
Abstract
Background:
Continuous subcutaneous infusions combining several drugs are routinely used in palliative care, particularly for severe pain management. Parenteral administration routes, however, have been found to be prone to errors. According to previous studies, standardising the compositions of parenteral mixtures can improve medication safety.
Objectives:
To evaluate the potential for standardisation of parenteral drug mixtures used in palliative and hospice care by identifying the most commonly administered compositions of mixtures containing morphine or oxycodone.
Design:
A retrospective medical record review of parenteral drug mixture administrations containing morphine or oxycodone.
Methods:
Drug administration records of 120 deceased patients treated in two inpatient units and in the At-home hospital providing palliative and hospice care in the City of Helsinki, Finland, were collected. The data were analysed with descriptive statistics.
Results:
The patients (n = 120) received a total of 329 parenteral morphine or oxycodone containing drug mixtures administered as continuous subcutaneous infusions during a 10-month period from 28 April 2022 to 28 February 2023. Altogether, 29 different drug combinations were administered, of which the combinations of haloperidol and midazolam admixed with either morphine or oxycodone were the most prevalent ones (26.4% and 21.9% of all administrations, respectively). Of the 329 administrations, 175 different compositions were identified. In some of the mixtures, an increase in opioid quantity correlated with an increase in the other component quantities.
Conclusion:
Although palliative and hospice care patients need individualised medications, standardisation might be possible for the morphine-based drug mixtures and for the mixtures containing midazolam and haloperidol admixed with morphine or oxycodone.
Keywords
Introduction
With the ageing global population and the rising prevalence of cancers and other chronic diseases, the demand for palliative and hospice care is increasing.1,2 In palliative care, oral administration may not be possible for example, due to swallowing difficulties caused by neurological diseases or dysphagia during final days of life.3,4 Therefore, parenteral administration routes are favoured.5–7 However, parenteral administration poses unique challenges to medication safety, such as issues related to drug stability, 8 concentration accuracy, 9 and microbiological risks. 10
Continuous subcutaneous infusions combining several different drugs are widely used in palliative care, although the stability and compatibility of the mixtures are often not confirmed. 11 The mixtures typically contain drugs for managing symptoms such as pain, nausea, agitated delirium or dyspnea. Strong opioids relieving severe pain are frequently included components in these mixtures, to which other medicines, such as midazolam and haloperidol, are combined.5–7 In Finland, the most frequently used opioids are morphine (hydrochloride) and oxycodone (hydrochloride), 12 which are considered high-alert medications. 13 Thus, in addition to the potential incompatibilities that may lead to infusion complications, these drugs carry a significant risk of adverse events, such as oversedation and respiratory depression, if unintentionally overdosed.14,15
Delivering individualised medications to patients with severe symptoms in a rapid and flexible manner is crucial. Therefore, compounding is often carried out in clinical environments rather than in hospital pharmacies, despite the regulations set by the Finnish Medicines Agency. 16 However, compounding parenteral drug mixtures involves multiple, often complex steps. 9 Inconsistent approaches in compounding processes may, for instance, jeopardise aseptic techniques, which can promote infections. 10 Furthermore, prescribing and administration procedures for continuous subcutaneous infusions vary locally due to the lack of evidence-based guidelines. In practice, in care units without routine for parenteral drug delivery, the fear of errors may even lead to delays, or neglections in initiating the parenteral therapy.
To prevent adverse events caused by medication errors, the current trend is to develop prospective risk management at the organisational level. 17 Evidence-based systemic defences are intended to mitigate the risk of medication errors. 18 It has been shown that standardising the compositions of parenteral mixtures and centralising the compounding process effectively reduce medication errors, such as dose calculation and concentration accuracy errors.9,19,20 However, a review of the compositions of parenteral drug mixtures used in palliative and hospice care is required before deciding on standardised formulations.
The aim of this study was to evaluate the potential for standardisation of parenteral drug mixtures used in palliative and hospice care by identifying the most commonly administered compositions of mixtures containing morphine or oxycodone.
Methods
Study design and setting
In Finland, palliative care is recommended to be organised according to a three-tier model, consisting of specialised levels A, B and C, in addition to the basic level. 21 The basic level and level A units provide palliative care in all social and healthcare units treating patients at the end of life, such as community health centres, assisted living facilities and hospitals. Level B units are specialised in palliative care and include, for example, patient wards in community hospitals and at-home hospitals. Demanding special level C palliative care is provided by the palliative centres of university hospitals. This study was conducted in two palliative and hospice care inpatient units with bed capacities of 25 and 18, and additionally in the at-home hospital, which provides hospice care for 350–400 patients annually. All three units provide specialised level B palliative care in the City of Helsinki, Finland. Currently, these units compound all drug admixtures for their patients in the care units.
In this study, the retrospective data collected from medical records included 120 deceased patients who had received medical treatment in the aforementioned care units. This study focused solely on parenteral drug mixtures containing morphine or oxycodone, making these two drug substances, as well as the parenteral administration route, specific inclusion criteria for data extraction. An additional inclusion criterion was the time of death, which was 28 February 2023 or any earlier date until the full data set of 120 patients was extracted. Demographics such as age, gender, diagnosis, symptoms and duration of treatment were neither inclusion nor exclusion criteria.
This article follows the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement guidelines to ensure the transparency of the reporting. 22
Data extraction
The data were extracted from the EPIC-based electronic health record system Apotti. As the Act on the Secondary Use of Health and Social Data restricts researchers’ access to patient record systems, data extraction was performed by an external analytics specialist (Apotti Oy). The complete dataset consisted of specific elements extracted from the medical administration records, as outlined in Supplemental Appendix 1.
Data were collected in reverse chronological order based on the time of death, starting from 28 February 2023 and continuing backwards. The sample size of 120 deceased patients was based on an estimation that the patient population would rotate 1–2 times, which were predicted to reduce the potential risk of bias. Data on the composition and use of parenteral drug mixture administrations containing morphine or oxycodone were extracted (Supplemental Appendix 1). In addition, relevant patient demographics and the medication orders related to the administrations were included.
Data analysis
A biostatistician was consulted in the data analysis. The data were analysed using descriptive statistics with Microsoft Office Excel and IBM SPSS Statistics programs. Patient characteristics were analysed regarding age and ICD-10 diagnosis groups. 23 The prevalence of the various drug products (components) included in the administered drug mixtures, as well as their combinations, was identified to provide an overview of the sample. The infusion durations for the compounded mixtures were analysed by combining information from instructions in open fields of the medication orders and structured fields containing specific component quantities of the entire mixtures.
The most common compositions of parenteral morphine and oxycodone mixtures were identified by quantifying the number of parenteral mixtures with equal drug components and equal amounts of these components. To evaluate the potential for standardising some parenteral opioid mixtures, Spearman’s correlation coefficient was used to assess the correlation between the quantities of various drug components in the drug mixtures (e.g. whether an increase in opioid amount would correlate with an increase in the amounts of other drugs). This correlation was determined for the 10 most prevalent drug combinations. Statistically significant (p < 0.05) correlations were classified according to their strength.24,25 Additionally, drug combinations with the highest number of different compositions were identified to evaluate the variation in compositions and the potential for standardisation.
The data extraction process provided insufficient information on some mixtures administered as bolus and, therefore, bolus administrations were excluded from the study to reduce the risk of bias.
Results
The mean age of the patients (n = 120) was 79 years (range 54–103) and 90% (n = 108) were 65 years or older. The total number of ICD-10 classified diagnoses per patient varied from 0 to 28, Fifty-eight per cent (n = 70) of the patients were diagnosed with the ICD-10 code Z51.5 (palliative care), making it the most prevalent code among the patient population. Neoplasms, diseases of the circulatory, genitourinary, nervous, or digestive systems, and infections were diagnosed in 21%–63% (n = 25–76) of patients.
The study population received parenteral drug mixtures containing morphine or oxycodone during the period from 28 April 2022 to 28 February 2023. Most medication administrations occurred in January and February 2023, as the sample size of 120 deceased patients was reached and only 4 patients had received treatment according to the inclusion criteria before January 2023. The dataset comprised 329 administered drug mixtures containing morphine or oxycodone as the opioid component. One patient may have received several drug mixtures during their treatment. All mixtures were administered as continuous subcutaneous infusions. A majority of the mixtures (94.5%) were compounded to provide a continuous infusion over a period of 4 days. Other durations included 1 day (2.1%) and 5 days (0.3%), or the duration could not be determined (3%) due to inconsistencies between the instructions in the open and structured fields of the medication orders.
Morphine was administered more often than oxycodone, at higher concentrations and with a broader range of concentrations (Supplemental Appendix 2). The opioid was switched from oxycodone to morphine or vice versa for six patients during their treatment. Besides morphine and oxycodone, 10 distinct drugs were used as components in the drug mixtures in the study cohort. Midazolam and haloperidol were the most frequently used.
In total, 29 different drug combinations were administered to the patients (Figure 1). In addition to multi-drug combinations, one mixture contained only oxycodone diluted with sodium chloride 0.9%. The combination of morphine, haloperidol and midazolam, as well as the combination of oxycodone, haloperidol and midazolam were administered significantly more often than any other combination.

Drug combinations administered (N = 329) and their prevalence by combination (%) in the study cohort. Abbreviations “mo” and “oxy” refer to morphine and oxycodone, respectively.
Most of the mixtures comprised three drugs (58.1%), followed by four-drug (19.5%) and two-drug mixtures (16.1%). Sodium chloride 0.9% was the only diluent identified in the study cohort, used in 225 (68.4%) mixtures. The recorded total volumes of the mixtures ranged from 2.2 to 80 ml. A majority of the mixtures (55.9%) were 20 ml in volume. Volumes greater than 20 ml were recorded in 135 (41%) mixtures, and volumes below 20 ml in 10 (3%) mixtures. The use of a diluent was found to be associated with mixtures of 20 ml volume: of the 184 mixtures with a volume of 20 ml, 178 (96.7%) contained a diluent. In mixtures with volumes greater than 20 ml, a diluent was used in 47 mixtures (35.1%). No diluent was used in mixtures below 20 ml.
Of the 329 administered drug mixtures, 175 different compositions (differences in not only drug components but also in doses or volumes of mixtures with the same drug components) were identified (Figure 2).
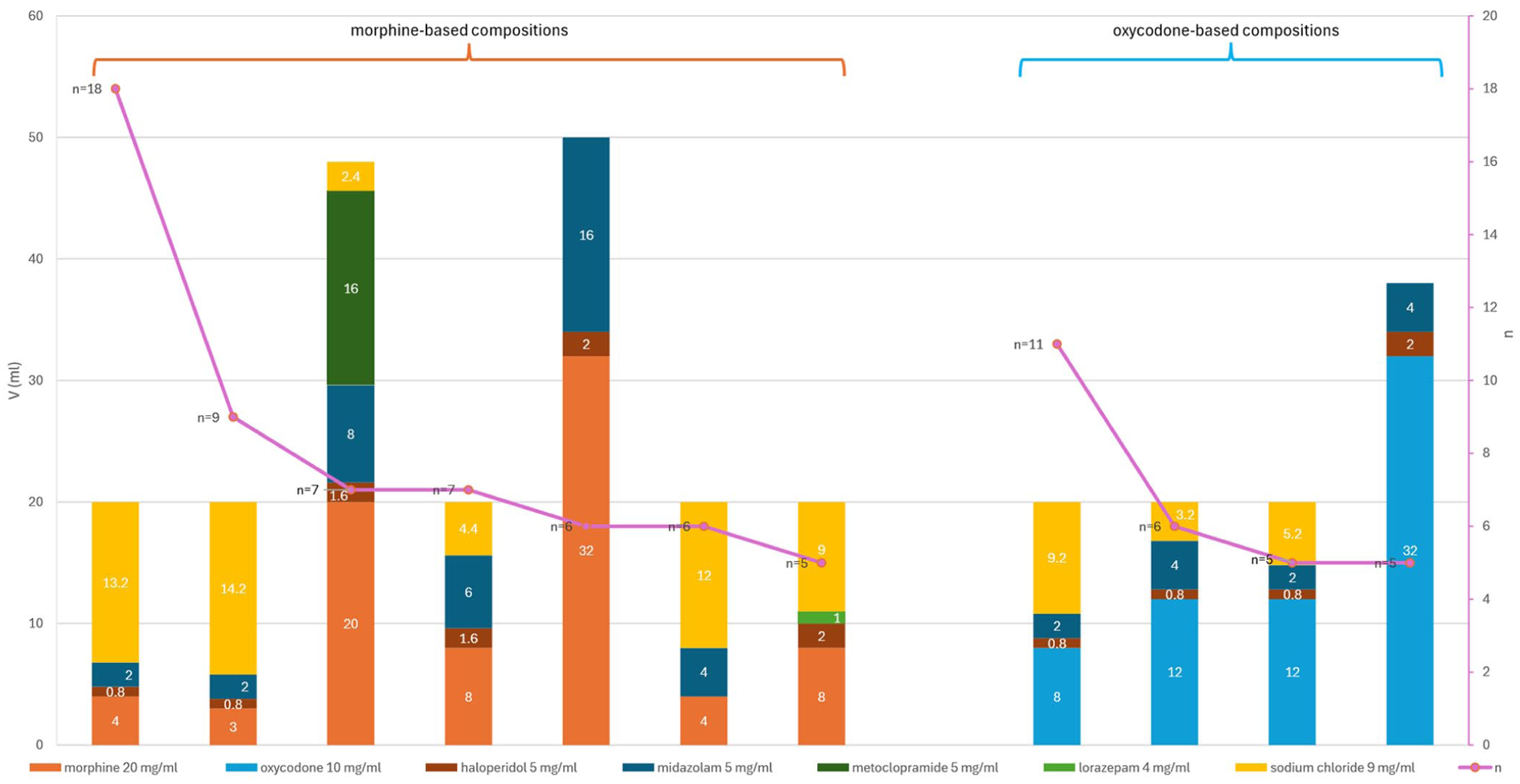
Prevalence of administered drug compositions occurring more than four times in the data (85/329). Bar chart represents volumes of the components in each composition (left Y-axis). Line chart represents the prevalence of the compositions (right Y-axis).
The most prevalent drug combinations, (1) morphine, haloperidol, midazolam and (2) oxycodone, haloperidol and midazolam (Figure 1), accounted for most (8/11) of the compositions presented in Figure 2. However, these two combinations were also the ones with the highest variation in compositions (Table 1).
Number of different compositions among the 10 drug combinations with the greatest variation in compositions.

In 50% of the 10 most frequently used drug combinations, a statistically significant correlation in drug quantities was observed between all the included drug components (Table 2). For example, in all 87 drug combinations containing different quantities of morphine, midazolam and haloperidol, statistically significant correlations were observed between the various quantities of morphine and various quantities of midazolam, as well as morphine and haloperidol, and midazolam and haloperidol, respectively. In 4/10 of the combinations, correlations were statistically significant between only some components, and in 1 combination, no statistically significant correlations were found.
Ten most frequently administered drug combinations categorised by statistical significance of correlation between their component quantities.

Statistically significant correlations (p < 0.05) are highlighted in bold. The drug combinations are presented (1) in ascending order by the number of components, (2) listing morphine-based combinations before oxycodone-based combinations, and (3) in descending order by the prevalence of a component in the data. The drug components in pairs are presented (1) listing opioid containing pairs first and (2) in descending order by the prevalence of a component in the data.
Correlation could not be calculated due to a constant variable.
When reviewing the drug components in pairs, statistically significant correlations were observed in 8/20 drug pairs at least in some of the most prevalent combinations (Table 3). The strength of correlation varied from weak to very strong.
Drug component pairs from the 10 most commonly administered combinations.

cc: correlation coefficient value.
The number of drug combinations in which the component quantities in pairs correlated are categorised by the correlation strength. Only significant correlations (p < 0.05) are presented. Drug pairs are presented in order of (1) morphine containing pairs, (2) oxycodone containing pairs, and (3) in descending component prevalence.
Discussion
Main findings
This study identified a great variety of drug compositions administered as continuous subcutaneous infusions, indicating that palliative and hospice care patients often require individualised medications. However, identifying the most frequently used combinations and investigating correlations between drug quantities provided essential information on admixtures that may be feasible and relevant for standardisation. The combinations of (a) morphine, haloperidol and midazolam, and (b) oxycodone, haloperidol and midazolam were the most frequent drug combinations. Correlation between drug component quantities was particularly strong in morphine-based combinations when the correlation was statistically significant. These findings suggest that standardisation may be possible, especially for certain morphine-based mixtures containing midazolam and haloperidol. Nevertheless, the clinical relevance must be considered alongside correlation-based dosing.
What this study adds
Our findings represent the first step towards the standardisation of drug mixtures administered as continuous subcutaneous infusions for palliative and hospice care patients. To our knowledge, no previous studies have specifically addressed the standardisation of subcutaneous drug mixtures. However, the benefits of standardising intravenous admixtures have been widely evaluated.20,26,27 Also standardisation of continuous subcutaneous infusions could therefore improve medication safety.
Midazolam and haloperidol were the most frequently used drugs in addition to morphine and oxycodone in this study. The frequent use of midazolam and haloperidol in combination with opioids in parenteral drug mixtures in palliative care has also been reported in previous studies.5–7,28 In addition to morphine hydrochloride and oxycodone, other opioids and salt forms (e.g. hydromorphone and morphine sulfate) have previously been highlighted.5–7,29 Levomepromazine and hyoscine butylbromide have also been found common in the mixtures, which differs from our findings.5–7 Global differences in availability of authorised drug products available must be considered when adapting research findings locally.
In this study, morphine and oxycodone were utilised relatively equally, suggesting that both of them are needed in standardised drug mixtures for different clinical situations. The opioid was switched from one to the other for six patients during their treatment. While opioid rotation is a common clinical practice in palliative care, evidence supporting this approach remains limited.30,31 The opioid choice may be dependent on conditions such as kidney or liver failure, tolerability or practical considerations, for example, the volume of the dose to be administered. Subjective factors, including physician’s clinical experience, cost and availability, may also influence opioid selection. Further research is needed to assess why the morphine-based combinations demonstrated stronger correlations between component quantities than oxycodone-based combinations.
According to the correlation analysis, especially certain morphine-based mixtures showed strong, statistically significant correlations between the component quantities. Evaluating such correlations is clinically relevant when considering standardisation, particularly as medication orders may include instructions to increase the infusion rate, thereby escalating the doses of all components. Spearman’s correlation coefficient is, however, a quantitative method for assessing the potential for standardisation and therefore does not account for clinically appropriate dosing. Since safe and effective dose range is wider for opioids than for many other drugs, the component quantities may not correlate when opioid doses become sufficiently high. Moreover, the dose of each drug must always be individually adjusted according to the symptom severity and drug tolerability.
While it may be possible to standardise mixtures administered in this study, further research is needed in several aspects, including the clinical requirements, compatibility and stability of the mixtures, as well as the potential benefits of standardisation. First, the Delphi method could be suitable for evaluating clinically relevant drug mixtures, as it has been used in previous studies.7,26 Second, although compatibility and stability assessments have been conducted on various commonly used mixtures, the exact compositions selected for standardisation should be studied, as variations, for example, in concentration may affect the results.29,32 Finally, standardisation and centralisation of compounding may be especially beneficial in basic-level palliative care units, as it could free up clinicians’ time for actual patient care and lower the threshold for less specialised clinicians to initiate parenteral medication when needed. Nonetheless, the fast and flexible drug delivery should be ensured.
Strengths and limitations
This study examined real-world data from medical records of specialised palliative and hospice care inpatient units and at-home hospital, which are among the largest palliative care providers in Finland. Compared to previous studies that have reported frequently used drug combinations administered as continuous subcutaneous infusions,5–7 our study aimed to evaluate the potential for standardising these combinations. Therefore, we chose to analyse not only the components of the most frequently used combinations but also the quantities of the components and correlations between them.
In this study, we focused mainly on the most frequently used combinations of drug components. Other important aspects relevant to standardisation, which require future evaluation, include infusion durations and pharmacotherapeutic appropriateness. Infusion duration determines how long the admixture must remain microbiologically, physically and chemically stable. In addition, the relevance of mixing the components for very short infusions should be questioned. Finally, it is essential that the mixtures selected for standardisation are critically evaluated in terms of their pharmacotherapeutic usefulness.
The retrospective medical record review study design may be subject to limitations such as inaccuracy, incompleteness and complexity.33,34 In this study, ICD-10 code Z51.5 (palliative care) was recorded only for 70 patients (58.3%), although it is recommended from the beginning of the palliative treatment to ensure appropriate care. 21 The absence of this code in the electronic patient medication record may result from neglections of reporting or the absence of a formal decision for initiation of palliative treatment. While our study was not limited by this finding, as Z51.5 was not an inclusion criterion, the risk of outdated diagnoses should be acknowledged in future research. In addition, the data included ten continuous subcutaneous infusion administrations with volumes below 20 ml. Typically, a minimum of 20 ml is required to fill a cassette reservoir used in patient care units for continuous infusion. Although the reasons for these anomalies could not be verified, the administrations were analysed as recorded.
Although the size of the study population was selected by evaluating the risk of bias, the generalizability of the findings is limited by the relatively small sample. Additionally, since the bolus doses and dose escalations via increased infusion rates were excluded from the analysis, actual daily medication consumption was likely higher and infusion durations shorter than reported.
The data extraction process posed a challenge to this study. Under the Finnish Act on the Secondary Use of Health and Social Data, researchers are not permitted to access patient record system directly, and the dataset of this study was therefore extracted by an external analytics specialist. Consequently, it was not possible to verify the accuracy of the data extraction. Nevertheless, the collected data were found to be sufficiently robust during the analysis phase.
Conclusion
Although palliative and hospice care patients often require individualised medications, this study shows that standardisation might be feasible for mixtures containing midazolam, haloperidol or both, in addition to morphine or oxycodone. Morphine-based drug mixtures appear to have the greatest potential for standardisation according to our statistical findings.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251397004 – Supplemental material for Parenteral morphine and oxycodone mixtures administered in specialised palliative and hospice care units: A retrospective medical record review
Supplemental material, sj-docx-1-pcr-10.1177_26323524251397004 for Parenteral morphine and oxycodone mixtures administered in specialised palliative and hospice care units: A retrospective medical record review by Ilona Niittynen, Jonna Juvankoski, Kaisla Mannerla, Hanna M. Tolonen, Marja Airaksinen and Maria Rautamo in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251397004 – Supplemental material for Parenteral morphine and oxycodone mixtures administered in specialised palliative and hospice care units: A retrospective medical record review
Supplemental material, sj-docx-2-pcr-10.1177_26323524251397004 for Parenteral morphine and oxycodone mixtures administered in specialised palliative and hospice care units: A retrospective medical record review by Ilona Niittynen, Jonna Juvankoski, Kaisla Mannerla, Hanna M. Tolonen, Marja Airaksinen and Maria Rautamo in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524251397004 – Supplemental material for Parenteral morphine and oxycodone mixtures administered in specialised palliative and hospice care units: A retrospective medical record review
Supplemental material, sj-docx-3-pcr-10.1177_26323524251397004 for Parenteral morphine and oxycodone mixtures administered in specialised palliative and hospice care units: A retrospective medical record review by Ilona Niittynen, Jonna Juvankoski, Kaisla Mannerla, Hanna M. Tolonen, Marja Airaksinen and Maria Rautamo in Palliative Care and Social Practice
Supplemental Material
sj-docx-4-pcr-10.1177_26323524251397004 – Supplemental material for Parenteral morphine and oxycodone mixtures administered in specialised palliative and hospice care units: A retrospective medical record review
Supplemental material, sj-docx-4-pcr-10.1177_26323524251397004 for Parenteral morphine and oxycodone mixtures administered in specialised palliative and hospice care units: A retrospective medical record review by Ilona Niittynen, Jonna Juvankoski, Kaisla Mannerla, Hanna M. Tolonen, Marja Airaksinen and Maria Rautamo in Palliative Care and Social Practice
Footnotes
Acknowledgements
We are grateful to Professor, Chief physician Tiina Saarto, Chief physician Taina Toivanen and Chief physician Jaana Saarenheimo for their time and for sharing their expertise in palliative care. We thank Kanerva Korhonen and Annika Häkkinen for their assistance in understanding the protocols in care units, and within electronic health record system, Apotti, and Sanni Kylkilahti for collecting background information in the care units providing palliative care in Helsinki and in wellbeing services counties in the region. Finally, we would like to thank Marisa Eronen and Maiju Visti for their collegial support and contributions during the research project.
Ethical considerations
This study was conducted according to the World Medical Association Declaration of Helsinki and the Finnish Act on the Secondary Use of Health and Social Data, which correspond with the EU’s General Data Protection Regulation. Guidelines for the responsible conduct of research by the Finnish national board on research integrity TENK were followed. Study approval was obtained from the Helsinki Social Services and Health Care Division.
Consent to participate
No separate ethical approval nor patient consents were obtained as the study design was a retrospective non-interventional medical record review, and the data were extracted from the records of deceased patients. The data were pseudonymised for analysis and processed in an audited secure research environment.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: The data extraction performed by an external analytics specialist was funded by Helsinki Hospital. The open access publication fee is funded by University of Helsinki.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Access to the data supporting the findings of this study is restricted due to confidentiality and data protection and, therefore, is not publicly available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.