
Abstract
Background:
Continuous subcutaneous infusion is a common and well-established method for administering medications in palliative care. However, limited evidence exists regarding the safety of subcutaneous plastic cannulas in patients with severe thrombocytopenia (platelet count ⩽20 G/L), a population at higher risk of bleeding complications. Understanding the safety profile in this context is essential for guiding clinical practice.
Aim:
To determine the complication rates associated with the use of subcutaneous polyurethane cannulas for continuous subcutaneous infusion in patients with severe thrombocytopenia in a German palliative care unit.
Design:
A retrospective observational study was conducted, analyzing all patients treated in a palliative care unit over 4 years. Data on the use of polyurethane cannulas, number of subcutaneous punctures, days of cannulas in situ, and associated complications were collected and reviewed.
Setting/participants:
The study was conducted in a single German palliative care unit. Of 1475 patients treated during the study period, 61 patients (4.1%) had severe thrombocytopenia (platelet count ⩽20 G/L). Of these, 17 patients received 37 subcutaneous punctures, accounting for a total of 150 days with polyurethane cannulas in situ.
Results:
No complications related to the use of polyurethane cannulas in patients with severe thrombocytopenia were observed in the studied population (n = 0, 0%).
Conclusions:
The findings suggest that the use of polyurethane cannulas is safe even in patients with severe thrombocytopenia. Further research could explore larger sample sizes and different settings to validate these findings.
Keywords
Introduction
Subcutaneous cannulas are a common method for continuous infusion therapy, especially in palliative care patients where the insertion of peripheral venous catheters can be challenging and burdensome. 1 However, uncertainty remains regarding the use of subcutaneous cannulas in patients with severe thrombocytopenia (⩽20 G/L). In the past, subcutaneous cannulas were sometimes avoided in this patient group due to the perceived high risk of bleeding, and alternative options such as port systems or peripheral venous catheters were recommended instead. Some authors have recommended to avoid subcutaneous cannulas in patients with platelet counts of 10 G/L or less. 2 However, the evidence supporting the risk of bleeding in continuous subcutaneous infusion is limited and largely based on general recommendations. We did not identify any studies specifically addressing this question.
On the other hand, the introduction of subcutaneously placed Teflon cannulas reduced the incidence of local reactions. 3 Moreover, these cannulas allowed longer durations of use.4,5 These findings suggest improved tissue compatibility, which may also lower the risk of bleeding complications. However, there is currently no strong evidence to support this hypothesis.
Therefore, the aim of our analysis was to estimate the incidence of bleeding complications associated with subcutaneous plastic cannulas in severely thrombocytopenic patients in a tertiary palliative care unit.
Methods
This retrospective descriptive study included all patients admitted to an adult palliative care unit of a university Hospital in Germany between January 1, 2020, and September 30, 2024, who had severe thrombocytopenia (platelet count ⩽20 G/L) upon admission. Data were extracted from the electronic medical records of the selected patients. The following variables were recorded: gender, age, primary diagnosis, the Australian-modified Karnofsky Performance Status on admission, platelet count, INR, PTT. From the patient charts, we identified whether subcutaneous cannulas were inserted, their location, and their duration of use. Additionally, other catheters (i.e. peripheral venous catheters, central venous catheter, peripherally inserted central catheter, or port) were documented. Specific search terms such as “blut” (blood), “häm” (hem), and “blau” (blue; German/Latin word stems connected to blood and bruises) were used to identify bleeding complications in the electronic patients records. These were categorized as follows: small hematoma (<5 cm), medium hematoma (5–10 cm), large hematoma (>10 cm), bleeding at the insertion site, or bleeding after catheter removal.
The collected data were entered into an Excel spreadsheet and subsequently analyzed using SPSS (version 29.0.0.0). The patient cohort, laboratory values, the number of subcutaneous punctures, and the duration of the polyurethane cannulas were analyzed descriptively. T-tests and Chi-square tests were used to calculate the statistical significance of differences in complication rates.
The local research ethics committee at the Medical Faculty of Ludwig-Maximilians-University approved the study (No. 24-0863).
Results
A total of 1475 patients were admitted to the palliative care unit during the specified period. Of these, 4.1% (n = 61) had a platelet count of 20 G/L or less on admission. The median age on admission was 66.5 years (range = 26–94 years) and 26/61 (42.6%) of the patients were female.
The most frequent diagnoses were acute myeloid leukemia (AML; n = 21, 34.3%), followed by prostate cancer (n = 5, 8.2%), multiple myeloma (n = 4, 6.6%), acute lymphoblastic leukemia (ALL), B-NHL, T-NHL, mantle cell lymphoma (MCL), myelodysplastic syndrome (MDS; each n = 3, 4.9%) liver cirrhosis and immune thrombocytopenia (ITP; each n = 2, 3.2%), and with other diagnoses accounting for the remaining 12 patients (19.7%, each n = 1: bronchial carcinoma, cancer of unknown primary, cholangiocellular carcinoma, diffuse large cell b cell lymphoma, endocarditis, diffuse large cell B-cell lymphoma, breast cancer, Hodgkins lymphoma, neuroendocrine carcinoma, ovarian carcinoma, sarcoma, sepsis, and small cell lung carcinoma). The median platelet count was 10 G/L (range = 0–20 G/L).
The subcutaneous cannulas used were Saf-T-Intima™ from Becton Dickinson (BD), with sizes of 20 or 22 G, and the cannula material was BD vialon™, a bio material based on polyurethane.
Of the 61 patients with severe thrombocytopenia, 17 (27.9%) received a subcutaneous cannula. Diagnoses in this subgroup were AML (8/17, 47.1%), each 2/17 (11.8%) with B-NHL and ITP, and each 1/17 (5.9%) with MDS, T-NHL, SCLC, sarcoma, and endocarditis. Their median platelet count was 12 G/L (range = 1–20 G/L). Table 1 shows a more detailed representation of the platelet count of both populations.
Overall number of patients with thrombocytopenia and subpopulation with subcutaneous needles grouped by platelet count.
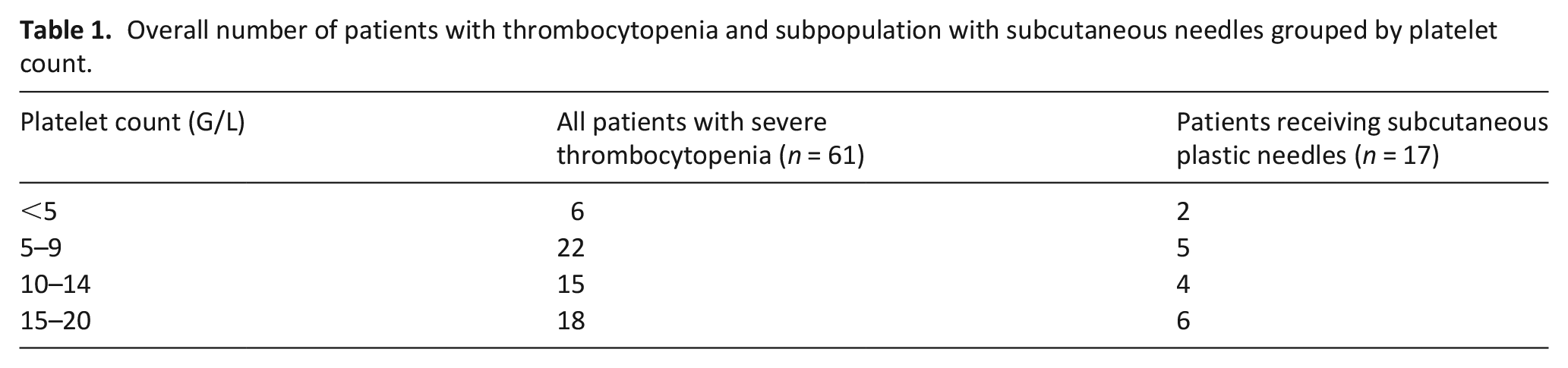
In these 17/61 patients a total of 37 punctures were performed for the placement of subcutaneous cannulas. 11/17 (64.7%) of the patients were punctured only once, 1/17 (5.9%) two times, 2/17 (11.8%) three times, and each 1/17 (5.9%) four, five, and nine times.
The cumulative duration of the subcutaneous cannulas was 150 days, with a median dwell time of 4.00 days (range = 1–8 days). The most common localization of cannula was abdomen (n = 14, 17.3%), followed by upper thigh (n = 8, 9.9%), scapula (n = 7, 8.6%), upper arm and unclear (each n = 4, 4.9%).
No bleeding complications were reported in relation to the insertion, dwell time, or retention of the subcutaneous cannulas during the observation period (n = 0). Therefore, a risk analysis was deemed unnecessary.
In addition to the subcutaneous cannulas, other vascular access devices were used for some patients (multiple per patient in some cases, totaling n = 61): 15 times for port systems, 29 times for peripheral venous catheters, 5 times for central venous catheters, 11 times for peripherally inserted central catheters, and once for an arterial catheter. These were usually started on previous wards and continued on the palliative care unit. One case of bleeding upon removal of a peripheral venous catheter that required pressure bandage was found.
Discussion
This retrospective study indicates that the use of subcutaneous plastic cannulas in patients with severe thrombocytopenia in palliative care is safe. These results are of high clinical relevance as they address existing concerns about the use of subcutaneous cannulas in this particularly vulnerable patient group. 2 Furthermore, this study is the first one to focus on that question. Previous studies have already shown a lower rate of local reactions with Teflon cannulas compared to metal needles 3 and demonstrated a potentially longer dwell time in polyurethane cannulas. 4 We suspect that earlier recommendations, which advised caution, were based on the use of metal needles, which are associated with greater trauma to the subcutaneous tissue. However, these needles are now rarely used. Additionally, in our studied patient population, a single instance of post-removal bleeding requiring intervention occurred after the removal of a peripheral venous catheter, while no bleeding complications were associated with the use of polyurethane cannulas. From our perspective, the current recommendations should be revised to indicate that, at least for plastic cannulas, their use can be recommended even for patients with severe thrombocytopenia.
A significant limitation of this study is its retrospective design and the relatively small sample size of punctured patients with severe thrombocytopenia. Furthermore, no comparison groups with different platelet counts were analyzed, which could limit the generalizability of the results. Additional observational studies are warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.