
Abstract
Acute exercise has been shown to transiently improve specific aspects of cognitive function, however the mechanism governing these effects remain unclear. Blood pressure responses during exercise have been hypothesized to be a primary contributing factor, in part through its influence on cerebral blood flow. In this counterpoint, we highlight the inconsistent and weak associations between changes in blood pressure, cerebral blood flow and cognitive responses during and following acute exercise. Despite sound theoretical foundation, cognitive responses to exercise do not appear strongly related to blood pressure and more likely stem from a complex integration of multiple mechanisms.
There has been longstanding interest in the benefits of regular exercise on brain health and cognitive function. Epidemiological evidence regarding regular exercise and exercise training on brain health has driven interest in the acute effects of exercise on cognitive function under the premise that acute responses may contribute to long-term adaptation. 1 The exact mechanisms governing the effects of acute exercise on cognitive function remain elusive. 1 Recently, Washio et al. 2 noted greater blood pressure responses during isometric hand grip exercise were associated with attenuated acceleration/slowing of reaction time (RT) during a post-exercise go/no-go task. These data add to the inconsistent literature examining associations between cardiovascular and cognitive responses to exercise and revived debate over whether changes in blood pressure dictate exercise-induced changes in cognitive function.
If blood pressure responses to exercise modulate cognitive function, then increases in blood pressure during exercise should be associated with improved cognition during exercise. We note no association between changes in mean arterial pressure (MAP) and cognitive function, assessed as accuracy and RT on executive function (Flanker, 2-back tasks) or memory tasks (memory recognition), during moderate intensity aerobic exercise (Figure 1, panel a, secondary analysis of Lefferts et al. 3 ). It is possible that greater exercise blood pressure responses could attenuate post-exercise cognitive benefits (as seen in Washio et al. 2 ), rather than cognitive function during exercise. Existing data, however, suggest 1) compared to light intensity-, acute moderate-to-vigorous intensity exercise requires a larger pressor response and elicits larger beneficial effects on post-exercise cognitive function, and 2) individuals who experience greater blood pressure during aerobic exercise (e.g. adults with hypertension) exhibit similar beneficial effects of acute exercise on post-exercise cognitive function. 4 We also leveraged our prior acute exercise data in 60 middle-aged adults4,5 and observed no association between changes in MAP during aerobic exercise and post-exercise changes in cognitive function (Figure 1, Panel c). Cumulatively, these observations suggest that blood pressure responses during exercise do not appear related to changes in cognitive function during or following acute exercise.
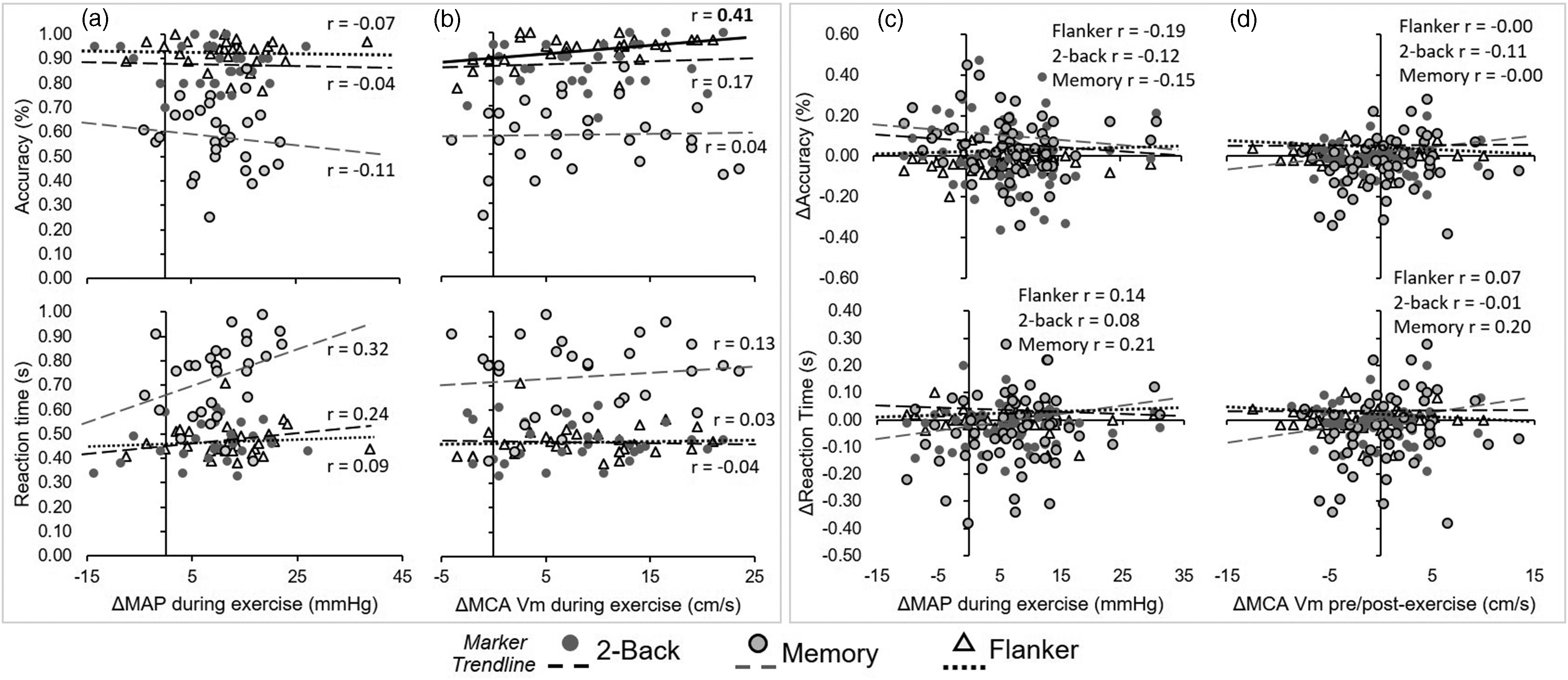
Association between cognitive function during exercise and (a) changes in mean arterial pressure (MAP) and (b) middle cerebral artery (MCA) mean blood velocity (Vm) in young healthy adults (n = 29); and associations between post-exercise changes in cognitive function and (c) changes in MAP during exercise, and (d) changes in post-exercise MCA Vm during cognitive testing in middle-aged adults (n = 59). Bold Pearson correlation coefficient (r) and solid trend line denote significant linear association, p < 0.05.
An alternative perspective could posit that blood pressure responses during exercise might be positively, or indirectly, associated with improvements in cognitive function through modulation of cerebral blood flow, a key mechanism governing cognitive function. 6 Unfortunately, although cerebral blood flow is linked with cognitive function under resting conditions, their relationship with exercise remains unclear. 7 Our data suggest changes in MAP during aerobic exercise are not consistently associated with the change in middle cerebral artery (MCA) mean blood velocity (only associated in one (p = 0.052) of three cognitive tasks during aerobic exercise, unpublished observations from Lefferts et al. 3 ). Although increases in MCA mean blood velocity were associated with greater attention performance during aerobic exercise (r = 0.41, p < 0.05; Flanker task), no associations were seen with working memory or memory recognition task performance (Figure 1, Panel b). Indeed, most studies have not observed direct associations between cerebral blood flow and cognitive function during aerobic exercise, 8 including those that eloquently manipulate blood flow to test relations with cognitive function.6,7,9 These data suggest that although theoretically linked, relations between cerebral blood flow and cognitive function during exercise are tenuous.
Exercise-induced increases in blood pressure could also contribute to post-exercise cognitive function by modulating post-exercise cerebral blood flow. Although we are unaware of any original investigations of this nature, secondary analyses of our prior work4,5 suggest that changes in MCA mean blood velocity during post-exercise cognitive tasks are positively related to exercise workload (r = 0.37–0.28, p = 0.01–0.03) but not change in MAP (r = −0.03–0.10, p = 0.46–0.81) during aerobic exercise. Ultimately, changes in MCA mean blood velocity from pre- to post-exercise cognitive task are not associated with changes in cognitive performance within our data and it is not uncommon to see disparate changes in blood flow and cognitive function post-exercise. 10 These observations suggest the beneficial effects of acute exercise on cognitive function are not strongly related to post-exercise changes in cerebral blood flow.
Adequately assessing cognitive function is difficult and could confound the ability to detect relations between hemodynamic exercise responses and cognitive function. Although changes in RT and accuracy are the most readily available parameters from behavioral cognitive tasks, they are not necessarily strictly indicative of performance. 4 Currently, much of the literature relies on interpreting accelerated RT (often during very simple cognitive tasks) 2 as improved cognitive function. RT, however, encompasses visual encoding of the stimuli, the actual decision-making process (explicit cognitive processing), and motor response.3,4 Our work using novel drift-diffusion modeling indicate that accelerated RT post-exercise may stem from changes in visual encoding and motor response, rather than the decision making process itself. 4 As such, whether accelerated RT truly indicates improvements in cognitive processing, rather than simply accelerated motor response from the motor cortex or sympathoexcitatory/arousal pathways, remains questionable. Caution should be used when interpreting singular associations between changes in cognitive function and specific candidate mechanisms. Associations between a mechanism (e.g. blood pressure) and singular specific cognitive outcome after exercise (e.g. RT on a Flanker task) does not mean the candidate mechanism is critical for all cognitive exercise responses. Cognitive exercise responses and their relation to blood pressure/cerebral hemodynamics may be specific to the cognitive task-/domain and type of exercise (aerobic, isometric vs dynamic resistance, high-intensity interval), and modulated by individual-level characteristics (fitness, age, sex, genetics, health status [e.g., impaired cerebral hemodynamics or autoregulation]), however these remain under-examined. Identifying relations between exercise-induced changes in blood pressure, cerebral blood flow, and cognitive function are further complicated by cerebral autoregulation, which contains inherent asymmetry (e.g. hysteresis) and may regulate blood flow differently during different types of exercise (steady-state aerobic vs high-intensity interval, static vs dynamic resistance exercise). Ultimately, the beneficial cognitive response to acute exercise likely stems from multiple, integrated mechanisms that include: 1) increases in cerebral blood flow that stimulate release of neurotrophic factors (e.g., brain-derived neurotrophic factor) from cerebral endothelial cells, 2) enhanced neural activation of motor/sensory systems, 3) sympathoexcitation/arousal, and 4) increased circulating hormones and neurotransmitters (e.g., norepinephrine, acetylcholine, dopamine, serotonin). 1 The particular mechanism in a specific scenario may additionally differ between exercise types, modalities, and intensities and be further modified by individual subject characteristics.
In conclusion, although blood pressure and its relations with cerebral blood flow remain feasible mechanistic contributors to post-exercise cognitive function, empirical support for their links with post-exercise cognitive function appear inconsistent and tenuous. Future work examining mechanisms behind acute exercise-induced cognitive benefits should strengthen their methodological approach by integrating behavioral cognitive and neurophysiological measures (e.g. drift-diffusion modeling, pre-motor time via EMG, EEG, cerebral blood flow, etc.) and accounting for latent aspects of cognitive function that influence RT and accuracy on post-exercise cognitive tasks.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data presented herein were funded in part by the American College of Sports Medicine (Foundation Research Grant, WKL), American Heart Association (Predoctoral Fellowships 16PRE31220031, WKL), and Joan N. Burstyn Endowed Fund for Collaborative Research in Education at Syracuse University (WKL)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.