
Abstract
Background:
The last three months of life (end-of-life phase) are profoundly challenging for patients with brain tumours and their family caregivers. Post-bereavement outcomes are largely unknown.
Aim:
To better understand long-term outcomes of a brain tumour diagnosis on families, we aimed to describe caregiver experiences during the end-of-life phase and beyond.
Design:
In this sequential mixed-methods study designed together with bereaved caregivers, we used an online survey. This comprised end-of-life experiences, and post-bereavement outcomes (family functioning: Family APGAR; resilience: CD-RISC-10; mood: HADS; prolonged grief: PG-13-R; post-traumatic stress: TSQ).
Setting/Participants:
Caregivers of patients with brain tumours who were bereaved ⩾6 months ago were invited through social media and charities.
Results:
105 bereaved neuro-oncology caregivers participated. The end-of-life phase was marked by high symptom burden and disruption to family life, compounded by often unsatisfactory information provision and support. Forty-three percent did not describe the patient’s death as dignified. Most caregivers were not well-supported post-bereavement, and current functioning was impacted by notable rates of prolonged grief disorder (64%), post-traumatic stress disorder (42%), depression (35%), anxiety (61%), disruption to family life (53%) and low levels of resilience. Multivariable regressions found better resilience and family functioning to be protective factors for both post-traumatic stress disorder and prolonged grief disorder symptoms, with a dignified death additionally linked to caregivers’ prolonged grief scores, explaining 23.8% and 51.0% of variance, respectively.
Conclusions:
Bereaved neuro-oncology caregivers have high rates of adverse mental health outcomes, highlighting a pressing need for improvements in palliative, end-of-life and post-bereavement services.
Brain tumours diagnosed in adults can and often do lead to death;
Symptom burden is high throughout the disease trajectory and increases during the end-of-life phase, defined as the final 3 months.
Bereaved caregivers often report unsatisfactory information provision and support in the end-of-life phase;
Long-term adverse outcomes include high rates of prolonged grief disorder (64%), post-traumatic stress disorder (42%), depression (35%), anxiety (61%), disruption to family life (53%) and low levels of resilience;
Better resilience and family functioning are protective factors for post-traumatic stress disorder and prolonged grief disorder.
Patients with brain tumours and their caregivers both have profound palliative and end-of-life care needs which should be addressed;
Caregivers additionally require support into the post-bereavement phase to limit severe and long-lasting mental health and family life outcomes.
Introduction
Primary brain tumours can be classed as non-malignant or malignant, with a combined annual age-adjusted incidence rate of 24.25/100,000 (non-malignant 17.18/100,000; malignant: 7.06/100,000;). 1 Non-malignant brain tumours are typically less aggressive, however, depending on the location and treatment response, these can still result in significant disease burden2,3 and ultimately may lead to death. 4 Malignant, high-grade gliomas in particular are associated with a disproportionate share of cancer morbidity and mortality. 5 These aggressive tumours can rapidly progress to the end-of-life phase,5,6 defined as the last 3 months of life.7,8
During the trajectory, symptom burden which includes oncological and neurological issues tends to increase over time, impacting on both patients’ and their families’ quality-of-life.5,9 –11 Family caregivers consistently report high burden and unmet support needs,12,13 which can extend into the end-of-life and post-bereavement period.14 –17 The neurological deterioration makes the neuro-oncology end-of-life experience different to other cancers, 5 with a higher frequency of disease-specific symptoms shortly before death. 18 In the end-of-life phase, family caregivers can feel particularly unprepared and unsupported as patients experience, for example, loss of consciousness, difficulty swallowing, incontinence, seizures, progressive neurological and cognitive deficits, and headaches.14,18,19 Still, specialist palliative care remains underutilized with between 57% and 80% of brain tumour patients not receiving services.20,21 Indeed, among advanced cancer patients, those diagnosed with brain tumours are least likely to receive palliative care. 22 Following the patient’s death, transitioning from providing care to being bereaved can be difficult. 16 Whilst very little is known on post-bereavement outcomes of neuro-oncology caregivers, 23 a small-scale study noted high levels of distress. 15 From research performed predominantly in other populations, we know caregivers are at risk for long-lasting negative impact on physical health, finances, family dynamics and relationships.24 –28 In non-central nervous system cancer, better end-of-life experiences and quality of death have been linked to better caregiver quality-of-life post-bereavement. 29
Most published evidence is not specific to neuro-oncology, yet this population often has adverse outcomes compared to other oncological groups. We therefore aimed to describe the end-of-life experiences of brain tumour patients, as observed by their caregivers, and explore the longer-term impact on bereaved neuro-oncology caregivers. This work, co-designed and co-delivered by bereaved caregivers (PB and RM), will help highlight areas for improvement in palliative and end-of-life care, and post-bereavement support.
Methods
This report is part of a sequential mixed-methods study, comprising a quantitative survey followed by focus groups. Here, we report on the survey. The University of Leeds School of Medicine Research Ethics Committee provided approval (MREC 23-002).
Participants and procedures
Adult bereaved caregivers of brain tumour patients were invited to complete an online survey. Caregivers were eligible if they: had been bereaved for ⩾6 months; lived in the United Kingdom; had sufficient mastery of English to complete study procedures; had internet access and were able to provide consent. Caregivers were recruited from a closed Facebook group (‘Bereaved by a brain tumour’) which had ~1500 members and through charities’ (brainstrust and the Brain Tumour Charity) social media channels and/or newsletters. All participants confirmed consent and following survey completion, participants were offered a £10 voucher.
Outcome measures
Guided by caregiver representatives (PB and RM), outcome measures were selected which were deemed not too burdensome, taking ~60 min to complete. Self-reported basic sociodemographic and clinical information was collected alongside:
End-of-Life experiences: End-of-life Phase of Patients with a Malignant Brain Tumour Questionnaire. 30 This tool has adequate psychometric properties (content validity, internal consistency) and covers the last 3 months and last week of life. Questions focus on how caregivers thought the patient would have responded (38 items), and on caregivers’ own experiences during and following the end-of-life phase (21 items). Some items were modified to reflect the UK healthcare context.
Family functioning: Family APGAR.31,32 This 5-item scale with adequate psychometric properties 33 yields a total score ranging from 0 to 10 with higher scores indicating better family functionality. Cut-off scores can discriminate between severely (0–3 points) and moderately dysfunctional families (4–6 points) and functional families (7–10 points).
Resilience: Connor-Davidson Resilience Scale-10 (CD-RISC-10). 34 This scale has good psychometric properties (construct validity, internal consistency) and includes 10 statements describing aspects of resilience scored on a 5-point scale (0–4). The total score ranges from 0 to 40, with higher scores indicative of greater resilience.
Anxiety and depression: Hospital Anxiety and Depression Scale (HADS).35,36 HADS has adequate psychometric properties in caregiver studies (internal consistency).37,38 In 14 items, scored on a 4-point scale (0-3), anxiety and depression are assessed. Clinically relevant cut-off scores exist for mild (0–7), moderate (8–10) and severe (11-21) symptoms of anxiety or depression.
Prolonged grief: Prolonged Grief Disorder-Revised (PG-13-R). This 13-item measure has excellent psychometric properties (internal consistency, test-retest reliability, discriminatory ability) 39 and maps onto the DSM-5-TR diagnostic criteria for prolonged grief disorder. A summary score ⩾30 is used to indicate the need for further evaluation and treatment of prolonged grief disorder. 40
Posttraumatic stress: the Trauma Screening Questionnaire (TSQ). 41 The 10-item screening instrument is a valid tool with good sensitivity and specificity42,43 and consists of five re-experiencing and five arousal items from the DSM-5 criteria for post-traumatic stress disorder. The optimal cut-off score for high risk of post-traumatic stress disorder is ⩾6.
Life events: the Life Events Checklist for DSM-5 (LEC5-standard). 44 This measure has good cross-cultural validity and reliability45,46 and covers 16 events known to be highly distressing and/or associated with post-traumatic stress disorder, plus one additional item assessing any other extraordinarily stressful event.
Data analysis
Data were analysed using SPSS v.28. The sample’s sociodemographic and clinical characteristics were analysed descriptively. Questionnaires were scored along the respective scoring manuals and/or established criteria for clinically relevant cut-off scores. Descriptive statistics were generated to describe the end-of-life experiences (i.e. symptoms, support, quality-of-care, quality-of-life, quality-of-death) and caregivers’ initial post-bereavement outcomes. Current caregiver functioning was described using the scale scores, total scores, and clinically relevant cut-offs of the APGAR (family functioning), CD-RISC-10 (resilience), HADS (anxiety, depression), PG-13 (prolonged grief) and TSQ (post-traumatic stress). Life events were described using the LEC-5, with responses dichotomized to indicate whether caregivers had experienced a highly distressing life event (happened to them, witnessed it, learned about it, part of their job: yes) or not (not sure, doesn’t apply, do not want to answer: no), with a total score calculated to reflect the number of life events experienced.
Univariable regression analyses were done to explore potential factors associated with poor caregiver outcomes. For high risk of post-traumatic stress disorder (TSQ ⩾ 6) we explored associations with time since bereavement (<2 years or ⩾2 years), patient survival time (<18 months or ⩾18 months), patient age at death (<50 years or ⩾50 years), relationship (partner or other), stressful life events (LEC-5 excluding the items linked to illness, severe human suffering and ‘other’ as these could directly capturing the experience of caring for a brain tumour patient), 47 resilience (CD-RISC-10 total score),48,49 family functioning (APGAR total score), 50 patient quality-of-life in the last 3 months (scale 1–7), 51 dignified death (yes/no), 48 quality of care in the last 3 months (scale 1–7) and last week of life (scale 1–7), 48 and whether caregivers reported having had sufficient support in the end-of-life phase (yes/no). 48 Secondly, we ran univariable models to explore associations with prolonged grief in the subset of caregivers who were >12 months post-bereavement aligning with DSM criteria (symptoms present for ⩾1 year 52 ): univariable regression analyses with time since bereavement (<4 years or ⩾4 years), patient survival time (<18 months or ⩾18 months), patient age at death (<50 years or ⩾50 years), relationship (partner or other), resilience (CD-RISC-10 total score), 53 family functioning (APGAR total score), 54 patient quality-of-life in the last 3 months (scale 1–7), 51 dignified death (yes/no), 55 quality-of-care in the last 3 months and last week of life (scale 1–7),55,56 and whether caregivers reported having had sufficient support in the end-of-life phase (yes/no). 57 Those variables associated with post-traumatic stress disorder and prolonged grief disorder at p < 0.20 were taken forward into multivariable logistic regression models, where a manual backward selection was used to find the model with best fit (fewest number of variables, most variance explained using Nagelkerke R2, examining model χ2, p-values and Hosmer and Lemeshow tests).
Results
In total, 105 bereaved caregivers completed the survey between March and June 2024, see Table 1 for sociodemographic information and Supplementary Table 1 for participants’ religious/spiritual beliefs. Over half of our sample (N = 54, 51.4%) had an annual household income below £30,000, which is below the average UK household (median £32,400). 58
Caregiver and patient sociodemographic and clinical details.

1 missing.
2 missing.
Indian n = 1.
White and Black African n = 2.
British n = 52; English n = 35; Irish n = 2; Scottish n = 8; Welsh n = 1; Other White background n = 4.
Other = Hemangiopericytoma; Malignant melanoma; Medulloblastoma; Pineoblastoma; Primary CNS Lymphoma; Brain metastases.
End-of-life experiences
Symptoms and family functioning
Patients’ end-of-life symptoms are displayed in Figure 1 and Supplementary Figure 1 shows the frequency of epileptic seizures. 11 Thirty-two caregivers (31.1%) reported other symptoms reported as free text responses most frequently sight problems (N = 6, 5.7%), confusion (N = 5, 4.8%) and behaviour changes (N = 5, 4.8%).
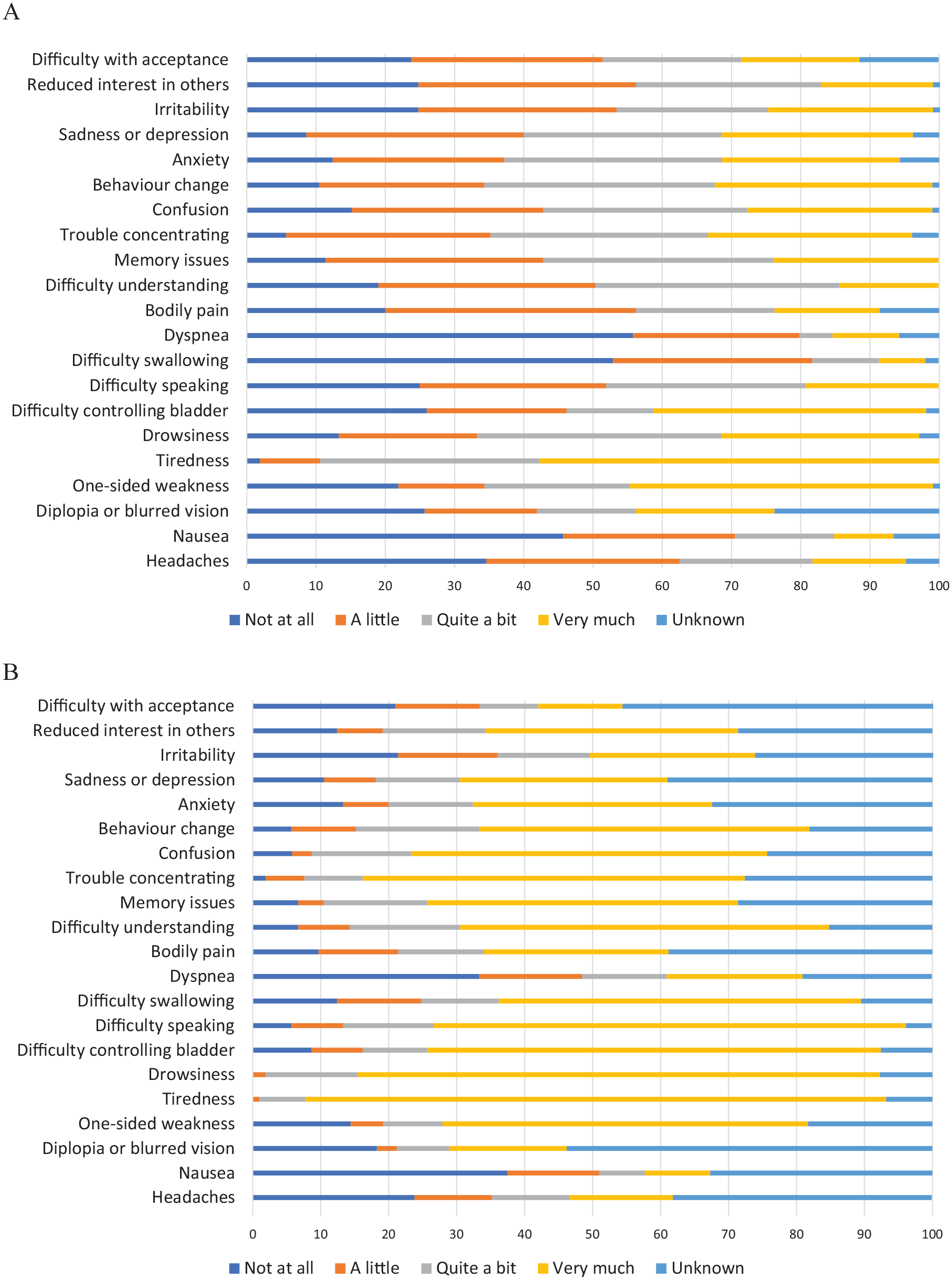
Symptoms in the last 3 months (panel A) and last week of life (panel B) as reported by the caregiver.
Social activities were nearly always impacted (quite a bit or very much: N = 93, 88.6% in the last 3 months; N = 84, 80.0% in the last week of life for patients; N = 102, 97.1% in the final 3 months for caregivers). Caregivers commonly reported severe (N = 81, 77.1%) or moderate (N = 16, 15.2%) disruption to family life. The relationship between caregiver and patient often became disrupted (N = 40, 38.1%) or more intense (N = 46, 43.8%). Caregivers’ work ability was often impacted (N = 77, 73.3%). Nearly half reported disease-related financial difficulties (a little to very much: N = 49, 46.7%).
Quality of care and quality-of-life
About half of caregivers found the quantity of information provided about the illness insufficient (N = 53, 50.5%). Caregivers often did not receive the professional support they needed in the last 3 months, with 46 receiving some, but not enough support (43.8%) and 18 receiving no support at all (17.1%). Supplementary Table 2 displays the healthcare workers encountered during the disease.
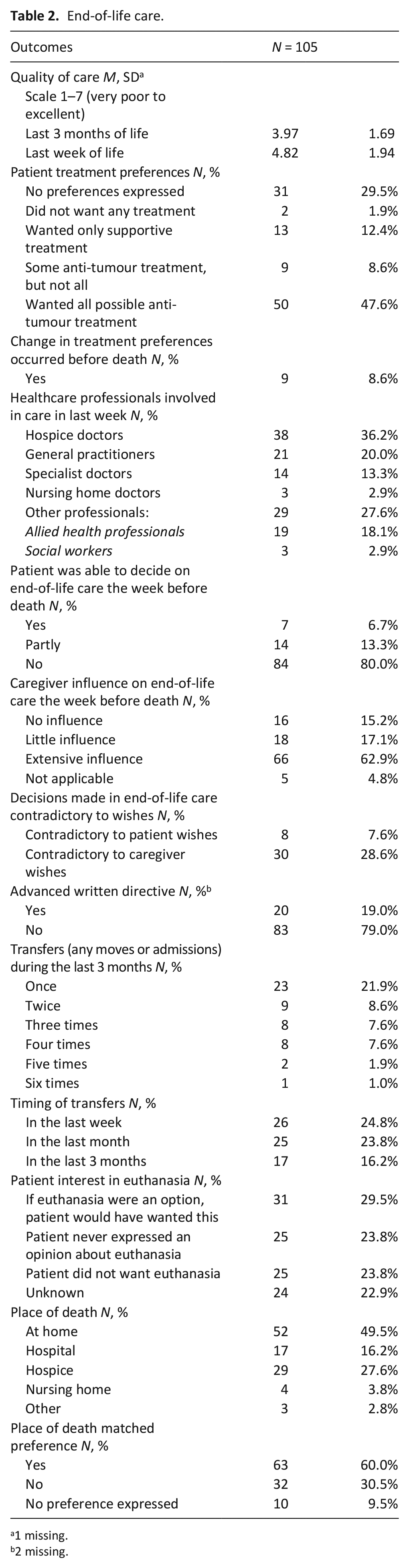
Quality of care in the last 3 months before death was rated average (M = 3.97, SD = 1.69, scale 1 to 7 (very poor-excellent). This was better during the last week of life (M = 4.82, SD = 1.94). In most cases, healthcare professionals involved in delivering care in the last week (see Table 2) explained end-of-life care options to either the patient (N = 6, 5.7%), the caregiver (N = 34, 32.4%), or both (N = 38, 36.2%). Most caregivers were satisfied with the contact with this professional (N = 60, 57.1%), their own role (N = 64, 61.0%) and with their involvement in decision-making (N = 67, 63.8%), although over a third felt insufficiently involved (N = 38, 36.2%). Healthcare professionals were not always accessible (sometimes accessible: N = 52, 49.5%; not accessible: N = 9, 8.5%). Over half of caregivers indicated that healthcare professionals should have played a larger role in patient care (N = 54, 51.4%).
End-of-life care.
1 missing.
2 missing.
Caregivers’ proxy ratings of patient quality-of-life in the last 3 months before death, was poor (M = 2.13, SD = 1.46, scale from 1 to 7 (very poor-excellent)). They rated their own quality-of-life in the end-of-life phase similarly poor (M = 2.40, SD = 1.42). Most patients were aware of their imminent death either fully, or more-or-less (N = 72, 68.6%). Advance directives were made by N = 20 (19.0%) patients, wills were prepared or discussed by N = 46 (43.8%).
Quality of death
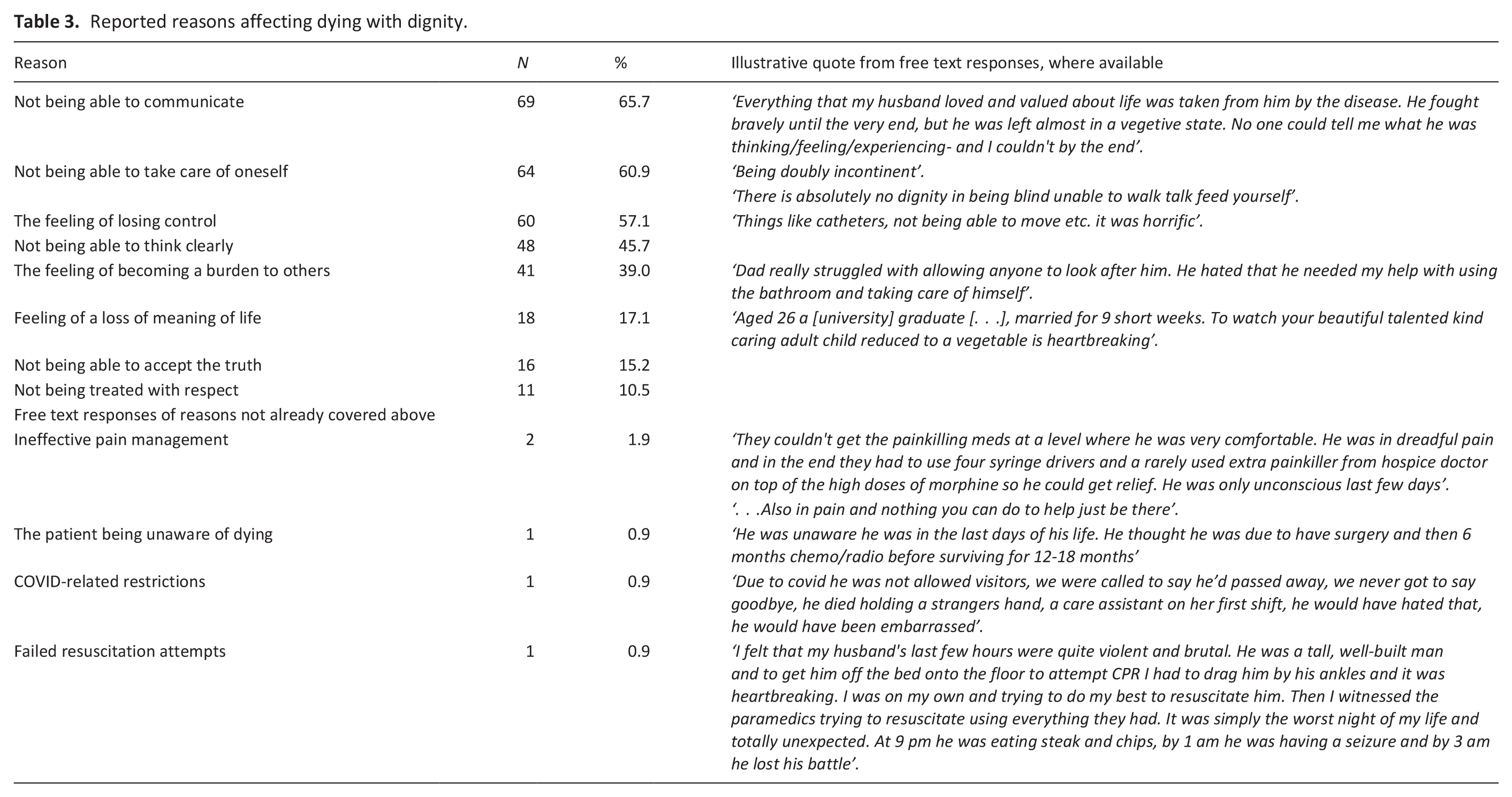
The death of the patient was described as dignified or very dignified by 60 caregivers (57.1%). However, 22 caregivers (20.9%) felt the death was neither dignified nor undignified, and 23 caregivers (21.9%) reported the death as undignified. Table 3 displays factors reported as influencing the dignity of death.
Reported reasons affecting dying with dignity.
Immediate post-bereavement outcomes and support needs
Approximately half (N = 53, 50.5%) of caregivers felt insufficiently supported by friends and family following the patient’s death. About a third of caregivers were in contact with the patient’s healthcare professionals following the patient’s death (N = 31, 29.5%), but only 14 (13.3%) had been offered the opportunity to discuss end-of-life care after death. Over half of caregivers expressed needing professional help after the patient’s death (N = 54, 51.4%), but only 11 received as much help as they needed (10.5%), with 30 receiving some help (28.6%), and 13 receiving no help (12.4%).
Current functioning of bereaved caregivers
Caregivers had been bereaved for a median of 1.5 to 2 years (range: 6 months to 10+ years) (see Table 1). Caregivers rated their current quality-of-life as average (M = 3.93, SD = 1.57). Over a third of caregivers had severe symptoms of depression (HADS-D > 8, N = 37, 35.2%), and nearly two-thirds had severe symptoms of anxiety (HADS-A > 8, N = 64, 61.0%), see Table 4. Over half currently experienced disruption to family functioning (APGAR moderate/severe dysfunction, N = 56 (53.3%)). In general, resilience was low with M = 21.98 (SD = 9.24) on CD-RISC-10 (norm population M ≈ 32). 34 The majority (N = 82, 78.1%) had resilience scores falling within the lowest quartile of population-based norms. 34 Nearly all caregivers experienced ⩾1 symptom of post-traumatic stress disorder in the past week (N = 92, 87.6%), and 44 caregivers (41.9%) were at high risk for post-traumatic stress disorder (TSQ ⩾ 6).
Long-term outcomes of bereaved caregivers.
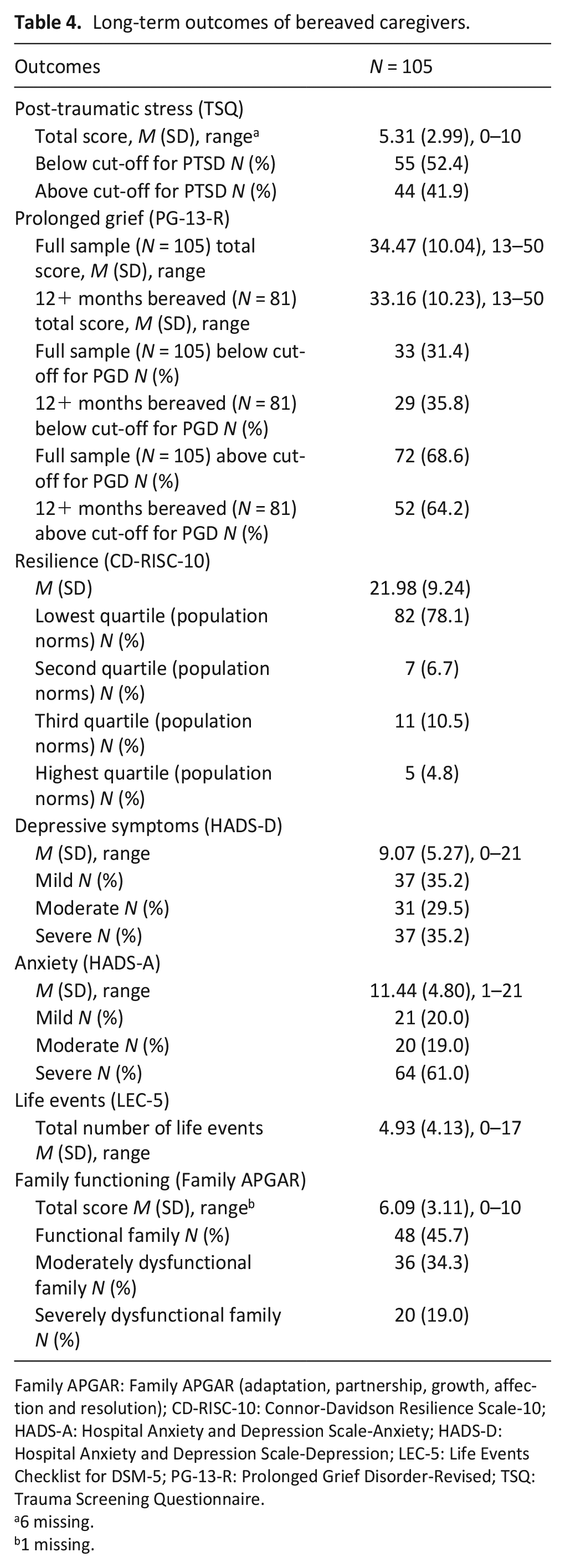
Family APGAR: Family APGAR (adaptation, partnership, growth, affection and resolution); CD-RISC-10: Connor-Davidson Resilience Scale-10; HADS-A: Hospital Anxiety and Depression Scale-Anxiety; HADS-D: Hospital Anxiety and Depression Scale-Depression; LEC-5: Life Events Checklist for DSM-5; PG-13-R: Prolonged Grief Disorder-Revised; TSQ: Trauma Screening Questionnaire.
6 missing.
1 missing.
Univariable logistic regressions to explore potential predictors of risk for developing post-traumatic stress disorder are shown in Supplementary Table 3. The multivariable model which included resilience and family functioning was statistically significant χ2(2) = 19.192 p < 0.001, and explained 23.8% of the variance in post-traumatic stress (Nagelkerke R2). Better resilience (CD-RISC-10 total score) and family functioning (APGAR total score) was associated with a reduction in the likelihood of caregivers displaying post-traumatic stress disorder (B = −0.078, p = 0.005, OR = 0.925, 95% CI = 0.876 to 0.977, family functioning (B = −0.163, p = 0.079, OR = 0.849, 95% CI = 0.728 to 0.991).
81 respondents were ⩾12 months post-bereavement, see Figure 2. Of those, 64.2% (N = 52) had scores indicative of prolonged grief disorder (PG-13-R ⩾ 30). Univariable logistic regressions to explore potential predictors for caregivers’ risk of developing prolonged grief disorder are shown in Supplementary Table 3. The multivariable model including resilience and dying with dignity was statistically significant χ2(2) = 37.298 p < 0.001, and explained 51.0% of the variance in prolonged grief disorder (Nagelkerke R2). Better resilience as measured with CD-RISC-10 (B = −0.193, p < 0.001, OR = 0.824, 95% CI = 0.748–0.908), better family functioning (B = −0.181, p = 0.089, OR = 0.835, 95% CI = 0.678–1.028) and the patient dying with dignity (B = −2.031, p = 0.025, OR = 0.131, 95% CI = 0.022–0.771) were associated with a reduction in the likelihood of caregivers exhibiting prolonged grief disorder.
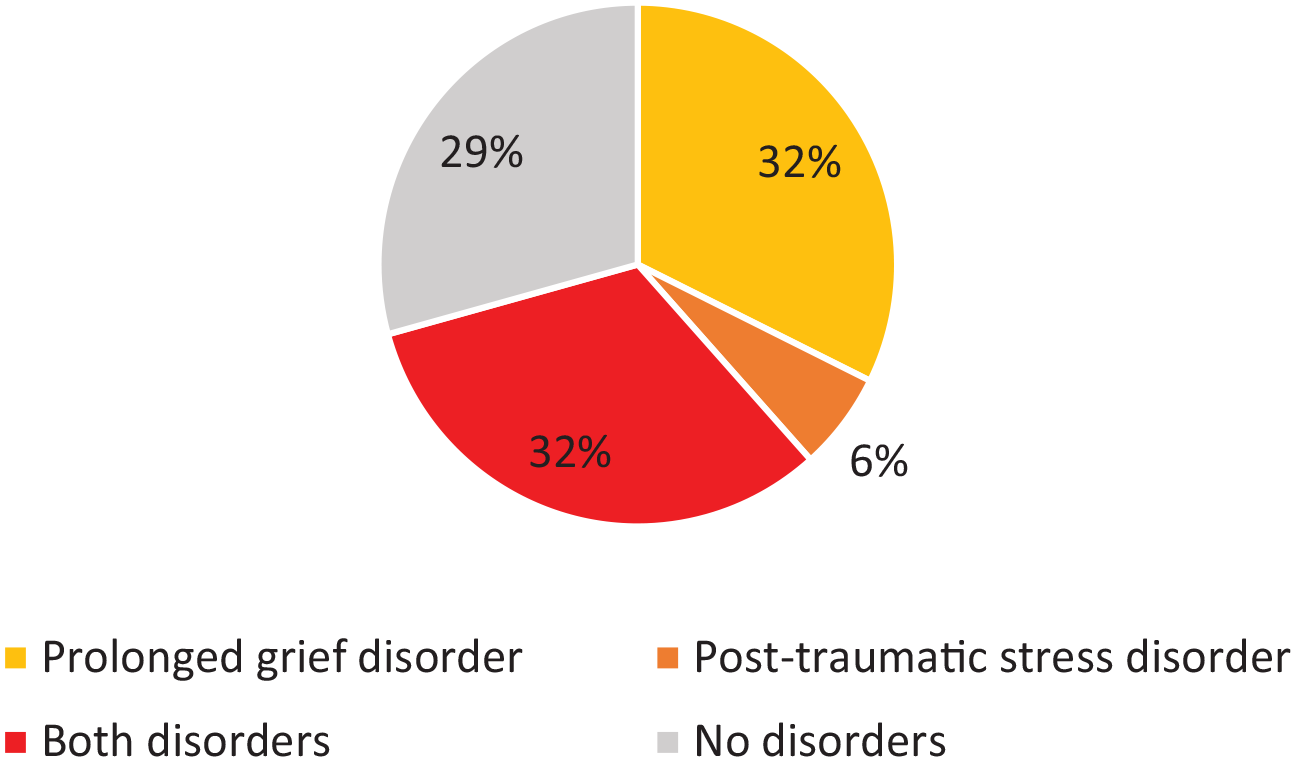
The proportion of caregivers, at least 12 months since bereavement, who scored above the cutoff for prolonged grief disorder and/or post-traumatic stress disorder.
Discussion
Key findings
Our study covers experiences and long-term outcomes of 105 bereaved neuro-oncology caregivers, yielding five key results. First, caregivers report high patient symptom burden and disruption to family life in the end-of-life, with room for improvement in terms of quality of care around information, support and accessibility of healthcare professionals. Second, a significant proportion of bereaved caregivers (~43%) did not describe the death of the patient as dignified. Third, over half of caregivers did not feel well-supported following the death of the patient. Fourth, caregivers’ current functioning post bereavement was suboptimal with notable rates of depression (35%), anxiety (61%), disruption to family life (53%) and low levels of resilience. Fifth, 42% scored above the threshold for high risk of post-traumatic stress disorder and 64% of those who were at least a year post-bereavement scored above the threshold for high risk of prolonged grief disorder, both mental disorders according to DSM-V.
Post-traumatic stress and prolonged grief disorders
The rates for high risk of post-traumatic stress disorder found in our investigation (42%) are higher than those observed in bereaved caregivers of other terminal cancer patients (30%) 59 or neuro-intensive care unit patients (22%). 60 We found greater resilience and better family functioning to be protective factors for post-traumatic stress disorder, explaining 23.8% of variance. This indicates other factors are involved. Other studies found negative affectivity, social support, locus of control in relation to the loss, 59 time spent at the bedside and lower household income 60 linked to post-traumatic stress disorder. Post-traumatic stress disorder is also directly associated with prolonged grief disorder. 61 In our sample, the rates of prolonged grief disorder were high at 64%, considering only 7% to 10% of adults typically develop prolonged grief issues. 62 Other studies using self-report measures show prevalence rates of 5% to 22%.60,63,64 Our findings contrast other evidence suggesting bereaved caregivers’ prolonged grief scores often return back to the levels of matched controls by 9 to 10 months follow-up. 65 In bereaved cancer caregivers, prolonged grief disorder can precede the development of major depressive disorder. 66 Indeed, 35% of our sample had scores indicative of high risk for depression. In our study, better caregiver resilience, family functioning and a dignified death were protective factors for prolonged grief disorder, explaining 51% of the variance, which is broadly in line with the literature. Other investigations additionally identified that pre-loss anticipatory grief, early prolonged grief symptoms, greater bereavement dependency, a spousal relationship to the patient, greater caregiver burden, poor family functioning, poor coping and low levels of optimism were risk factors for developing symptoms of prolonged grief disorder.54,64
It is striking, though perhaps unsurprising given the low rates of timely specialist palliative care involvement,20 –22 that our sample appears at higher risk for adverse outcomes post-bereavement than other caregiver populations. With its combination of neurological and oncological symptom burden, the often-rapid decline in patient functioning and high end-of-life symptom burden, the neuro-oncology caregiver experience can be described as combining the worst of cancer and dementia. 67 The focus groups performed in a nested sample of survey participants (manuscript in preparation) will shed further light on the potential reasons for adverse post-bereavement outcomes.
Guidelines exist for the management of post-traumatic stress disorder and prolonged grief disorder. For post-traumatic stress disorder, individual or group-based cognitive behavioural therapy with a trauma focus, and/or eye movement desensitization reprocessing is recommended by the World Health Organization and the National Institute for Health and Care Excellence.68,69 For post-traumatic stress disorder, pharmacological treatment is not advised.68,69 The National Institute for Health and Care Excellence does not have prolonged grief disorder guidelines and interestingly, the World Health Organization only recommends what not to do in people without prolonged grief disorder: interventions should not be offered routinely to all bereaved individuals. 68 However, benzodiazepines and grief counselling may be advised for those who do meet criteria for prolonged grief disorder as a mental disorder. With recent systematic reviews not identifying any trials of support interventions targeted at bereaved neuro-oncology caregivers,70 –73 there is a need for future work.
Strengths and limitations
This investigation was designed and delivered together with bereaved caregivers. There is some recruitment bias from the Facebook group, possibly overestimating the prevalence of issues. We attempted to counter this by also recruiting through charities. The sample is predominantly made up of white, female spousal caregivers, which, although common in neuro-oncology caregiver studies, is a limitation in terms of diversity. Given the variable time since bereavement, recall bias for the end-of-life experiences cannot be ruled out. The cross-sectional nature of the study did not enable us to explore the development of risk factors for mental disorders over time. Strengths include the relatively large sample, and detailed assessment of both end-of-life experiences and post-bereavement outcomes. The qualitative findings from our focus groups will provide further explanatory value in a separate article.
Conclusions
Our work highlights significant and enduring vulnerabilities in bereaved neuro-oncology caregivers. Timely intervention is needed to prevent long-lasting adverse impacts of brain tumours on families, extending beyond the disease trajectory.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251344164 – Supplemental material for End-of-life care experiences and long-term outcomes of bereaved neuro-oncology caregivers: A cross-sectional survey
Supplemental material, sj-docx-1-pmj-10.1177_02692163251344164 for End-of-life care experiences and long-term outcomes of bereaved neuro-oncology caregivers: A cross-sectional survey by Shaista Meer, Peter Buckle, Rosanna Miller, Louise Murray, Lucy Ziegler, Karin Piil and Florien Boele in Palliative Medicine
Footnotes
Acknowledgements
We would like to thank all participants for their time and effort. We also thank brainstrust and the Brain Tumour Charity for supporting recruitment.
Authorship
Conceptualization: PB, RM, LM, LZ, KP, FB
Methodology: PB, RM, LM, LZ, KP, FB
Investigation: SM, PB, RM, FB
Data curation: SM, PB, RM
Formal analysis: SM, FB
Writing (original draft): SM, FB
Writing (review & editing): SM, PB, RM, LM, LZ, KP, FB
Resources: FB
Data availability
The data that support the findings of this study are available from the corresponding author (FB), upon reasonable request and following appropriate agreements.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FB: speaker (Medscape, Medtalks, Servier); KP: consultancy (Servier), speaker (Medscape).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of Leeds Academic Development Grant and Yorkshire Cancer Research (L389FB).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.