
Abstract
Background:
Systematic adaptation of evidence-informed interventions is critical for effective transfer across settings. Public health palliative care interventions pose unique challenges because of their complexity and embedding in dynamic, real-life settings. The ADAPT guidance provides a comprehensive framework for systematically adapting evidence-informed health interventions, yet its application in public health palliative care remains unexplored.
Aim:
Within the EU NAVIGATE project, this study describes the international adaptation process of a Canadian navigation program supporting older people with cancer experiencing declining health, for implementation in six European countries. It also reflects on the methodological insights gained from applying the ADAPT guidance in public health palliative care.
Design:
Using an iterative five-stage multi-method approach, we followed the ADAPT guidance and its recommended frameworks. Stage 1 assessed context-intervention fit and identified core and adaptable components of the original intervention. Stage 2 adapted implementation materials, while stage 3 involved a contextual analysis. Stage 4 focused on adapting the training for implementers, and stage 5 reviewed feasibility.
Results:
The ADAPT guidance proved flexible and useful, though systematic adaptation posed challenges due to the unique complexities of public health palliative care interventions. These included balancing intervention integrity with cultural sensitivities and local juridical regulations regarding end of life. Our process addressed these challenges through contextual assessments, identifying core components, engaging with original developers, and collaboration between local and international adaptation teams.
Conclusions:
A systematic adaptation process, guided by the ADAPT guidance is feasible, but transferring public health palliative care interventions requires careful methodological, contextual, and conceptual considerations.
Systematic adaptation can improve context-intervention-fit when transferring evidence-based population health interventions across settings. This enhances their adoption, implementation, effectiveness, and sustainability.
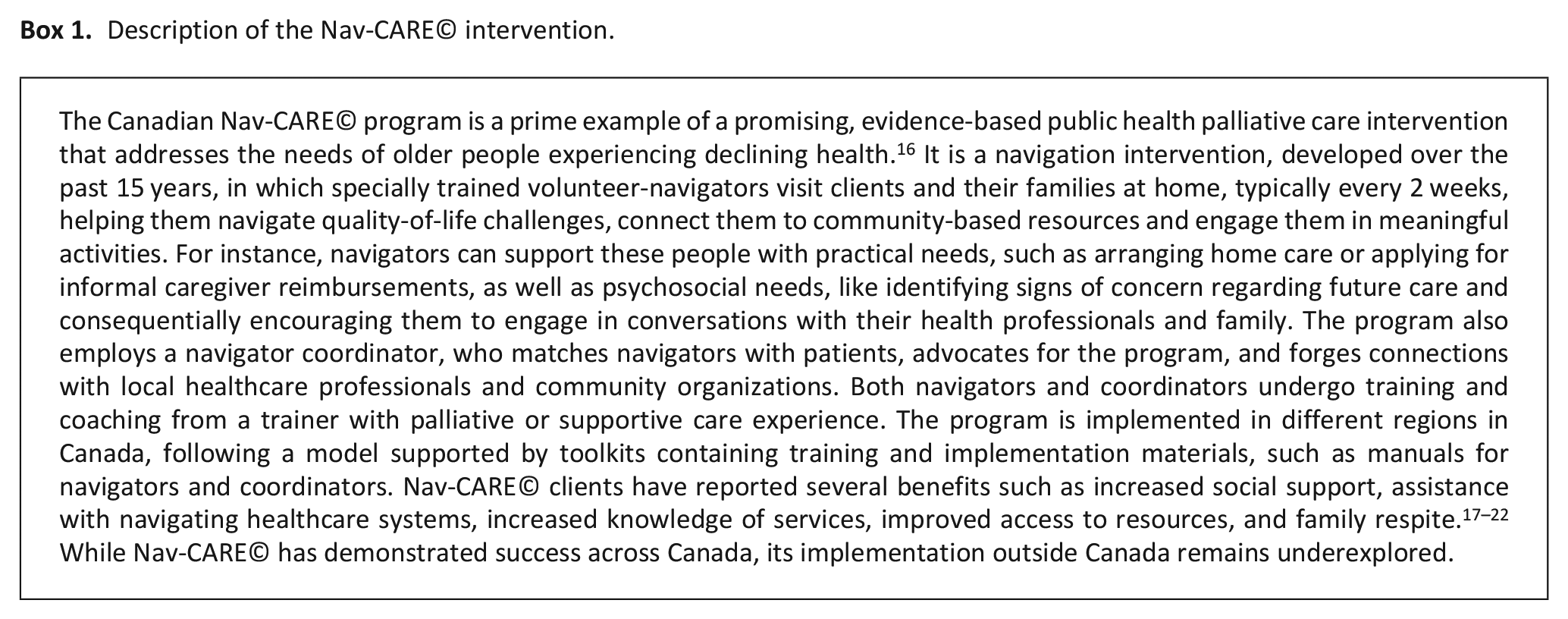
Adapting public health palliative care interventions to new (international) settings is especially challenging, as they operate at the community level, where complexity arises from several factors, including their multiple components, implementation in large scale environments, and the unpredictability and variability inherent to real-life settings. Furthermore, cultural sensitivities around serious illness and palliative care play a critical role in shaping the delivery and reception of interventions.
The ADAPT guidance provides evidence and consensus-informed guidance for systematically adapting and transferring evidence-informed population health interventions to new settings, but research demonstrating how it can be practically applied by researchers in the context of public health palliative care interventions is scarce.
In addition to the ADAPT guidance, we found that 1 conducting thorough contextual assessments, 2 identification of the intervention’s core functional components to maintain its integrity, 3 engaging with original developers, and 4 involving both local and international adaptation teams throughout the process greatly facilitated the adaptation of our public health palliative care intervention.
Key challenges included balancing intervention integrity with local adaptation needs, managing the adaptation process across international settings, and estimating the consequences of adaptations before implementation.
Future research on the systematic adaptation of public health palliative care interventions should focus on investigating how adaptations influence implementation processes and outcomes.
Systematic adaptation can be highly beneficial to incorporate as an implementation strategy in implementation frameworks to enhance the adoption, effectiveness, and sustainability of public health palliative care interventions.
Background
The systematic adaptation of evidence-based interventions is increasingly recognized as essential for effective transfer across different settings or populations. This article considers systematic adaptation as to improve the intervention-context fit while maintaining the intervention’s integrity. 1 Tailoring interventions to align with the unique contextual characteristics of the implementation setting can improve their fit and potential impact. Contextual differences between the original and new settings can significantly influence intervention outcomes, and replicating interventions without thorough adaptation often fails to achieve comparable or sustainable results.1 –3 These challenges are especially pronounced in public health palliative care interventions, which are inherently complex and deeply embedded in real-life settings.4 –6 Unlike interventions implemented in more controlled environments, such as hospitals, public health palliative care interventions operate at the community level, where complexity arises from several factors, including their multiple components,5,7 implementation in large scale environments like communities or cities, and the unpredictability and variability inherent to real-life settings.8,9 Furthermore, cultural sensitivities around serious illness and palliative care play a critical role in shaping the delivery and reception of interventions, and can vary widely between countries and settings, requiring careful adaptation to respect local values, beliefs, and practices while maintaining the integrity of the intervention.
Given the growing recognition of these challenges, a variety of theories, frameworks, guidelines, and tools have emerged to support the systematic adaptation of interventions. These resources are aimed at recognizing and documenting adaptations,10,11 designing and implementing tailored modifications, 2 and systematically planning and evaluating the adaptation process.12,13 Among these, the ADAPT guidance 1 stands out as the most recent and comprehensive framework offering evidence and consensus-informed guidance14,15 for systematically adapting and transferring evidence-informed population health interventions to new settings. However, despite its potential, limited research exists demonstrating how the ADAPT guidance can be practically applied by researchers, particularly in the context of complex public health palliative care interventions.
Several European countries face significant challenges in meeting the needs of older people with cancer and their families. In these countries, healthcare systems often struggle with fragmented care delivery, lack of coordinated care and services, limited or unequal access to care and resources, and insufficient social support for patients and families. European countries have reported rising numbers of older adults with cancer, highlighting the potential of programs like Nav-CARE© (Box 1) to address the needs of older people with cancer and their families.16,22,23 However, to achieve similar benefits in European countries as in Canada, a systematic adaptation of Nav-CARE© is essential.
Description of the Nav-CARE© intervention.
Within the Horizon Europe-funded EU NAVIGATE project,24,25 we aim to adapt, implement, and evaluate the Nav-CARE© program for older people with cancer across the continuum of supportive, palliative, and end-of-life care in six European countries: Belgium, the Netherlands, Ireland, Italy, Poland, and Portugal, representing different contexts and health care systems. This paper describes the international and systemic adaptation process of the Canadian Nav-CARE© program 15 and reflects on the use of the ADAPT guidance 1 in the context of international public health palliative care interventions. By sharing these reflections, we aim to provide valuable insights for researchers and practitioners seeking to transfer complex public health interventions across settings, particularly in palliative care.
Methods
Study design
We used an iterative five-stage multi-method approach (Figure 1), 24 using the ADAPT guidance 1 and its recommended frameworks (described below) to adapt the Nav-CARE© program to six EU countries: Belgium, Ireland, Italy, the Netherlands, Poland, and Portugal. Table 1 outlines the main stages suggested by the ADAPT guidance, detailing how we applied these stages in our adaptation process, including data sources and output per stage.
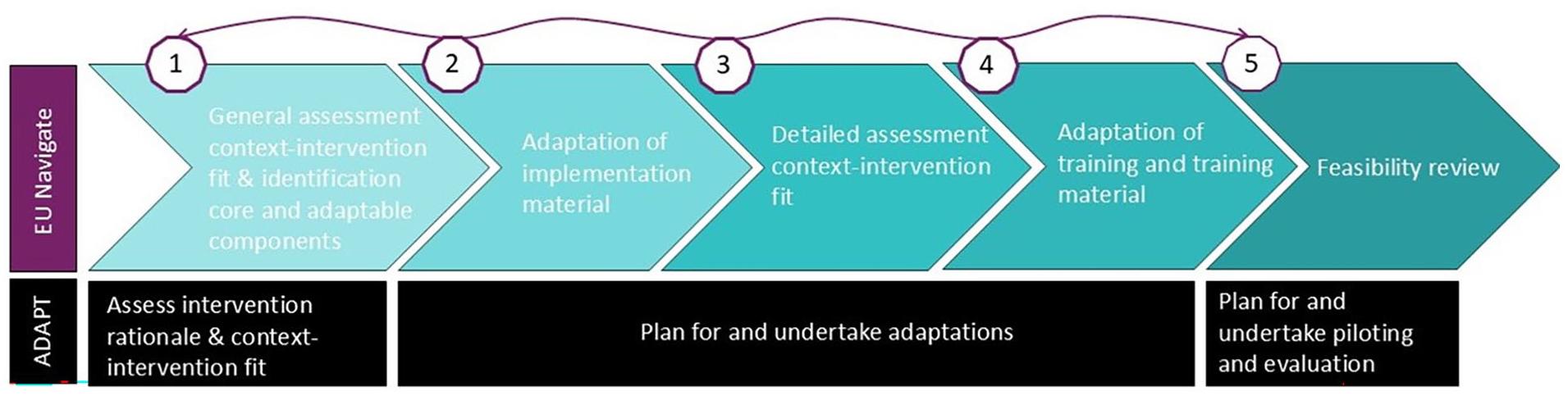
Flowchart adaptation process within the EU Navigate project, informed by the ADAPT guidance.
Overview of the recommended stages by the ADAPT guidance, the adaptation process used in EU NAVIGATE project, the data sources, and output.
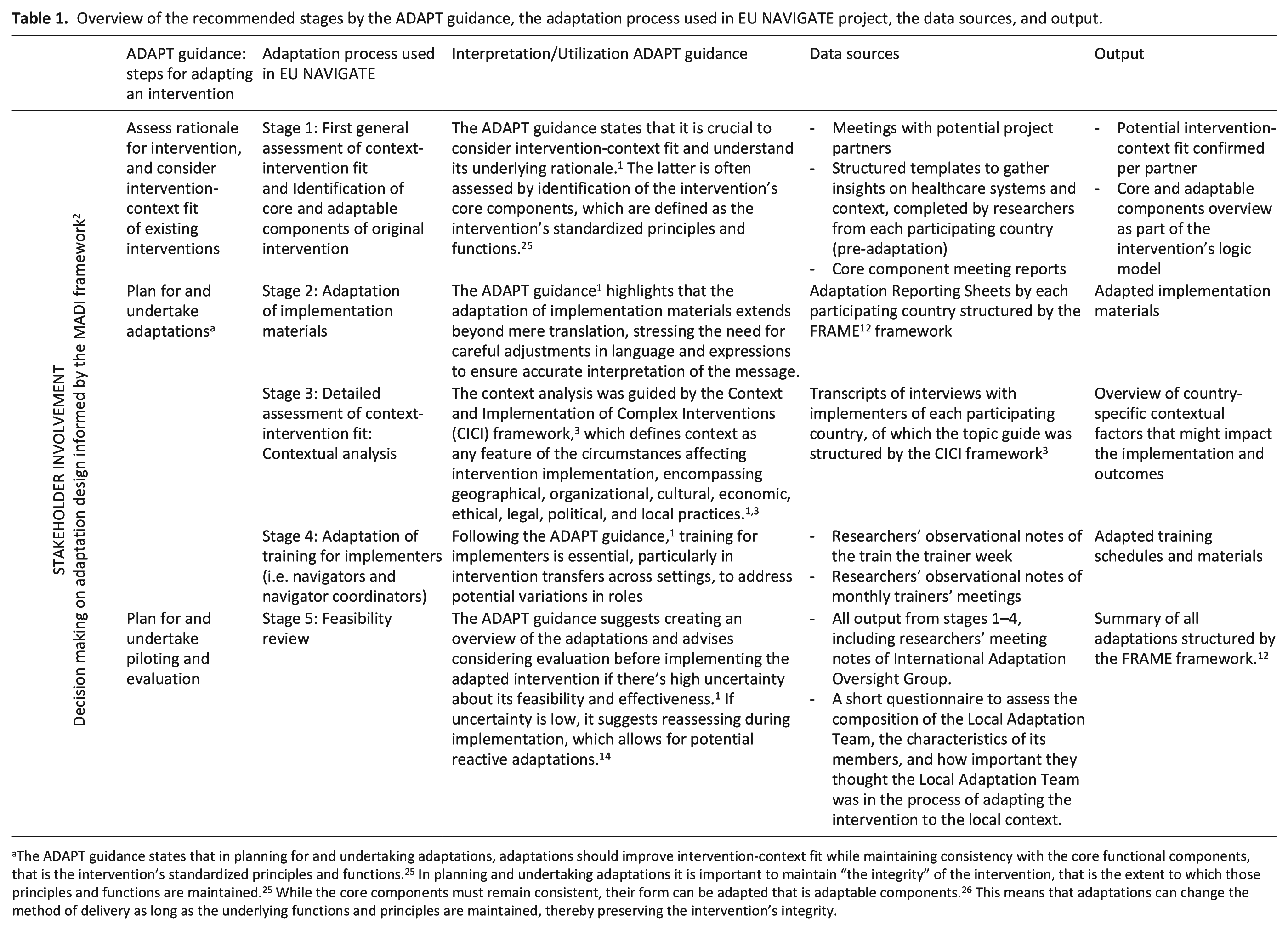
The ADAPT guidance states that in planning for and undertaking adaptations, adaptations should improve intervention-context fit while maintaining consistency with the core functional components, that is the intervention’s standardized principles and functions. 25 In planning and undertaking adaptations it is important to maintain “the integrity” of the intervention, that is the extent to which those principles and functions are maintained. 25 While the core components must remain consistent, their form can be adapted that is adaptable components. 26 This means that adaptations can change the method of delivery as long as the underlying functions and principles are maintained, thereby preserving the intervention’s integrity.
We used three frameworks, described in the ADAPT guidance as optional, throughout the adaptation process. The Model for Adaptation Design and Impact (MADI) structured our decision-making on adaptation design at the end of all stages, considering relationships among adaptations and their potential impact on outcomes. 2 The Context and Implementation of Complex Interventions (CICI) framework guided the context analysis in stage 3, facilitating a structured holistic conceptualization and assessment of context. 3 The Framework for Reporting Adaptations and Modifications-Expanded (FRAME) was used in the final stage to integrate, summarize, and report all adaptations and to reflect on the process. 12
Study settings
The Nav-CARE© program was adapted for implementation across six European countries: Belgium, Ireland, Italy, the Netherlands, Poland, and Portugal. The selection of implementation settings (such as a specific region, city, or community), and implementation organizations (a particular local organization with whom the research teams collaborate for implementation) aimed to ensure diverse healthcare system characteristics and contextual factors, in terms of the latest Healthcare System Typology of OECD¹ countries. 27 There are eight implementation settings in total, with two in Belgium and Italy and one in each other participating country. An overview of the implementation settings and organizations is shown in Table 2.
Overview of implementation settings, organizations, and type of health care system, based on the Healthcare System Typology of OECD a countries, per participating country in the EU NAVIGATE project.
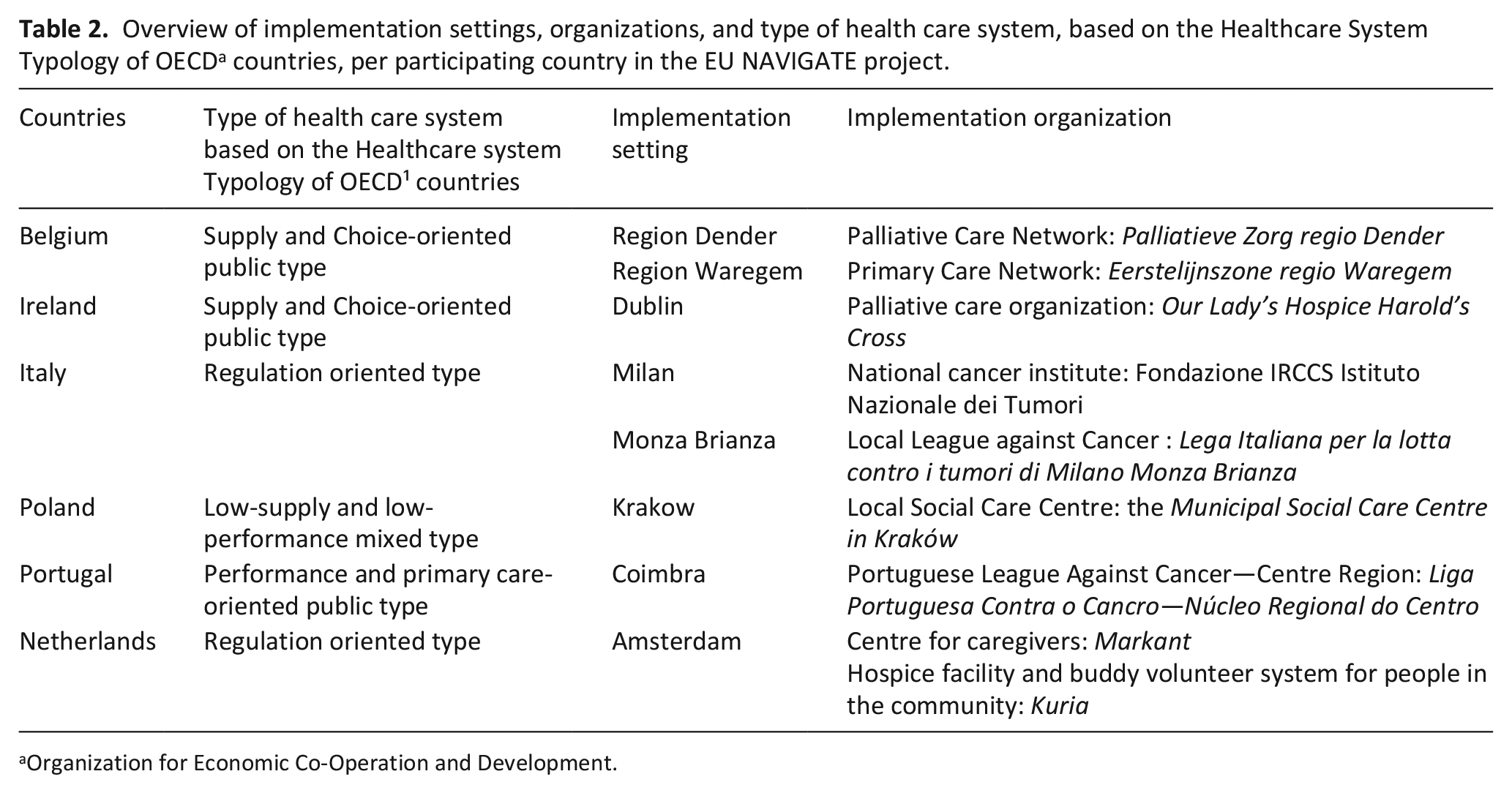
Organization for Economic Co-Operation and Development.
Adaptation teams
The ADAPT guidance stresses stakeholder involvement throughout all adaptation stages to enhance the intervention-context fit. This involves a core team, ideally comprising members of the public, patient populations, policy and practice stakeholders, and the researchers involved,1,28 following a multi-stakeholder and Patient Public Involvement approach.29,30 In EU NAVIGATE, each implementation setting assembled a Local Adaptation Team following this structure.
Additionally, we established an International Adaptation Oversight Group, consisting of the original Nav-CARE© program developers (BP and WD), the general trial and implementation coordinators (FVC and LVdB), and the adaptation and training coordinators of the EU NAVIGATE project (KC and JG). This group coordinated and facilitated the adaptation process, communicated planned or made adaptations bilaterally or consortium-wide, and aimed to balance the original intervention’s integrity with setting-specific adaptations. Cooperation between these two teams was central to ensure this balance.
Adaptation and data collection process
The steps suggested by the ADAPT guidance, our adaptation process, including data sources and output are displayed in Table 1.
Stage 1: General assessment intervention-context fit and identification core components
We asked experienced researchers from each participating country (KS; MFB; AD; DF; AVDP; and LVdB) to complete a structured template (Supplemental Appendix 1) to gather insights into the intervention-context fit at the start of the adaptation process. 31 The template had two sections: potential local implementation organizations, implementers, and local stakeholder groups such as volunteer or healthcare organizations. The second part included questions such as 1 the type of health care system, 2 the integration of end-of-life care within cancer care for older patients, 3 the current state of research, practice, and policy regarding navigation programs and 4 a preliminary feasibility assessment of the project in the potential implementation setting.
Additionally, we held several meetings with the International Adaptation Oversight Group to discuss the core versus adaptable components of the intervention. These discussions, informed by the original model 32 and data from previous studies,16 –21 resulted in an overview structured by the TIDieR 33 checklist, which were then integrated into the intervention’s logic model.
Stage 2: Adaptation of implementation materials
In the ADAPT guidance stage “planning and undertaking adaptations,” we translated and adapted the training and implementation materials, and performed a contextual analysis in the different countries.
During this stage, researchers (FVC and KC) collected Adaptation Reporting Sheets (Supplemental Appendix 1) completed by a research member of each Local Adaptation Team and structured by the FRAME framework. 19 The researchers categorized suggested adaptations into themes 34 according to the framework, 34 such as what is modified and for whom is the adaptation intended. These were discussed during multiple meetings with both the International Adaptation Oversight Group and Local Adaptation Teams in each country.
Stage 3: Detailed assessment of context-intervention fit: Contextual analysis
Two researchers (FVC and KC) conducted semi-structured duo-interviews with implementers of each participating country. 14 The topic guide (Supplemental Appendix 1), based on the seven contextual domains of the Context and Implementation of Complex Interventions framework,3,34 included questions such as “What regulations regarding palliative care, patient rights, and end-of-life decisions are in place in your implementation setting that could influence the implementation, delivery, or outcomes of this intervention?”. Transcribed verbatim (FVC), the data were coded into the seven contextual domains of the framework per participating country and discussed within the International Adaptation Oversight Group.
Stage 4: Adaptation of training for implementers
Designated trainers in each country adapted the training to the local context during an international five days “train-the-trainer week.” Six training modules were covered (Supplemental Appendix 2), with participants proposing adaptations to the curriculum that best suit their context after each module. These adaptations let to adapted training schedules and learning materials. The researcher (FVC) made observational notes during the training and follow-up meetings with the trainers, which were discussed with the International Adaptation Oversight Group.
Stage 5: Feasibility review
During this stage, researchers from each implementation setting completed a short questionnaire to assess the composition of their Local Adaptation Team, the characteristics of its members, and perceived importance of the Local Adaptation Team during the adaptation process. This was asked using a six-point Likert scale with questions such as “In general, how important do you consider this Local Adaptation Team during the adaptation process of this intervention in your implementation setting?”.
Data analysis and integration
The researcher (FVC) analyzed all qualitative data (completed structured templates, Adaptation Reporting Sheets, transcripts of the duo-interviews, observational notes of the train the trainer week and monthly trainers’ meetings), using directed content analysis 35 and pre-determined coding schemes structured by the frameworks stated above (Supplemental Appendix 1). Descriptive statistics, 36 such as the median and interquartile ranges, were used for the questionnaire assessing the Local Adaptation Team.
The researcher (FVC) assessed concordance and discordance of the adaptation information across data sources, including all meeting notes of the International Adaptation Oversight Group, using the categories of the FRAME framework. 12 This categorization was reviewed and discussed at team meetings (FVC, KC, LVdB, TS, LP, BP, and WD), which led to further refining and reflections reported upon in the results section. Once consensus was reached and feasibility assessed for, the researcher (FVC) completed the final version which is included as Supplemental Appendix 4.
Ethics
The protocol for this adaptation process was included as a Supplemental Appendix to the main trial protocol. 37 Approvals from the relevant ethics committees were obtained in all participating countries. Belgium: Commissie Medische Ethiek, 09/08/2023, EC-2023-164; Ireland: SJH/TUH Joint Research Ethics Committee, 14/11/2023, 3726; Italy: Comitato Etico Territoriale Lombardia, Istituto Nazionale dei Tumori, 31/07/2023, INT171/23; the Netherlands: METC Amsterdam UMC, 22/08/2023, 2023.0489; Portugal: Ethics Committee of the Faculty of Medicine of the University of Coimbra and Ethics Committee of the Portuguese Institute of Oncology of Coimbra Francisco Gentil, 25/09/2023, EO04/2023; Poland: Komisja Bioetyczna, Uniwersytetu Jagiellońskiego, 14/06/2023, 1072.6120.55.2023. The trial is registered on Clinicaltrials.gov (ID: NCT06110312). All members of the adaptation teams gave verbal informed consent prior to data collection. All obtained data were pseudonymized.
Results
Results, examples, and reflections on opportunities and challenges on the adaptation process are shown in Table 3, following a description of the composition and characteristics of the adaptation teams.
Overview of results and reflections on the use of the ADAPT guidance for the adaptation process of Nav-CARE © program.
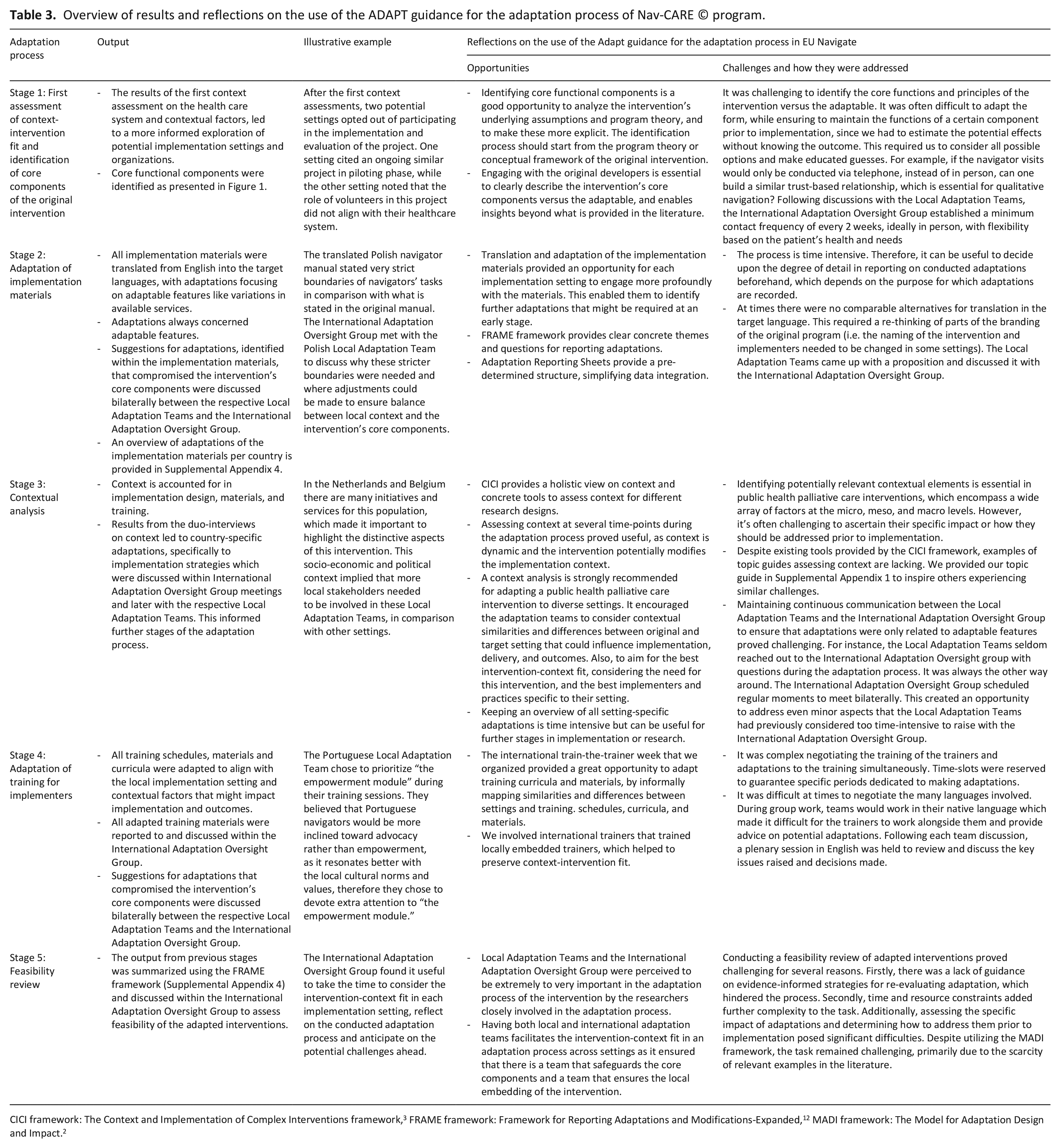
The adaptation process of the Nav-CARE© program was conducted from September 2022 until November 2023. The integration and analysis of all data sources and output included 6 completed structured templates on context, 6 completed adaptation reporting sheets, 36 adapted intervention materials, 6 duo-interview transcripts, 19 International Adaptation Oversight Group meeting notes, and 7 completed questionnaires on the composition and perceived importance of the Local Adaptation Teams.
Local adaptation teams
The Local Adaptation Teams included seven teams in total, one for each country except Belgium, which had two very distinct implementation settings and therefore two teams (Supplemental Appendix 3). The number of represented organizations in these teams varied from 2 to 12 between settings, with hospitals, universities/research groups and volunteer organizations, being the most represented in descending order. Members comprised researchers, implementers, representatives from the target population (i.e. older persons in declining health with cancer, close family caregivers, or volunteers), and health professionals working in the implementation setting (i.e. home care, oncology and palliative care nurses, community health workers, social workers, and psychologists). The number of members varied from 3 to 14 of whom most were health professionals followed by implementers or researchers. The number of meetings varied from 2, in Portugal, to 12, in the Netherlands and Poland, over approximately 1 year.
Results of the adaptation process
In stage 1, the International Adaptation Oversight Group identified and summarized core components of the intervention (Figure 2).
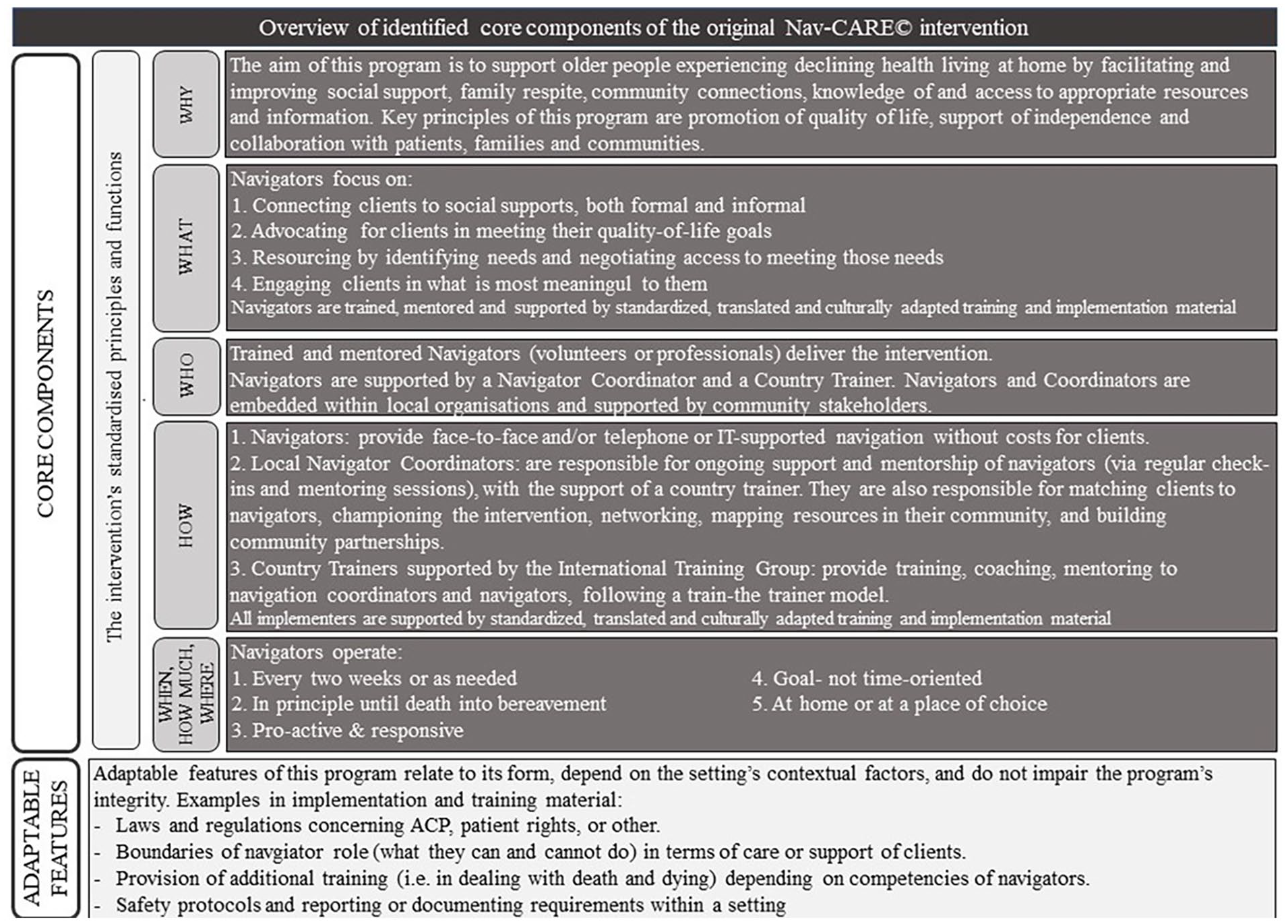
Overview of the identified core and adaptable features of the original Nav-CARE© program, based on the original program theory and guided by the TIDieR checklist. Created in stage 1 of the adaptation process for the EU NAVIGATE project.
Discussion
Main findings
The new ADAPT guidance 1 and its recommended frameworks proved useful to guide the systematic adaptation process of the Nav-CARE© program for the EU NAVIGATE project across settings in six EU countries. The flexibility of the ADAPT guidance allowed for tailoring of the adaptation process, enabling selection of stages, frameworks, and elements based on specific rationales, incentives, and adaptation needs of the intervention. It was challenging to identify the core versus adaptable components, to manage the complex adaptation process across different countries, and to assess potential contextual interactions that might be worth identifying prior to implementation.
Transferable learnings for those seeking to adapt and transfer public health palliative care interventions to new settings
Prior research to develop the ADAPT guidance already identified most of the abovementioned challenges and gaps in existing guidance for adapting evidence-based health interventions.14,15 This article can serve as an example of an approach that can build on the ADAPT guidance. We recommend thorough contextual assessments, identification of core components with engagement of original developers and involvement of both local and international adaptation teams throughout the entire adaptation process for those seeking to adapt and transfer a public health palliative care intervention to new settings.
Identifying core components to maintain the intervention’s integrity enables a systematic adaptation process and meaningful coherent evaluation.14,38,39 Drawn from the updated UK Medical Research Council guidance for developing and evaluating complex interventions, 32 we emphasize the importance of starting from the intervention’s original program theory (i.e. the Nav-CARE© navigation model 16 ) focusing on the principles and functions, to identify and overview the core components. We added more specificity based on the data from previous studies,16 –21 integrated this overview in the intervention’s logic model, and reconciled them with the original developers. Adopting an “integrity” perspective together with the developers facilitated the adaptation process. This aligns with experiences shared by other researchers in adaptation studies. 40 Integrity of an intervention moves beyond the discussion on implementation fidelity, but challenges intervention adapters to consider the why as well as the what of an intervention. 26
When adapting a public health palliative care intervention to diverse settings, we strongly recommend assessing implementation context at several time points with both local and international adaptation teams. Firstly, as these interventions are implemented in dynamic real-life settings and bound to a particular health care system with unique complexities and sensitivities (i.e. socio-economic and political challenges such as a fragmented healthcare system, socio-cultural challenges such as sensitivities regarding palliative care, etc.), a better intervention-context fit increases the likelihood of sustainable effects, similar to the original intervention. 3 The assessments in our adaptation process encouraged local adaptation teams to consider contextual similarities and differences between original and target setting that could influence implementation, delivery, outcomes, and sustainability. 32 For instance, identifying specific gaps in the target setting and profiling the program to other local stakeholders were key considerations. Secondly, as this intervention was adapted across multiple settings and countries, local adaptation teams for each site, and an International Adaptation Oversight Group played vital roles in maintaining the balance between intervention integrity and localization during the adaptation process, which is consistent with findings from other studies adapting interventions across diverse (international) settings. 15 In Poland, Portugal, Ireland, and Italy, implementation sites chose to remove sections on Medical Assistance in Dying (MAID) and Advance Care Planning (ACP) from the volunteer manual, as some of these topics are either inapplicable, unknown, or illegal in some countries. The International Adaptation Oversight Group identified key concepts and rationales within these topics that are important for volunteers in palliative care to understand. The Local Adaptation Teams then adapted the content to align with local regulations and context, using this list as a guide.
Keeping an overview of all setting-specific contextual adaptations was time- and resource-intensive, but useful in further stages of implementation and evaluation, such as the interpretation of outcomes (i.e. informational/social support) in a certain context or the differences between settings. When interventions are not effective, “context” is often cited as a potential reason,28,41,42 though this is not systematically assessed, examined, or reported upon beforehand—only afterwards in the process evaluation.
Strengths and limitations
Our international, multi-setting, multi-method, and multi-stakeholder systematic approach provided diverse and nuanced perspectives on the adaptation process, offering insights beyond the ADAPT guidance. However, modifications to stages, methods, and frameworks may be necessary for other public health palliative care interventions, considering variations in settings, contexts, and adaptation needs. 43 This article seeks to contribute to the systematic adaptation of such interventions, aiming to enhance their adoption, implementation, effectiveness, and sustainability. 44
One limitation of our adaptation process was the limited direct involvement of the target population, such as patients and families. Although we aimed to engage these groups, logistical challenges, cultural sensitivities, and varying capacities of the Local Adaptation Teams impeded their participation across sites. Instead, we relied on Local Adaptation Teams’ members, including professionals with lived experiences, to provide indirect insights into the perspectives of the target population. While this approach ensured some consideration of their needs, we acknowledge that this is not a substitute for direct participation.
Although we will conduct an elaborate evaluation as part of the EU NAVIGATE project 37 and this adapted intervention “borrows strength” from the evidence base of the original intervention, 45 one main limitation of this study is the relatively limited feasibility testing of the adapted interventions. Consistent with findings from similar adaptation research, 38 we found a lack of guidance on evidence-informed strategies for re-evaluating adapted interventions. Additionally, assessing the specific impact of adaptations and determining how to address them prior to implementation during data analysis posed significant challenges, despite utilizing multiple frameworks. More examples in the literature, illustrating re-evaluation of the adapted interventions, would aid greatly.
Recommendations for future research
Future adaptation research of public health palliative care interventions should explore systematic adaptation as an implementation strategy 13 and assess its impact on both implementation and effectiveness outcomes.14,15 Given the unique complexities in concept, scale, and setting of these interventions, 9 systematic adaptation can be a valuable technique to enhance adoption, implementation, effectiveness, and sustainability. 46 Rather than being viewed as an option during implementation, adaptation could be integrated as an implementation strategy in implementation frameworks such as RE-AIM. 47 Additionally, the impact of adaptation on implementation and effectiveness outcomes is rarely systemically assessed. Evaluation frameworks such as RAINBOW 48 should incorporate adaptation and provide relevant analysis methods, such as contribution analysis, 49 to evaluate this impact.14,15
Future research should prioritize strategies for directly engaging patients and families in adaptation processes to ensure their needs and preferences are effectively understood and incorporated. This may include developing tailored approaches to address logistical challenges, fostering cultural sensitivity, and enhancing the capacity of adaptation teams to facilitate meaningful and inclusive participation.
Conclusion
The systematic adaptation process of the Nav-CARE© program across six countries within the EU NAVIGATE project was guided by the new ADAPT guidance, proving flexible and useful despite challenges such as identifying core components and managing adaptation across diverse countries. In addition, engagement of original developers facilitates deeper insights into program theory and mechanisms. Involvement of local adaptation teams and an International Adaptation Oversight Group was crucial for maintaining integrity while allowing for localization. Overall, this study offers valuable insights into the systematic adaptation of public health palliative care interventions, potentially enhancing their adoption, implementation, and effectiveness across diverse settings.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163251320507 – Supplemental material for Systematic adaptation of public health palliative care interventions across settings using ADAPT guidance: Methodological learnings from the EU NAVIGATE project
Supplemental material, sj-docx-1-pmj-10.1177_02692163251320507 for Systematic adaptation of public health palliative care interventions across settings using ADAPT guidance: Methodological learnings from the EU NAVIGATE project by Fien Van Campe, Kenneth Chambaere, Lara Pivodic, Joni Gilissen, Barb Pesut, Wendy Duggleby, Tinne Smets, Katarzyna Szczerbińska, Maja Furlan de Brito, Andrew Davies, Davide Ferraris, Annicka van der Plas, Bianca Scacciati and Lieve Van den Block in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163251320507 – Supplemental material for Systematic adaptation of public health palliative care interventions across settings using ADAPT guidance: Methodological learnings from the EU NAVIGATE project
Supplemental material, sj-docx-2-pmj-10.1177_02692163251320507 for Systematic adaptation of public health palliative care interventions across settings using ADAPT guidance: Methodological learnings from the EU NAVIGATE project by Fien Van Campe, Kenneth Chambaere, Lara Pivodic, Joni Gilissen, Barb Pesut, Wendy Duggleby, Tinne Smets, Katarzyna Szczerbińska, Maja Furlan de Brito, Andrew Davies, Davide Ferraris, Annicka van der Plas, Bianca Scacciati and Lieve Van den Block in Palliative Medicine
Supplemental Material
sj-docx-3-pmj-10.1177_02692163251320507 – Supplemental material for Systematic adaptation of public health palliative care interventions across settings using ADAPT guidance: Methodological learnings from the EU NAVIGATE project
Supplemental material, sj-docx-3-pmj-10.1177_02692163251320507 for Systematic adaptation of public health palliative care interventions across settings using ADAPT guidance: Methodological learnings from the EU NAVIGATE project by Fien Van Campe, Kenneth Chambaere, Lara Pivodic, Joni Gilissen, Barb Pesut, Wendy Duggleby, Tinne Smets, Katarzyna Szczerbińska, Maja Furlan de Brito, Andrew Davies, Davide Ferraris, Annicka van der Plas, Bianca Scacciati and Lieve Van den Block in Palliative Medicine
Supplemental Material
sj-docx-4-pmj-10.1177_02692163251320507 – Supplemental material for Systematic adaptation of public health palliative care interventions across settings using ADAPT guidance: Methodological learnings from the EU NAVIGATE project
Supplemental material, sj-docx-4-pmj-10.1177_02692163251320507 for Systematic adaptation of public health palliative care interventions across settings using ADAPT guidance: Methodological learnings from the EU NAVIGATE project by Fien Van Campe, Kenneth Chambaere, Lara Pivodic, Joni Gilissen, Barb Pesut, Wendy Duggleby, Tinne Smets, Katarzyna Szczerbińska, Maja Furlan de Brito, Andrew Davies, Davide Ferraris, Annicka van der Plas, Bianca Scacciati and Lieve Van den Block in Palliative Medicine
Footnotes
Acknowledgements
We would like to thank all stakeholders and researchers who participated in the Local Adaptation Teams and in the International Adaptation Oversight Group.
Author contributions
All authors have contributed to the following categories for authorship. Study conception and design: Gilissen, Chambaere, Van den Block, Pesut, Duggleby, Pivodic, Smets, and Van Campe. Acquisition of data: Van Campe and Chambaere. Analysis and interpretation of data: Van Campe, Chambaere, Pivodic, Pesut, Duggleby, Smets, and Van den Block. Drafting the manuscript: Van Campe. Critical revision: Van Campe, Chambaere, Pivodic, Gilissen, Pesut, Duggleby, Smets, Szczerbińska, Furlan de Brito, Davies, Ferraris, Scacciati, Van Der Plas, and Van den Block. All authors approved the final manuscript and agreed to be accountable for all aspects of the work. Questions related to the accuracy or integrity of any part of the work will be appropriately investigated and resolved.
Data availability
The data that support the findings of this study are available from the corresponding author, FVC, upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Union, Horizon Europe (2022-2027) [grant no. 101057361].
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.