
Abstract
Cerebral aneurysms are weakened blood vessel dilatations that can result in spontaneous, devastating hemorrhage events. Aneurysm treatment aims to reduce hemorrhage events, and strategies for complex aneurysms often require surgical bypass or endovascular stenting for blood flow diversion. Interventions that divert blood flow from their normal circulation patterns have the potential to result in unintentional ischemia. Recent developments in computational modeling and in vivo assessment of hemodynamics for cerebral aneurysm treatment have entered into clinical practice. Herein, we review how these techniques are currently utilized to improve risk stratification and treatment planning.
Background
Cerebral aneurysms are focal dilations resulting from weaknesses in blood vessel walls. They are found in 3% of the general population and carry a risk of rupture and potentially devastating brain hemorrhage. 1 Treatment is ideally carried out before hemorrhage occurs and can be accomplished with microsurgical clip occlusion or with the endovascular coil embolization to exclude the aneurysm from the native circulation. For more complex aneurysms, such as those that incorporate large segments of multiple blood vessels, simple clipping or coiling of the aneurysm may not be feasible without sacrificing blood flow in parent and branch vessels. In these cases, advanced surgical bypass techniques or flow diverting endovascular stents are used to thrombose the aneurysm and preserve blood flow to the normal circulation. Preoperative knowledge regarding how these interventions alter local cerebral hemodynamics has been largely unknown, particularly with respect to preservation of small perforating arteries that supply critical structures (such as the brainstem). While once a strictly research interest, the ability to model cerebral blood flow based on 3D blood vessel morphology (computational fluid dynamics (CFD)) as well as to perform quantitative in vivo measurements via phase contrast magnetic resonance imaging (MRI) (4D Flow MRI) has become an important clinical tool to stratify procedural risk as it relates to perforating and branch artery preservation.2–9 Various treatment strategies can be compared in a simulation model to guide clinicians toward a strategy that ensures aneurysm obliteration and minimizes complications. For endovascular flow diverting treatments in particular, CFD modeling may be able to predict hemodynamic forces that could result in aneurysm hemorrhage following treatment. 10
Techniques
The process of modeling blood flow begins with defining the blood vessel lumen architecture, typically with the use of high-resolution, contrast-enhanced MR, CT, or 3D rotational angiography. 11 3D projections representing the luminal boundaries are then transferred into a modeling software environment, where the aneurysm is selected, along with its proximal and distal parent arteries. Small perforating arteries, if not visualized on the source imaging, can be virtually added based on typical anatomic patterns. These smaller branches of the basilar artery provide vital blood flow to the brainstem and their patency is often a major focus of predictive modeling. Their anatomical patterns are well known based on surgical and cadaveric studies, and major deviations seen on digital subtraction angiography can be accounted for on a case-by-case basis. In brief, addition of perforating arteries is accomplished in the preprocessing phase by creating a circular opening in the basilar wall and then creating a 3D spline representing the typical path for the vessel. Next, a surface of the vessel can be constructed by sweeping the opening circumference along the spline. Next, computational methods (numerical solutions of flow equations) are used to simulate blood flow patterns in the system as previously described, 3 assuming inlet flow and outlet flow are constant, in addition to other mathematical assumptions. Patient-specific blood flow velocities in the inflow vessels can be measured via phase contrast MRI and then used as references in these models. Ultimately, a multitude of alternative treatment options can be constructed and analyzed preoperatively. In the case of evaluating surgical strategies, virtual proximal occlusion and revascularization techniques can be introduced. When endovascular stenting is simulated, virtual stents with varying levels of porosity can be deployed. 12 Visualization of these treatment options using a “virtual contrast” technique can then assess changes in the streamline flow patterns through the aneurysm and surrounding vessels, intra-aneurysmal flow residence time, as well as changes in the intra-aneurysmal velocity and pressure.10,13 Various commercial CFD software programs such as Fluent and Ansys CFX (ANSYS, Inc., Canonsburg, PA, USA), ADINA (ADINA R&D, Inc., Watertown, MA, USA), COMSOL (COMSOL, Inc., Burlington, MA, USA), CFD-ACE (ESI Group, Paris, France), Flow-3D (Flow Science, Inc., Pasadena, CA, USA), and STAR-CD (CD-adapco, Melville, NY, USA), among others, are available for utilization.
In addition to CFD, quantitative in vivo blood flow measurements can be obtained via time-resolved phase contrast MRI (4D Flow).14,15 In a comparison with CFD models, there is relatively good qualitative agreement between the two techniques,16,17 but an important discrepancy can be seen in regions of relatively low intra-aneurysmal velocities. 3 This noise, likely an artifact of low/disturbed flow regions, supports the need for further investigation of 4D Flow in aneurysms of different morphologies and locations.
Clinical application
Cerebrovascular bypass
For aneurysms that are not amenable to direct surgical clipping, such as those with dolichoectatic or fusiform morphologies, cerebrovascular bypass techniques (revascularization surgery) have been developed to provide an alternative source of blood flow in the setting of planned segment occlusion of major intracranial vessel(s).18,19 In even more complex scenarios, surgical strategies aim at blood flow reduction to the aneurysm, rather than elimination, in order to keep vital perforating vessels patent while minimizing the hemodynamic forces that lead to aneurysm growth and rupture. Historically, selection of these various bypass techniques has been guided by anecdotal experience at highly specialized centers. Complications, including bypass graft occlusion, perforator vessel occlusion, and parent vessel occlusion, can occur despite sound surgical technique. This has driven the need to better understand the hemodynamic changes brought about by revascularization surgery and ultimately make informed choices about technique options based on this. Preoperative CFD modeling provides crucial data in these complex scenarios to expand upon the surgeons’ intuition and individually assess resultant blood flow patterns for the treatment options considered (Figure 1). Necessity is an important driver of innovation, and we have used predictive modeling primarily in some of the most challenging aneurysms we have encountered in clinical practice, as in cases of dolichoectatic basilar artery trunk aneurysms.
20
Computational fluid dynamic modeling of treatment options for dolichoectatic vertebral-basilar artery aneurysm. Left: Preoperative conditions. Middle: The basilar artery is clipped below the superior cerebellar arteries, nondominant vertebral artery is occluded, and bypass is performed from the dominant vertebral artery to the contralateral posterior cerebral artery. Right: Nondominant vertebral artery is occluded and bypass is performed from the dominant vertebral to the contralateral posterior cerebral artery. Only in the scenario on the right does blood fill the basilar trunk sufficiently to perfuse all of the perforating arteries to the brainstem. Occlusion of the nondominant vertebral artery and bypass graft limits the hemodynamic forces imparted on the aneurysm.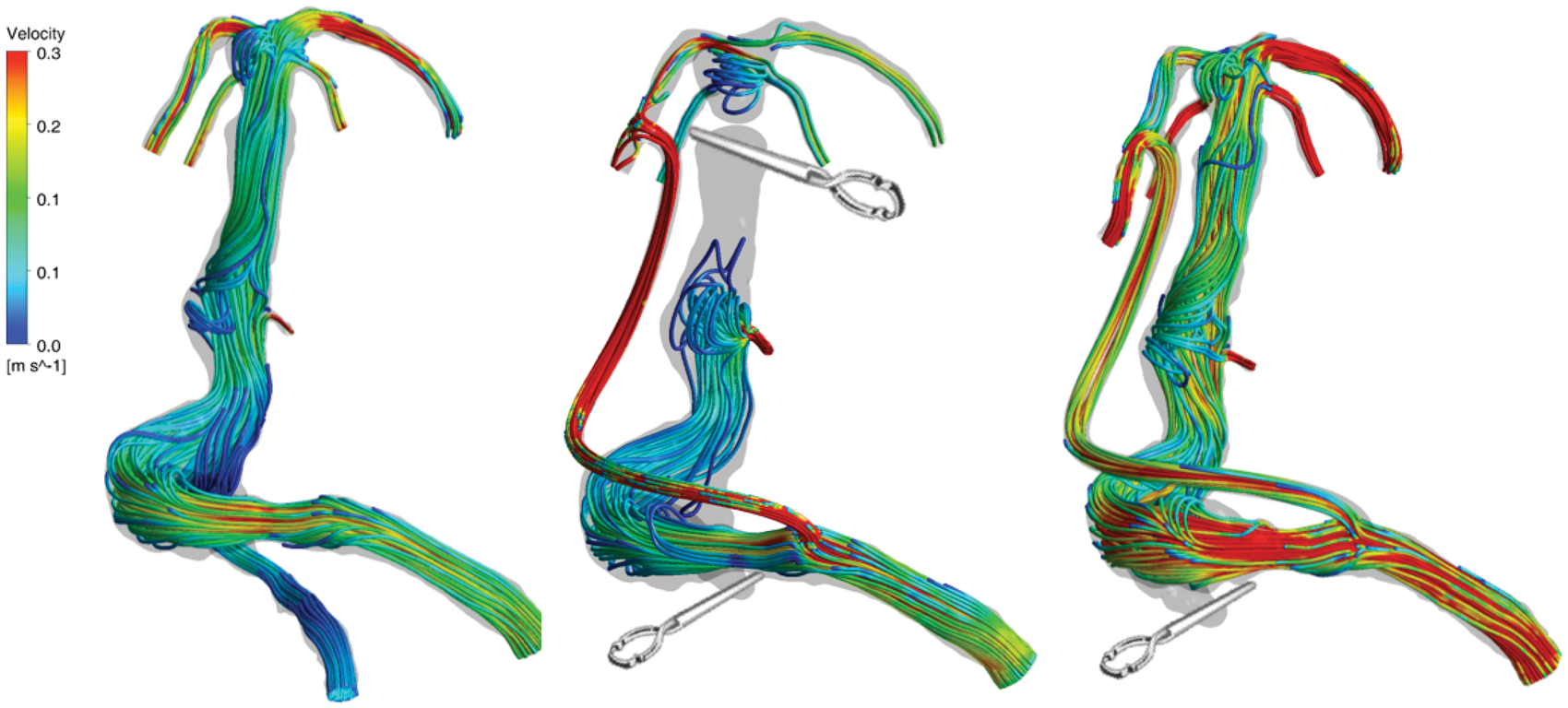
Endovascular flow diversion
Another treatment option for aneurysms that incorporate long segments of the parent artery is endovascular flow diversion. As opposed to other intravascular devices, such as cardiac stents that are placed to maintain the patency of blood vessels, flow diverting stents represent a method of treating cerebral aneurysms by redirecting blood flow away from the aneurysm into the parent vessel (Figure 2).21,22 Over time, because of the diverted blood flow, the aneurysm undergoes thrombosis and a new endothelium develops covering neck of the aneurysm, thereby reconstructing the native parent vessel. Since blood is diverted away from the aneurysm, it may also be diverted away from nearby perforator arteries, resulting in downstream ischemia.
23
Furthermore, a reduction in blood flow into the aneurysm does not necessarily equate to an immediate reduction in pressure experienced by the aneurysm wall,
24
and postprocedural hemorrhage is another known complication.
10
These potentially devastating adverse events have limited the widespread use of flow diversion as a treatment technique, and it is currently considered for only a subset of aneurysms of the proximal internal carotid artery that have been shown to be less prone to these complications.
25
CFD modeling has the potential to evaluate procedural risk, such as potential intra-aneurysmal pressure increases following stent deployment and risk of perforating artery occlusion for those branch arteries also covered by the stent.
26
Comparison of computational fluid dynamic and in vitro 4D Flow MRI modeling. A patient with a giant carotid artery aneurysm was evaluated prior to placement of a flow diverting stent. CFD modeling flow streamlines (top, left) matched closely with in vivo 4D Flow MRI measurements (bottom, left). CFD modeling (top, right) of stent placement also had close agreement with in vitro 4D Flow MRI models (bottom, right). MRI assessment after stent placement is not yet possible secondary to stent-related imaging artifact.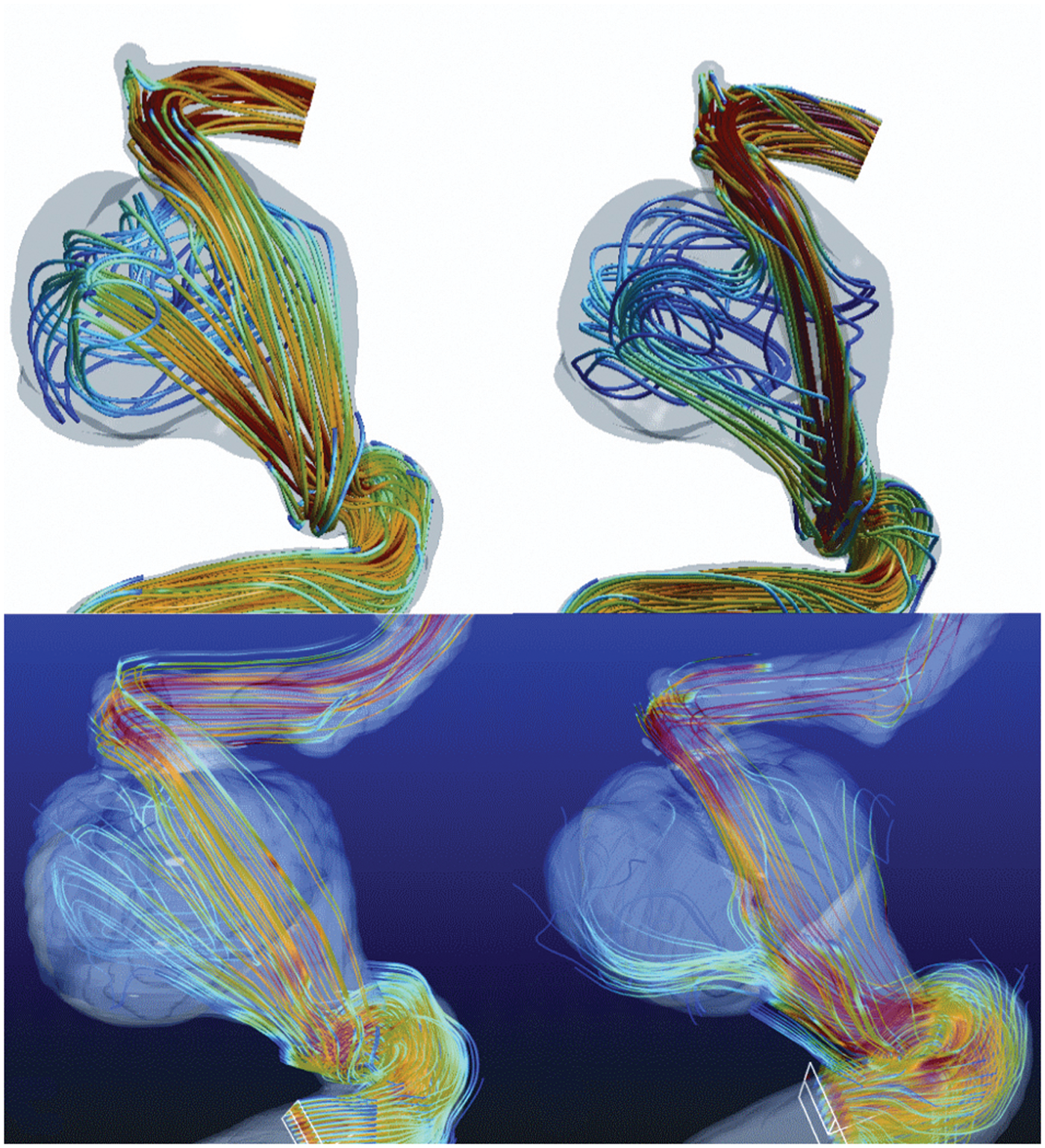
Future directions
Although still in the early stages of clinical application, blood flow modeling with CFD has been used to guide the treatment plans for many complex aneurysms.3,6 We continue to try to refine our surgical and endovascular treatment strategies for these lesions by ongoing comparison of predictive modeling and clinical outcomes. While treatment planning for every aneurysm is not practical or necessary, improved software workflow efficiency and close collaboration within a team of neurovascular clinicians and researchers allows for identification and preoperative study of many of the more complex clinical scenarios. Currently, the main utilization is to compare various surgical bypass options. Optimizing the predictive power of these models requires further study with endovascular quantitative flow assessment techniques and postoperative time-resolved angiography to provide further refinements and validation. 27 As CFD workflow routines become more streamlined and efficient, it is likely that other aneurysms, in addition to those not requiring bypass techniques, may also benefit from preoperative evaluation. Examples of this include preoperative models to reconstruct parent vessels with aneurysm clips prior to microsurgical clip occlusion and to determine flow alterations in branch arteries that originate from the aneurysm necks prior to flow diversion.
CFD modeling has also been instrumental in understanding the unexpected complication of hemorrhage following aneurysm treatment with flow diverting stents. While the mechanism is not yet fully elucidated, CFD suggests that failure to lower intra-aneurysmal pressure may be responsible for hemorrhage at a critical period after treatment when the aneurysm wall is weakened.10,28 It may be possible to predict those patients that would suffer posttreatment hemorrhage based on simulated pressure measurements. Other indications for flow diversion (off label), such as the vertebrobasilar circulation and distal anterior circulation are at the frontlines of investigation, particularly in the setting of next generation devices and a growing skillset.29–32 However, perforating artery patency (resulting in ischemic complications) remains one of the greatest concerns when placing a stent in these locations. Clinical and radiographic evaluation of named branch vessels in these locations, namely the ophthalmic artery,33,34 the anterior choroidal artery,35,36 and the posterior inferior cerebellar artery, 37 demonstrate that occlusion is rare and clinical sequelae from occlusion is exceedingly rare. Occlusion of these branch vessels can be explained by blood flow pressure gradients, which are largely influenced by collateral circulation patterns. Integration of these individualized collateral circulation patterns from the extracranial–intracranial circulation and across the Circle of Willis into predictive modeling calculations is an area of ongoing investigation.
Conclusions
CFD modeling is in clinical use to evaluate complex aneurysm treatment options preoperatively, predicting the effects of cerebrovascular bypass variations on aneurysm occlusion and perforator artery patency. Further applications in aneurysm treatment, including modeling of flow diverting stents and direct clip reconstruction strategies, may help to mitigate risk associated with these treatments.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received grant funding from the National Institutes of Health to MTL (grant # U54 NS065705), to DS (grant # RO1 HL114118), and to VR (grant #RO1 HL115267).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
All authors made a substantial contribution to the concept and design, acquisition of data or analysis and interpretation of data, drafted the article or revised it critically for important intellectual content, and approved the version to be published.