
Abstract
Ambulatory blood pressure (ABP) reflects the end-organ vascular stress in daily life; however, its influence on brain neuronal fiber integrity and cerebral blood flow (CBF) remains unclear. The objective of this study was to determine the associations among ABP, white matter (WM) neuronal fiber integrity, and CBF in older adults. We tested 144 participants via ABP monitoring and diffusion tensor imaging. The total level and pulsatile indices of CBF were measured by phase-contrast MRI and transcranial Doppler, respectively. Neuropsychological assessment was conducted in 72 participants. Among ambulatory and office BP measures, elevated 24-h pulse pressure (PP) was associated with the greatest number of WM skeleton voxels with decreased fractional anisotropy (FA) and increased mean diffusivity (MD). Furthermore, these associations remained significant after adjusting for age, antihypertensive use, aortic stiffness, WM lesion volume, and office PP. Radial diffusivity (RD) was elevated in the regions with decreased FA, while axial diffusivity was unaltered. The reduction in diastolic index explained a significant proportion of the individual variability in FA, MD, and RD. Executive function performance was correlated with WM fiber integrity. These findings suggest that elevated ambulatory PP may deteriorate brain neuronal fiber integrity via reduction in diastolic index.
Introduction
The aging brain may be vulnerable to increased arterial pulsatility.1,2 After middle age, central arterial stiffening contributes to the widening of pulse pressure (PP) as a consequence of increasing systolic blood pressure (SBP) and decreasing diastolic BP (DBP). 3 In older adults, elevated PP has been linked to higher incidences of stroke, cognitive impairment, and cardiovascular mortality independently from mean arterial pressure (MAP).4,5 Hypothetically, elevated PP transmitted into the brain may damage the underlying neuronal tissues via alteration of cerebral blood flow (CBF).1,2
BP fluctuates substantially in daily life, 6 thus its snapshot measurement at clinical office alone may not represent the cumulative effect on the brain. 7 Indeed, the progression of white matter (WM) lesions has been shown to correlate with the daily average BP, but not office BP. 8 WM lesions (e.g. hyperintensity signals in T2-weighted MR images) are associated with accelerated cognitive decline and likely to reflect cerebral small vessel disease. 9 Therefore, identification of individuals with elevated risk for developing WM lesion may lead to an earlier preventive therapy and slow the process of cognitive decline and impairment.
MR diffusion tensor imaging (DTI) can detect microstructural WM abnormalities preceding the lesions10,11 and further probe into the neurobiological mechanism(s) of axonal fiber damage.12,13 Specifically, it has been shown that lower fractional anisotropy (FA) and higher mean diffusivity (MD) indicate the overall reduction in WM fiber integrity, 12 and elevated radial (RD) and axial (AxD) diffusivities may, at least in part, reflect axonal demyelination and/or degeneration.14,15
To date, the influence of ambulatory BP (ABP) on DTI metrics of WM fiber integrity has not been studied. In addition, we do not know which BP parameter(s) is associated with DTI metrics and whether alteration of CBF accounts for their variabilities. The purpose of this study was to determine the associations among BP (including ambulatory and office measures), WM fiber integrity, and CBF in older adults. We hypothesized that (1) elevated 24-h PP is associated with the reduction in WM neuronal fiber integrity, as manifested by the lower FA and higher MD and (2) elevated 24-h PP is correlated with augmented CBF pulsatility which in turn explains the reduction in WM fiber integrity. In addition, we examined the correlation between neuropsychological performance and WM fiber integrity in a subgroup of participants.
Material and methods
Participants
We used data obtained from the baseline testing of longitudinal studies conducted in cognitively normal (CN) adults and patients with mild cognitive impairment (MCI). In total, 94 CN adults and 50 MCI patients had complete dataset for analysis, except for neuropsychological assessment that was available in 72 participants (22 CN and 50 MCI, Table S1). All participants were recruited through a community-based advertising in the Dallas-Fort Worth metropolitan area. Inclusion criteria were men and women aged 55–80 years with normal cognitive function or MCI. Exclusion criteria included a history of cardiovascular (e.g. angina, myocardial infarction), cerebrovascular, or psychiatric disease, uncontrolled hypertension or dyslipidemia, diabetes mellitus, obesity (body mass index > 35 kg/m2), current or a history of smoking within the past two years, or chronic inflammatory disease. Individuals with a pacemaker or any metal in their body that precludes MRI were also excluded. The diagnosis of MCI was based on the Petersen criteria, 16 as modified by the Alzheimer's Disease Neuroimaging Initiative project (http://adni-info.org). Specifically, MCI patients had to meet the following criteria: (1) subjective memory complaint, (2) a global Clinical Dementia Rating of 0.5 with a score of 0.5 in the memory category, (3) objective memory loss as indicated by the Logical Memory subtest of the Wechsler Memory Scale-Revised, and (4) Mini-Mental State Exam score between 24 and 30. This study was approved by the Institutional Review Board of the University of Texas Southwestern Medical Center and Texas Health Presbyterian Hospital Dallas and was performed in accordance with the guidelines of the Declaration of Helsinki and Belmont Report. All subjects gave informed written consent before participation.
Data collection and analysis
Each participant underwent MRI and cerebral hemodynamic assessment. MRI was performed on a 3-Tesla scanner (Philips Medical System, Best, The Netherlands) using whole body coil transmission and an 8-channel head coil reception. The detailed information of each MRI sequence is provided in the Data Supplement. Cerebral hemodynamic assessment was performed in an environmentally controlled room. All laboratory data were collected in the supine position after abstaining from alcohol, caffeinated beverages, and intense physical activity for >12 h.
WM fiber integrity
DTI scan was performed twice with a single-shot echo-planar imaging sequence with a sensitivity encoding parallel imaging scheme. Diffusion weighing was encoded along 30 independent orientations. The FMRIB Software Library (FSL, https://surfer.nmr.mgh.harvard.edu/fswiki) was used for image preprocessing and voxelwise statistical analysis. 17 First, two scans of DTI data were averaged to increase the signal-to-noise ratio. Next, a brain mask was created by the Brain Extraction Tool and the DTI data fitting algorithm was used to calculate DTI metrics of FA, MD, RD, and AxD. Individual FA, MD, RD, and AxD images were visually inspected to detect artifacts and subsequently analyzed by voxelwise and region-of-interest (ROI) statistics.
To perform voxelwise and ROI statistics, individual FA images were eroded slightly, zeroed the end slices to remove likely outliers from the diffusion tensor fitting, and registered into the JHU-ICBM-FA template as a common space. 18 The JHU template was used to corroborate the results of voxelwise statistics and ROI analysis. The mean FA image was created and thinned to generate a mean FA skeleton which represents the center of WM tracts common to all participants. We set a threshold for voxels with FA value greater than 0.20 to minimize partial volume effects from gray matter and cerebrospinal fluid. The resulting mean FA skeleton included 128,926 1 × 1×1 mm WM skeleton voxels. Finally, individual MD, RD, and AxD images were projected onto the mean FA skeleton and fed into voxelwise and ROI-based cross-subject statistics. ROI analysis was performed using the ICBM-DTI-81 White-Matter atlas. 18
WM lesion
The WM lesion volume was measured by hypointensity signals in T1-weighted image and normalized to intracranial volume. 19 FreeSurfer software (http://ftp.nmr.mgh.harvard.edu) was used for brain tissue segmentation and volume calculation. 20 WM hypointensities in T1-weighted images have been shown to have similar spatial distribution and volume to those measured by hyperintensities in T2-weighted images (e.g. FLAIR),21,22 as confirmed by our data in a subset of study participants (n = 68, Figure S1).
Cerebral hemodynamics
Non-gated phase-contrast MRI (PC-MRI) was collected four times at different stages of the cardiac cycle (time interval = 6.5 s) and averaged to generate a single image. 23 Total CBF (TCBF) was calculated as a sum of the blood flow in the bilateral internal carotid and vertebral arteries. Cerebrovascular resistance was calculated by dividing MAP by TCBF.
Transcranial Doppler was used to record CBF velocity (CBFV) waveform from the middle cerebral artery (TCD, DWL, Singen, Germany). The pulsatile indices of CBFV were calculated as the ratio of systolic, diastolic, and pulsatile CBFVs to the mean CBFV based on the following equations.
23
TCD data were inspected visually to exclude artifacts and analyzed offline (Acknowledge, BIOPAC Systems, Goleta, CA, USA).
Blood pressure and aortic stiffness
ABP was recorded for ≥24 h using a non-invasive oscillometric BP monitoring (Suntech Medical Instruments, Morrisville, NC, USA). 24 Each participant wore a brachial cuff on their non-dominant arm. Measurements were made every 30 min during the individually scheduled awake period and every 60 min during the scheduled sleep period. ABP data are reported as an average of 24-h measurement to represent the cumulative effect of BP on the brain. Sleep BP dip was calculated according to the standard guideline. 25 Office BP and heart rate were measured during a laboratory visit in the seated position using an ECG-gated electro-sphygmomanometer (Suntech). Aortic stiffness was measured by carotid-femoral pulse wave velocity based on the standard procedure. 26
Statistical analyses
CN and MCI participants were similar in age, ambulatory and office BP, WM integrity assessed by DTI and lesion volume, and CBF measures (Table S1); hence, both groups were combined for subsequent analyses.
We first conducted voxel-based linear regression analysis of FA and MD with ambulatory and office BP parameters using tract-based spatial statistics (TBSS). 27 In TBSS, multiple comparisons were corrected by threshold-free cluster enhancement with 5,000 permutations. 28 The corrected statistical maps were thresholded by P < 0.05. Subsequently, we compared the number of significant FA and MD voxels associated with each BP parameter.
The individual mean values of FA and MD were extracted from the significant TBSS skeletons for further analysis. Multiple linear regression analysis was performed to examine the statistical effects of 24-h PP and covariates. The covariates were selected based on the tertile comparison of 24-h PP which used one-way analysis of variance or chi-squared test. Office PP was also entered in the model to determine the independent effect of 24-h PP.
To examine the potential underlying mechanism of altered WM fiber integrity, the individual mean values of RD and AxD were extracted from the regions of significant FA voxels. These RD and AxD values were compared among the 24-h PP tertiles using general linear model.
Cerebral hemodynamic data were first compared among the 24-h PP tertiles and further analyzed by stepwise linear regression. In the stepwise model, DTI metrics were entered as dependent variable while TCBF, cerebrovascular resistance, and pulsatility indices were entered as independent variable.
The correlation between WM fiber integrity and neuropsychological performance was tested in 72 participants (22 CN and 50 MCI) using partial correlation adjusted for age, sex, and education. In all analyses, the Bonferroni correction was applied for multiple pairwise comparisons. Statistical significance was set a priori at P < 0.05. SPSS 20 was used for analyses (SPSS Inc., Chicago, IL, USA).
Results
ABP and WM fiber integrity
Summary of tract-based spatial statistic analyses demonstrating the number of significant white matter skeleton voxels with fractional anisotropy and mean diffusivity along with their correlational directions.
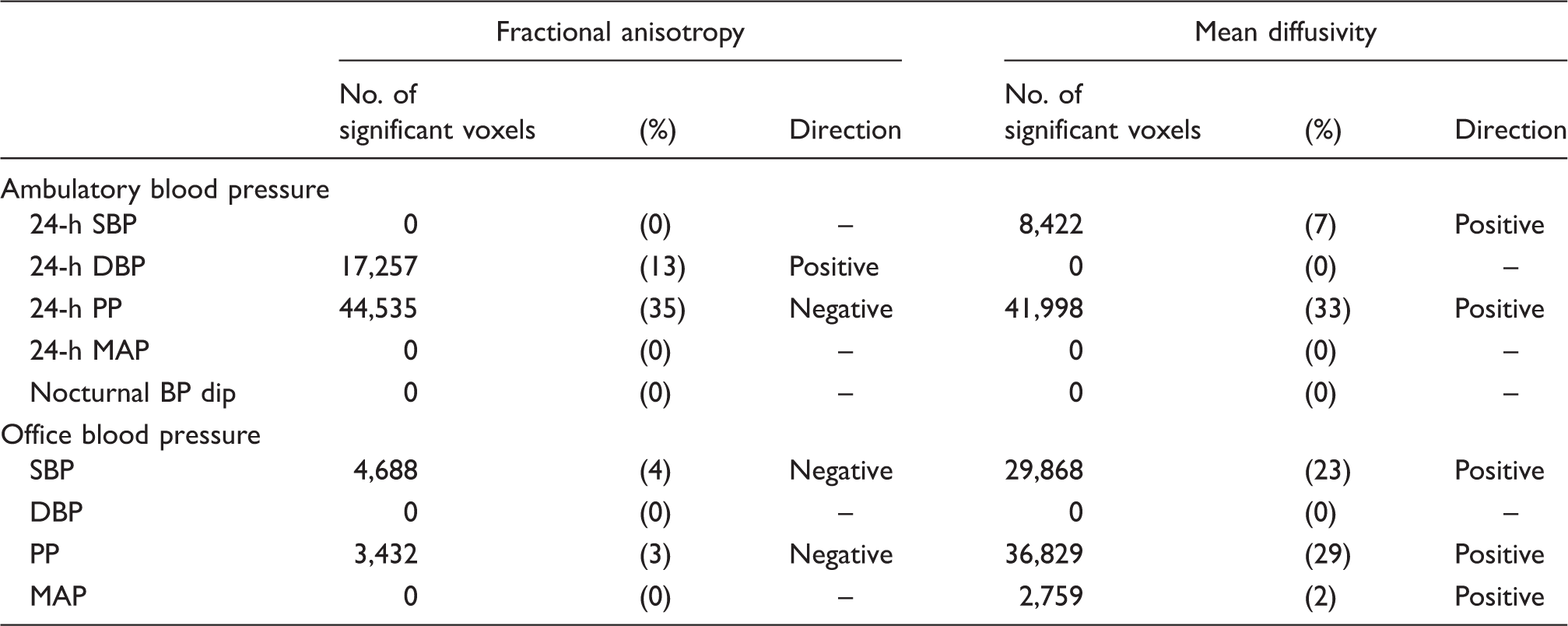
Note. (%) represents the percent of significant white matter skeleton voxels relative to the total count (i.e. 128,926 voxels). Analysis included 144 participants. BP: blood pressure; DBP: diastolic BP; MAP: mean arterial pressure; PP: pulse pressure; SBP: systolic BP.
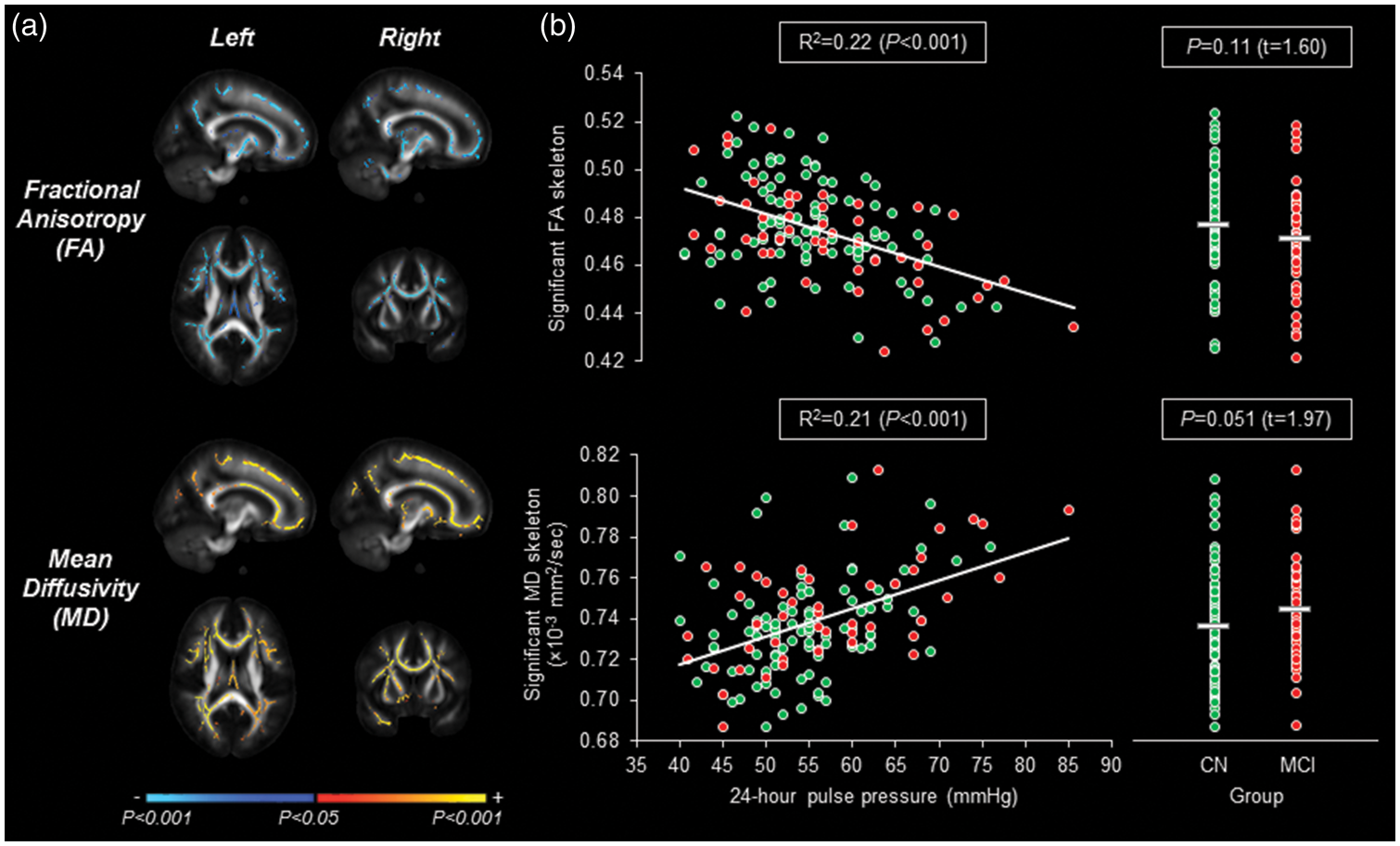
(a) Tract-based spatial statistic maps demonstrating the association of 24-h pulse pressure with fractional anisotropy (FA) and mean diffusivity (MD). The color bar indicates the directionality and P value of their associations. (b) Scatter plots show the correlations of FA and MD with 24-h pulse pressure (green: cognitively normal (CN) and red: mild cognitive impairment (MCI)). The individual mean values of FA and MD were extracted from the significant white matter skeletons. Horizontal line shows a mean value for CN and MCI groups. Analysis included 94 CN adults and 50 patients with MCI.
Subject demographics and cardiovascular variables in 24-h pulse pressure tertiles.
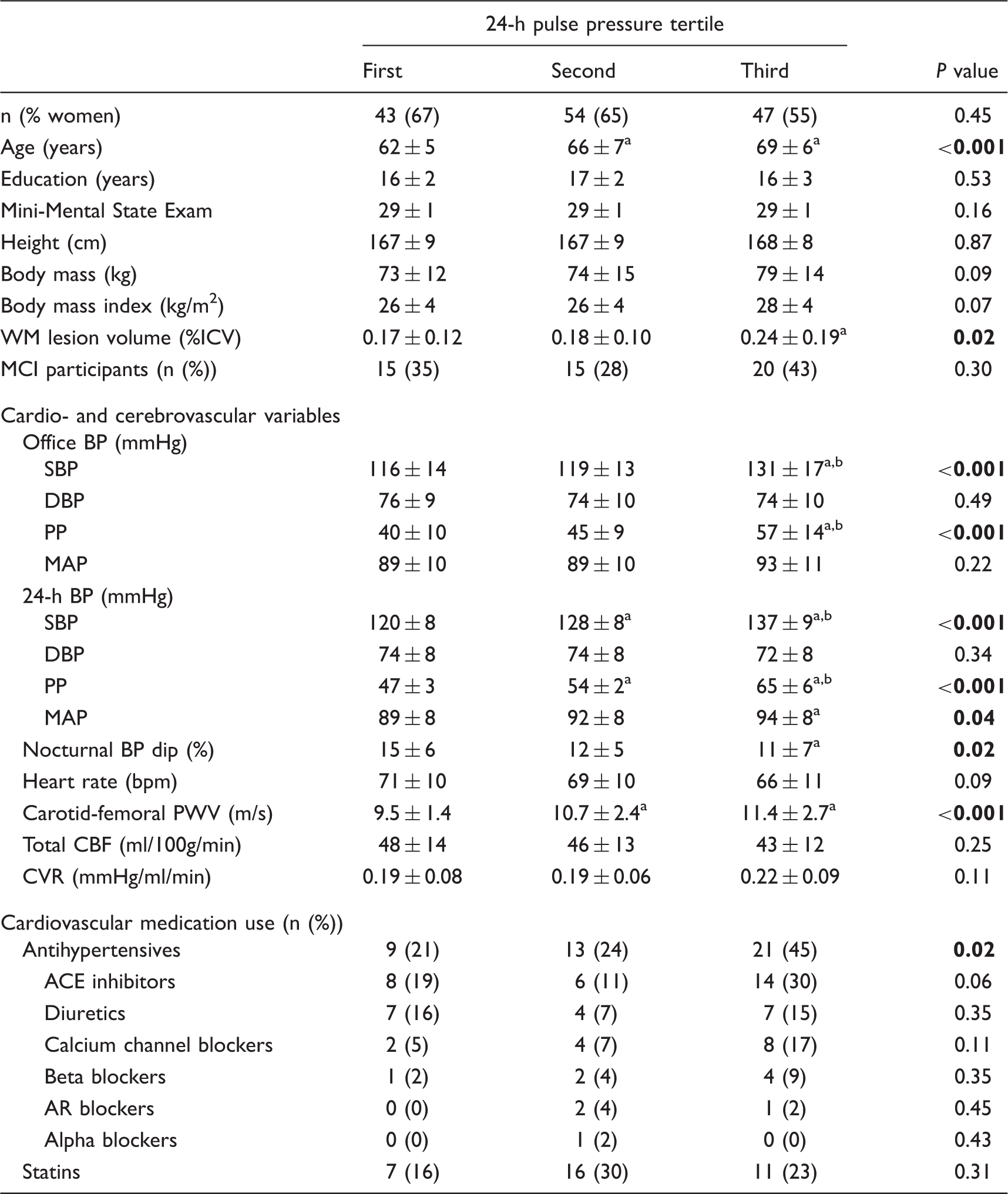
Note. Values are mean ± standard deviation. Tertile range: first<51 mmHg, second=51–57 mmHg, and third>57 mmHg. P values in boldface represent statistical significance (P < 0.05) with the Bonferroni correction. ACE: angiotensin-converting enzyme; AR: angiotensin receptor; BP: blood pressure; CBF: cerebral blood flow; CVR: cerebrovascular resistance; DBP: diastolic BP; ICV: intracranial volume; MAP: mean arterial pressure; MCI: mild cognitive impairment; PP: pulse pressure; PWV: pulse wave velocity; SBP: systolic BP; WM: white matter.
vs. first tertile.
vs. second tertile.
Hierarchical multiple linear regression analysis of white matter diffusion metrics.
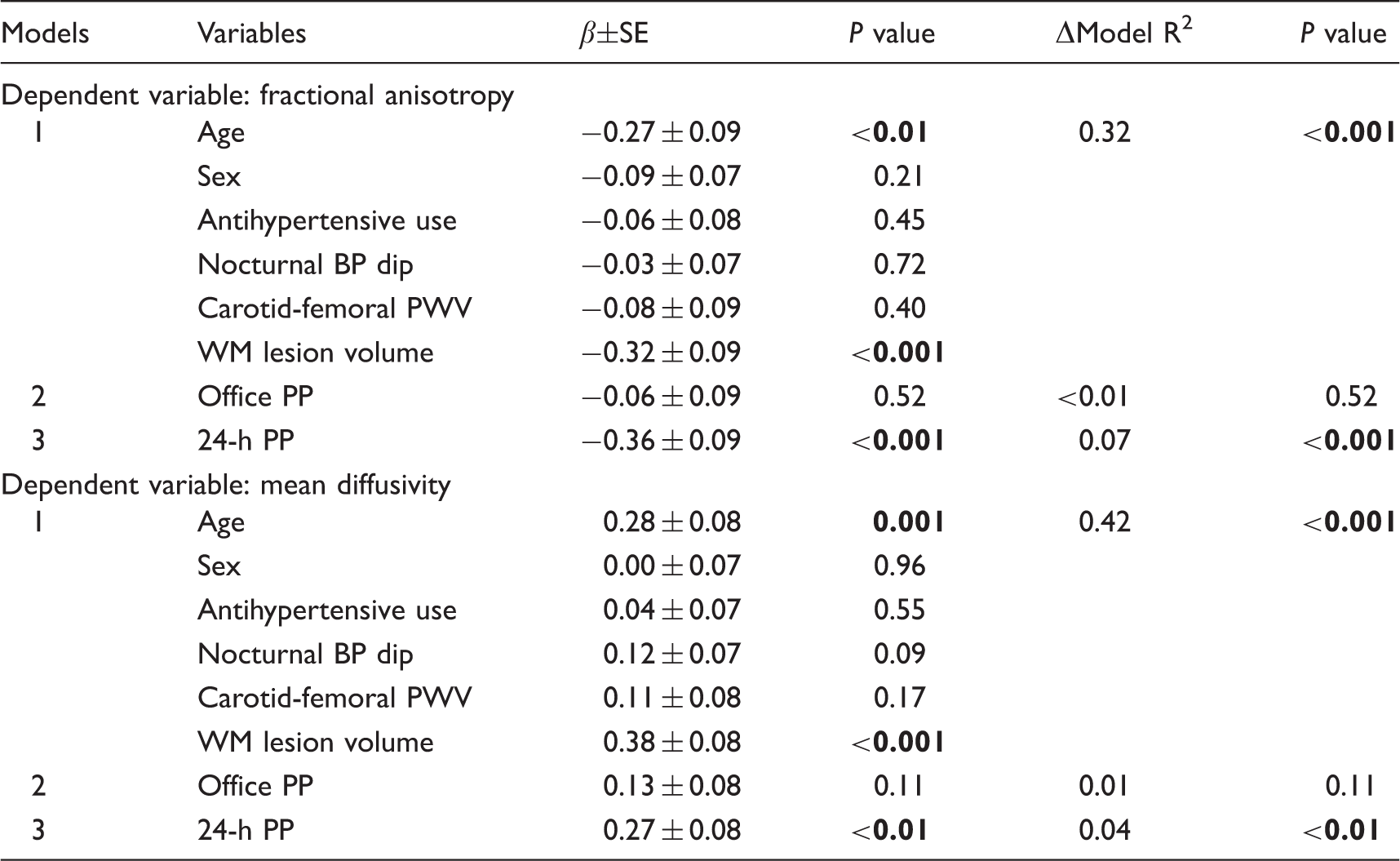
Note. Diffusion metrics were extracted from significant WM skeletons presented by Figure 1(a). P values in boldface represent statistical significance with the Bonferroni correction (P < 0.025 ( = 0.05/2)). Sex was entered as men=0 and women=1. WM lesion volume was log-transformed before analysis. Analysis included 144 participants. β: standardized beta coefficient; BP: blood pressure; PP: pulse pressure; PWV: pulse wave velocity; SBP: systolic BP; SE: standardized error; WM: white matter.
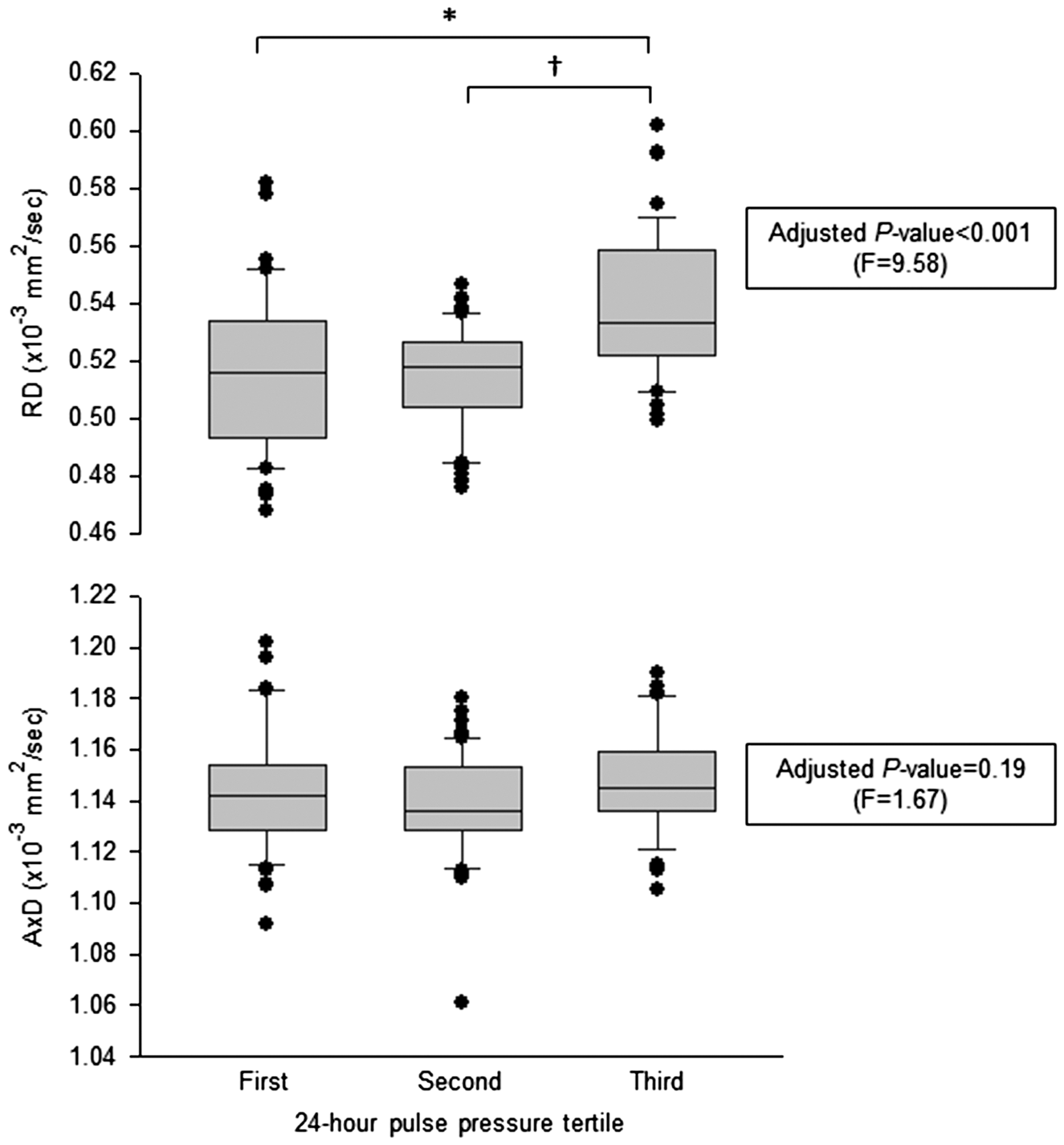
Radial (RD) and axial (AxD) diffusivities compared among the 24-h pulse pressure tertiles. The individual mean values of RD and AxD were extracted from the significant fractional anisotropy voxels, as shown in Figure 1(a). P values are adjusted for age, sex, antihypertensive use, sleep blood pressure dip, carotid-femoral pulse wave velocity, white matter lesion volume, and office pulse pressure. *vs. first tertile. †vs. second tertile. Tertile range: first<51 mmHg (n = 43), second = 51–57 mmHg (n = 54), and third>57 mmHg (n = 47).
CBF and neuropsychological performance
Participants in higher 24-h PP tertiles showed the elevated systolic and pulsatile but reduced diastolic indices with adjustment for age, sex, antihypertensive use, sleep BP dip, carotid-femoral PWV, WM lesion volume, and office PP (Figure 3). TCBF and cerebrovascular resistance were similar across the tertiles (Table 2). These observations were also confirmed by multiple linear regression analysis (Table S4).
The pulsatile indices of cerebral blood flow compared among the 24-h pulse pressure tertiles. P values are adjusted for age, sex, antihypertensive use, sleep blood pressure dip, carotid-femoral pulse wave velocity, white matter lesion volume, and office pulse pressure. *vs. first tertile. †vs. second tertile. Tertile range: first<51 mmHg (n = 43), second = 51–57 mmHg (n = 54), and third>57 mmHg (n = 47).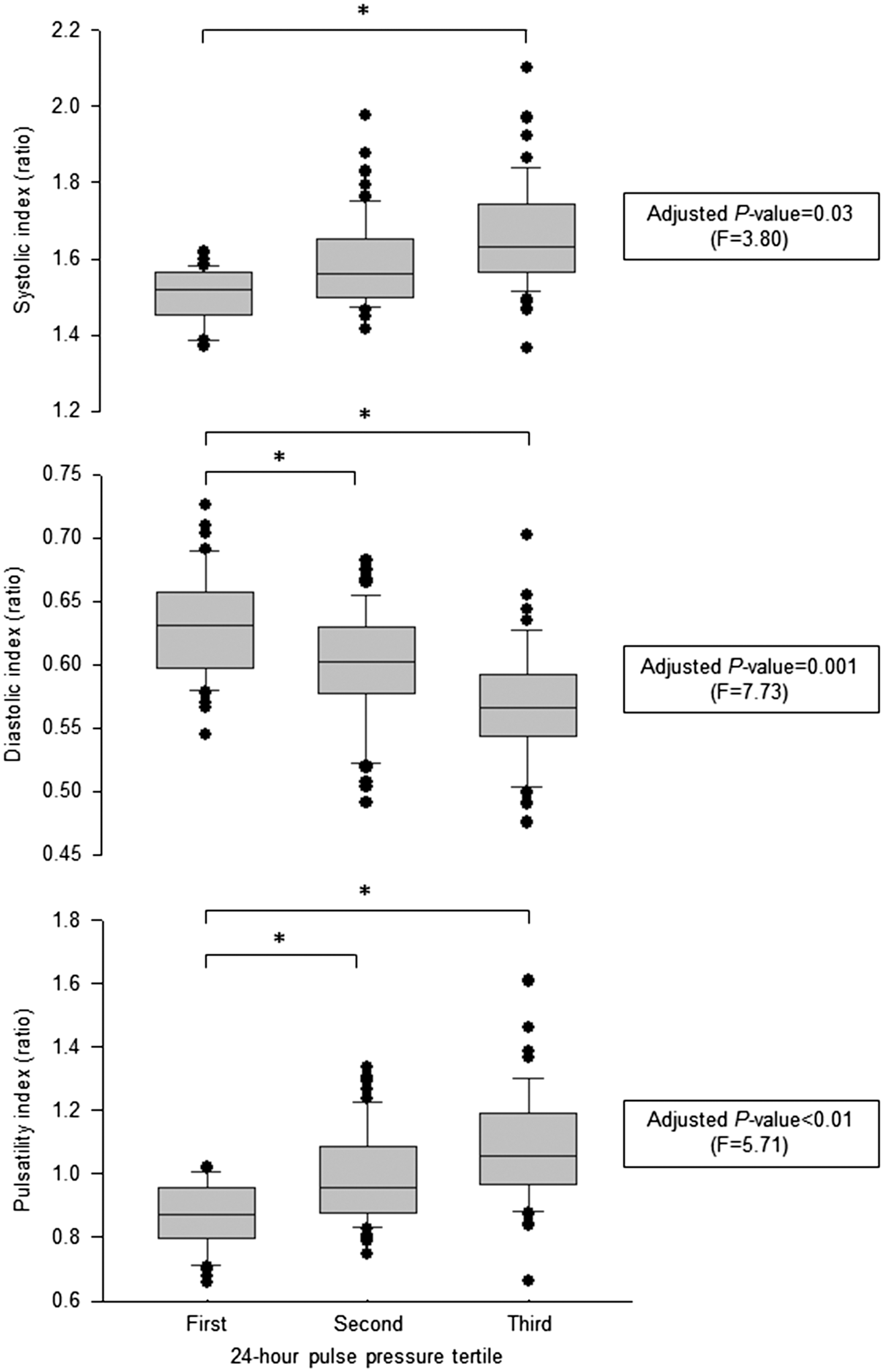
Stepwise linear regression analysis of white matter diffusion metrics and cerebral blood flow.
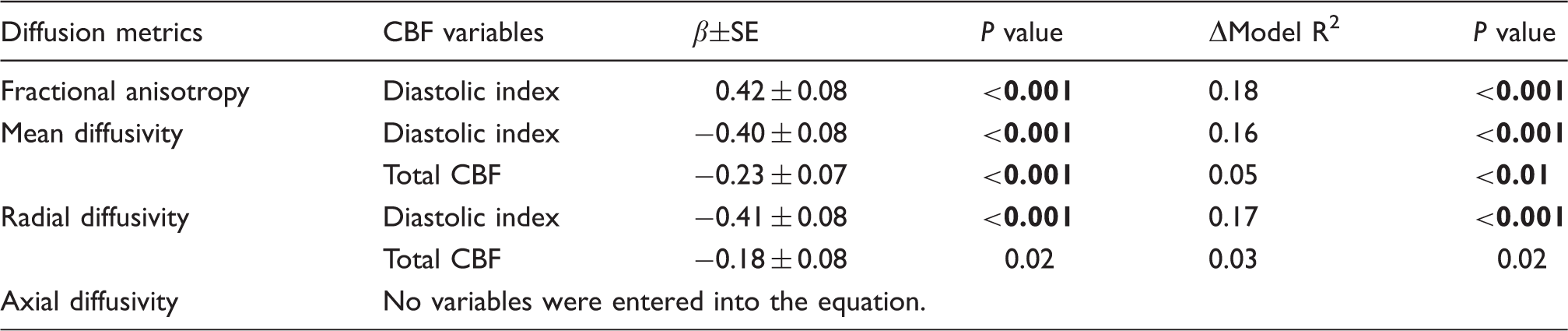
Note. Stepwise method was used to enter CBF variables. Fractional anisotropy and mean diffusivity were extracted from the significant voxels presented by Figure 1(a). Radial and axial diffusivities were extracted from the significant fractional anisotropy voxels. P values in boldface represent statistical significance with the Bonferroni correction (P < 0.0125 ( = 0.05/4)). Analysis included 144 participants. β: standardized beta coefficient; CBF: cerebral blood flow; SE: standardized error.
Higher RD was correlated with worse performance in executive function, as measured by Trail Making Test part B, with adjustment for age, sex, and education (Table S6).
Discussion
The main findings from this study are as follows. First, among the ambulatory and office BP measures, elevated 24-h PP is associated with the reduced WM neuronal fiber integrity, independently of age, antihypertensive use, aortic stiffness, and WM lesion volume. Second, participants with elevated 24-h PP have higher systolic and pulsatile but lower diastolic indices. Moreover, lower diastolic index accounted for the reduction in WM fiber integrity. Finally, deterioration of WM fiber integrity is associated with worse performance of executive function in a subgroup of study participants. Overall, these findings support our hypothesis that age-related increase in arterial pulsatility, as assessed by elevated ambulatory PP, is associated with the reduction in WM neuronal fiber integrity.
ABP has a better prognostic value for cardio- and cerebrovascular mortality than office BP.7,29 The present study extended these previous observations by examining the relation between ABP and WM fiber integrity. The finding that among BP measurements, 24-h PP is the independent correlate of WM fiber integrity suggests that the aging brain is vulnerable to elevated arterial pulsatility in daily life. Overall, our findings are supported by previous studies demonstrating that (1) higher ambulatory PP is associated with increased risk of cognitive impairment, 30 (2) elevations of central PP and CBF pulsatility are associated with higher incidences of cerebral small vessel disease,31,32 and (3) CBF pulsatility is correlated with WM microstructural integrity. 33 The novel and important observation of the current study is that it is the 24-h PP and the diastolic index that are related to WM fiber integrity. In addition, the correlation between neuropsychological performance and WM fiber integrity underscores the clinical relevance of our findings.
RD was increased in the regions where higher 24-h PP is associated with lower FA. FA is calculated based on the directionality of water diffusion along the axonal fiber tract and influenced by the degrees of cellular integrity and alignment. 12 FA expressed in normalized unit is the most widely used DTI metric and reflects the overall integrity of WM axonal tract. 12 On the other hand, RD is a measure of directional water diffusion perpendicular to the main axis of WM fiber tract and has been shown to reflect the level of axonal myelination.14,15 For example, spinal cords autopsied from multiple sclerosis patients demonstrated the elevation of RD accompanied by axonal demyelination. 14 In addition, histological study of the optic nerve exposed to retinal ischemia showed an elevation of RD that occurred with axonal demyelination. 15 Therefore, our findings suggest axonal demyelination as one of the potential mechanisms underlying the reduced WM integrity, although further studies are needed to confirm the neurobiological underpinning of DTI metrics.
This is the first study to investigate the association of WM fiber integrity with the pulsatile components of CBF, including systolic, diastolic, and pulsatility indices. Our recent study demonstrated that pulsatility index increases with age as a result of increasing carotid PP. 23 The present study extended these observations by showing that elevated 24-h PP is associated with increased systolic and pulsatile but reduced diastolic indices. Mechanistically, age-related central arterial stiffening and premature arterial pressure wave reflection may augment systolic but attenuate diastolic portions of CBF. 23 Furthermore, using stepwise regression analysis, we found that among CBF measurements, diastolic index accounts for 18%, 16%, and 17% of the individual variability in FA, MD, and RD, respectively. These findings have potential implications that the relative reduction in diastolic CBF could represent a sensitive hemodynamic marker for brain damage, particularly the WM microstructural abnormalities. Although the exact mechanism remains unknown, the presence of substantial beat-to-beat diastolic CBF reduction may cause intermittent hypoperfusion and impair substrate exchange and clearance of neuronal waste products during each cardiac cycle, leading eventually to neuronal damage and dysfunction.34,35
The WM fiber tracts associated with 24-h PP exhibited an anterior-to-posterior gradient. The individually extracted FA and MD values were also correlated with executive function performance. Consistently, a recent Framingham study demonstrated an association between SBP and FA in the frontal WM regions. 36 The frontal-striatal circuit underlies a neuronal substrate of executive function and is particularly vulnerable to age and cardiovascular risk factors (e.g. hypertension). 37 This study provides further evidence that 24-h PP is likely to be one of the important cardiovascular risk factors for brain structural integrity and cognitive function.
The lack of significant differences in global WM fiber integrity between CN and MCI participants was unexpected, although we observed a trend of decreased FA and increased MD in MCI compared with CN participants (Figure 1b). The previous DTI studies that compared MCI patients with age-, sex-, and education-matched CN participants generated mixed findings and their differences are likely to depend on the severity of cognitive impairment.38–40 Our MCI participants had a mean MMSE score of 29 (a global neurocognitive function assessment) that is a similar score to CN participants (P = 0.65 based on unpaired t-test, Table S1). Hence, differentiation of MCI and CN participants using DTI was potentially limited at the early phase of MCI in our study. In addition, a lack of statistical power due to limited sample size and/or other coexisting brain pathologies (e.g. cortical amyloid and/or tau depositions) may account for the absence of group difference. 41
This study is strengthened by the use of multimodal physiological approach. ABP represents the cumulative, vascular stress in daily life, which is clinically relevant as ABP has been shown to have a better prognostic value for cardio- and cerebrovascular mortality.7,29 DTI provides quantitative metrics that are sensitive to neurobiological alterations of WM fiber tract. The complementary use of PC-MRI and TCD increases spatial and temporal resolutions in characterizing the dynamic and static profiles of CBF. The inclusion of MCI participants may increase the generalizability of our findings to older populations in community settings. 42
There are several study limitations. First, this is a cross-sectional study with a small sample size which limits an interpretation of causal relations. Future intervention studies need to confirm whether pharmacological or non-pharmacological treatment of PP would improve WM fiber integrity, CBF profile, and cognitive performance. Second, assessment of WM microstructural integrity using DTI may be limited by the anatomical orientation of WM fibers. For example, crossing fibers are common in the brain WM and may influence DTI metrics (e.g. FA) independent of their structural integrity. 43 Also, increasing brain tissue motion with elevated PP may lead to phase change and intravoxel signal loss, although the magnitude of its effect is less clear and may be small due to the presence of less blood vessels in the WM compared with the gray matter. 44 Third, WM lesion assessment based on hypointensity signals in T1 images may not be as sensitive as the assessment using T2 images. In this study, T2-weighted FLAIR images were not available from all participants; however, we observed that lesion volume and spatial distribution measured by both imaging methods were similar in a subgroup of participants (Figure S1), as confirmed by several other studies.21,22 Fourth, the correlations between DTI metrics and neuropsychological test scores were modest and not available in all participants.
Conclusions
This study demonstrated that among ambulatory and office BP measures, 24-h PP is associated with brain neuronal fiber integrity, independently from age, antihypertensive use, aortic stiffness, WM lesions, and office PP. The elevated RD within the regions of decreased FA may suggest axonal demyelination as a potential mechanism of the WM fiber damage. The diastolic index was decreased in the individuals with elevated 24-h PP and accounted for the reduction in WM fiber integrity. Although longitudinal studies need to confirm our findings, these results suggest that augmented ambulatory PP in daily life may elevate the risk of WM fiber damage and ABP monitoring may help identify the individuals at risk for brain structural and functional impairments.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the National Institute of Health (R01AG033106, R01HL102457, and K99HL133449) and the American Heart Association (14POST20140013).
Acknowledgments
The authors would like to thank the study participants for their time and effort.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
Study concept and design: Dr Tarumi and Dr Zhang R. Data collection, analysis, and interpretation: Dr Tarumi, Dr Zhang R, Dr Thomas, Ms Wang, Dr Zhang L, Dr Liu, Mr Turner, Mr Riley, Ms Tangella, Dr Womack, Dr Kerwin, Dr Cullum, Dr Lu, Dr Vongpatanasin, and Dr Zhu. Drafting and revising the manuscript: Dr Tarumi, Dr Zhang R, Dr Thomas, Dr Liu, Mr Riley, Dr Womack, Dr Kerwin, Dr Cullum, Dr Lu, Dr Vongpatanasin, and Dr Zhu.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.