
Abstract
Acute ischemic stroke represents a major cause of long-term adult disability. Accurate prognostication of post-stroke functional outcomes is invaluable in guiding patient care, targeting early rehabilitation efforts, selecting patients for clinical research, and conveying realistic expectations to families. The involvement of specific brain regions by acute ischemia can alter post-stroke recovery potential. Understanding the influences of infarct topography on neurologic outcomes holds significant promise in prognosis of functional recovery. In this review, we discuss the recent evidence of the contribution of infarct location to patient management decisions and functional outcomes after acute ischemic stroke.
Introduction
Acute ischemic stroke (AIS) is a significant cause of long-term disability. Two out of three AIS survivors will have residual neurologic deficits and up to half will require assistance with activities of daily living.1,2 Understanding the variables influencing AIS outcomes, therefore, has widespread clinical utility. Effective tools for the prediction of recovery after AIS can potentially guide patient selection for individualized therapies, end-of-life care, and early rehabilitation strategies.3,4 Moreover, accurate prognostic information offers value in clinical trial design because of the potential to enhance patient selection, reduce sample size, and improve the choice of clinical end points.5–7 However, the precise contributions of individual patient traits to post-stroke recovery are not well known, and improving our understanding of these influential factors on functional outcomes offers great clinical opportunity.
Infarct volume, as assessed on either CT or MRI, has been demonstrated to only moderately correlate with clinical outcomes.8–10 Analyses of multiple large data sets, however, have shown that age and stroke severity, measured by the National Institutes of Health Stroke Scale (NIHSS) score, have significant impact on post-stroke outcomes. 11 The inclusion of age and NIHSS, and other clinical variables, into models that also incorporate infarct volume improves the prediction of the likelihood of survival or functional recovery after AIS.12–14 More recently, an additional radiographic feature, namely the infarct location, has shown enhanced capabilities, compared to infarct volume alone, in predicting stroke and rehabilitation outcomes. 15 The importance of ischemic stroke location for functional outcomes has also been reported in delayed cerebral infarction after subarachnoid hemorrhage 16 and strokes involving specifically the cerebellum.17,18 Because of these complexities, long-term functional outcome of patients remains the primary end point in the majority of stroke trials and is the accepted outcome measure by regulatory agencies in trials of new drugs.
In this review, we will first discuss the more common scales employed in evaluating ischemic stroke outcomes. It is important to understand the advantages and disadvantages of instruments for evaluating stroke severity, post-stroke disability and recovery before exploring how infarct topography influences stroke recovery as assessed by these scales. We will then examine the role of stroke laterality on global outcome measures and proceed to investigate the effects of lesion topography on acute patient management and functional outcomes, such as motor, language and cognition. Finally, research on the role of acute infarct topography on acute treatment decisions and outcomes will be summarized.
Outcome measurement in stroke
Understanding the strengths and weaknesses of the commonly used stroke scales is critical for evaluating the individual impact of acute ischemic stroke injury on stroke recovery and functional outcomes as well as clinicians’ interpretation of stroke research findings.
19
The use of composite clinical rating scales, such as the NIHSS, has prompted many to stress the importance of using modality-specific outcome measures as primary end points in clinical trials of stroke.
20
This issue is of special importance in understanding the role of infarct location in functional outcomes. In short, the region of brain injury will manifest specific clinical symptoms that, depending on the outcomes scale, will exert different contributions to the score. For example, small ischemic strokes positioned in eloquent areas such as the corticospinal tracts or brainstem can induce severe deficits comparable to those attributed to large hemispheric strokes (Figure 1).
Stroke severity is dependent on location of ischemic stroke. DWI images of two patients admitted with AIS with identical admission NIHSS but different functional outcomes. (a) 56-year-old male found unresponsive. Neurologic exam notable for fixed pupils, present corneal and gag reflexes, absent oculocephalic reflexes, and flaccid paralysis of all extremities. MRI brain showed restricted diffusion in the medial thalami bilaterally and dorsal midbrain. Magnetic resonance angiography (MRA) of the head and neck (not shown) showed occlusive thrombus at the top of the basilar artery extending into the P1 segments of the posterior cerebral arteries bilaterally. Admission NIHSS 24; 90-day mRS 6. (b) 48-year-old male with atrial fibrillation presented with left middle cerebral artery (MCA) syndrome. Neurologic exam notable for a global aphasia and weakness of his right face and arm. MRI of the brain showed restricted diffusion in the left frontal operculum and anterior temporal lobe. Admission NIHSS 24; 90 day mRS 1. Images are shown in radiographic orientation.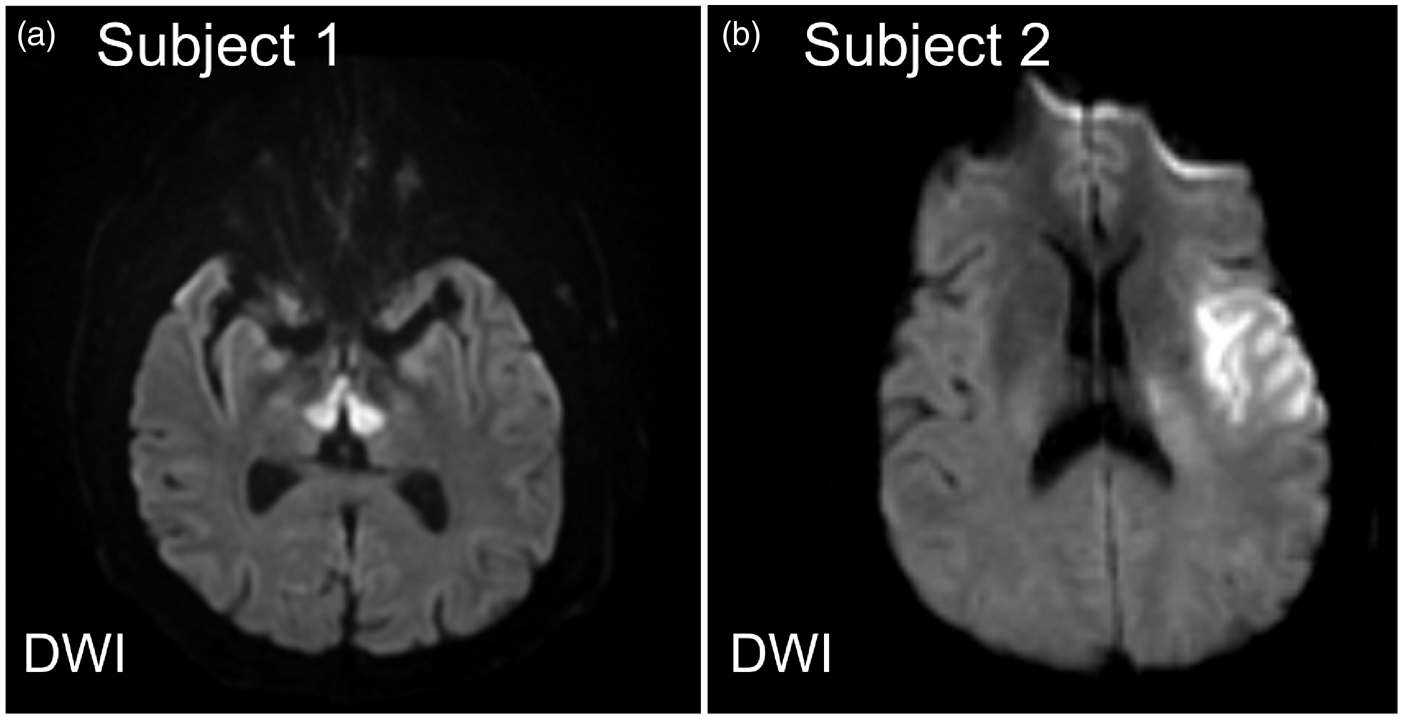
A number of different measures of stroke outcomes have been employed in clinical trials of ischemic stroke and post-stroke rehabilitation. These metrics each emphasize different aspects of stroke recovery and an understanding of the weights given to various factors of commonly utilized scales is important for interpreting stroke severity and functional recovery. In 2010, in an effort to standardize clinical research for stroke, the National Institutes of Neurological Disorders and Stroke (NINDS) set of Common Data Elements (CDE) was developed.21,22 These included frequently used scales to quantify neurologic outcomes such as the modified Rankin Scale (mRS), and NIHSS.19,23 The mRS is a global outcomes disability scale that has been widely employed in the evaluation of functional outcomes in clinical stroke trials.24,25 The mRS is an ordinal scale between 0 and 6 that assesses the degree of disability of an individual after stroke, with higher values representing greater morbidity (0 = no symptoms, 1 = some symptoms but can carry out all activities, 2 = slight disability but independent, 3 = moderate disability, requires assistance with affairs, 4 = unable to walk unassisted, 5 = bedridden, 6 = death). It is important to note that the mRS accentuates the level of functional independence and, as such, there is significant weight on motor performance (e.g. ambulatory status) as opposed to other areas of stroke recovery such as language. In fact, the mRS scale has been criticized as a disability assessment tool for being too dominated by motor recovery. 20
The NIHSS has been used for quantifying initial stroke severity and serial assessments as well as functional outcomes. The NIHSS is an ordinal scale (range 0 to 42) consisting of 11 items to measure degree of dysfunction across various domains including language, ataxia, motor strength, sensation, and neglect, where increasing values represent greater stroke severity. Multiple studies have exemplified that the NIHSS is a powerful, validated tool for assessing clinical stroke severity with high inter-rater reliability that correlates strongly with clinical outcomes.26–28 An important limitation of the NIHSS, however, is that the variables of its scoring system place greater emphasis on deficits associated with left-hemisphere function (e.g. language) rather than right hemisphere or posterior circulation (Figure 2).29,30 This observation is directly related to the inherent composition of the NIHSS: dominant (left) hemisphere dysfunction in the form of aphasia can influence multiple items as opposed to hemispatial neglect from non-dominant (right) hemisphere dysfunction being scored with only one question. Consistent with these points, analysis of hemispheric stroke patients has shown a lower NIHSS in right versus left hemisphere infarcts when controlled for stroke volume.
30
Overall, the NIHSS is a powerful tool for evaluating ischemic stroke; however, one of its limitations is the need for either an in person or video-conference examination.
The NIHSS emphasize dominant/left hemisphere functions. Representative MR images of two patients admitted with right and left hemisphere ischemic strokes. Each patient had the same admission NIHSS and 90-day mRS; however, the ischemic stroke volume was greater in the right hemisphere lesion. (a–d) 53-year-old man with atrial fibrillation and hypertension presents with left facial droop and arm weakness, dysarthria, and decreased sensation in his left arm. NIHSS 11 for right MCA syndrome including left hemineglect. MRI of the brain shows ischemic stroke involving the right insula, frontal operculum, and superior and middle temporal gyri on DWI sequences (a) without evidence of perfusion mismatch on Mean Transit Time (MTT) (b), time to maximum value of the deconvolved residue function (Tmax) (c), and cerebral blood flow (CBF) (d) maps. (e–h) 79-year-old male with coronary artery disease and hyperlipidemia that developed a non-fluent aphasia and right arm weakness. NIHSS 11 for left MCA syndrome involving language output and mild right face and arm weakness. MRI shows a subacute infarct involving the left inferior frontal gyrus on DWI sequences (e) with a matched focal perfusion abnormality on MTT (f), Tmax (g), and CBF (h) to suggest no additional territory at risk.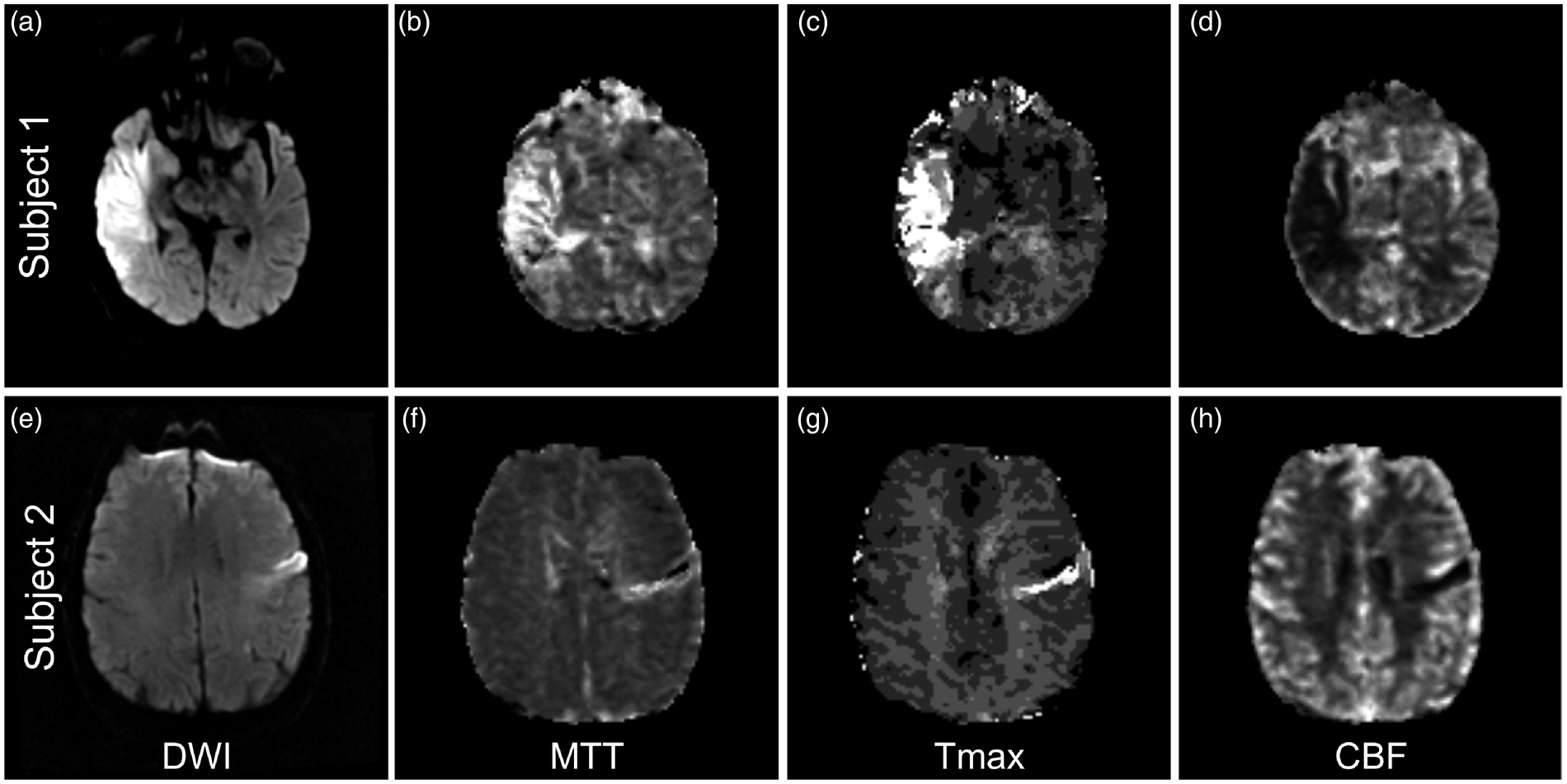
In addition to these assessments of global functional status, there is a number of modality-specific scales, for example looking specifically at motor function (e.g. Fugl-Meyer Assessment and Functional Independence Measure (FIM) motor subscale), used more frequently in the rehabilitation setting for gauging progress with physical therapy.31,32 FIM is a proprietary 18-item scale that requires assessment by speech, physical, and occupational therapists to assess cognitive and language domains. 33 Other NINDS CDE recommended outcome metrics measure emotional and cognitive status (e.g. Montreal Cognitive Assessment (MoCA), center for epidemiologic studies depression scale, trail making test parts A&B), self-reported quality of life (EuroQoL-5, PROMIS-10), and performance measures (walking speed). Each of these scales offers advantages and disadvantages in quantifying post-stroke disability and, as a result, emphasizes slightly different aspects of stroke recovery.
Effect of hemispheric involvement on functional outcomes
Ischemic strokes involving the dominant hemisphere, which in the majority of the population is the left hemisphere, versus the non-dominant or right hemisphere can cause distinctive clinical syndromes and deficits depending on the regions involved.
Studies of the effects of AIS hemispheric lateralization on outcomes have shown mixed results.34–42 A number of investigations have demonstrated that right hemispheric involvement portends worse functional outcomes in patients with AIS.34,37,38,43,44 When ambulatory status was assessed in 183 patients with small or medium-sized infarcts, right hemisphere AIS was associated with significantly worse locomotion: 64.9% of right hemisphere versus 82.1% of left hemisphere AIS patients were walking independently at the completion of rehabilitation. 36 On the other hand, there have been reports of hemispheric lateralization having no impact on functional outcomes.39–41 In a study of 70 patients with proximal large vessel occlusion (LVO) that underwent intra-arterial intervention, there was no difference in the rates of good outcomes (mRS≤ 2) at three months between right and left hemisphere AIS patients. 42 In an analysis of 1644 patients from the Virtual International Stroke Trials Archive, while baseline NIHSS was higher for left hemisphere strokes, hemispheric lateralization showed no influence on 90-day mRS and mortality, suggesting no relationship with AIS lateralization and functional outcomes. 35
The interpretation of these findings bears caution for two reasons. First, as mentioned earlier, the NIHSS is weighted for left hemisphere deficits and so it is not surprising that left hemispheric stroke patients might have higher baseline NIHSS scores. Secondly, the mRS as a marker of global functional status is largely predicated on ambulatory status and lacks sensitivity for deficits in other domains that certainly impact functional outcomes, such as language or neglect. Because of these inherent limitations of the mRS, alternative approaches to evaluating functional outcomes and the impact of AIS lateralization are necessary.
One approach to elucidate the contribution of infarct lateralization to post-stroke outcomes is to examine the relationship of the admission NIHSS with acute lesion volume and the affected hemisphere lateralization. As mentioned above, left hemisphere ischemic stroke patients will typically score higher on the NIHSS than patients with similar infarct volumes involving right hemisphere strokes. In an analysis of 153 patients with acute ischemic stroke, NIHSS scores of 0 to 5 points in right hemisphere strokes were associated with a two-fold increase in diffusion-weighted MRI (DWI) volume (DWIv; 8.8 vs. 3.2 cm3). 30 Furthermore another study of patients with similar NIHSS scores up to 20 points found that the median volume of infarct in the right hemisphere was approximately double than the left. 29 These findings emphasize the point that there is frequently a mismatch between the clinical presentation and the acute DWI volume depending on the afflicted hemisphere. Using clinical-DWI mismatch (CDM) defined as the NIHSS score exceeding 8 points when the DWIv is less than 25 cm3, the frequency of mismatch was higher in patients with left versus right hemispheric infarcts (65% vs. 38%, p = 0.001). This observation implies that small left hemispheric infarcts (DWIv< 25 cm3) are more likely to manifest with higher stroke severity (NIHSS> 8 points) as compared to an equivalent right hemisphere lesion. Interestingly, patients with CDM were more likely to experience early neurologic deterioration (defined as an increase in NIHSS of 4 or more points in first 72 hours of the admission) and infarct growth at 30 days. 45 As left hemisphere infarcts were more frequently associated with CDM, one could interpret these observations as if left hemisphere strokes could be more prone to infarct growth; however, there is a potential bias related to the infarct laterality and the NIHSS use that needs to be considered, given that worsening of clinical symptoms related to the dominant hemisphere is more likely to be detected.
Another interpretation of these findings is that CDM may be the result of a larger area of dysfunctional tissue extending beyond the infarct core visualized on acute DWI sequences. As discussed earlier, acute DWI volume has been shown to moderately correlate with functional outcomes and post-stroke disability.8–10,46,47 For this reason, using perfusion-weighted MRI (PWI) volume (PWIv) may hold value in accurately correlating stroke severity with final infarct volume and stroke outcomes (Figure 3). The initial PWIv has been demonstrated to be a strong predictor of final infarct volume
48
and clinical outcome.9,49,50 In support of this hypothesis, PWIv of non-dominant hemisphere and dominant hemisphere stroke patients correlated significantly better than NIHSS with tests of neglect performance and aphasia, respectively.
51
When PWIv was compared to DWIv in 40 subjects with acute hemisphere strokes, the performance on cognitive testing strongly correlated with the volume of hypoperfused tissue rather than DWIv.
52
These findings suggest that the regional location of hypoperfusion in AIS offers insight into understanding causes of stroke severity and could improve the neuroimaging prognostication of functional outcomes.
Does perfusion-weighted imaging provide a more accurate correlation with stroke severity? (a–d) DWI and PWI images for a 60-year-old male with hypertension that presented with a right MCA syndrome. NIHSS 14 for left facial droop and homonymous hemianopsia, weakness of the left arm and leg, dysarthria, and left hemineglect. MRI shows a small area of restricted diffusion in the right insula on DWI (a) with PWI evidence of mismatch and a potentially large territory at risk on MTT (b), Tmax (c), and CBF (d). (e–h) DWI and PWI images for a 18-year-old male that presented with sudden onset left sided hemiplegia. NIHSS 14 for right MCA syndrome including right gaze deviation and left hemineglect. MRI brain shows a large area of restricted diffusion in the right basal ganglia, frontal operculum, insula, and inferior parietal lobe on DWI (e), with PWI showing additional territory at risk on MTT (f), Tmax (g), and CBF (h).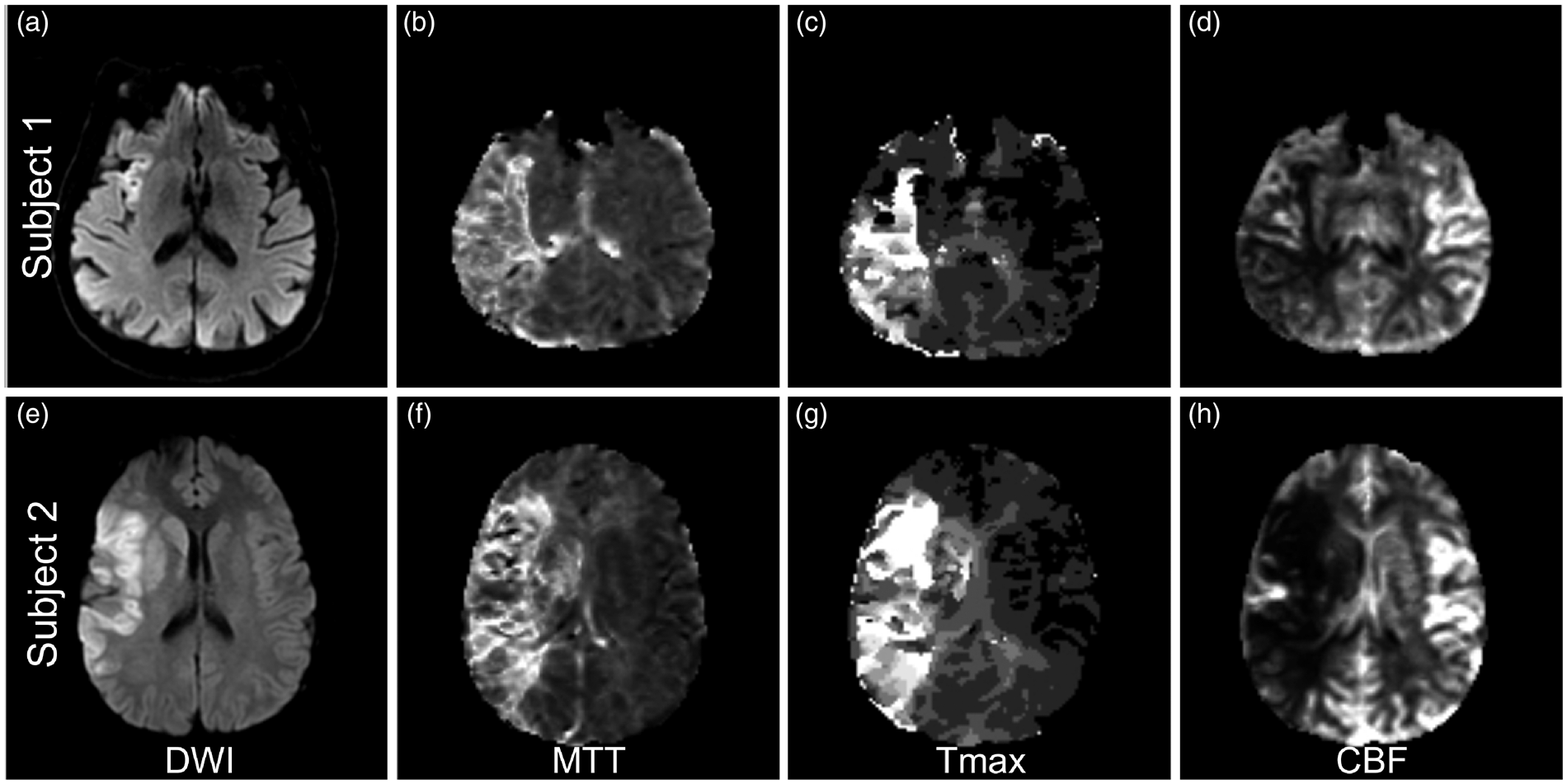
An alternative hypothesis for the possible discrepancy between right versus left hemisphere infarcts and stroke outcomes is delays in hospital presentation in non-dominant hemisphere strokes. 53 While language dysfunction from left hemisphere injury is more immediately apparent and easily recognized, the subtleties of hemispatial neglect with possible overlay of anosognosia may delay recognition of stroke onset. Further supporting this point, stroke severity, as assessed through scales such as the NIHSS, inversely correlates with time to hospital arrival and thus eligibility for intravenous thrombolysis.54–56 In addition, patients with severe neglect from a right hemisphere stroke or a fluent/receptive aphasia from a left hemisphere stroke may have difficulties participating in certain aspects of rehabilitation therapies, which will impact functional outcomes.
The hemisphere sustaining ischemic injury likely has multifactorial influences on post-stroke recovery through its affects on delay in hospital presentation and thrombolysis eligibility as well as impairing rehabilitation efforts. To further our understanding of the influence of acute stroke topography on functional recovery, we will discuss the role of injury to specific brain regions in various outcome domains.
Infarct topography and modality-specific recovery
The ability to accurately predict recovery of specific neurologic deficits following AIS is challenging but represents a critical question for guiding rehabilitation therapies and counseling the patient and/or family members. While there is evidence to suggest the extent and time course of recovery vary with severity of injury and the specific deficit,57–59 there is a growing body of evidence suggesting a role for infarct topography in modality-specific recovery. We will now review some of the key evidence on the role of infarct location in the recovery of several different neurologic deficits.
Motor recovery
The characterization of motor recovery in AIS is well studied, which is likely a reflection of the number of quantitative assessment tools for measuring motor performance. As a result, our understanding of the role of infarct topography in motor outcomes is more advanced than other areas of stroke recovery. The involvement of specific brain regions in AIS clearly and logically has a strong influence on motor recovery (Figure 1). Comparing cortical versus mixed or subcortical lesions, there is a strong correlation with upper limb motor recovery after AIS. In a study of stroke rehabilitation patients with pure cortical compared to subcortical strokes, 3 out of 4 patients in the cortical group versus 1 out of 17 in the subcortical group had recovery of upper limb motor function of it. 60 Importantly, only 1 of 28 patients with radiographic evidence of involvement of the posterior limb of the internal capsule had recovery of upper limb movement compared to 5 out of 13 patients with sparing of it. 60 One explanation for these findings is that the lesion load of the corticospinal tract portends motor recovery potential.61,62
In addition to injury of the corticospinal tract, infarction of specific regions of the cortex may also strongly influence motor recovery. Acute involvement of the somatosensory cortex, intraparietal sulcus, and primary motor cortex, evidenced by restricted diffusion on DWI, are associated with worse motor recovery and functional outcomes after AIS.63,64 Another study showed that CT perfusion within 9 h of stroke onset identified multiple brain regions including the insular cortex, superior temporal gyrus, postcentral gyrus, putamen, caudate, and internal capsule that were all independent predictors of motor recovery. 65 Involvement of the putamen has also been shown to increase the likelihood of a residual gait disorder following AIS. 66
Voxel-based lesion-symptom mapping (VLSM) approaches have also shown value in understanding the role of infarct topography on motor recovery. VLSM compares neurobehavioral scores between patients with and without lesions on a voxel-wise basis. 67 VLSM analysis showed that the areas most associated with worsening motor performance are situated at the junction of the corona radiata and corticospinal tract. 68 In a study of 50 patients with recent ischemic or hemorrhagic stroke, while corticospinal tract lesion load volume on FLAIR MRI sequences performed three to eight weeks post-event was predictive of performance in two functional mobility scales, using VLSM, walk speed response to gait rehabilitation was predicted by damage to the putamen, external capsule, and insula. 69
Not surprisingly, the extent of ischemic injury to the components of the motor pathway will affect motor recovery. These regions include the eloquent portions of the cortex involved in motor function as well as the corticospinal tract as it converges within the corona radiata and descends in the internal capsule. Using clinical variables alone to prognosticate motor recovery post-stroke is only moderately effective. 70 Incorporating region-specific or tract-specific involvement, however, is likely to improve predictions of motor recovery.
Recovery of language
In AIS, aphasia is frequently the result of ischemic injury to the language centers of the dominant hemisphere. Post-stroke aphasia is exceedingly common, as 20–40% of AIS patients will present with aphasia as an initial symptom.71–73 While the potential for motor recovery is heavily weighted by the extent of ischemic injury to the corticospinal tracts, the potential for recovery of language after AIS is dependent on the cortical involvement of the language centers. AIS infarct burden in language regions is an important predictor of aphasia recovery potential. 74
Multiple studies have highlighted the importance of the superior temporal gyrus (STG) and, in particular, the posterior portion, in aphasia recovery.75–78 In one study, the severity of auditory comprehension deficits was strongly correlated with the extent of injury to the posterior STG: patients with damage to less than half of the STG, detected on CT scans acquired six months post-stroke, were more likely to have good comprehension at six months. 78 Lesions of the dominant hemisphere STG also appear more likely to cause a persistent global aphasia as opposed to involvement of the inferior frontal gyrus or pre- and postcentral gyrus. 76 These studies suggest that the degree of sparing of the STG is critical for functional aphasia recovery. In addition, in a study of 97 patients with aphasia secondary to left hemisphere AIS, patients with exclusively subcortical involvement (e.g. basal ganglia) had less severe aphasias than those patients with cortical lesions involving Broca’s and Wernicke’s areas. 79
Perfusion imaging and, in particular, perfusion-diffusion mismatch (PDM) has also been shown to have prognostic utility in aphasia recovery. The presence of PDM in Brodmann area 37 (left posterior inferior temporal cortex) on MRI 24 h post-stroke, for example, independently predicted the degree of acute improvement in naming performance in a population of patients with acute left hemisphere ischemic strokes. 51 In another population of 58 patients with aphasia secondary to AIS, CT perfusion imaging within 9 h of symptom onset demonstrated near-normal to hyperemic relative cerebral blood flow values in the left angular gyrus and insular cortex were independent predictors of aphasia improvement by hospital discharge. 80 Moreover, when these variables were incorporated into a model also containing the admission NIHSS aphasia score and presence of a proximal cerebral artery occlusion, there was 91% accuracy in the prediction of aphasia outcomes. These findings would suggest that preserved or recovered perfusion in specific brain regions inform on the presence of salvageable tissue and as a result, could be useful in predicting functional aphasia recovery.
In summary, the potential for language recovery after AIS is influenced by the involvement of different cortical regions including the STG as well as potentially the angular gyrus and insular cortex of the dominant hemisphere. Incorporating the presence or absence of injury of these brain regions into prediction models with standard clinical variables could offer improved prognostication for post-stroke recovery of language deficits.
Cognitive outcomes
Following an ischemic stroke, 10% of patients will develop secondary dementia. 81 Understanding the factors that influence the development of post-stroke dementia is of major value in counseling patients and families on recovery expectations. The clinical determinants of post-stroke cognitive dysfunction seem to be heavily influenced by cortical injury or hemispheric involvement.82,83 In one study of 190 patients with first stroke, 74% of patients with cortical stroke compared to 46% of patients with subcortical stroke had evidence of cognitive impairment. 84 Another study of patients with AIS performed neuropsychiatric testing and observed that cognitive dysfunction was associated with the specific arterial territory involved and presence of white matter hyperintensity, but not the laterality of the ischemic stroke. 85
VLSM have also been used to identify region-specific predictors of cognitive outcomes. One group used VLSM analysis to identify eloquent voxels in patients with AIS using DWI obtained between 24 and 72 h after onset, which were found predominantly in the left hemisphere prefrontal, cingulate, peri-insular, middle, superior temporal cortex, amygdala, hippocampus, and deep nuclei. 86 Furthermore, they demonstrated that infarct location was the strongest predictor of good cognitive outcomes (MoCA> 25). 86
White matter tract integrity may also be informative in prognosticating cognitive outcomes after ischemic stroke. In a study of 14 right hemispheric stroke patients and 18 healthy controls, diffusion tensor imaging maps were compared between patients with good and poor cognitive recovery, where good recovery was defined as improvement in neuropsychological test results administered at three months post-stroke compared to results from 72 h. 87 The poor cognitive recovery group showed decreased contralesional axonal integrity at three months post-stroke in several left hemisphere regions when compared to healthy controls. 87 This data highlight the contributions of infarct topography as well as white matter tract integrity on post-stroke recovery of cognitive function. Moving forward, the use of standardized advanced imaging techniques to characterize infarct topography combined with outcome measures representative of the NINDS CDEs could improve the accuracy of prognostication.
To further understand the specific effects of infarct topography on post-stroke outcomes, it is important to consider the potential downstream effects of the infarct on brain functional network activity. A novel approach that has recently been used to explore these points is lesion-based functional connectivity network analysis. 88 By evaluating the blood-oxygen-level-dependent time course in regions of the brain exhibiting lesions in resting state functional MRI from healthy controls, common networks of brain regions were found to be involved in specific clinical syndromes such as peduncular hallucinosis, post-stroke pain and subcortical aphasias despite heterogeneous location of lesions. 88 The promise of this approach is that the inclusion of network analysis into infarct topography analysis could augment prediction models of more sophisticated outcome measures.
Acute tissue infarction location and prediction of long-term outcomes
In the acute setting, visualizing the infarct location intrinsically impacts the clinical decision-making process including the triage of the patient, the work up pursued for stroke mechanism, and additional therapies. Arguably more so than infarct volume, which is often dichotomized into large versus small, infarct topography influences patient management. For example ischemic strokes involving the posterior fossa will often require close monitoring for cerebral edema and potential prophylactic sub-occipital craniectomy. Alternatively, in strokes damaging the corticospinal tracts there is an expectation for significant hemiparesis and dysphagia that can influence enteral nutrition strategies and discharge destination.
The ability to accurately prognosticate clinical and ischemic tissue outcomes in the acute setting holds significant clinical implications for guiding acute management and accurately informing the patient/family to guide their decision-making. There have been several analytical and imaging approaches used to evaluate infarct topography with respect to AIS outcomes.
The current role of imaging in acute patient triage for clinical trials is predominantly volumetric, most likely due to ease of calculation. We will first discuss volumetric approaches before addressing the potential role of infarct location in patient selection for clinical trials. The current evidence on the effect of infarct volume and topography on functional outcomes following AIS has employed both CT- and MRI-based approaches. In clinical practice, CT-based imaging for AIS is much more widespread due to the speed of acquisition; however, MRI-based approaches afford a more sensitive and specific evaluation of acute ischemic brain parenchyma.89,90 The current data suggest that both approaches are informative in predicting outcomes.
Volumetric analyses
For intravenous (IV) recombinant tissue plasminogen activator (tPA) trials, acute lesion volumes on CT or MRI greater than 1/3 MCA territory are often used as exclusion criteria.91–96 Other MRI approaches proposed for trials investigating IV tPA in extended windows are PDM, LVO site and FLAIR-diffusion mismatches. 97 Additional details can be found in another review article. 97 Although studies have shown that CDM and PDM are closely related, 98 PDM was found to be more accurate for selecting patients likely to benefit from reperfusion therapy in the 3–6-h window, 99 with CDM patients showing no increased benefit from thrombolysis.99,100 Because of these findings and known limitations of the clinical score (i.e. NIHSS) from its weighting of left hemispheric infarcts and lesions involving the motor pathways as described above, selection of patients for extended time window treatment based on CDM, although easier to execute, is currently not clinically indicated. However, there is a clinical thrombectomy trial underway investigating the utility of CDM in patients with known MCA LVO. 101
In recent thrombectomy trials, infarct volume had a large effect on likelihood of good outcome (mRS< 3). In one study of 107 patients with anterior circulation LVO that underwent endovascular thrombectomy (EVT), follow-up infarct volume of 40 to 50 cm3 (at median time of 41.8 h from symptom onset and assessed with CT in 58.9% of the population) had the highest accuracy for predicting good outcome (sensitivity 74.1–81.5%; specificity 77.5–85.0%). 102 Aside from infarct volume, the early clinical response to EVT appears to be highly predictive of functional outcome. In one study, the authors looked at markers of early stroke severity, including infarct volume and baseline NIHSS, and showed that the trajectory of the two-day longitudinal NIHSS revealed subgroups of patients with large, minimal, and no improvement following EVT. 103 Not surprisingly, the subgroup with large improvement was more likely to have good outcomes at 90 days and had an accuracy of 84.5% in predicting 90-day mRS. 103 Infarct volume continued to have a role, as the “large improvement” subgroup was represented by younger patients with larger regions of hypodensity on acute CT. In a single center MRI study, 104 patients classified as likely to benefit from EVT (DWI volume< 70 cm3, age< 80 and pre-stroke mRS< 2), were also found to have more favorable outcomes after treatment. In this study, DWI lesion volume was estimated at the MRI console using measurements from three perpendicular axes and an assumed ellipsoid geometry (ABC/2). 105
In the EVT trials, ischemic core volume was one criteria; however, perfusion mismatch 106 and collateral status 107 were incorporated into the patient selection algorithm for several trials. In ESCAPE, delayed-phase CTA was employed to characterize collateral status and infarct core size as part of the trials inclusion criteria for potential EVT. 107 EXTEND-IA and SWIFT PRIME used CT perfusion (CTP) for CT sites or PDM for MRI sites for patient selection. CTP was used to determine the presence of a target mismatch profile by defining the ischemic core as tissue with relative CBF less than 30% of normal tissue and the “penumbra” as tissue with Tmax greater than 6 s. 106,108 The use of CTP to represent the ischemic core in these and other studies, however, is somewhat controversial as it is unclear whether reductions in relative perfusion metrics represent tissue infarction or mere hypoperfusion that can be reversed with revascularization. 109 Nonetheless, in patients with a target mismatch profile, reperfusion therapy was strongly associated with a favorable clinical response defined as NIHSS score of 0 to 1 or a ≥ 8-point improvement on NIHSS at 90 days.110,111 DEFUSE-3112 is an ongoing prospective randomized Phase III multicenter controlled trial addressing whether a target mismatch profile can be used to select patients likely to benefit from endovascular treatment in an extended time window.
Aside from using anterior circulation LVO as an inclusion criterion, infarct topography was not utilized in the decision process of patient eligibility for EVT trials. Instead patient selection was based on lesion volumes facilitated by the use by the use of either automated software 113 or visual assessment (ABC/2). 105 Future studies are needed to compare automated with manual approaches for patient selection for revascularization therapies.
Region-of-interest analyses
The Alberta Stroke Program Early CT Score (ASPECTS), 114 which was originally created to assess early acute ischemic injury and is incorporated into many decision models for pursuing endovascular therapy, is one approach that is used to link specific acute infarct locations to long-term stroke outcomes.115–117 Multiple studies have shown that integrating ASPECTS score into prediction models might be clinically useful. In one study, ASPECTS score was evaluated in data from the original NINDS tPA study and lesions involving the primary motor cortex/parietal lobe (M6) and lentiform nucleus increased the likelihood of disability (mRS> 2). 116 A simplified ASPECTS (sASPECTS) score, which scored only the caudate, lentiform nucleus, insula, and M5 region lesions, produced similar results to the ASPECTS score, and was found to be an independent predictor of three-month mRS> 2 in patients with anterior circulation AIS. 118
Although ASPECTS is traditionally performed on non-contrast CT scans, ASPECTS has also been applied to DWI. One study compared the performance of CT-ASPECTS and DWI-ASPECTS in a large EVT cohort. 119 In 74 patients, the inter-rater agreement for CT-ASPECTS and DWI-ASPECTS was 0.58 and 0.87, respectively. DWI-ASPECTS correlated with functional outcome while CT-ASPECTS did not. Both CT- and MRI-based ASPECTS, however, correlated with DWI volume but DWI-ASPECTS was superior. 119 In a cohort of patients with AIS treated with intravenous tPA that underwent CT and MRI in the hyperacute stage <3 h), the accuracy (with 1 being the highest accuracy) for CT-ASPECTS was 0.62 and DWI-ASPECTS 0.64 for predicting mRS < 3 at 90 days. 120 Comparing CT- to DWI-ASPECTS in AIS patients within 3 h of onset, the detection rate was significantly higher for DWI than CT (76.9% vs. 30.0%; p < 0.01). 121 These results suggest the sensitivity for detecting early ischemia is greater with MRI. However, this may be due to later acquisition of DWI than CT, since typically MRI is performed later than CT scans.
One group showed that in 213 patients with intracranial internal carotid artery, M1 or M2 middle cerebral artery occlusions who underwent EVT, on multivariable logistic regression, only M4 and M6 involvement on DWI ASPECTS, obtained < 72 h from symptom onset, were associated with poor outcomes (3 month mRS > 2). 117 Interestingly, in right hemispheric strokes, M6 involvement independently predicted poor outcome (odds ratio 5.8; 95% confidence interval 1.9–20.3), whereas in left hemispheric strokes, M4 involvement was a predictor of poor outcomes (odds ratio 4.3; 95% confidence interval 1.3–15.0). 117
The advantage of ASPECTS is that in trained professionals, it can quickly be calculated on CT or DWI performed in the acute stages and, appears to be associated with long-term functional outcomes. There are also efforts to automate ASPECTS calculation, 122 which will simplify the approach further. The ASPECTS score, either manual or automatically determined, has not yet been found to be able to select patients likely to benefit from endovascular therapy. 123 The role of ASPECTS in most current trials is predominantly to exclude patients who present with large strokes (e.g. ASPECTS < 7) as opposed to focusing on particular regions that are involved (e.g. lentiform nuclei).
Voxel-based analyses
Because of the poor sensitivity of CT in the hyperacute stage, voxel-based approaches using CT have been rarely used and therefore discussion will be limited to MRI. As mentioned earlier, acute infarct volume only correlates moderately with AIS outcomes.8–10 The integration of lesion location into models predicting functional outcomes after AIS offers promise for improving the accuracy of long-term prognostication models. An early example is a hazard atlas, which utilized discharge or chronic imaging lesion location combined with an “expert” atlas to predict NIHSS. 15 Another study used penalized logistic regression based on chronic imaging lesion location and extent to predict NIHSS. 124 These preliminary proof-of-concept studies linking lesion location with degree of disability has motivated the development of new techniques aimed at characterizing the specific role of acute infarct topography on global functional outcome metrics beyond laterality or specific functional domains.
VLSM has also been used to assess long-term global functional outcomes using acute imaging. In 101 patients with middle cerebral artery infarcts and two to three day DWI, greater disability as measured on the one-month mRS were associated with acute injury to the corona radiata, internal capsule, and insula, with asymmetric impact patterns found with respect to injury to the right angular gyrus and left superior temporal gyrus.
125
In this study, however, lesion volumes were not taken into consideration. Another study involving 490 AIS subjects who had DWI obtained within 48 h of last known well included lesion volume in VLSM analysis to investigate the role of acute lesion topography in AIS severity and long-term functional outcome.
126
Figure 4 shows the T-score results, on a voxel-by-voxel basis, of the effect of injury to each voxel on three to six month mRS. Adjusting for age and gender (Figure 4(b)), larger regions of tissue in the right hemisphere were implicated with worse mRS, while the opposite was true for the left hemisphere compared to unadjusted results (Figure 4(a)). When also adjusting for lesion volume (Figure 4(c)), injury to smaller regions within only the left hemisphere (e.g. corona radiata, internal capsule, postcentral gyrus, putamen, and operculum) was found to be independently associated with poor mRS. That is, patients with acute infarcts in these regions (independent of age, sex and lesion volume) were likely to have more disability at three to six months, as measured by mRS, than patients who did not have lesions affecting those regions. Similar results were observed when the analysis was limited to only patients who were still alive at six months post-stroke (Figure 4(d)). Moreover, the authors showed that left hemisphere injury, especially to the posterior limb of the internal capsule and white matter tracts was also associated with higher admission NIHSS.
126
VLSM has also been used to identify critical regions in functional outcomes after cerebellar ischemic strokes by examining injury at two weeks on 3D T1-weighted image
17
or within 72 h.
18
Both studies showed that in patients with impaired motor performance after cerebellar stroke lesions were more common in the paravermal lobules IV/V, deep cerebellar nuclei, and the middle cerebellar peduncle.17,18
Voxel-based lesion symptom mapping results for acute ischemic stroke functional outcomes (mRS). T-score maps with voxel-wise threshold of p < 0.001 and permutation method for follow-up mRS scores without covariates (a), using sex and age (b), or sex, age, and lesion volume as covariates (c). Subset analysis for patients alive at 6 months post AIS (d). A voxel with a high T-score (red) indicates that patients with lesions involving the individual voxel had worse mRS scores than patients who did not have a lesion at that voxel. Conversely, a voxel with a low T-score reflects no statistically significant difference (p > 0.001) in mRS scores between patients with and without a lesion at that voxel. From Ona Wu, Lisa Cloonan, Steven JT Mocking, Mark JRJ Bouts, William A Copen, Pedro T Cougo-Pinto, Kaitlin Fitzpatrick, Allison Kanakis, Pamela W Schaefer, Jonathan Rosand, Karen L Furie, Natalia S Rost. Role of acute lesion topography in initial ischemic stroke severity and long-term functional outcomes. Stroke 2015; 46: 2438–2444 and reproduced with permission from Wolters Kluwer Health.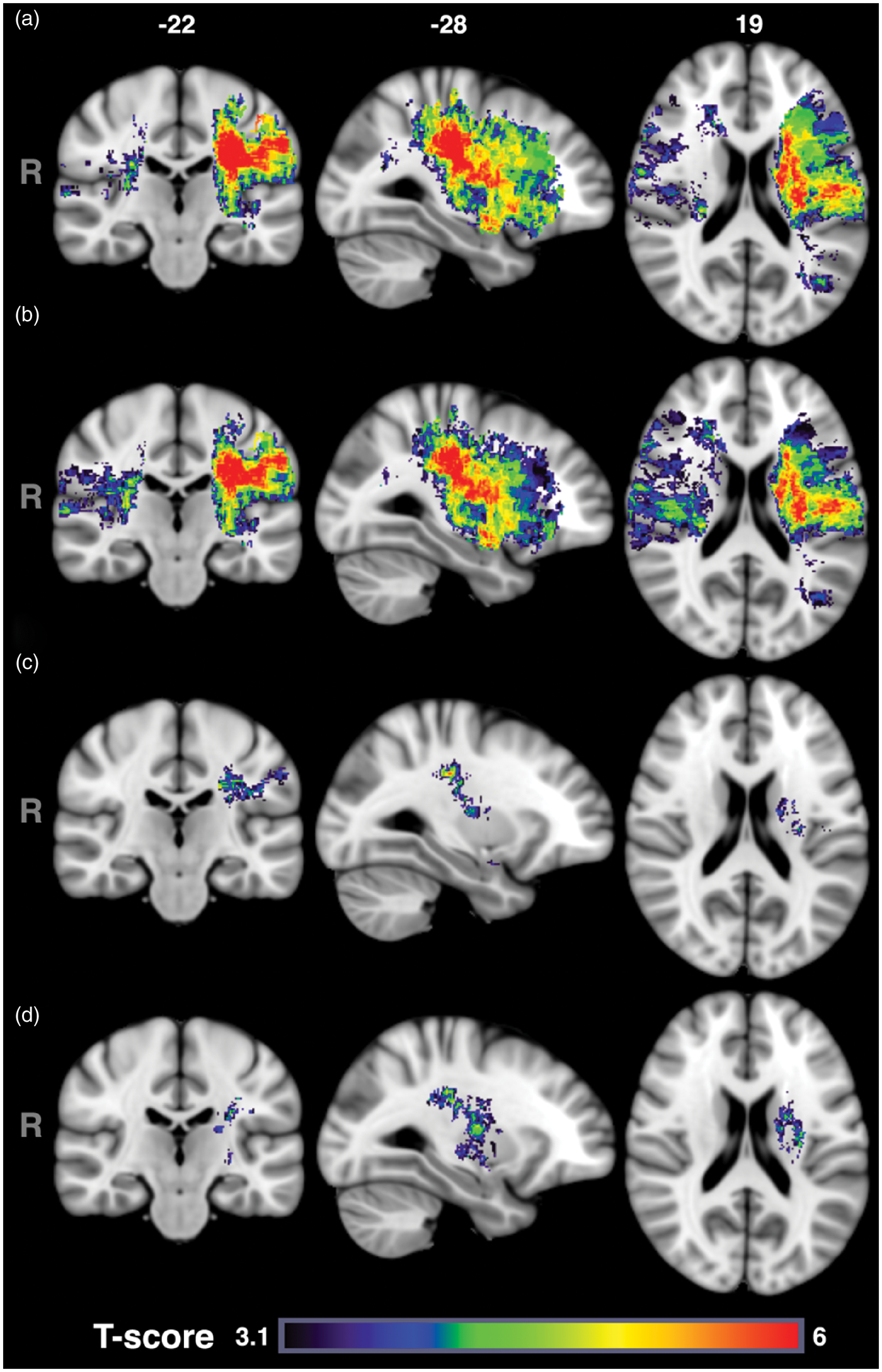
The use of the ASPECTS score and VLSM represents two approaches to incorporate acute lesion location into predictions of long-term outcomes at the acute stage. Early identification of patients at risk of poor recovery can potentially be used for selection of patients for clinical trials, aggressive intervention and focused post-stroke rehabilitation programs. Although ASPECTS on CT or MRI is becoming frequently used for selection of patients for thrombectomy in clinical trials, 101 anatomical territories identified by VLSM analyses as regions linked with poor long-term outcomes if infarcted are not currently being used. Indeed, these VLSM identified regions overlap the “clinically relevant penumbra” found by others to determine functional outcome after thrombolysis more so than volume of salvaged tissue.127,128 Future prospective studies are needed to validate both techniques for their utility in patient selection for revascularization therapy.
Conclusions and future directions
Understanding ischemic stroke functional topography holds major potential value in the acute management of patients with AIS as well as in targeting individualized early rehabilitation strategies. The outstanding questions are twofold: first, what is the additive value of considering infarct topography in the acute and chronic setting; and secondly, what neuroimaging approaches are most practical in the acute setting?
At present, the incorporation of infarct topography into hyperacute prognostication models holds significant promise of improving predictive accuracy of individualized recovery potential but with the current evidence, clinical implementation would be premature. Future studies evaluating the utility of infarct topography in patient selection trials are warranted.
The current data suggest that infarct topography has significant influence on post-stroke functional recovery and, as a result, including infarct location into post-stroke outcome prediction models holds major promise. In addition, for novel stroke trials targeting specific cognitive domains and brain regions,129,130 knowledge of the role of infarct topography on behavioral outcomes will be critical. Lesion topography has a role in improving our understanding of post-stroke disability and treatment planning for the rehabilitation setting.
Search strategy and selection criteria
We searched PubMed from January 2000 to October 2016, using the terms and synonyms “ischemic stroke,” “outcomes,” “topography,” “cognitive dysfunction,” “functional recovery,” “speech,” “aphasia,” “cognitive,” and “motor,” in combination with the key terms “infarct location” and “ischemic stroke”. We only searched for papers published in English. Of identified original research articles and relevant reviews, reference lists were also searched to identify additional relevant papers. Subsequently, we selected mainly original research articles or systematic reviews reported in core clinical journals during the past 16 years. Our final selection of references was made on basis of the relevance to the topics covered in this review.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health NINDS R01NS059775; R01NS082285; R01NS086905, P50-NS051343 and NIBIB P41EB015896.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ona Wu is the co-inventor of a patent on “Delay-compensated calculation of tissue blood flow,” US Patent 7,512,435. 31 March 2009, and the patent has been licensed to General Electric, Siemens, Imaging Biometrics and Olea Medical.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.