
Abstract
Nearly all stroke neuroprotection modalities, including selective intra-arterial cooling (SI-AC), have failed to be translated from bench to bed side. Potentially overlooked reasons may be biological gaps, inadequate attention to reperfusion states and mismatched attention to neurological benefits. To advance stroke translation, we describe a novel thrombus-based stroke model in adult rhesus macaques. Intra-arterial thrombolysis with tissue plasminogen activator leads to three clinically relevant outcomes – complete, partial, and no recanalization based on digital subtraction angiography. We also find reperfusion as a prerequisite for SI-AC-induced benefits, in which models with complete or partial reperfusion exhibit significantly reduced infarct volumes, mitigated neurological deficits, improved upper limb motor dysfunction in both acute and chronic stages; however, no further neuroprotection is observed in those without reperfusion. In summary, we discover reperfusion as a crucial regulator of SI-AC-induced neuroprotection and provide insights of long-term functional benefits in behavior and imaging levels. Our findings could be important not only for the translational prerequisite and potential molecular targets, but also for this thrombus-thrombolysis model in monkeys as a powerful tool for further translational stroke studies.
Keywords
Introduction
Ischemic stroke is still a leading causes of death and disability worldwide.1,2 Despite significant advances in increased intravenous tissue plasminogen activator (tPA)/alteplase as well as the more recently approved endovascular thrombectomy modalities, many stroke patients remain severely disabled.3,4 A meta-analysis from recent clinical trials has also shown that approximately 50% patients still have severe disability or die at 90 days despite mechanical thrombectomy (MT) treatment. 5 Thus, it is imperative to explore adjunctive approaches to minimize infarct volume and improve neurological outcomes in ischemic stroke.6,7 However, there has been a long history of failed clinical trials of neuroprotection in stroke. This failure may be attributed to a series of key mismatches between preclinical and clinical stroke research, including but not limited to biological gaps, unbalanced attention to reperfusion states, and disaccord in functional evaluation. 8 For example, there are significant differences between rodent models and patients in brain size, anatomy, and compositions. Additionally, preclinical studies mainly rely on infarct size for treatment effects, while clinical trials pay much attention to long-term functional outcomes.
Therapeutic hypothermia is considered as a robust neuro-protectant to improve clinical outcomes due to multiple synergistic effects on decreasing brain tissue injury from ischemia and reperfusion, but, its clinical use has largely been limited due to reasons such as delayed cooling onset, prolonged duration to achieve a lowered core temperature, as well as significant side effects.9,10 Recent preclinical studies have found that a fast and short-term hypothermia exerts better neuroprotective effects on all cell types in the neurovascular unit. 11 Long-term benefits of local hypothermia have also been reported in rodent focal ischemia models owning to better preservations of white matter.12,13 Previous studies have shown that the infusion of cold saline, i.e. selective intra-arterial cooling (SI-AC), is a feasible technique for inducing local hypothermia during endovascular treatment of intracranial occlusion and confers neuroprotection in rodent stroke models.14,15 More recently, our team has shown that SI-AC combined with endovascular recanalization can be safely achieved in acute ischemic stroke patients. 16 However, we fail to demonstrate improvements in functional outcomes with SI-AC treatment because of inhomogeneous patients’ characteristics, a relatively lower cooling volume, and potential patient selection bias. 17 We need a standardized evaluation of SI-AC in higher order nonhuman primates (NHPs) models.
NHPs model has been clearly recommended by the Stroke Therapy Academic Industry Roundtable (STAIR) group to improve a fast and successful translation of neuroprotectants. 18 Hence, this study is designed to develop a novel thrombus-thrombolysis model in rhesus monkeys in order to conduct a prospective pre-clinical trial to test the safety and utility of SI-AC in focal cerebral ischemia and bridge gaps between bench and bed side.
Material and methods
Animals
A total of 50 adult male rhesus monkeys (Macaca mulatta), aged 7–11 years old and weight 7.0–10.6 kg, were used in this study. All animals were screened and were free of Tuberculosis, Shigella, Salmonella, Helminths, Ectoparasites, Entamaebahistolytica and B virus. The monkeys were caged individually in stainless steel cages in the same room. They were fed with commercially prepared monkey food twice daily with fruits and unrestricted water supply. This study was approved by the Animal Use and Care Board of the Institute of Laboratory Animal Sciences, Capital Medical University. All experiments were also in compliance with national guidelines and in accordance with the Guide for the Care and Use of Laboratory Animals. 19 All experiments reported are in compliance with the ARRIVE guidelines. Animal information has been provided in the supplementary data with parameters including age, weight and infarct side.
Clot preparation
As described previously by us in NHPs models and in rodents, clot was made by the blood from the femoral vein.20,21 An autologous clot measuring 10 cm in length was used for embolization.
Anesthesia
Animals were fasted for 12 h prior to the induction of anesthesia. Anesthesia was initiated and maintained as described previously by us in NHPs models. 20
Endovascular surgery
As described previously by us in NHPs models, a Prowler-10 micro-catheter (Codman) with a SilverSpeed™-10 Hydrophilic micro-wire was introduced into the guiding catheter and navigated to the distal end of M1 segment of the right MCA. Next, the clot was transferred into micro-catheter and flushed into the end of M1 segment with 2 mL saline. 20
IA thrombolysis and SI-AC
There is no standardized protocol for intra-arterial (IA) t-PA administration in acute ischemic stroke, especially in NHPs. We used alteplase (Boehringer Ingelheim Limited) for IA thrombolysis based on established protocols, in which the full t-PA dose was infused did not exceed 0.9 mg per kilogram of body weight (maximum, 90 mg for patients with a body weight of ≥100 kg).22,23 The conversion of drug doses between species based on surface area is a commonly used first-pass “estimated” approach, then 1.1 mg/kg is adopted in this study.24,25 SI-AC was done as described in our previous study. 15 In brief, a total of 100 mL of iced lactated Ringer’s solution (0–4°C) was infused into the MCA vessel vascular distribution over 20 min (5 mL/min) via the micro-catheter.
Assessment of recanalization
Cerebral angiography was performed at various time points: (1) before thrombus injection; (2) before t-PA thrombolysis; (3) 10 min after t-PA. Based on reports in NHPs and ischemic stroke patients, recanalization was scored over three grades: no recanalization or complete occlusion at the main trunk of M1-MCA; partial recanalization or complete recanalization at the main trunk of M1-MCA, but no recanalization at M2-MCA branch; complete recanalization and no occlusion at both M1-MCA trunk and M2-MCA branch.22,26
MRI scanning
MRI scanning was performed on a Magnetom Trio MRI Scanner (3.0 T; Siemens AG, Siemens Medical Solutions, Erlangen, Germany). MRI sequences and parameters were reported in our previous study. 20 MRI scanning was performed at 1 h following the injection of t-PA (approximately 4 h of ischemia) and at 1, 7 and 30 days following the onset of ischemia. Infarct volumes were calculated using ITK-Snap contouring software (Pittsburgh) with stacks of average diffusion images reconstructed in three dimensions. Two independent and blinded observers analyzed the MRI images.
Post-surgical management
Post-surgical management and disposition were described previously by us. 20 Briefly, mannitol (1 g/kg, i.v.) and antibiotics (Ceftriaxone Sodium, 50 mg/kg, i.v.) were given. Buprenorphine (Buprecare, 20 μg/kg, i.m.) was injected to reduce pain. We sacrificed the animals earlier than the desired endpoint as described previously because of serious neurological or other clinical compromise and the inability of the animal to care for itself or inactivity and lack of alertness for a continuous 24-h period. 27
Neurological assessments
Neuro-behavioral outcomes were measured at 24, 48, and 72 h and one and four weeks after ischemia using NHPSS and Spetzler score.20,24,28 Modified movement assessment panel (mMAP) was in accordance to a previous study by us prior to, 14 and 30 days post ischemia. 29
Statistical analysis
Statistical analysis was performed with SPSS for Windows, version 21.0 (SPSS, Inc.). Infarct size and neurological deficit score at the acute stage were compared using independent sample t tests. Univariate general linear model was adopted to analyze the effects of hypothermia, reperfusion and the interaction. Repeated-measures ANOVA was used to measure the effects of SI-AC on repeated variables. A univariate general linear model was adopted to analyze the effects of hypothermia and reperfusion. P < 0.05 was defined as statistical difference.
Results
Thrombus-thrombolysis ischemic models in NHPs
To investigate thrombus-thrombolysis treatment of ischemic stroke, a model with identical autologous clot load delivered by the micro-catheter was developed for this study to best emulate the clinical situation. As shown in Figure 1(a) to (c), the M1 segment of the middle cerebral artery (MCA) was occluded and confirmed radiographically on both anterior-posterior and lateral digital subtraction angiography (DSA). Vessel occlusion was confirmed 2.5 h after the onset of ischemia (before thrombolysis) in all animals. After t-PA injection, complete (Figure 1(a)), partial (Figure 1(b)) and no (Figure 1(c)) recanalization were observed and quantified using DSA with the thrombolysis in cerebral infarction (TICI) grade. As shown in Figure 1(d), we also included 17 consecutive monkeys and the first diffusion-weighted imaging (DWI) image was performed at 1 h after the onset of ischemia. Based on reperfusion status according to DSA images after thrombolysis, there were no abnormal high signals in DWI images in models with final complete (n = 6) and partial reperfusion (n = 6), but high signals existed in models without reperfusion (n = 5) (Figure 1(e)). These results indicated an equal clot load and baseline infarct sizes before thrombolysis among models with reperfusion or without reperfusion. On the follow-up MRI images at 24 h, complete or partial reperfusion was confirmed to rule out the possibility of delayed re-occlusion (Figure 1(f)). Complete recanalization was achieved in 14 animals (28.0%, 14/50), partial recanalization in 15 (30.0%, 15/50), and no recanalization in 21 (42.0%, 21/50). Nine animals without reperfusion died within 24 h after the onset of ischemia despite routine supportive treatments and SI-AC treatments (n = 4). In addition, 12 animals died within 72 h, with three models receiving SI-AC treatments. All ischemic monkeys with complete reperfusion survived 7 and 30 days after ischemia. Furthermore, only one animal with partial reperfusion died at 3 days due to severe neurologic deficits, while the remaining other 14 monkeys with partial reperfusion survived for 7 and 30 days (Figure 1(g)). Based on recanalization outcomes determined by DSA images after the t-PA injection, a total of 42 animals (n = 14 each for complete, partial reperfusion or no-reperfusion) were randomized to receive SI-AC or no SI-AC based on random number sequence to further analyze the therapeutic efficacy of SI-AC. SI-AC induced a rapid decrease in temperature reaching a mild hypothermic (<35.0°C) level at 10 min after onset of cooling infusion and mild hyperemia lasted for approximately 20 min according to our previous findings. 15
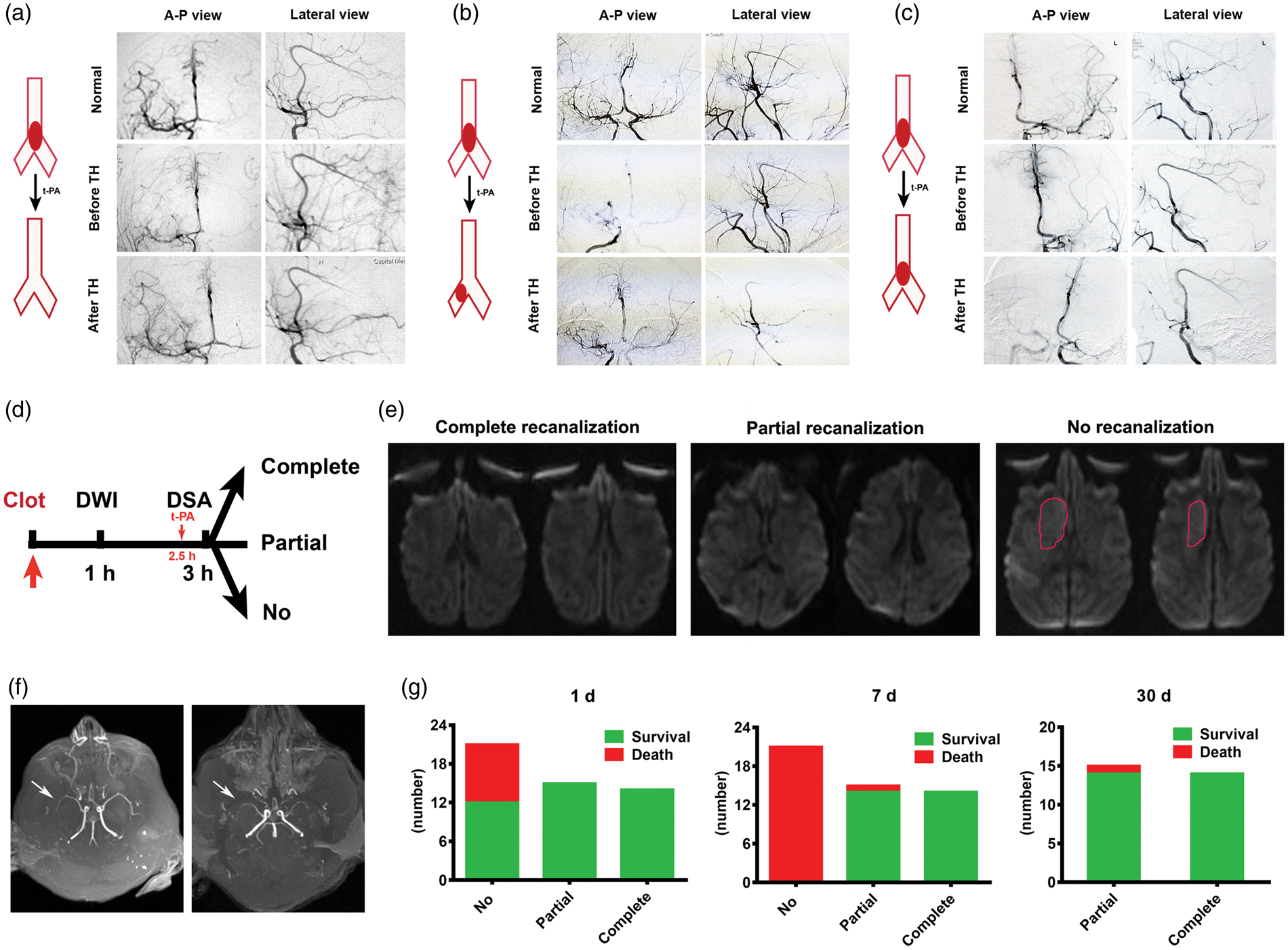
Thrombus – thrombolysis in M1 segment and outcomes. Graphical and DSA images of complete (a), partial (b) and no reperfusion (c). Anterior-posterior (A-P) and lateral views of M1 perfusions at normal state, before thrombolysis (TH), and after TH. Schematic of clot injection, DWI scanning at 1 h, and reperfusion outcomes based on DSA at 3 h post ischemia (d). In complete and partial recanalization states, all models (six with complete and six with partial reperfusion) did not show abnormal high signals at DWI images, while high signals (in red circle) existed in five models without reperfusion (e). Magnetic resonance angiography (MRA) imaging exhibited a generally normal perfusion at 24 h after ischemia with a complete and a partial reperfusion (f). The survival and death number at 24 h, 7 days, and 30 days after ischemia (g).
Efficacy of SI-AC in the acute stage
Fourteen ischemic monkeys with complete recanalization were included in the analysis (Figure 2(a)). We evaluated infarct volume and the increase of infarct volume with DWI images at 4 h and DWI images at 24 h in the t-PA (Figure 2(b)) and t-PA plus SI-AC (Figure 2(c)) groups. There was no difference in infarct volume between t-PA group and t-PA plus SI-AC groups at 4 h (Figure 2(d)). But, SI-AC treatment led a smaller infarct volume in t-PA plus SI-AC group compared with t-PA group (Figure 2(e)) at 24 h. Additionally, SI-AC treatment also decreased the infarct volume increase and percentage increase between 4 h and 24 h (Figure 2(f) and (g)). T2 images at 24 h in the t-PA group and in t-PA plus SI-AC group confirmed infarcts volumes seen on the DWI images (Figure 2(h)). There were no significant differences in mean arterial pressures (MAP), rectal temperatures, and oxygen saturation (SpO2) between two groups (Figure 2(i)).
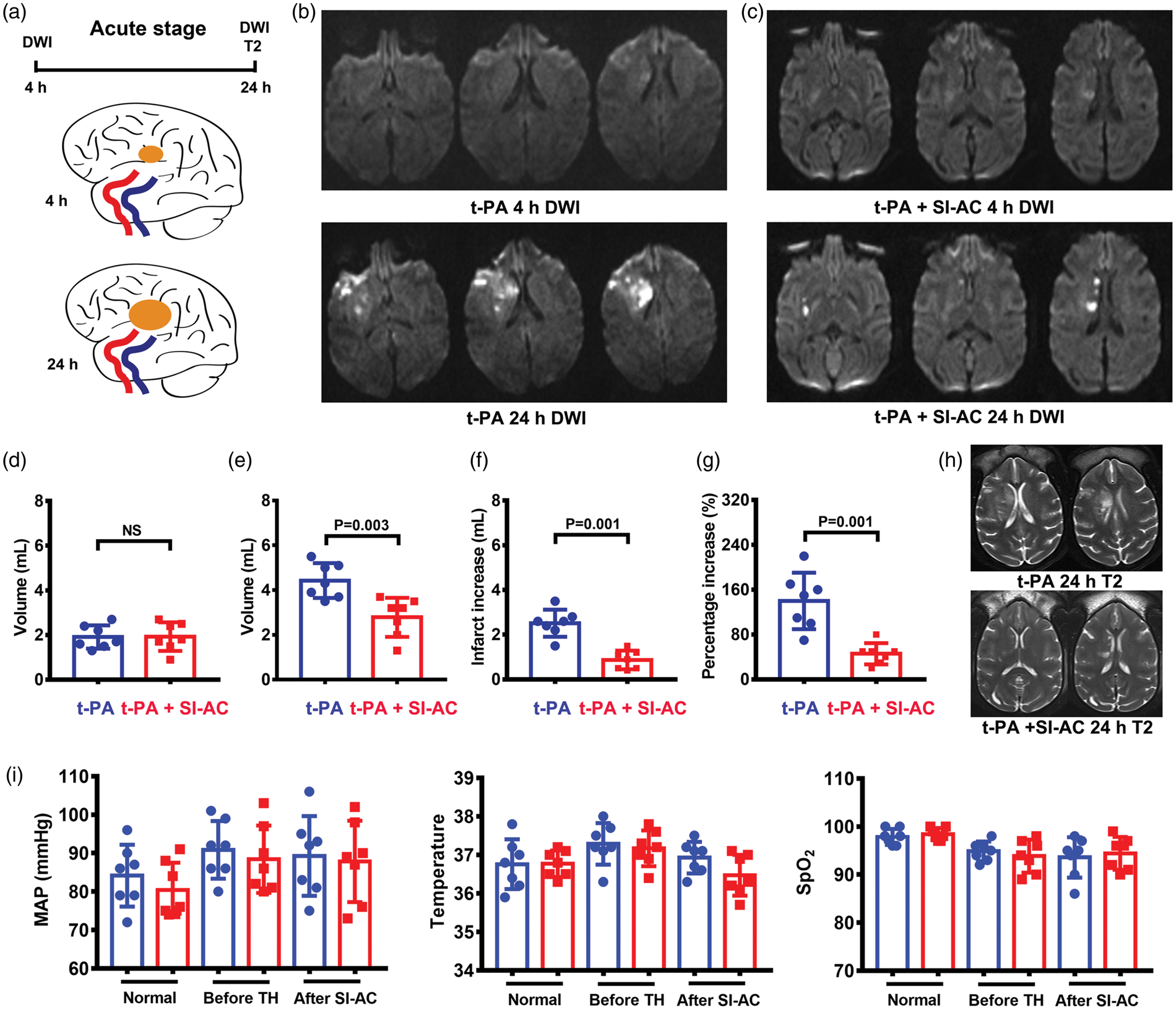
Treatment with SI-AC led to a reduced increase of infarct size between 4 h and 24 h when complete recanalization achieved. Schematic of MRI images and infarct increase (a). Representative DWI images at 4 h and at 24 h after the onset of ischemia in t-PA (b) and t-PA plus SI-AC (c) groups. Comparison of infarct volumes at 4 h (d) and those at 24 h (e) between t-PA and t-PA plus SI-AC groups. SI-AC led to both a reduced infarct increase (f) and a decreased percentage infarct increase (g) between 4 h and 24 h. T2 images at 24 h confirmed the infarct size on DWI images after t-PA and t-PA plus SI-AC (h). Mean arterial pressures (MAP), rectal temperatures, and oxygen saturation (SaO2) were shown at baseline, before thrombolysis treatment (TH), and after SI-AC treatment, with no significant differences between two groups (i). N = 7 per group. NS means not significant.
Fourteen ischemic monkeys with partial recanalization exhibited an overall severe degree of symptoms and a larger infarct volume than the complete recanalization group on DWI and T2 (Figure 3). There was no difference in infarct volume between the t-PA group and t-PA plus SI-AC group at 4 h (Figure 3(b) to (d)). But, SI-AC treatment led a smaller infarct volume in the t-PA plus SI-AC group compared with t-PA group (Figure 3(e)) at 24 h, and a reduced infarct volume increase and percentage increase between 4 h and 24 h (Figure 3(f) and (g)) was also observed. T2 imaging at 24 h confirmed the infarcts volumes observed on the DWI images (Figure 3(h)). There were no significant differences in major physiological parameters between two groups (Figure 3(i)).
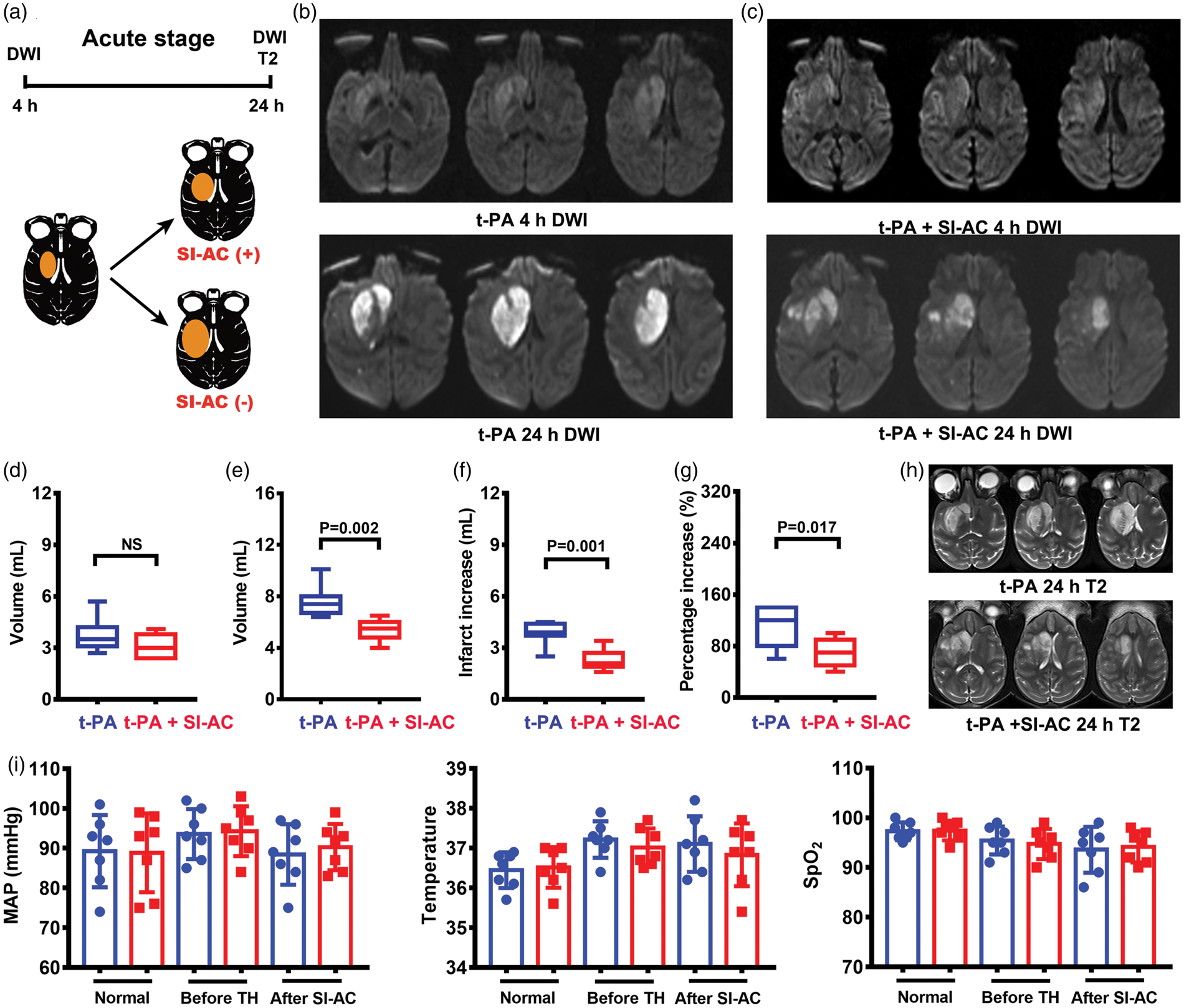
Treatment with SI-AC also reduced infarct increase when partial recanalization achieved. Schematic of MRI images and infarct increase (a). DWI images at 4 h and at 24 h after the onset of ischemia in t-PA (b) and t-PA plus SI-AC (c) groups. Despite a similar infarct volume (d) at 4 h between two groups, SI-AC led to a reduced infarct size (e), a decreased infarct increase (f) and a decreased percentage infarct increase (g) between 4 h and 24 h. T2 images at 24 h confirmed the infarct size on DWI images after t-PA and t-PA plus SI-AC (h). Mean arterial pressures (MAP), rectal temperatures, and oxygen saturation (SaO2) were not significantly different between two groups (i). N = 7 per group.
All rhesus monkeys (n = 14) without recanalization were either in a comatose state or had minimal awareness of their surroundings. Infarcts typically involved most of the MCA territory at 4 h after ischemia in both groups (Figure 4(a) and (b)). There was no difference in infarct size (Figure 4(c)), nonhuman primate stroke scale (NHPSS) and Spetzler scores between two groups (Figure 4(d)). Triphenyl tetrazolium chloride (TTC) staining post mortem confirmed the MRI observations (Figure 4(e)). Hematoxylin-eosin staining exhibited characteristic pathological features of acute ischemic stroke in both groups, including shrunken and darkly basophilic nucleus and vacuolation of the cytoplasm (Figure 4(f)). There were no significant differences in major physiological parameters between two groups (Figure 4(g)).
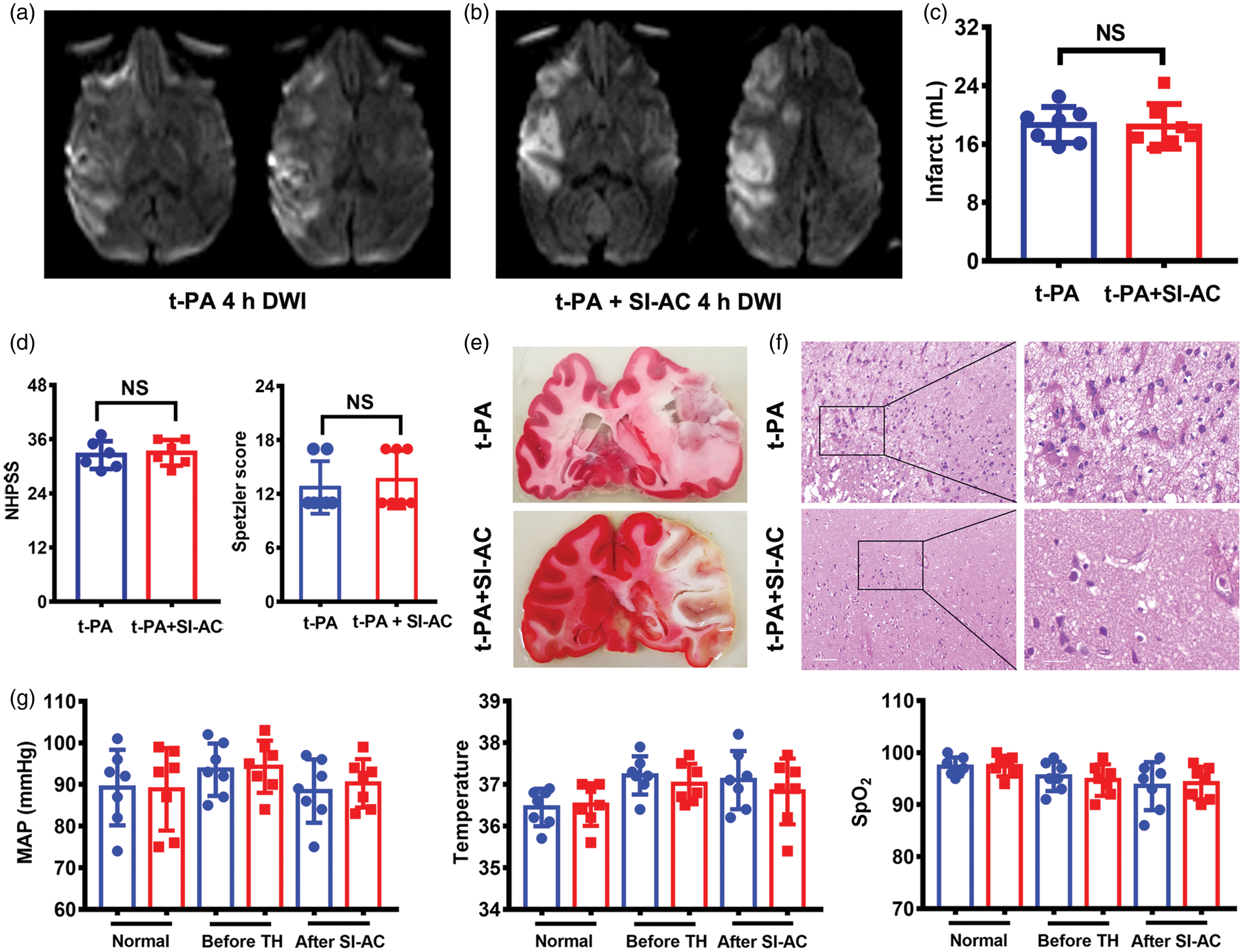
SI-AC did not improve outcomes without recanalization. Representative DWI images in both t-PA (a) and t-PA plus SI-AC (b) groups indicated a large infarct size at 4 h after ischemia. Infarct sizes measured by DWI at 4 h were not reduced by the SI-AC treatment (c). Higher NHPSS index and lower Spetzler scores also indicated severe neurological impairments in both groups with or without SI-AC after t-PA (d). Representative TTC staining images confirmed the MRI images in both groups (e). Hematoxylin-eosin staining indicated a characteristic changes in acute stage, including shrunken and darkly basophilic nucleus and vacuolation of the cytoplasm (f). There were no differences in mean arterial pressures (MAP), rectal temperatures, and oxygen saturation (SaO2) between two groups (g). N = 7 per group.
Efficacy of SI-AC in the chronic stage
Long-term neurological function analysis was conducted throughout the 30 days after ischemia in models with complete and partial recanalization.24,28 Compared to animals only with complete reperfusion, those treated with SI-AC exhibited a reduced infarct volume (Figure 5(b)) at 30 days, improved NHPSS (P = 0.004, Figure 5(c)) and Spetzler scores (P = 0.025, Figure 5(d)) during the observation period. In addition, SI-AC treatment decreased the total time for picking up the food with the affected arm at both 14 and 30 days (P = 0.017, Figure 5(e)). Ischemic monkeys with partial recanalization exhibited an overall more severe degree of symptoms and larger infarct volumes as compared to the complete recanalization group. Animals treated with SI-AC also showed a reduced infarct size (Figure 5(f)), improved NHPSS (P = 0.002, Figure 5(g)) and Spetzler scores (P = 0.006, Figure 5(h)) through the 30-day observation period. Furthermore, SI-AC decreased total time for picking up food and withdrawal of the affected arm (P = 0.026, Figure 5(i)), suggesting an enhanced degree of motor function preservation.
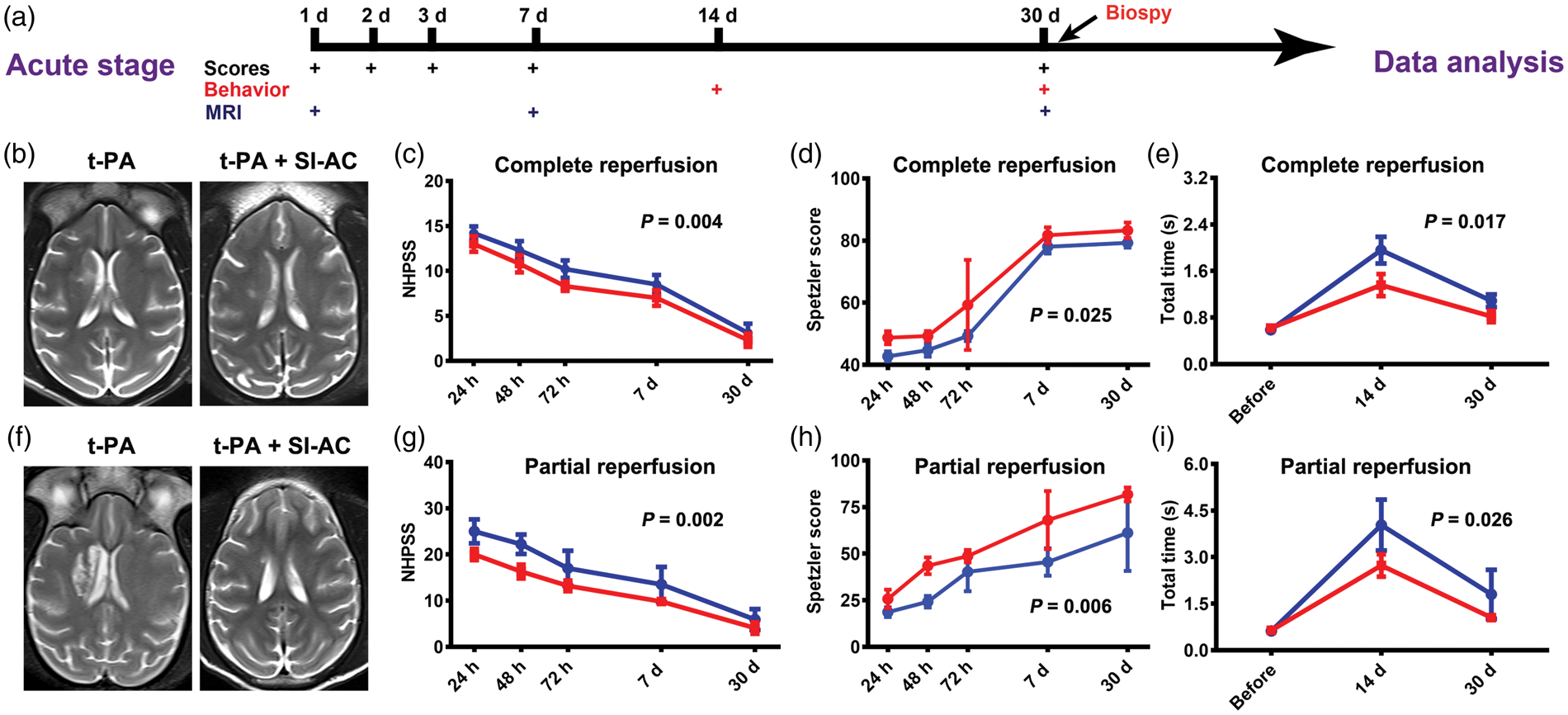
SI-AC treatment improves MRI and functional outcomes when recanalization achieved. Schematic of neurological scores, behavior test, and MRI imaging throughout a 30-day observation period (a). In complete recanalization, monkeys with SI-AC treatment exhibited decreased infarct size at 30 days (b), better NHPSS scores (c) and Spetzler Scores (d) over the 30 days, reduced the total time for the affected arm to pick up and withdraw food (e). In partial reperfusion, treatment with SI-AC also led to decreased infarct volumes (f), better NHPSS scores (g) and Spetzler scores (h) over the 30 days, reduced the total time for the affected arm to pick up and withdraw food (i). N = 7 per group. Data are mean ± SD, two-way repeated-measures analysis of variance.
The effects of hypothermia and recanalization on neuroprotection
How did SI-AC and reperfusion states affect infarct size (T2, at 24 h) and functional prognosis (NHPSS, at 30 d) deserved further analysis. As shown in Figure 6(a), both SI-AC (P = 0.001) and reperfusion state (P = 0.030) led to a smaller infarct size at 24 h based on T2 images. The infarct increase based on DWI images at 1, 4 and 24 h post ischemia further illustrated the smallest infarct size when combining complete reperfusion and SI-AC treatment (Figure 6(b)). Both SI-AC (P = 0.001) and reperfusion (P = 0.001) led to a better NHPSS score at 30 days (Figure 6(c)). As shown in Figure 6(d), models with complete reperfusion and SI-AC treatment appeared to have a better functional prognosis. Therefore, better neurologic function and a smaller infarct size seemed to be dependent on both SI-AC and timely reperfusion. However, we did not observe the interaction of hypothermia and recanalization on a smaller infarct size and better NHPSS score based on existing limited data.
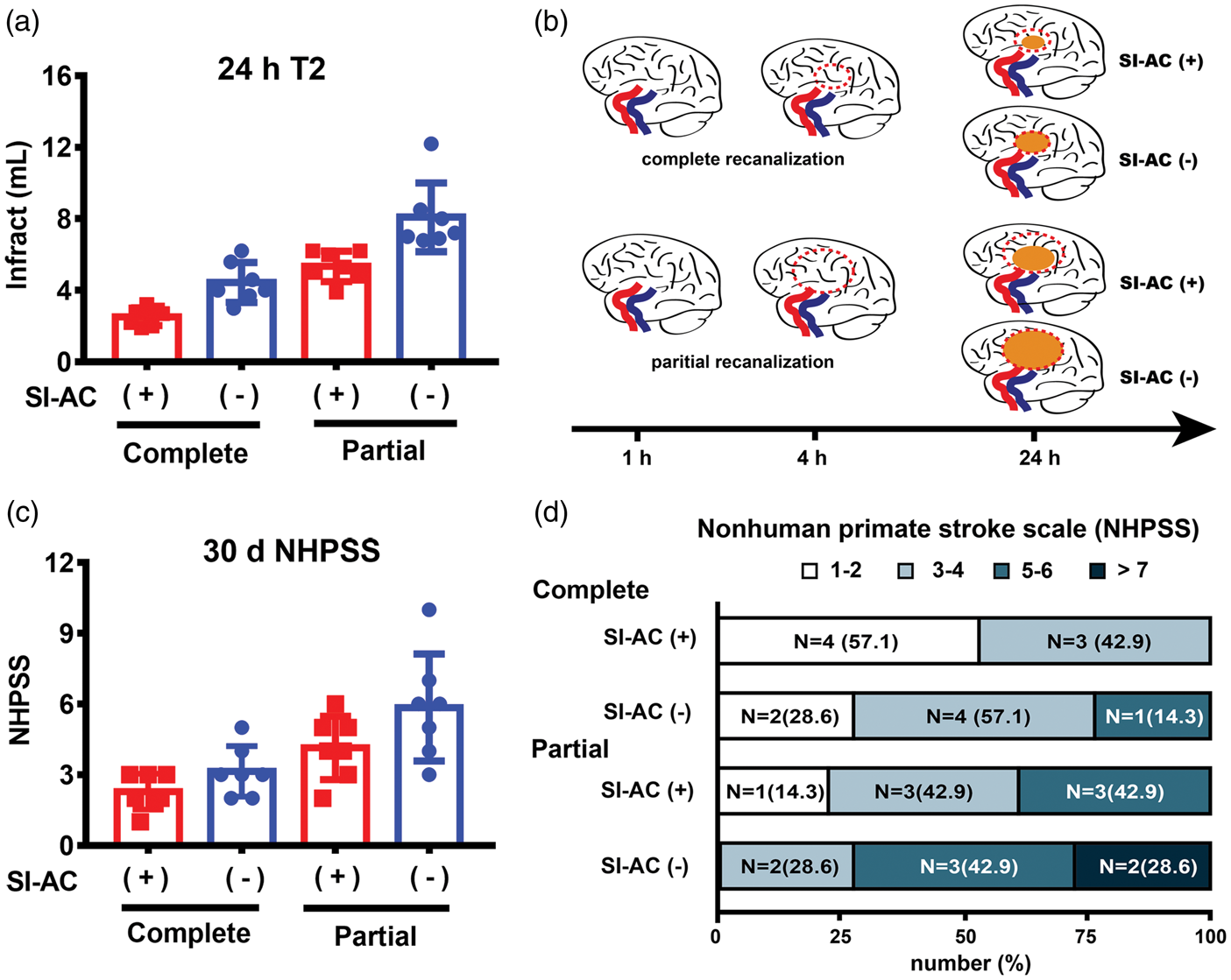
The effect of SI-AC and recanalization on infarct size and functional outcomes over a 30-day observation period. Both recanalization state and hypothermia led to a lower infarct size at 24 h (T2) after the onset of ischemia (a). The figure depicts a time course of the ischemic increase at various time scenarios after stroke, indicating that SI-AC may reduce infarct sizes from an expected size (in red dotted lines) to an actual one (in yellow circle) between 4 and 24 h post ischemia and that complete reperfusion plus SI-AC led to a smaller infarct size (b). Both recanalization state and hypothermia led to a better NHPSS score at 30 days after the onset of ischemia, in which models with complete reperfusion plus SI-AC had the best functional scores (c). There was a significant difference favoring the complete reperfusion plus SI-AC over other groups in the overall distribution of better NHPSS scores (d).
Discussion
Mismatch theory (Penumbra tissue) is the basis for successful recanalization treatments at present; however, great mismatch still exist between bench and bed side, which may account for the failure of nearly all neuroprotectants in clinical trials. In order to advance stroke therapy, we first developed a clinically applicable and relevant ischemic model in rhesus monkeys to lessen the genetic gap. We also bridged gaps of reperfusion state and long-term functional assessments between preclinical and clinical studies by simulating varying degrees of recanalization and using a 30-day functional score in monkey models. Importantly, we resorted to MRI images and biopsy to further link the association of functional recovery and gene expressions. Therefore, neuroprotective effects due to an optimized hypothermic strategy were observed in a higher order NHPs brain, and the importance of reperfusion as a direct prerequisite for neuroprotection was demonstrated, and potential genes and pathways for long-term benefits were discovered in this translational study.
NHPs are considered an ideal but difficult animal model for preclinical and translational research, specially advocated by STAIR group for translational stroke study. 18 This in part is due to significant cerebrovascular, neuroanatomical and biomolecular homology between nonhuman primates and humans. Compared to rodent models, these similarities may allow us to more closely mimic the physiology and pathophysiology of stroke in humans. NHPs stroke models have been explored by a few groups in the past.24,30 The use of a thrombus as the means of vessel occlusion enabled us to simulate the pathological mechanism that occurs in ischemic patients with an embolic stroke.31,32 In addition, the micro-catheter system served as an endovascular route for the local delivery of t-PA and SI-AC, simulating what can be done in a human clinical trial. The three revascularization outcomes we observed were similar to those found in ischemic stroke patients undergoing endovascular thrombectomy with or without t-PA. 33 Our thrombus-thrombolysis ischemic model in rhesus monkeys meets three basic criteria for an ideal NHPs stroke model: (1) formation of a relatively large infarction, (2) notable neurologic impairments and (3) long-term survival period (at least seven days) with successful treatment.24,34,35 This unique NHPs stroke model paves way for us to refine the therapeutic application of SI-AC as well as other potential neuroprotectants in the future. However, it is still difficult to simulate clot retrieval in monkey models due to the smaller diameter of MCA (1.0 mm) and relatively bigger diameters of available retrieval stents.
Hypothermia is one of the best-studied and most effective forms of neuroprotection. 36 Nearly all preclinical studies on hypothermic therapy have reported beneficial outcomes in animal models of focal ischemia, while most clinical studies obtained neutral or negative results.9,37 Classical hypothermia approaches, induced by whole-body surface cooling and subsequently via endovascular cooling are associated with an extended hypothermia induction period and side effects, such as cardiac arrhythmias, bradycardia, and pneumonia. These side effects due to systematic hypothermia were demonstrated in the ICTuS-L and ICTuS 2 studies.38–40 Recently, several studies have attempted selective hypothermic methods to exclusively cool brain and maintain systematic temperature generally normal.41,42 We have established a proof of concept of SI-AC in a rodent model. 14 We also showed that rapid induction of brain hypothermia with a localized coolant infusion mitigated the degree of brain infarction and neurological deficits with little disturbances to major physiological parameters.15,16 Choi et al. 43 also supported the efficacy of local brain hypothermia in which intra-carotid infusion of cold saline led to a rapid temperature decrease among patients. In the present study, we not only reinforced our previous findings regarding the therapeutic effect of SI-AC but also demonstrated the effect of its benefit with both partial and complete reperfusion of revascularization. Selective hypothermic therapy has great translational promise due to its better benefits and less side effects.
The current prevailing belief that neuroprotectant, including hypothermia, has an uncertain role in providing clinical benefits can be attributed to various reasons. However, previous clinical stroke studies paid much attention to hypothermia per se (route, depth, duration and delay) but less to reperfusion states due to technical difficulties.44,45 Timely reperfusion can reduce the degree of infarction in hypo-perfused brain tissue and limit the expansion of already irreversibly injured tissue, leading to smaller infarct volumes and improved clinical outcomes in both bench and at bed side. 46 Mild or moderate hypothermia, including SI-AC, was found to be beneficial in rodent models with transient MCA occlusion, while less benefits seen in rodents with permanent MCA occlusion. 8 There is no consensus on the neuroprotective effects of mild or moderate hypothermia in different reperfusion states in patients. Only one earlier paper did report positive effects of therapeutic hypothermia in ischemic stroke patients with angiographically proven reperfusion. 47 Our recent finding suggested the safety and feasibility of local hypothermia in stroke patients, but we did not find functional benefits. 17 In the present study, we observed less infarct growth and improved long-term neurological functions, thus providing direct evidence that reperfusion is essential for neuroprotection of therapeutic hypothermia in acute brain ischemia. When over 70% of patients treated with endovascular thrombectomy achieved successful reperfusion, this study also provide insights to combine endovascular thrombectomy with previously failed approaches in future translational or clinical studies, including uric acid, human albumin, DP-B99, cerebrolysin.8,48
Another important mismatch between preclinical and clinical study is the unbalanced focus on infarct sizes and long-term functions. The 90-day modified Rankin score is widely used to evaluate neurological benefits in clinical studies; however, only 1/3 preclinical studies evaluated neurological functional outcomes, fewer than 30% of which monitored long-term functional recovery. 8 We used similar functional evaluations in this preclinical study as implemented by clinical studies to complete both neurological scores and behavior tests. Evidence from animal models suggested that greatest gains in recovery only occurred in a time-limited window.49,50 Together with data in this study, we also provided insights that neuro-protectants following reperfusion therapy would increase plasticity and compensate for tissue loss due to focal ischemia in the chronic stage.
There are several caveats to keep in mind. First, local hypothermia induced by SI-AC was very transient and further optimization of the cooling period may increase efficacy. Second, DSA and MRA, appropriate for the assessment of large vessel occlusion, did not reflect the real cerebral blood flow and tissue perfusion levels. Third, we were unable to directly monitor cerebral temperature because of the risk of intracranial hemorrhage and potential infections.
In conclusion, our study describes a novel thrombus-thrombolysis stroke model in adult rhesus monkeys and proves that beneficial effects of SI-AC are closely linked with reperfusion states. In a broader translational context, our new NHPs models allow us to explore a wide range of other potential adjuvant therapies that can be supplemented into current t-PA and thrombectomy reperfusion protocols in ischemic stroke.
Supplemental Material
JCB903697 Supplemental Material - Supplemental material for Selective intra-arterial brain cooling improves long-term outcomes in a non-human primate model of embolic stroke: Efficacy depending on reperfusion status
Supplemental material, JCB903697 Supplemental Material for Selective intra-arterial brain cooling improves long-term outcomes in a non-human primate model of embolic stroke: Efficacy depending on reperfusion status by Di Wu, Jian Chen, Mohammed Hussain, Longfei Wu, Jingfei Shi, Chuanjie Wu, Yanhui Ma, Mo Zhang, Qi Yang, Yongjuan Fu, Yunxia Duan, Cui Ma, Feng Yan, Zixin Zhu, Xiaoduo He, Tianqi Yao, Ming Song, Xinglong Zhi, Chunxiu Wang, Lipeng Cai, Chuanhui Li, Shengli Li, Yongbiao Zhang, Yuchuan Ding and Xunming Ji in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Authors’ Note
Ming Song is now affiliated with Brainnetome Center, Institute of Automation, Chinese Academy of Sciences, Beijing, China and Yongbiao Zhang is now affiliated with Interdisciplinary Innovation Institute of Medicine and Engineering, Beijing Advanced Innovation Center for Big Data-Based Precision Medicine, School of Biological Science and Medical Engineering, Beihang University, Beijing, China.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Chang Jiang Scholars Program (#T2014251 to X.J.) from the Chinese Ministry of Education; National Natural Science Foundation of China for Outstanding Youth (81325007 to X.J.); National Natural Science Foundation of China (81871022 to D.W., 81771260 to J.C.); National Natural Science Foundation of China (81620108011 to X.J.); National Key R&D Program of China (2017YFC1308401 to X.J.); and the “mission” talent project of Beijing Municipal Administration of Hospitals (SML20150802 to X.J.); Beijing Municipal Administration of Hospitals’ Youth Programme (QML20170802 to D.W.).
Authors’ contributions
XJ, YD and DW designed and planned the study. DW, JC, LW, JS, CW, YM, MZ, QY, YF, YD, CM, FY, ZZ, XH, TY, MS, XZ, CW, LC, CL, SL, and YZ obtained and analyzed data. DW, MH, and YD made a draft of the manuscript and further revision.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.