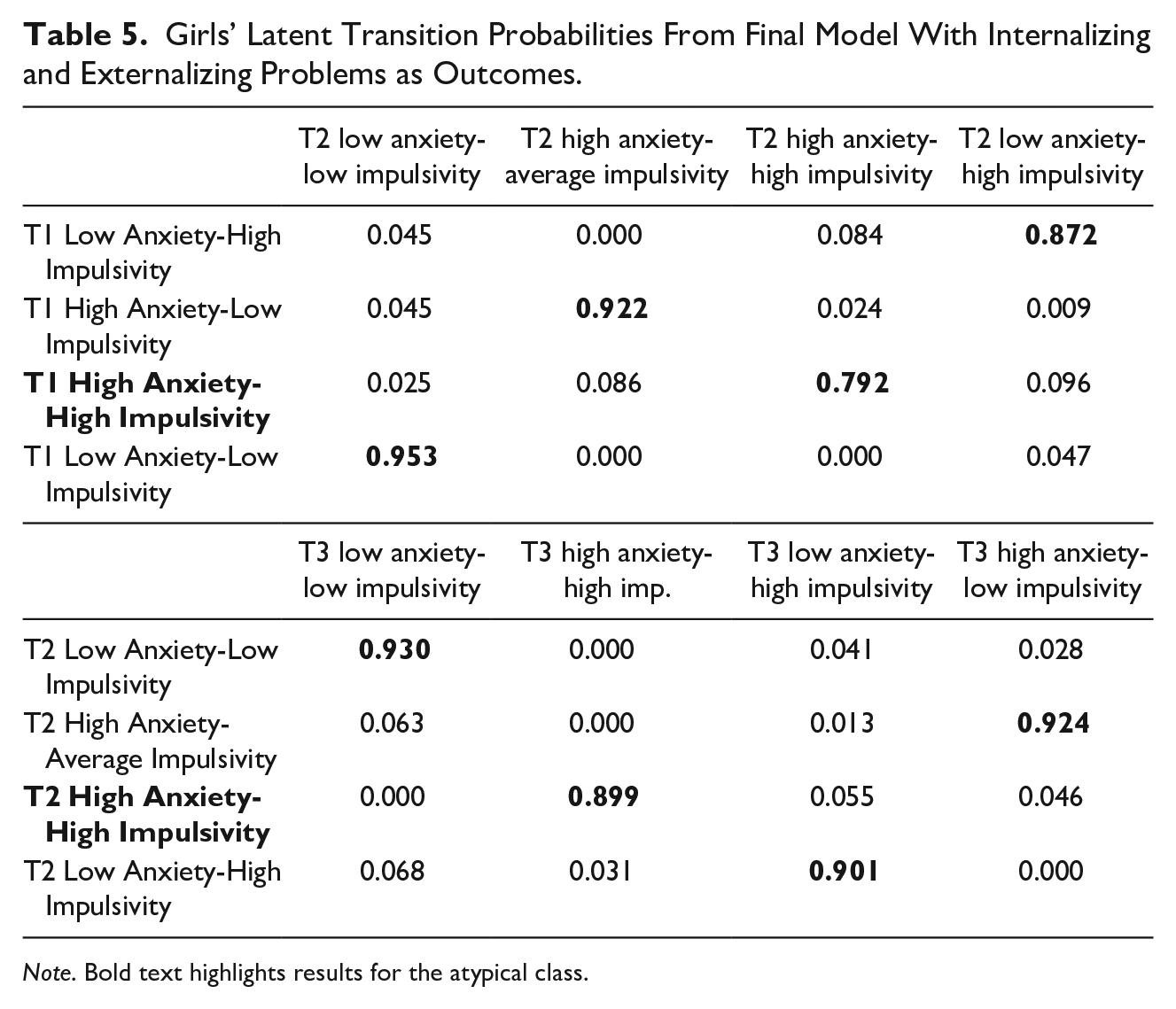
Note. Bold text highlights results for the atypical class.
Boys’ Latent Transition Probabilities From Final Model With Internalizing and Externalizing Problems as Outcomes.
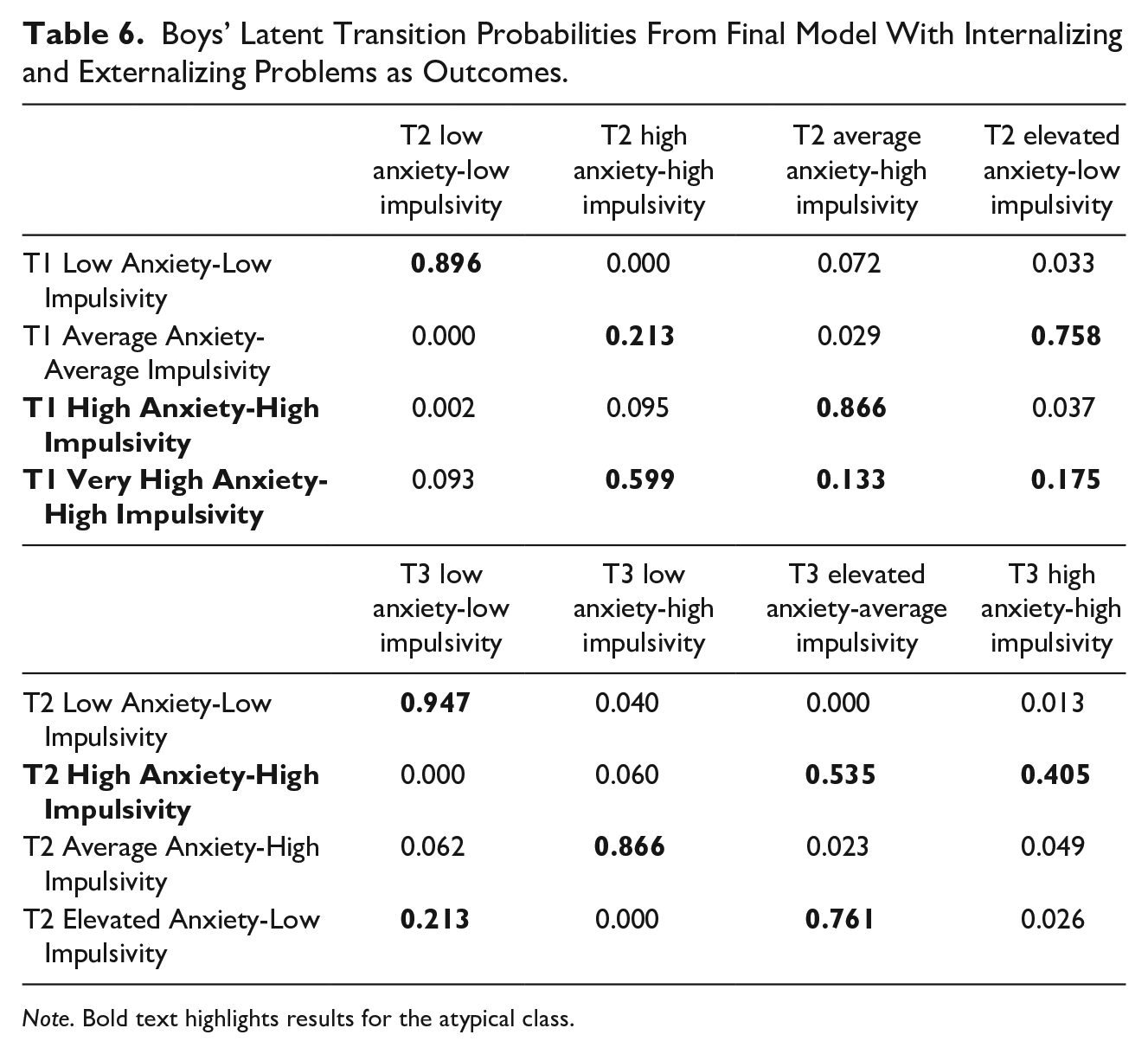
Note. Bold text highlights results for the atypical class.
LTA results for girls
As can be seen from the upper part of Table 4, the largest subgroup identified at Time 1 (50%) for girls was a Low Anxiety-Low Impulsivity class. As Table 5 shows, girls in this class had a 95% and a 93% probability of transitioning into the same class at Times 2 and 3, respectively. This was the most stable class across the time points, and girls in this class had average levels of internalizing and low levels of externalizing problems at Time 4 (as shown in Table 4). There was also a typical High Anxiety-Low Impulsivity class at Time 1 (comprising 21%), where girls had a 92% probability of transitioning into a High Anxiety-Average Impulsivity class at Time 2, followed by a 92% probability of transitioning into a High Anxiety-Low Impulsivity class at Time 3. Thus, girls in this class tended to retain high levels of anxiety across time (with slight variations in levels of impulsivity), and this trajectory predicted high levels of internalizing and low levels of externalizing problems at Time 4.
We also identified an atypical High Anxiety-High Impulsivity class at Time 1 (comprising 5%), where girls had a 79% and a 90% probability of transitioning into the same class at Times 2 and 3, respectively. Some girls in the atypical class had a 9% probability of transitioning into the High Anxiety-Average Impulsivity class, and a 10% probability of transitioning into the Low Anxiety-High Impulsivity class at Time 2. Similarly, some girls in the atypical class at Time 2 had a 5% probability of transitioning into the High Anxiety-Low Impulsivity class, and a 6% probability of transitioning into the Low Anxiety-High Impulsivity class at Time 3. Thus, some girls in the atypical class had a small probability of either developing high levels of social anxiety or high levels of impulsivity later on. Overall, however, this trajectory was relatively stable for girls across the three time points. Being in the atypical class at Time 3 predicted very high levels of internalizing and average levels of externalizing problems at Time 4. The final class identified was a Low Anxiety-High Impulsivity class at Time 1 (comprising 24%), where girls had an 87% and a 90% probability of transitioning into the same class at Times 2 and 3, respectively. The girls in this trajectory had high levels of both internalizing and externalizing problems at Time 4. The Wald test of parameter estimates indicated significant differences between all of the internalizing and externalizing problems across all of the classes (Wald = 247.033; df = 6; p < .00001).
LTA results for boys
The lower part of Table 4 shows means, whereas Table 6 shows their latent transition probabilities across the first three time points. Boys in the Low Anxiety-Low Impulsivity class at Time 1 (comprising 56%) had a 90% and a 95% probability of transitioning into the same class 1 and 2 years later, respectively. Just like for girls, this was the most stable trajectory for boys across time, and these class transitions predicted low levels of both internalizing and externalizing problems at Time 4. There was also an Average Anxiety-Average Impulsivity class at Time 1 (comprising 25%), where boys had a 76% probability of transitioning into an Elevated Anxiety-Low Impulsivity class, and a 21% probability of transitioning into a High Anxiety-High Impulsivity class at Time 2. Nevertheless, the Average Anxiety-Average Impulsivity class was not identified at either Times 2 or 3.
Just as for girls, we also identified a High Anxiety-High Impulsivity class at Time 1 (comprising 17%—a much larger percentage compared to girls). Boys in this class had an 87% probability of transitioning into an Average Anxiety-High Impulsivity class, and a 10% probability of transitioning into a similar High Anxiety-High Impulsivity class at Time 2. In turn, boys in the High Anxiety-High Impulsivity class at Time 2 had a 41% probability of transitioning into the same class, or a 54% probability of transitioning into an Elevated Anxiety-Average Impulsivity class at Time 3. Boys in the Average Anxiety-High Impulsivity class at Time 2, on the other hand, had an 87% probability of transitioning into a Low Anxiety-High Impulsivity class at Time 3. Thus, for boys, there was more change in the atypical High Anxiety-High Impulsivity class across time compared to girls. Finally, we also identified a Very High Anxiety-High Impulsivity class at Time 1 only (comprising 2%). Boys in this class had a 60% probability of transitioning into the High Anxiety-High Impulsivity class, a 13% probability of transitioning into the Average Anxiety-High Impulsivity class, and an 18% probability of transitioning into the Elevated Anxiety-Low Impulsivity class at Time 2. The Very High Anxiety-High Impulsivity class was not identified later on. Generally speaking, boys’ trajectories across the classes were less stable compared to girls, as indicated by more movement and diversity over time.
Regarding outcomes, boys who had transitioned into the Low Anxiety-High Impulsivity class at Time 3 had high levels of both internalizing and externalizing problems at Time 4. Thus, just like for girls, highly impulsive boys with low social anxiety were worse off compared to all other classes. Those who had transitioned into the Elevated Anxiety-Average Impulsivity group at Time 2 had low levels of internalizing and externalizing problems a year later. Finally, and similarly to girls, boys who had transitioned into the atypical High Anxiety-High Impulsivity class at Time 3 had very high levels of internalizing, but low levels of externalizing problems at Time 4. The differences between the Time-4 means across the classes were significant, as indicated by the Wald test of parameter estimates (Wald = 102.914; df = 6; p < .00001). Contrary to previous findings, then, boys in the atypical Anxious-Impulsive class developed internalizing rather than externalizing problems, whereas highly impulsive boys were worse off in terms of both internalizing and externalizing problems later on.
Discussion
A growing literature has identified a small and uncharacteristic subgroup of highly socially anxious individuals who are also impulsive among clinical adults (Kashdan & McKnight, 2010; Kashdan et al., 2009; Mörtberg et al., 2014), and subclinical early adolescents (Tillfors, Mörtberg, et al., 2013; Tillfors, Van Zalk, & Kerr, 2013) as well as adults (Kashdan et al., 2008; Nicholls et al., 2014). Using a subclinical longitudinal sample of Swedish early adolescents (NT1 = 2,509, Mage = 14.80; 52.6% girls), we expected to identify similar subgroups of social anxiety-impulsivity, including the atypical Anxious-Impulsive subgroup. Based on previous findings, we also expected the girls in this subgroup to demonstrate high levels of internalizing problems, whereas Anxious-Impulsive boys were expected to exhibit high levels of externalizing problems later on. Unlike previous studies with subclinical samples of adolescents identifying five subgroups (e.g., Tillfors, Van Zalk, & Kerr, 2013), we found four classes of social anxiety-impulsivity at each time point for girls and boys, respectively. This might be explained by the nature of the LTAs, which, although building on cross-sectional LCAs as a first step, subsequently take into account both stability and change of anxious-impulsive classes over time. Previous longitudinal studies have examined concurrent subgroups/clusters at separate time points, making result comparisons challenging. Conducting LTAs across three time points with internalizing and externalizing problems as distal outcomes at Time 4, we found a large stable trajectory of low social anxiety-impulsivity for both genders, as would be expected. Adolescents in this subgroup had the lowest average levels of both internalizing and externalizing problems later on. For both genders, we also identified a High Anxiety-High Impulsivity class at Time 1. This class was more stable for girls, as they were more likely to transition into the same class at Times 2 and 3—which was associated with higher levels of Time-4 internalizing problems in particular. This class was larger but less stable for boys, as they transitioned into average levels of social anxiety over time. Nonetheless, a Very High Anxiety-High Impulsivity class was also identified at Time 1 only, where boys had a high probability of transitioning into the High Anxiety-High Impulsivity class over time. Contrary to our expectations based on previous studies (but similar to previous findings for girls), this trajectory was linked to more internalizing problems at Time 4 for boys. Interestingly, the subgroup that fared the worst in this study were girls and boys who were low on anxiety but high on impulsivity, as they reported high levels of both internalizing and externalizing problems at Time 4. To our knowledge, this is the first study to adopt a latent transition framework to study trajectories of social anxiety-impulsivity over time.
The current results further support a growing literature showing that social anxiety is not defined merely by typically shy, inhibited behavior, but also by impulsivity—albeit for a small proportion of individuals. This finding is in line with Cloninger’s psychobiological model of personality, where a temperament factor identified in early childhood characterized by novelty-seeking was found to be relatively predictive of later behavior (Cloninger, Svrakic, & Przybeck, 1993). Another way of explaining this counterintuitive trait combination is via the limited self-regulatory resource theory (Baumeister et al., 2006). Many social interactions involve activities which require self-regulation, such as for instance impression management (Vohs, Baumeister, & Ciarocco, 2005). Not being able to escape an anxiety-provoking social situation would cost socially anxious individuals a lot of self-control (Baumeister et al., 2006), and draining such limited resources could give rise to increases in automatic, impulsive behaviors over time. If socially anxious individuals frequently experience fearful situations, therefore, they would likely be at higher risk for exhausting their self-control, which in turn might lead to higher impulsivity for some. According to the results from this study, this would be true for a small subset of adolescents with subclinical social anxiety. Social anxiety paired with impulsivity has indeed previously been linked with engaging in risky externalizing problems such as substance use (Kashdan & Hofmann, 2008), as well as drug use, unsafe sex, and aggression (Kashdan et al., 2008; Kashdan et al., 2009) for adults. Anxious-Impulsive girls as well as boys in this study primarily had high levels of internalizing problems (anxiety and depressive symptoms) a year later, however, which could be a sample- or an age-specific effect. Considering a general lack of previous longitudinal investigations of social anxiety-impulsivity subgroup transitions in early adolescence, more research on other longitudinal samples and age cohorts is required to corroborate the current findings.
There were some surprising findings in this study. First, girls had significantly higher mean levels of impulsivity than boys, which is contrary to previous literature. Generally speaking, boys reported lower means for all study variables except externalizing problems. This could be explained by a bias in self-reporting, as boys might be prone to self-promote externalizing but downplay internalizing in general. Boys might not feel as comfortable admitting anxious and depressive vulnerabilities compared to delinquency, alcohol intoxication, and drug use (or they might simply not even be aware)—a challenge perhaps reflected later in adulthood when men are less prone to seek help for internalizing compared to women because they find it difficult to recognize and communicate internalizing symptoms (Seidler, Dawes, Rice, Oliffe, & Dhillon, 2016). In addition, even though we expected the Anxious-Impulsive boys to be worse off in terms of externalizing problems (based on previous findings), both Anxious-Impulsive boys and girls had primarily high levels of internalizing problems later on. In contrast, Anxious-Impulsive boys, but not girls, had higher levels of externalizing problems compared to boys in other anxiety–impulsivity subgroups in a previous Swedish sample (Tillfors, Van Zalk, & Kerr, 2013). This could be explained by different measures of impulsivity used across studies. In the aforementioned study, the authors used a measure taken from an instrument created to assess psychopathic traits (Tillfors, Van Zalk, & Kerr, 2013), whereas this study used a measure developed to gauge urgency-impulsivity in general (Whiteside & Lynam, 2001). Previous work might have therefore captured individuals with antisocial tendencies as well. In addition, this study identified four subgroups of early adolescents based on social anxiety and impulsivity across 3 years, which might help explain the difference in findings compared to the previous literature. Our results could also be explained by high variation in transition trajectories for boys in particular, whereas previous literature has not examined stability of these subgroups over time (and lower stability in boys’ subgroups would indicate higher level of changes in anxious-impulsive traits compared to girls). More research on stability and changes in anxious-impulsive traits is required for both genders.
This study has some limitations that should be noted. First, the more extreme Very High Anxiety-High Impulsivity class for boys was very small at Time 1 (2%), which is under the recommended value of at least 5% of the sample when evaluating model fit (Speece, 1994). Compared to a 3-class or a 5-class solution, however, the 4-class solution at Time 1 for boys was chosen based on its interpretability, parsimoniousness, as well as fulfilling all other model fit criteria. In addition, this subgroup had a high probability of transitioning into the High Anxious-High Impulsive subgroup across time, which comprised a higher number of boys. Another limitation is the period between the time lags, which were 1 year in this study. Scholars have pointed out that both the timing and spacing of observations in longitudinal design might have an impact on which conclusions can be drawn from the data (Collins & Graham, 2002). When the time between observations is long compared to how rapidly transitions might occur, transitions might happen between measurement occasions. Thus, we might have missed important transitions—though how and when these happen is currently unclear, considering the scarce longitudinal literature on heterogeneity of social anxiety-impulsivity. Predicting social anxiety-impulsivity transitions might be more accurate in the future with more frequent or differently timed measurements. In addition, the measure of intoxication frequency relied on only one item, with more items being preferable in terms of reliability and validity. Nevertheless, the measure as such has been used in previous research as an indicator of how much adolescents drink (Koutakis et al., 2008; Van Zalk et al., 2011). Finally, as in most longitudinal studies, there were missing data across the time points due to participant attrition. The study used a longitudinal design following participants over time from 18 public schools. Due to the structure of the Swedish educational system, participants in the seventh and eighth grades would have changed schools when transitioning into high school at Times 2 and 3, respectively. Thus, depending on where the participants moved (i.e., whether they went to one of the high schools that were participating in the Three City Study), data attrition was inevitable (as is the case for most longitudinal designs). Despite the high rates of attrition for certain variables at later time points, removing participants without complete data from the statistical analyses would result in bias or lack of statistical power (Little, 2013). Using an estimation approach such as FIML is less biased than both of those options, as it relies on all information to inform parameter values and standard errors in the model (Little, 2013). Despite its limitations, nevertheless, the study has several strengths, such as the size of the early adolescent sample as well as its longitudinal design. Girls and boys were followed over a period of 4 years, with three time points serving as basis for identifying latent transitions of social anxiety-impulsivity subgroups, whereas changes in latent transitions predicted levels of internalizing and externalizing problems at Time 4. As such, this study is unique in the current literature, which has mainly relied on cross-sectional samples, with the majority of studies focused on adults. Because social anxiety tends to develop during early adolescence (Epkins & Heckler, 2011; Rapee & Spence, 2004), our results expand the understanding about its heterogeneity during early emergence.
Social anxiety is not only an unpleasant experience in itself but is also linked to individual impairment. The links between social anxiety and problem behavior are many and far-reaching, during adolescence as well as later on in life. For instance, adolescent social anxiety is associated with low peer acceptance (Erath, Flanagan, Bierman, & Tu, 2010), increased peer victimization (Siegel, La Greca, & Harrison, 2009), poor relationships with parents (Van Zalk & Kerr, 2011), and high levels of loneliness (Stoeckli, 2010). During early and late adulthood, social anxiety is linked with high levels of alcohol consumption as means of self-medication (Ham & Hope, 2005), few and low-quality friendships (Leary & Buckley, 2000), low self-esteem, poor attitudes about one’s appearance, low life satisfaction, less positive affect (Kerr, 2000), and poor career prospects—especially for men (Kerr, Lambert, & Bem, 1996). Subclinical levels of social anxiety are also forerunners of SAD, as well as other mood and substance-use disorders later on in life (Tang et al., 2017), and studies indicate a high prevalence of clinical levels of social anxiety in Western populations, with rates varying between 2.7% and 15.6% depending on country and culture (Furmark et al., 1999). The typical assumption about socially anxious individuals is that they are shy and socially fearful—yet a budding literature (including this study) shows that social anxiety can co-occur with high levels of impulsivity for a small number of individuals. In addition, our results show that this trait combination is relatively stable over time. Although the combination of social anxiety-impulsivity is contrary to common expectations, it could be particularly problematic in terms of long-term implications such as driving socially anxious adolescents into situations resulting in increased risk for depression or anxiety in general. This heterogeneity has implications for both policy and practice, showing that not all socially anxious adolescents are in a similar risk zone for developing problems further ahead. These findings also imply that a strong co-occurrence between social anxiety and depressive symptoms might be partially explained by the presence of impulsivity, and these links are particularly strong for girls. For girls, exhibiting impulsive behaviors is likely less accepted than for boys, which could help explain differences in outcomes between boys and girls with social anxiety-impulsivity.
Identifying patterns of data (i.e., using a person-oriented rather than a variable-oriented approach) is a useful methodological tool for the study of interindividual differences (Bergman, Magnusson, & El-Khouri, 2003). A person-oriented approach emphasizes a holistic-interactionist view of human development, as individuals are expected to exhibit different patterns of mental, biological, and behavioral factors operating at all levels of individual functioning (Bergman et al., 2003). Importantly, being socially anxious and impulsive appears to be linked to various negative outcomes over time. Risk-prone behavior can be adaptive in the short term by helping to reduce anxiety via for instance taking drugs, but can be detrimental in the long term and compromise individual’s well-being and social adjustment (Kashdan & McKnight, 2010). Because of the (expectedly) small number of people in the atypical anxious-impulsive subgroup, it is likely to go undetected by those whose job it is to help alleviate anxiety, such as mental health professionals (Kashdan & McKnight, 2010). Understanding heterogeneous behavior patterns of young people with elevated levels of social anxiety and impulsivity is therefore crucial if we are to help prevent potentially negative consequences of this counterintuitive trait combination. Using a person-oriented approach such as LTA allows for understanding these processes for subgroups of individuals, rather than focusing on population averages (as most studies do). If practice is to become more personalized toward creating unique outcomes on an individual basis, longitudinal person-oriented approaches will have to be more widely adopted to increase understanding about development and change in psychopathology.
Footnotes
Acknowledgements
This study used data from the “Three Cities Study,” a longitudinal research project at the Department of Law, Psychology, and Social Work at Örebro University, Sweden. We gratefully acknowledge the support of pupils, teachers, parents, and principals who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by a shared grant from FORMAS, Swedish Research Council for Health, Working Life and Welfare (FORTE), Swedish Research Council (VR) and Vinnova (grant number 2012-65).