
Abstract
Patients with asymptomatic, high-grade internal carotid artery stenosis often suffer from subtle cognitive impairments with unclear underlying neuro-cognitive mechanisms. Thus, we hypothesized that stenosis-related unilateral cerebral hypoperfusion leads to an ipsilateral attentional bias; 22 patients with asymptomatic, one-sided high-grade carotid stenosis and 24 age-matched healthy controls underwent pseudo-continuous arterial spin labeling to assess brain perfusion in the territory of the carotid arteries. Furthermore, a parametric assessment of attention functions was carried out on the basis of the computational Theory of Visual Attention. Both patients' perfusion and spatial attention were significantly more lateralized than those of healthy controls. Critically, both asymmetry indices were significantly correlated in patients, i.e. the stronger one-sided relative hypoperfusion, the stronger ipsilateral bias of attention. This association was specifically pronounced in parietal cortices and independent of white matter hyperintensities as a surrogate for cerebrovascular brain damage. Results provide evidence for a link between lateralized hypoperfusion and lateralized attentional weighting in asymptomatic, high-grade carotid stenosis. Data suggest that lateralized hypoperfusion with simultaneous spatial attentional bias might serve as a potential therapeutic target in one-sided carotid stenosis.
Keywords
Introduction
Patients with asymptomatic high-grade internal carotid artery stenosis do not show – by definition – any signs of transient or permanent cerebral ischemia. Careful neuropsychological assessments, however, often reveal subtle cognitive impairments, particularly in tasks relying on voluntary attention processes.1,2 Attention processes depend on an extended fronto-parietal system,3,4 which is mainly supplied by the carotid arteries. Damage to this system, particularly to parietal cortices, can lead to, primary spatial, attentional deficits, i.e. spatial bias to one hemifield. The severity of resulting deficits ranges from a slight tendency for extinction behavior to severe spatial hemi-neglect. Notably, even mild spatial attentional bias is known to interfere with a multitude of daily life activities (from reading to car driving). 5 Moreover, patients with carotid stenosis often show a progressive increase of cognitive deficits.6–8 While such deficits might be related to the lateralized hypoperfusion, the underlying neuro-cognitive mechanisms are still unclear. An improved mechanistic understanding of these deficits is important as it could serve to define therapeutical targets and the identification of subgroups of patients who would benefit from an aggressive treatment, such as revascularization.
Potential effects of one-sided stenosis on spatial attention can be investigated by a psychophysical partial report based on the mathematically formulated Theory of Visual Attention (TVA). 9 The TVA model states that elements in the visual field compete – in terms of a race model – for getting encoded into capacity limited visual short term memory. The probability of being encoded, i.e. consciously perceived, is proportional to the attentional weight of the given element. Thus, the higher the weight, the higher the probability for the element to get encoded. Mathematical modelling of accuracy across the different experimental conditions delivers parameters for separate attentional weights for the left and right hemifield, which allows revealing even subtle spatial attentional bias towards one hemifield.
As unilateral carotid stenosis frequently causes unilateral relative hypoperfusion in areas including the parietal cortices,10,11 we wanted to clarify two research questions: As a primary research question, we investigated whether unilateral relative hypoperfusion in the anterior circulation is associated with an ipsilateral attentional bias in patients with unilateral asymptomatic carotid stenosis. As a secondary research question, we tested whether specifically parietal perfusion asymmetries are linked with ipsilateral attentional bias. To address these questions, we conducted a psychophysical TVA-based partial report paradigm, which is known to permit the sensitive estimation of even subtle spatial attentional bias. 12 We estimated perfusion by perfusion-weighted MR-imaging using pseudo-continuous arterial spin labeling (pCASL) in carotid stenosis patients and controls. Laterality indices of visual attention and perfusion were correlated within the anterior circulation. The analysis was controlled for structural brain lesions (i.e. white matter hyperintensities (WMHs)) as a potential confound when analyzing the particular relevance of perfusion deficits for attention.
Materials and methods
Participants
Twenty-nine patients (9 females, 70.3 ± 7.0 years (mean ± standard deviation)) with an asymptomatic, one-sided high-grade extracranial carotid artery stenosis (confirmed by duplex ultrasonography; all > 70% according to the NASCET criteria 13 ) and 30 healthy, age-matched control participants (17 females, age 70.3 ± 4.8 years) participated in this prospective study. The study was approved by the medical ethical board of the Klinikum rechts der Isar, in line with the Human Research Committee guidelines of Technische Universität München. All participants provided informed consent in accordance with the standard protocol approvals. Patients were recruited in the outpatient clinic for carotid stenoses of the Department of Vascular and Endovascular surgery and Angiology of the Klinikum rechts der Isar, Technische Universität München. Typically, patients are referred to this outpatient clinic for further evaluation by primary care doctors and physicians from private practices after an incidental finding of a high-grade carotid stenosis. Patients were considered clinically ‘asymptomatic’ as they did not show any signs of stroke or neurological symptoms attributable to transitory ischemic attacks and had no history of overt stroke as confirmed by FLAIR and diffusion-weighted imaging. Healthy participants were recruited by word-of-mouth advertisement. Examination of each participant included the assessment of medical history, the application of a computerized partial report paradigm, and an MR scan. Exclusion criteria for entry into the study were a history of stroke, transitory ischemic attack, or of brain surgery, mild cognitive impairment or dementia, affective disorders, schizophrenia or other severe neurological and psychiatric diseases, clinically remarkable structural MRI (e.g., silent territorial ischemic lesions or bleedings), visual impairment that would interfere with the computer-based attention test, severe chronic kidney disease, and MR contraindications. Several paper-and-pencil screening tests and questionnaires, including Mini-Mental State Examination, Line Bisection Test, Trail making test A and B, Beck's Depression Inventory, and State Trait Anxiety Inventory, were conducted to assess basic cognitive status, spatial attention, as well as executive and affective functions. In particular, the Line Bisection Test was conducted as a widely used clinical screening of unilateral spatial neglect. 14 We used a version with 17 horizontal lines as provided by Stroke Engine Intervention, Montreal (https://www.strokengine.ca/en/psycho/lbt_psycho/).
Data acquisition
Scanning was performed on a clinical 3T Philips Ingenia MR-Scanner (Philips Healthcare, Best, The Netherlands) using a 16-channel head/neck-receive-coil. All participants underwent pCASL, FLAIR and MP-RAGE imaging. Additionally, a contrast-enhanced angiography of the neck and the aortic arch vessels was performed. None of the healthy control participants showed relevant stenoses of the brain supplying arteries according to MRA.
The MR imaging parameters were as follows:
pCASL
All parameters were explicitly set according to the recommendations of the ISMRM perfusion study group. 15 The labeling plane was individually planned on the basis of a phase contrast angiography of the neck to ensure perpendicular labeling of a straight segment of both internal carotid arteries at least 2 cm distal to the stenosis. Label duration 1800 ms; post label delay 2000 ms; segmented 3D GRASE readout; four background-suppression pulses and proton density weighted (PDw) scan for normalization; TR/TE/α = 4377 ms/7.4 ms/90 °; 16 slices; three dynamics; voxel size: 2.75 × 2.75 × 6.0 mm3, TSE factor 19, EPI factor 7, acquisition time 5 min 41 s. A cerebral blood flow (CBF) signal reduction of 25% by reduced labeling efficiency as a consequence of the four background-suppression pulses of the pCASL was assumed.16,17
MP-RAGE
TI/TR/TE/α = 1000 ms/2300 ms/4 ms/8 °; 170 slices covering the whole brain; FOV 240 × 240 ×170 mm3; voxel size 1.0 × 1.0 × 1.0 mm3, acquisition time 5 min 59 s.
FLAIR
TR/TE/α = 4800 ms/289 ms/90 °; 163 slices covering the whole brain; FOV 250 × 250 × 183 mm3, acquisition size: 1.12 × 1.12 × 1.12 mm3 (reconstructed voxel size 1.0 × 1.0 × 1.0 mm3), TSE factor 167, inversion delay 1650 ms, acquisition time 4 min 34 s.
Data preprocessing
Cerebral blood flow maps of brain perfusion
Perfusion-weighted images were calculated in custom MATLAB programs (MathWorks, Natick, MA, USA) using SPM12 (Wellcome Department of Cognitive Neurology, London, UK). Label and control images were motion corrected, averaged, subtracted, normalized by a PDw-image and converted to CBF maps following. 15 Resulting CBF maps were spatially normalized to the standard space of the Montreal Neurological Institute (MNI) and smoothed by a Full Width at Half Maximum (FWHM) Gaussian kernel of 5 mm. Before CBF maps were analyzed for perfusion lateralization, they were controlled for arterial transit time (ATT) artifacts, i.e. artifacts that occur when most of the labeled blood has not yet reached the capillary bed at the time point of signal read-out. This was conducted in two steps: First, unsmoothed CBF maps in single subject space were visually inspected by a neuroradiologist (J.G., three years of experience), who screened for significant signal increases in precapillary arterioles and for signal drop-outs, especially in typical watershed areas. None of the CBF-maps had evidence of ATT artifacts. Second, to quantify contributions of ATT artifacts to the perfusion signal of the participants, the spatial coefficient of variation of the unsmoothed CBF-maps was analyzed. This measure was found to correlate with ATT artifacts and can therefore be used as an indicator for this kind of artifact. 18 The coefficients of variation were not significantly different between hemispheres (paired t-test of mean individual ATT in the left vs. right hemisphere in patients/controls: t = −0.37/−1.05, p = 0.71/0.31; Supplemental Figure 1) and groups (mean patients/controls: 39.2 ± 5.4/39.0 ± 11.1; two-sample t-test: t = 0.07, p = 0.95). This indicates equal contributions of ATT artifacts to the perfusion signal in both groups, suggesting that group differences in perfusion lateralization are not explained by distinct ATT differences.
WMH segmentation
Segmentation of WMHs of FLAIR images was conducted in single subject space by using the lesion prediction algorithm of the lesion segmentation toolbox for SPM (www.statisticalmodelling.de/lst.html). 19 A lesion probability threshold of 0.3 was applied (Supplemental Figure 2). Afterwards, each FLAIR image was visually evaluated by a neuroradiologist (J.G.) and segmentation maps were manually modified if necessary using Vinci (MPI for Neurological Research, Cologne, Germany).
Measurement of lateral bias of attentional weights in partial report
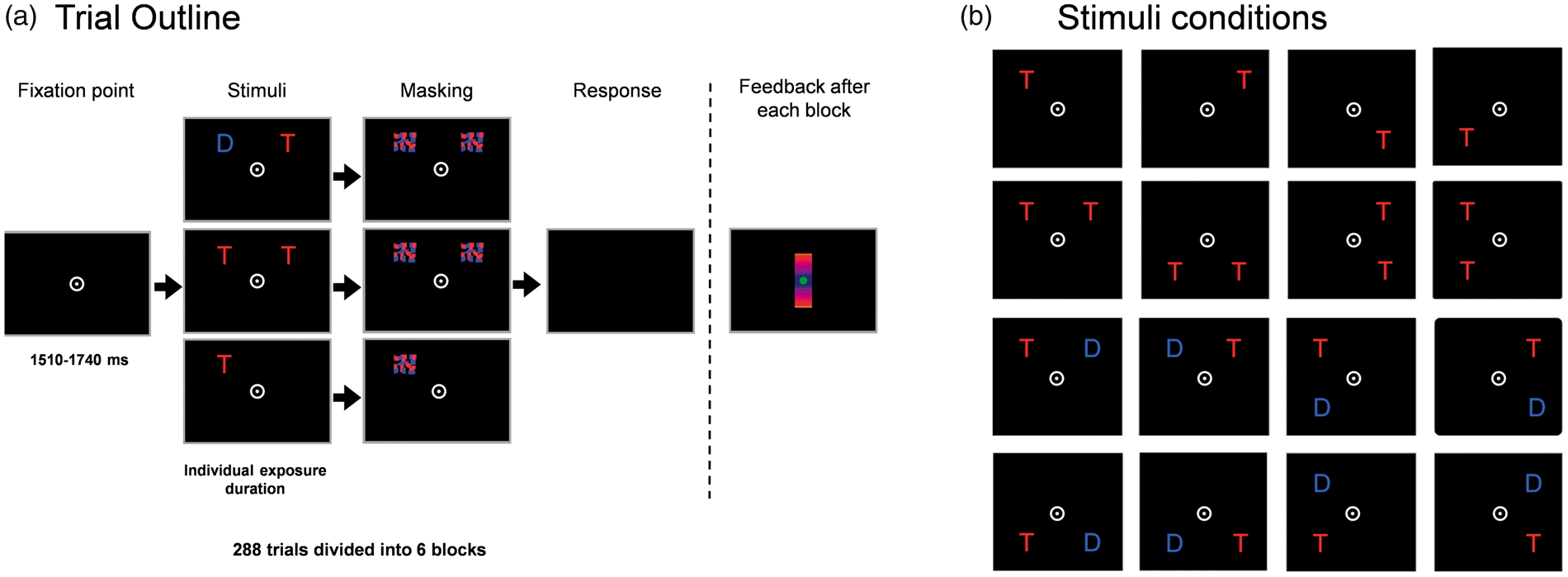
MRI and TVA-based assessment of partial report was conducted on the same day in all participants. Stimuli were presented on a 21.5-inch monitor (1920 by 1080-pixel resolution, 100 Hz refresh rate), in a dimly lit and quiet room. The viewing distance was set at approx. 50 cm. Partial report testing lasted approx. 30–40 min. The participants were instructed to fixate on a central white circle presented throughout the experiment. Within a given trial, the fixation circle was first presented alone for 1510–1740 ms on a black background. Subsequently, red and/or blue letters were briefly displayed. Letters on each trial were randomly chosen from the set [A, B, D, E, F, G, H, J, K, L, M, N, O, P, R, S, T, V, X, Z], with the same letter appearing only once on a given trial. All stimuli were masked to erase the visual afterimage. Participants had to report only the red letters (i.e. targets), while ignoring the blue letters (i.e. distractors). Any verbally reported letters were entered into a keyboard by the experimenter who was blinded to group assignment (Figure 1(a)). Either a single target, two targets, or a target together with a distractor appeared at the corners of an imaginary square with an edge length of 5 ° centered on the midpoint of the screen, resulting in 16 conditions (4 single target, 4 dual target, and 8 target + distractor conditions; Figure 1(b)). Individual exposure durations were determined in a practice session with 32 trials and set at a length at which the participant could report single targets with 80% accuracy and dual targets with at least 50% accuracy. However, the maximum exposure duration was set at 200 ms to prevent saccades towards the letter stimuli. In two participants, this maximum exposure duration was used although they did not reach the desired accuracy range in the pretest. Nevertheless, both subjects performed within this desired accuracy range during the main experiment. The pretest was followed by 288 trials, separated into 6 blocks of 48 trials. Within each block, the different trial types were presented equally often in randomized order. The average exposure duration of patients was 137 ms (±28.1 ms) and that of healthy controls was 114 ms (±29.4 ms) with comparable single target accuracy in both groups (mean patients/controls: 0.77 ± 0.10/0.77 ± 0.11; two-sample t-test: t = 0.07, p = 0.95).
Assessment of attentional selection parameters based on the computational Theory of Visual Attention (TVA). (a) Temporal outline of an experimental trial: The participants were instructed to fixate on a central white point. Subsequently, randomly chosen red and/or blue letters were briefly depicted for an individually adjusted exposure duration and masked to erase the visual afterimages. Participants had to verbally report only the red letters (i.e. targets), while ignoring the blue letters (i.e. distractors). (b) The experiment consisted of 16 trial types: 4 single target (top row), 4 dual target (row 2), and 8 target with distractor (row 3 and 4) conditions. By this procedure, attentional weights can be assessed separately for target letters (w
T
) and distractors (w
D
), and for the right and left hemifield (w
R
and w
L
) enabling the calculation of the parameters top-down control α ( = w
D
/w
T
) and laterality of spatial weighting w
λ
( = w
L
/(w
R
+w
L
)).
Clinical characteristics.
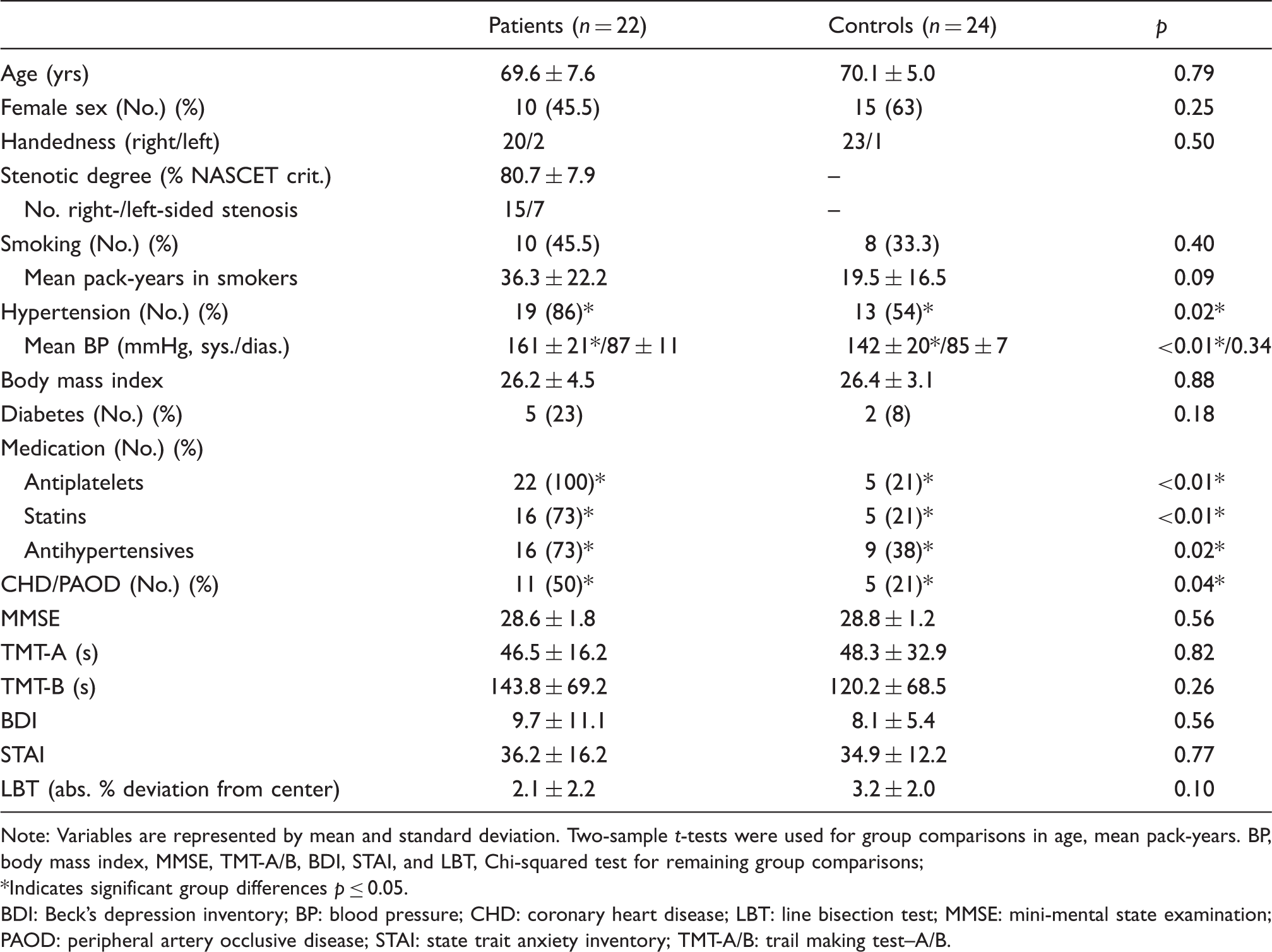
Note: Variables are represented by mean and standard deviation. Two-sample t-tests were used for group comparisons in age, mean pack-years. BP, body mass index, MMSE, TMT-A/B, BDI, STAI, and LBT, Chi-squared test for remaining group comparisons;
*Indicates significant group differences p ≤ 0.05.
BDI: Beck's depression inventory; BP: blood pressure; CHD: coronary heart disease; LBT: line bisection test; MMSE: mini-mental state examination; PAOD: peripheral artery occlusive disease; STAI: state trait anxiety inventory; TMT-A/B: trail making test–A/B.
In addition to separate estimates of attentional weights for the left and right side, parameter values for sensory effectiveness s reflecting the basic ability to perceive stimuli in each hemifield were estimated. This allows differentiating between true attentional effects related to the participants' spatial distribution of attention and pure sensory effects (better visual abilities in one hemifield). The index s λ = s L /(s L +s R ) thus provides an index of whether basic sensory effectiveness is lateralized across the right and the left field. Furthermore, the index |0.5-s λ | can be used as an index of the general degree of lateralization of sensory effectiveness, regardless of its direction towards either side.
Imaging data analysis – Measures of lateralization
To analyze perfusion lateralization, mean CBF values were calculated in MNI space within a mean gray matter template (probability threshold at 0.7) for the left and right anterior circulation (CBFL and CBFR), corresponding to the territory of the anterior and middle cerebral artery according to Tatu et al.
24
(Figure 2(a)). Furthermore, we extracted mean CBF values within the temporal, parietal, frontal and prefrontal cortex using templates from the WFU pickatlas (http://fmri.wfubmc.edu/software/PickAtlas). In analogy to w
λ
, an asymmetry index (AICBF) was calculated according to the formula: AICBF = CBFR/(CBFL+CBFR). Scores of 0.5 indicate balanced perfusion, scores > 0.5 left-sided relative hypoperfusion and scores < 0.5 right-sided relative hypoperfusion. It has been shown that women have a higher CBF compared to men; however, we do not expect systematical side differences of perfusion in both sexes of healthy controls, i.e. a relevant deviation of AICBF = 0.5.
25
Template of the anterior vascular territory and patient with one-sided relative hypoperfusion. (a) Template of combined vascular territories of the anterior and middle cerebral arteries defining the left (red) and right (blue) anterior circulation according to Tatu et al.
24
This template was used to compare CBF values between both sides in order to calculate an asymmetry index for each participant. (b) Example of a patient with a left-sided stenosis showing perfusion signal reductions on the side of the stenosis. This is reflected in an asymmetry index > 0.5 (AICBF = CBFR/(CBFR+CBFL)). However, there were also patients showing asymmetrically reduced CBF contralateral to the stenosis, i.e. the side of the stenosis did not reliably predict the side of hypoperfusion in each case. Middle: Raw CBF map in single subject space before any preprocessing steps. Right: Preprocessed maps after spatial normalization to the standard space of the MNI and smoothing. High CBF is depicted in red, low CBF in blue (colorbar). The vascular territory and perfusion maps are overlaid on a T1 weighted image in MNI space.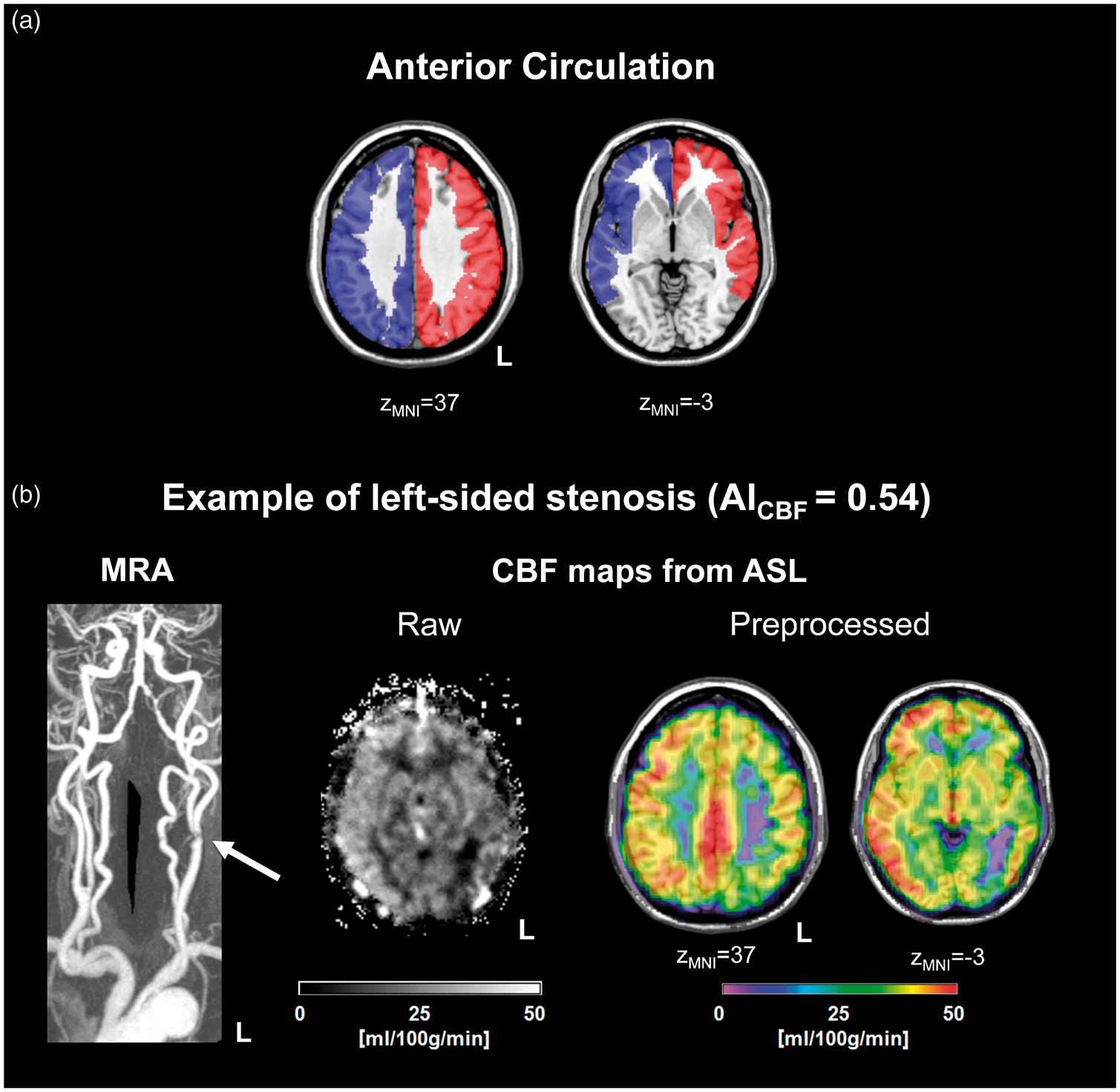
Accordingly, the number of segmented voxels of WMHs was normalized to the number of voxels of an individual whole brain mask including gray and white matter, resulting in the total normalized volume of WMHs for each subject. Furthermore, an asymmetry index (AIWMH) was calculated according to the formula: AIWMH = WMHR/(WMHL+WMHR) with WMHL and WMHR being the normalized amount of segmented WMH voxels in the left and right hemisphere, respectively (Supplemental Figure 2).
Statistical analysis
Absolute deviations of lateralized parameters w λ , s λ , AICBF, and AIWMH from the balanced value 0.5 were compared between groups using two-sample t-tests. In a second step, perfusion asymmetry scores (AICBF) and spatial attentional bias (w λ ) were associated by Pearson correlation. To control whether associations of asymmetries in AICBF and w λ were driven by WMHs, partial correlation was conducted controlling for asymmetries of WMH burden (AIWMH). A p-value ≤ 0.05 was considered statistically significant. MATLAB statistics and machine learning toolbox as well as SPSS (SPSS Inc., Chicago, Illinois, version 24.0) were used for statistical analyses.
Results
Sample characteristics
From the initially recruited sample, seven patients and six healthy controls had to be excluded due to motion artifacts in perfusion imaging (3 patients/2 controls) and inability to conduct or finish the whole visual attention testing (2/2 due to visual impairments, 1/2 due to lack of motivation to finish the task and 1/0 due to technical problems). The final sample, contributing to the results, included 22 patients and 24 healthy participants. Table 1 reports sample characteristics in those, including co-morbidities with particular focus on cerebrovascular diseases, medication, as well as cognitive, executive and affective functions of participants. Hypertension, cerebrovascular diseases, such as coronary heart disease and peripheral artery occlusive disease, and associated medications were significantly more frequent in the patient group. Age, sex, and handedness, as possible confounders for spatial attentional bias, as well as body mass index and history of smoking and diabetes did not differ significantly between groups. Furthermore, no significant group differences were observed for test scores of mini-mental state examination, trail making test A and B, Beck's depression inventory, and state trait anxiety inventory, excluding that differences of cognitive impairments and mood disturbances were biasing the results. Moreover, patients did not show significant differences in the line bisection test, used as a clinical screening tool for neglect (mean deviation from the center in patients/controls: 2.1 ± 2.2%/3.2 ± 2.0%; two-sample t-test: t = −1.69, p = 0.10).
Lateralized perfusion and non-lateralized white matter lesions in patients with carotid stenosis
Cerebral perfusion, white matter hyperintensities, and selection parameters of visual attention.
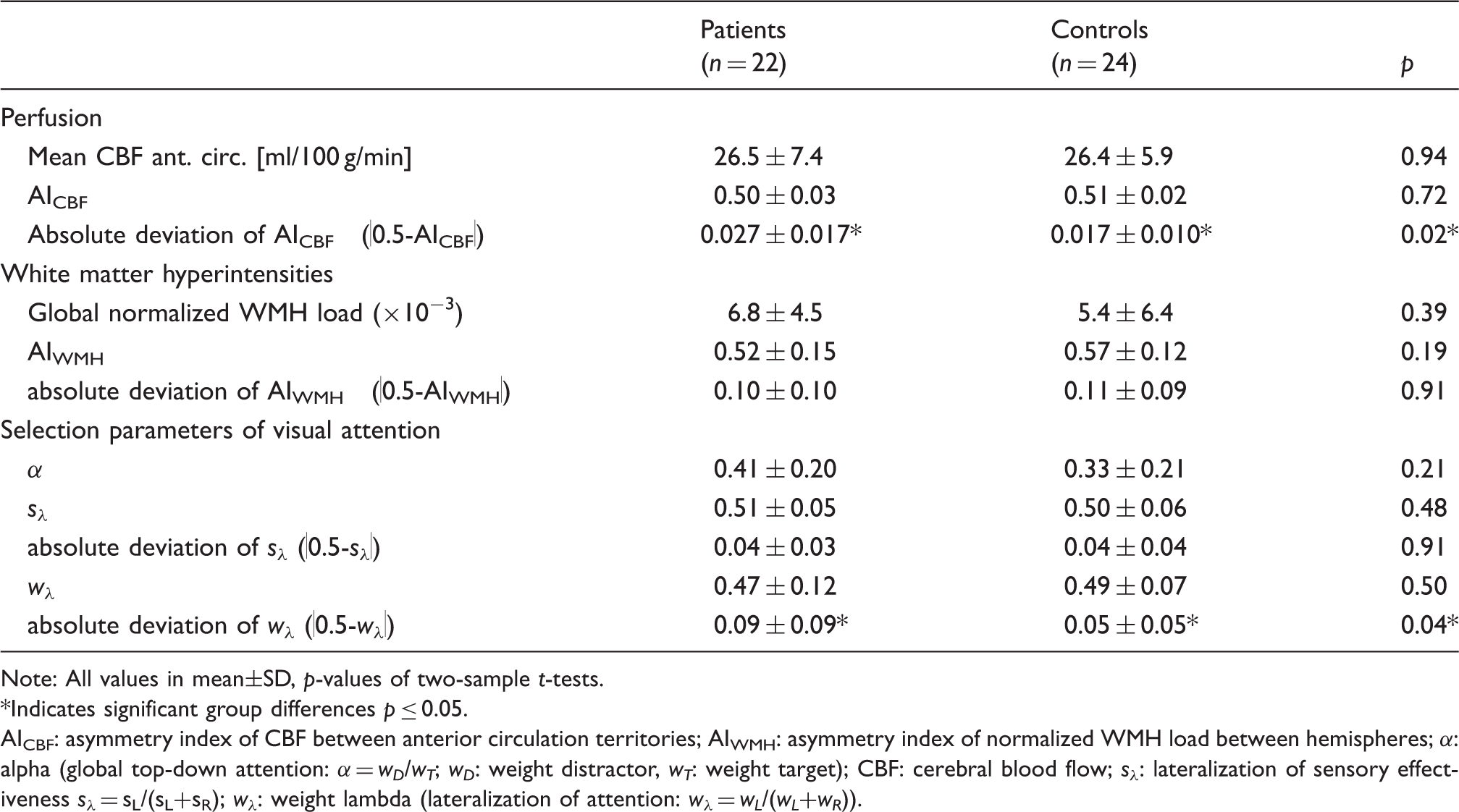
Note: All values in mean±SD, p-values of two-sample t-tests.
*Indicates significant group differences p ≤ 0.05.
AICBF: asymmetry index of CBF between anterior circulation territories; AIWMH: asymmetry index of normalized WMH load between hemispheres; α: alpha (global top-down attention: α = w D /w T ; w D : weight distractor, w T : weight target); CBF: cerebral blood flow; s λ : lateralization of sensory effectiveness s λ = sL/(sL+sR); w λ : weight lambda (lateralization of attention: w λ = w L /(w L +w R )).
Imbalance of spatial attention in patients and its association with imbalance of perfusion
To test whether the patients, in addition to the more lateralized cerebral perfusion would also show a more lateralized attention, we computed the absolute deviation of w λ from the optimally balanced value of 0.5, which reflects the degree of bias in spatial attentional weighting across hemifields. The deviation of w λ from 0.5 was significantly higher in patients (|0.5-w λ |: mean patients/controls 0.09 ± 0.09 / 0.05 ± 0.05, two-sample t-test: t = 1.78, p = 0.04, Table 2), indicating a more pronounced, albeit still relatively subtle spatial attentional bias in patients with carotid stenosis. The absolute deviation of sensory effectiveness s λ from the optimum, |0.5-s λ |, was not significantly different between groups (mean patients/controls 0.04 ± 0.03 / 0.04 ± 0.04, two-sample t-test: t = 0.11, p = 0.91, Table 2). Thus, no lateralization of sensory effectiveness was found that would indicate that the attentional lateralization rather results from more basic changes in the ability to perceive stimuli on one side of space. We did not find evidence that top-down control parameter α, reflecting task-related prioritizing of targets over distractors, was changed in patients (α: mean patients/controls 0.41 ± 0.20/0.33 ± 0.21, two-sample t-test: t = 1.26, p = 0.21, Table 2). Thus, specifically the balanced distribution of attention across hemifields seemed to be affected, while attentional weighting processes in general seemed to be preserved.
Critically, in patients, laterality of perfusion AICBF showed a significant, positive correlation with the laterality of attentional weights w
λ
(Pearson's r = 0.419, p = 0.03). Thus, one-sided relative hypoperfusion was associated with an ipsilateral attentional bias (Figure 3). This relationship between laterality of perfusion and attentional weighting appears to be specific for patients, as the correlation was not significant in controls (r = −0.050, p = 0.82). To further evaluate validity of this result, we tested whether patients’ w
λ
and AICBF values contained outliers using the ‘interquartile range rule’ according to Hoaglin and Iglewicz.
26
We did not find any outliers and values were normally distributed (Kolmogorov–Smirnov test for w
λ
/AICBF: p = 0.118/0.220), suggesting that the conducted Pearson correlation is valid. Furthermore, the correlation between laterality of perfusion and attentional weights was independent from the laterality of WMH, which was shown by a partial correlation controlled for AIWMH in patients (r = 0.424, p = 0.03).
Unilateral hypoperfusion is associated with ipsilateral attentional bias only in patients. A Pearson correlation of the laterality indices of perfusion AICBF and attention w
λ
was conducted, where AICBF and w
λ
greater than 0.5 indicate left-sided hypoperfusion and left-sided attentional bias, respectively. Accordingly, values smaller than 0.5 indicate right-sided hypoperfusion and a right-sided attentional bias, respectively. AICBF and w
λ
were found to be significantly positively associated only in patients, suggesting that a one-sided reduction of the perfusion signal is linked with an ipsilateral spatial attentional bias. *Significant Pearson correlation (p ≤ 0.05).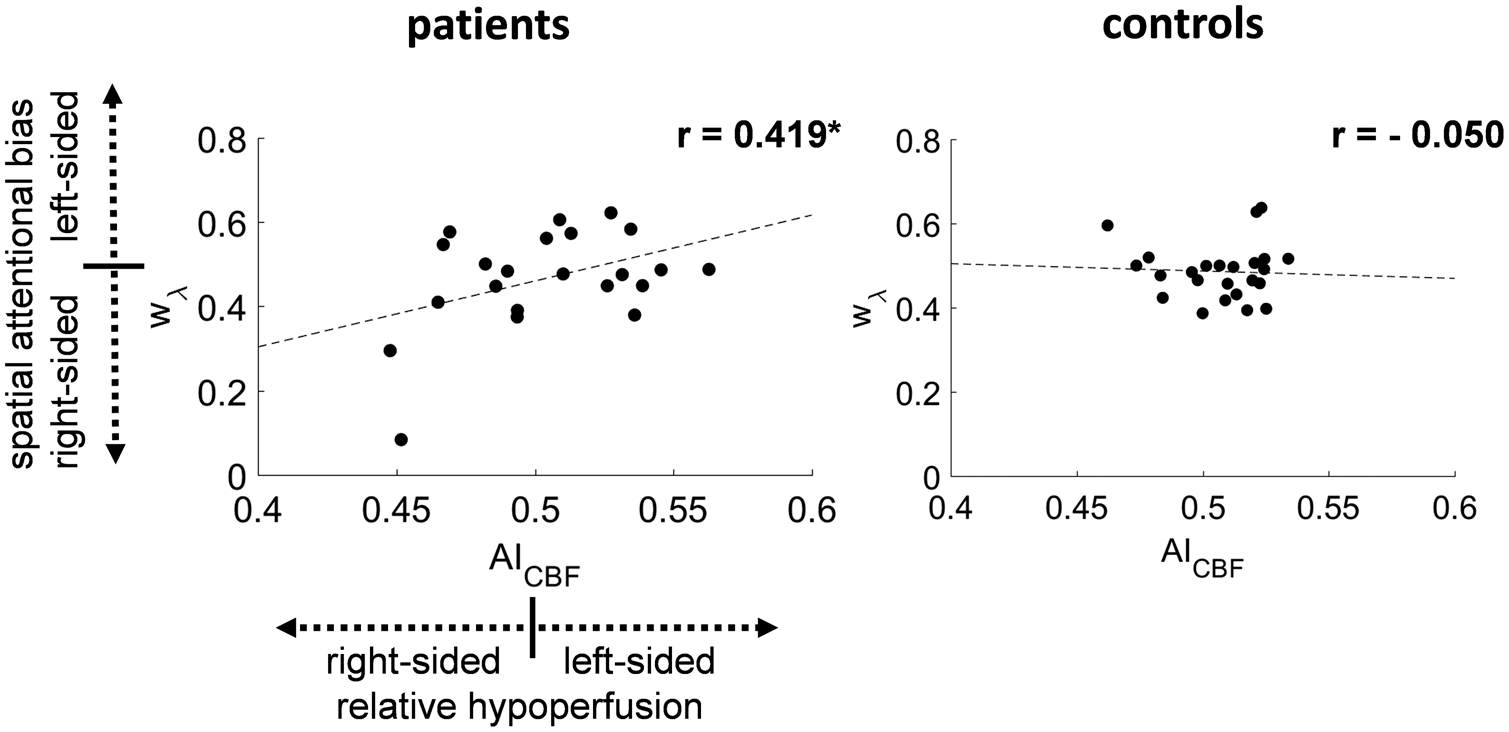
Association of spatial attentional bias and relative hypoperfusion is especially pronounced in parietal cortices
Concerning the regional specificity of results within the anterior circulation, we assessed whether the link between spatial attentional bias and perfusion asymmetries is particularly apparent in the parietal cortex due to its prominent role in attention selection. Control regions were the precentral, frontal and temporal cortex. All volumes of interest lay entirely within the template of the anterior circulation. In patients, the spatial distribution of attention w
λ
and AICBF showed a significant correlation for the parietal cortex (r = 0.368, p < 0.05), while the respective correlations were non-significant for the temporal cortex (r = 0.343, p = 0.06), the precentral gyrus (r = −0.001, p = 0.50) and the frontal lobe (r = 0.220, p = 0.16; Figure 4). In controls, no significant correlation between w
λ
and AICBF was found for the respective brain regions. Thus, the overall positive association between relative hypoperfusion and spatial attentional bias is especially pronounced in parietal cortices in patients with carotid stenosis.
Spatial attentional bias is specifically linked with parietal perfusion asymmetries. To investigate regional specificity of the association of perfusion asymmetries and spatial attentional bias, we analyzed four volumes of interest that lay entirely within the anterior circulation, i.e. parietal, temporal, precentral and frontal cortices. Perfusion asymmetries AICBF were significantly correlated with spatial attentional bias w
λ
within parietal cortices (blue, r = 0.368, p = 0.046), whereas no significant correlation was observed in the temporal cortices (cyan, r = 0.343, p = 0.059), the precentral gyrus (yellow, r = −0.001, p = 0.499) and the frontal cortices (red, r = 0.220, p = 0.163). *Significant Pearson correlation (p ≤ 0.05).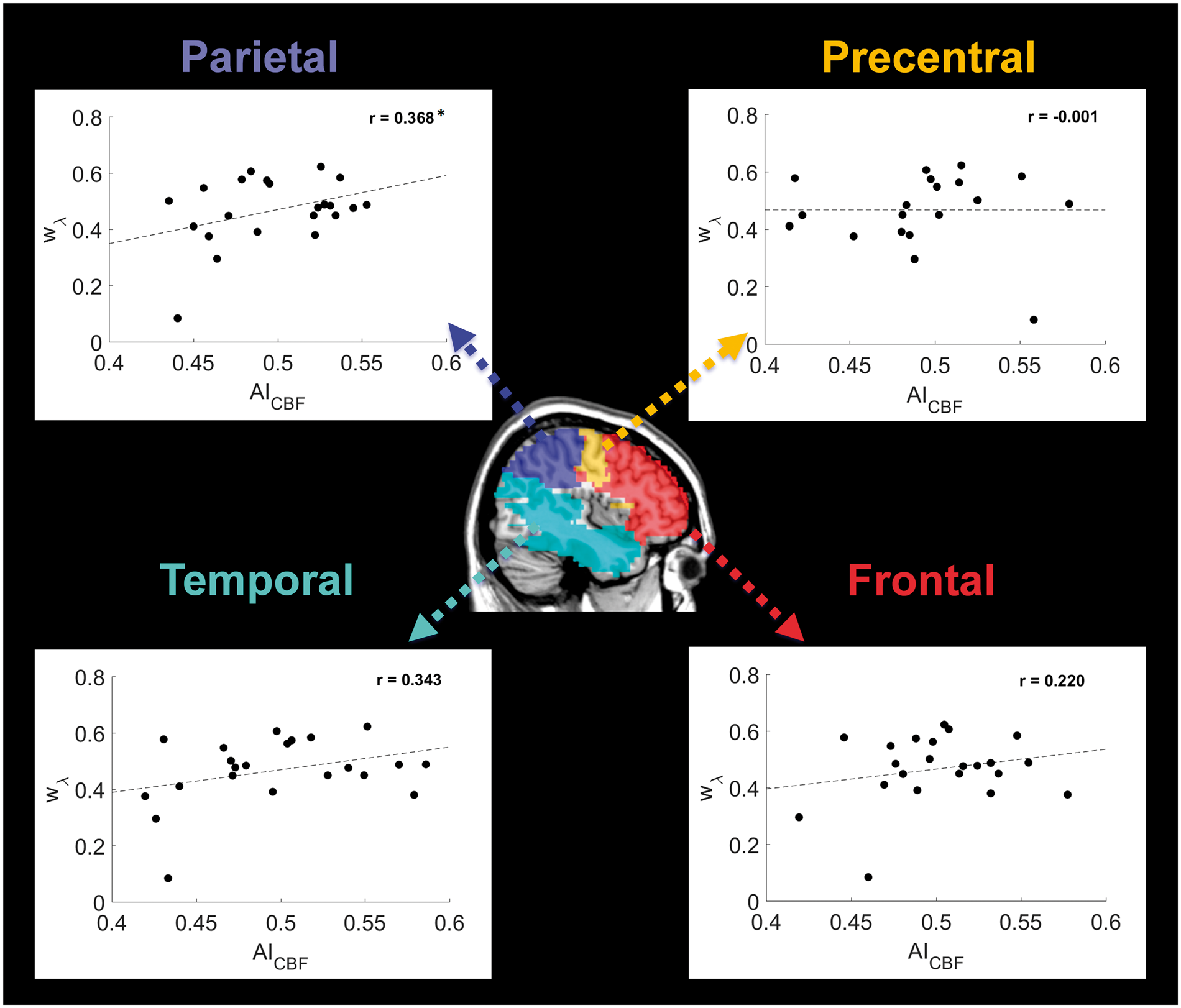
Discussion
This study demonstrated for the first time that one-sided relative hypoperfusion is significantly correlated with increased ipsilateral spatial attentional bias, independently from leukoaraiosis load, in patients with asymptomatic carotid stenosis. The relationship between lateralized perfusion and attention was most pronounced for parietal cortices, well known to be a critical lesion site in patients suffering from visuo-spatial hemi-neglect and/or extinction. 5 This finding suggests a pathophysiological model, according to which carotid stenosis leads to a lateral imbalance of parietal cortical perfusion, which in turn causes subtle spatial attentional bias. Unlike in our experimental partial report task, no group differences were found in the Line Bisection Test, which is a standard paper-and-pencil neglect screening task. This indicates that patients with unilateral stenosis do not show a visual hemi-neglect, but rather suffer from a more subtle spatial attentional bias that can only be revealed with a more sensitive paradigm with time-constraint viewing conditions.
We found that in patients, stronger one-sided relative hypoperfusion was significantly associated with more pronounced spatial attentional bias towards the hemifield ipsilateral to the hypoperfusion (Figure 3). One should note that patients with unilateral extracranial carotid stenosis often exhibit additional stenoses of the brain supplying arteries in more proximal or distal parts of the ipsilateral and/or contralateral common and internal carotid artery or the vertebral arteries (VA). Additionally, individual collateral flow via the circle of Willis is highly variable. Consequently, relative hypoperfusion can also occur on the contralateral side of the stenosis, which was observed in 4 of our 22 patients. Furthermore, bilateral high-grade VA stenosis or one-sided VA stenosis with a contralateral hypoplastic VA might lead to a hypoperfusion of the posterior circulation; however, we did not observe such condition in our study cohort. This means that individual cerebral perfusion patterns cannot easily be inferred with reasonable certainty from knowing the side of the carotid stenosis. Thus, our study was set out to test whether lateralized hypoperfusion – independent from the side of the stenosis – would induce ipsilateral attention bias in patients with carotid stenosis. The specific association of cerebral hypoperfusion and behavioral deficits in the setting of carotid stenosis is elusive, because most of these patients have underlying general atherosclerosis that impacts cognition itself. Therefore, we controlled our analysis by using WMHs as a proxy for atherosclerotic brain damage. We found that the association between lateralized perfusion and attention was independent of WMHs, which were symmetrically distributed across hemispheres (Table 2). This independence suggests that the stenosis-induced impaired hemodynamics have a critical contribution to the behavioral deficits, i.e. the subtle ipsilateral spatial attentional bias. Marshall et al. 27 also showed impaired performance on ‘hemisphere-specific’ cognitive tests (such as Target Cancellation for the right and Boston Naming Test for the left hemisphere) in symptomatic patients with carotid artery occlusion that were associated with an increased oxygen extraction fraction assessed by 15O-PET. The current findings extend these previous findings by demonstrating stenosis-related subtle cognitive effects of relative hypoperfusion even in clinically asymptomatic patients, using model-based parameters of attention functions.
Better object discrimination in one side of space could also result from a basal, unilateral perceptual deficit. In TVA parameters, this would be reflected by lower sensory effectiveness s within one hemifield compared to the other. As we did not find any indication for increased laterality of s values compared to the control group, we can infer that the spatial bias found in the patients with stenosis indeed reflects an attentional, rather than a sensory bias. Furthermore, we did not find significant group differences of top-down control efficiency α (Table 2), general cognitive status, as well as executive and affective functioning (Table 1), which excludes relevant contributions from a generalized attentional selection deficit, cognitive impairments, and mood disturbances. Instead, patients showed a specific association of spatial attention laterality and laterality of perfusion, which was particularly apparent across the parietal cortices (Figure 4). Although the different regions' perfusion in the anterior circulation are not to be expected to vary significantly and the correlative design of our study does not allow inferring clear causal relationships between brain and behavioral measures, this specific relationship indicates that the spatial bias is a consequence of the lateral parietal hypoperfusion induced by a stenosis. Importantly, spatial attentional bias was previously shown to arise not only from unilateral lesions in parietal regions in stroke patients,28,29 but also from imbalanced activity in parietal cortices in patients with early Alzheimer's disease. 30 Taken together, our data suggest an extinction model of carotid stenosis: carotid stenosis causes lateralized perfusion, which in turn seems to cause spatial attentional bias towards the hemifield ipsilateral to the resulting hypoperfusion.
By which neuronal mechanism might relative hypoperfusion cause imbalanced attentional weighting across visual hemifields? Cerebral perfusion and glucose metabolism are intimately linked31,32 and chronic hypoperfusion can result in neuronal hypometabolism and selective neuronal loss without evidence of stroke lesions.33,34 As neuronal metabolism mainly reflects postsynaptic neuronal processes,35,36 in chronically hypoperfused brain regions, a wide-spread postsynaptic gain impairment may be the consequence. According to the neural interpretation of the TVA model, 3 the likelihood of visual objects to win the competition for becoming encoded into visual short-term memory is a function of the number of cortical neurons representing the object and their activation level. Such mechanisms in brain circuits relevant for visual attention are highly dependent on intact postsynaptic gain, which is represented by weighting parameters of visual attention according to the TVA. A spatial imbalance of visual attention might therefore reflect unilateral impairments of postsynaptic activity caused by chronic relative hypoperfusion. And indeed, although ASL only infers tissue metabolism by tissue perfusion, we recently showed that ipsilateral oxygen metabolism was decreased on the side of carotid stenosis in asymptomatic patients, providing a possible link between impaired cognition and stenosis-related hemodynamic changes in patients with carotid stenosis. 37 However, observed flow reductions might also be secondary to underlying brain damage and neuronal loss, i.e. due to reduced oxygen demand. Especially in a later and/or stable stage of the disease, cumulative neuronal damage might be an additional driver of hypoperfusion. Although our analysis of WMHs did not show any significant structural changes both between the affected and unaffected hemisphere in patients as well as between patients and controls, we cannot exclude that this possible mechanism significantly contributes to hypoperfusion. Therefore, further studies with a follow-up design that focus on structural and cognitive changes in the course of the carotid artery disease are needed to disentangle the underlying causes of hypoperfusion. Here, an exhausted cerebral autoregulation as an indicator for reduced perfusion pressure, measured by a vascular dilatory stimulus, might play a key role to detect states of reduced cerebral perfusion pressure. Hence, we currently initiate a follow-up study that includes cognitive measurements as well as CO2-applications and simultaneous perfusion measurements.
An increasing body of evidence suggests that changes in hemodynamics due to stenoses are relevant for cognition, the risk for aggravation of cognitive deficits, and, thus, for developing dementia.7,38,39 Hypoperfusion is potentially reversible by surgical treatment of the stenosis.40–42 However, several studies investigating the effect of interventions on cognition in carotid stenosis patients found controversial results. Some reported improvement of cognitive function,43–46 others did not find any or even adverse effects.47–50 Importantly, only few studies have analyzed hemodynamic and cognitive effects of revascularization therapy. The RECON study investigating patients with more severely affected symptomatic carotid occlusion found that preferentially less impaired hemodynamics at baseline, as measured by oxygen extraction fraction, predicted greater cognitive improvement following extracranial-intracranial arterial bypass surgery compared to medical therapy alone. 50 The cognitive improvements after bypass surgery were not superior to the ones by medical therapy alone. However, in less severely affected patients with asymptomatic carotid stenosis and less invasive therapy options, interventional studies stratifying patients according to their cerebral hemodynamics into groups of different risk levels for cognitive impairment are sorely missing. To date, common criteria for therapeutic decisions account for important factors identified in clinical trials, i.e. the patient's risk for stroke, age, overall health, gender, and life expectancy. 51 Our results suggest that complementing this list by the risk for cognitive impairment might be reasonable. More specifically, the findings of (i) a spatial attentional bias in carotid stenosis patients and of (ii) a significant correlation between the severity of the attentional bias and the ipsilateral relative hypoperfusion has important clinical implications. On the one hand, a pathological bias in spatial attention can lead to significant impairments in daily life functions that depend on accurate and fast perception of stimuli within the affected visual hemifield, ranging from reading to participating in traffic situations.52,53 On the other hand, mild ‘pathological’ attentional bias might indicate an increased risk for further progression of cognitive decline, maybe mediated by the close link between vascular-hemodynamic deficits and neurodegeneration, particularly in Alzheimer's disease. 54 Remarkably, patients with carotid stenosis have a high risk for progressive cognitive decline,6,8 and patients with Alzheimer's disease also show early lateralization of attention.30,55 Thus, lateralized hemodynamics with simultaneously increased spatial attention bias could provide a specific marker for the cognitive implications in the natural course of the disease and could be used to select patients who may benefit from more aggressive treatment. Further longitudinal studies are necessary to test these ideas.
This study has several strengths and limitations. First, major strengths of the rigorous neurocognitive TVA model approach are that it allows for specific assessment of diverse attention functions, such as spatial laterality of attention, and that it is sensitive to even mild attentional changes. Second, a limitation is that CBF reductions should be interpreted with caution. The reported absolute CBF values for the whole anterior circulation are low compared to literature values of gray matter, which results from partial volume effects of white matter and susceptibility artifacts, especially in frontobasal and temporopolar regions as well as the basal ganglia (see Gottler et al. 37 ). However, as we only consider relative side differences of perfusion and not absolute CBF values, these systematical errors should not impact the results. Furthermore, the pCASL signal might also be influenced by an increased ATT on the side of the stenosis. However, we used several strategies to be independent of this effect: we applied a relatively long post-label delay, we visually excluded typical ATT artifacts, and we demonstrated that no group and side differences existed in the spatial covariance of the CBF signal, which has been shown to be related to ATT artifacts. Third, as labeling efficiency is dependent on flow velocity, which can be increased distal to a stenosis, label efficiency might be reduced. However, the labeling plane was positioned at least 20 mm distal to the stenosis based on a phase contrast angiography survey, where mean flow velocity is not supposed to be significantly increased. 56 Fourth, according to the ASL consensus paper by Alsop et al., 15 M0 should be corrected for T1 effects if TR is below 5000 ms. In our case, we used a TR of 4377 ms due to software constraints, resulting in a correction factor of 1.05 (assuming a T1 in gray matter at 3 T of approx. 1500 ms), which would decrease global CBF by 5%. However, this should not affect our results as we only focused on relative lateralization of perfusion. Fifth, there is a high variability of carotid perfusion territories due to anatomical variants of the Circle of Willis and also recruitment of collaterals due to stenosis-associated reduced perfusion pressure. The applied mask therefore can only serve as an approximation of the individual perfusion territory and does not account for individual vascular territory variations or shifts. Finally, the question whether long-standing perfusion reductions cause progressive cognitive decline can only be answered in a longitudinal follow-up study that investigates effects of hemodynamic impairment on brain structure and function.
Conclusion
Taken together, the results of this study indicate that lateralized perfusion induced by unilateral stenosis is associated with spatial attentional bias towards the side of relative hypoperfusion, and that this relationship is independent from WMHs as a proxy for atherosclerotic brain lesions. These findings suggest that stenosis-induced impaired hemodynamics independently contribute to subtle cognitive deficits. Thus, simultaneous one-sided hypoperfusion and attentional bias may serve as a biomarker for the identification of those patients with clinically asymptomatic stenosis who have an increased likelihood of further cognitive decline and who might benefit from more aggressive treatment.
Supplemental Material
Supplemental material for The stronger one-sided relative hypoperfusion, the more pronounced ipsilateral spatial attentional bias in patients with asymptomatic carotid stenosis
Supplemental Material for The stronger one-sided relative hypoperfusion, the more pronounced ipsilateral spatial attentional bias in patients with asymptomatic carotid stenosis by Jens Göttler, Stephan Kaczmarz, Rachel Nuttall, Vanessa Griese, Natan Napiórkowski, Michael Kallmayer, Isabel Wustrow, Hans-Henning Eckstein, Claus Zimmer, Christine Preibisch, Kathrin Finke and Christian Sorg: On behalf of the ESO-SAFE Secondary Prevention Survey Steering Group in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Research Foundation (grant no. FI 1424 to K.F., PR 1039/6-1 to C.P., and grant no. SO 1336/4-1 to C.S.) and further supported by the Faculty of Medicine of the Technische Universität München (grant to J.G.: KKF E12), by the Dr.-Ing. Leonhard Lorenz-Stiftung (grant to J.G.: 915/15), by the Friedrich-Ebert-Stiftung for S.K., and by a postdoc fellowship for J.G. of the German Academic Exchange Service (DAAD).
Acknowledgements
We thank Kim van de Ven for her support to implement the ASL sequence.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors' contributions
J.G., S.K., C.P., K.F. and C.S. designed the study, acquired, analyzed and interpreted the data, and drafted the article. R.N., V.G., N.N., M.K., I.W., HH.E., and C.Z. made a substantial contribution to the acquisition or analysis and interpretation of data, and critically revised the article for important intellectual content. All authors approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.