
Abstract
Palliative care must be integrated into primary care to achieve Universal Health Coverage and hit Target 3.8 of the 2030 Agenda for Sustainable Development – ‘health for all at all ages’. The definition and scope of primary palliative care must be clarified to achieve the goal of ‘palliative care for all’ as part of the global initiative for primary care-driven universal health coverage.
‘Health for all’ entails ‘palliative care for all’
An estimated 61 million people worldwide, 80% of whom reside in low-and-middle-income countries, experience serious health-related suffering that palliative care could alleviate. 1 Experts have identified palliative care as a component of the human right to health and an important aspect of health care. 2 Indeed, palliative care will become increasingly relevant as population ageing and the prevalence of non-communicable diseases continue to increase through the second quarter of the 21st century.2,3
The 2007 World Health Organization (WHO) public health strategy for palliative care introduced the vision of ‘Palliative Care for All’, echoing the vision of the 1978 Alma Alta Declaration – ‘Health for All by the year 2000’.4,5 Tireless advocacy led to the 2014 adoption of World Health Assembly Resolution 67.19,
6
which committed all WHO member states to provide appropriate and compassionate care for all patients regardless of underlying condition. A year later, the United Nations General Assembly adopted the 2030 Agenda for Sustainable Development Goals.
7
Goal three ‘Health for All’ includes the ambitious Goal 3.8, which includes universal health coverage. This declaration recognises that
universal health coverage implies that all people have access, without discrimination, to nationally determined sets of the needed promotive, preventive, curative, rehabilitative and palliative essential health services, and essential, safe, affordable, effective and quality medicines and vaccines, while ensuring that the use of these services does not expose the users to financial hardship, with a special emphasis on the poor, vulnerable and marginalized segments of the population (italics added).
8
In line with WHO policy on the management of non-communicable diseases, this resolution rightly recognised that comprehensive delivery of palliative care could be best achieved through primary care. 9 Alma Ata (1978) had emphasised the importance of primary care in achieving ‘health for all’, drawing on the tradition of Community Orientated Primary Care which had developed as a concept as far back as the 1940s in Africa. 10 Despite WHO’s ongoing commitment to achieving ‘health for all’ through primary health care, implementation continues to be elusive, largely as a result of the seductive nature of specialist over generalist approaches and polices that favoured disease-specific delivery systems. These include: maternal and child health, tuberculosis eradication and HIV management which were included in the Millennium Development Goals 2000–2015. Challenges notwithstanding and 40 years on, the 2018 Astana Declaration on Primary Health Care reaffirmed the vision of Alma Ata. 11
The evolution of the term ‘primary palliative care’
The term ‘primary palliative care’ gained traction at the turn of the millennium and was highlighted in the BMJ 20 years ago, with a call for investment and research. 12 Unfortunately, particularly in North America, the term ‘primary palliative care’ became synonymous with ‘generalist palliative care’, 13 blurring its distinctive identity as ‘palliative care delivered in a primary care context’. Primary palliative care as originally understood is a subset of generalist palliative care (i.e. provided in primary care) but is not equivalent to it.
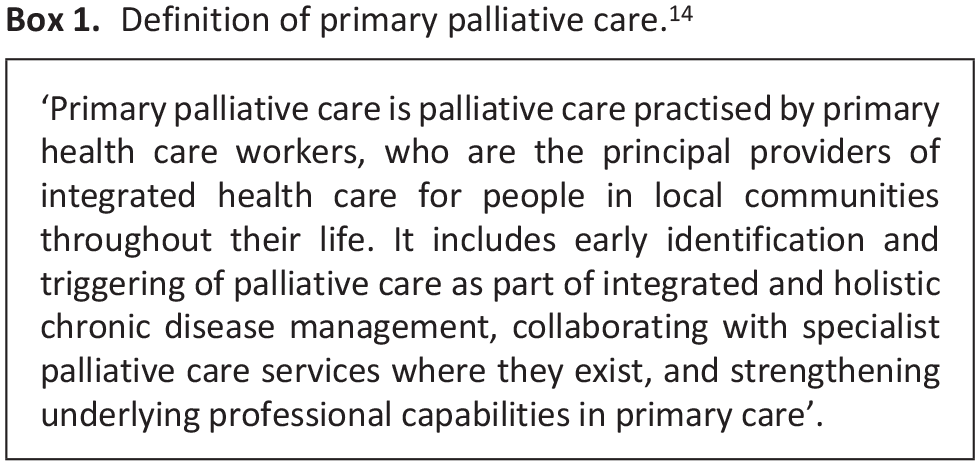
In 2019, Munday et al. published a definition stipulating that ‘primary palliative care is palliative care practised by primary health care workers’ (Box 1). 14 However, the COVID-19 pandemic eclipsed the article’s goal of stimulating discussion about the new definition.
Definition of primary palliative care. 14
Primary care and palliative care share similar strengths and attitudes
Primary care’s disciplinary strengths explain its potential to support high-quality universal health coverage in general, and palliative care in particular. Starfield et al. highlighted these in the 1990s, 15 arguing that primary care was the best approach for effective comprehensive healthcare. Primary care is the first point of contact for access to healthcare in the community; it ideally provides continuity of care and supports good communication and community involvement, thereby enabling recipients to define their own health care needs. The vibrant growth of general or family practice, which began in the 1960s as a distinctly modern, evidence-based, multidisciplinary practice, particularly in Western Europe, Australia, New Zealand and Canada, effectively demonstrates these primary care strengths. 16
The parallel development of palliative care, which also began in the 1960s with the hospice movement, and family practice as a specialism and academic discipline, is striking. 17 Both stress the importance of a multidisciplinary, holistic, person-centred approach involving patient and family, excellent communication skills and continuity of care. The underlying philosophy, values and practices of palliative care and effective family practice markedly overlap. 18
Palliative care needs are best identified and coordinated through primary care
Primary care, usually the first point of contact with a health system, ideally provides continuity of care and is best placed for early diagnosis and management of patients with potential palliative care needs associated with any illness – for example, through tools including SPICT, 19 GSF-PIG 20 or NECPAL. 21 Primary care can deliver palliative care through integrated chronic disease management combining treatment of underlying illness alongside health promotion, disease prevention, rehabilitation and palliative care. Primary care delivers care at, or close to, home: the local health centre or clinic, the family home, senior living and nursing facility, homeless shelter or detention facility. As primary care extends from cradle to grave, primary palliative care covers all ages from neonates to elders.
Many family practitioners have paid special attention to caring for people with palliative care needs, developing systems to ensure they receive excellent care and follow-up throughout the course of their illness. These systems were combined within initiatives such as Gold Standards Framework in the UK, which gave primary care teams a range of interventions to provide effective primary palliative care. 22 These frameworks built on the strengths of primary care and family practice and could be adapted to the delivery context within which local primary care functioned. They were ‘bottom-up’ – emerging from primary care, whilst learning from specialist palliative care. As they matured, the principles of primary palliative care were applied ‘upstream’ into earlier management of cancer and a multidisciplinary approach to all chronic life-limiting illnesses such as COPD, heart failure and neurological illness. These systems have been reviewed and distilled in the European Association of Palliative Care Toolkit to enable family practitioners and primary care teams to develop locally appropriate approaches. 23
Global primary care variation requires primary palliative care flexibility
The 77th World Health Assembly in May 2024 paid special attention to primary care delivery and universal health coverage. The global COVID-19 pandemic reinforced the understanding that universal health coverage can only be delivered through primary care. 24 WHO has recently launched a number of documents and frameworks 25 to enable countries to develop appropriate and high-quality primary care to make universal health coverage a reality.
Different models of primary care are emerging throughout the world. All should espouse the principles of primary care: first point of contact, comprehensiveness, continuity and communication. Compassion, now recognised and promoted by WHO Secretary General as an essential component of effective universal health coverage, should be added as another principle. 26 The palliative care community should partner with WHO, primary health care experts and health ministries to ensure that effective models of primary palliative care are co-created within wider primary care.
High-quality, effective primary care is quite distinct from the stereotype of generalists as ‘jacks of all trades’ and poor, albeit necessary, substitutes for specialist colleagues. The evidence shows that good primary care for people with chronic illness provides superior outcomes to specialist management alone. 15 However, more research and training are needed to ensure the quality of emergent primary care. Primary care professionals often report lack of knowledge, skills and attitudes for effective chronic disease management. 2
Primary palliative care can help with this. The person-centred approach, communication, continuity and problem-solving skills provided through palliative care education add value to health systems, especially to integrated chronic disease management. 27 Global palliative care advocacy should emphasise palliative care’s intrinsic value for health system strengthening. Not only does palliative care deliver whole-person care for patients experiencing serious health-related suffering, it is an asset for health systems, a catalyst that can make high-quality universal health coverage delivered through primary care a reality. 14
Numerous primary palliative care models are evolving worldwide, reflecting differing primary healthcare services and the availability of palliative care specialists. Peeler et al. in this special issue very helpfully describe five models in low-and-middle-income countries, including specialist outreach and care in secondary and even tertiary care. They define such models as ‘primary palliative care’ as some patients get first contact care in those settings. 28 However, this begs the question – ‘are such models of primary care sustainable for universal health coverage’? As low and middle income countries and regions develop primary health care systems and services in line with the WHO 14th Global Programme of Work, it is vital that palliative care be included within the new models of primary care. Pereira et al. 29 helpfully also in this special issue lay out some models developed in higher income settings which might also help to inform development in low and middle income countries. Clarity of terminology is needed to correctly identify studies in reviews, so that policymakers and clinicians can more easily grasp the way forward. The document ‘Integrating palliative care and symptom relief into primary health care: a WHO guide for planners, implementers and managers’ is helpful in this respect. 30
Call for action
We reaffirm the definition in Box 1 as most fit for purpose for the development of primary palliative care to achieve universal health coverage. Since 2022 the European Association for Palliative Care Primary Care Reference Group has hosted a number of webinars to analyse different models of palliative care in the community in Europe, Asia Pacific, Africa and the Americas. The group brought together leading practitioners and researchers at the European Association for Palliative Care Congress in Rotterdam in 2023 to work towards a consensus definition that clarifies the scope of primary palliative care. We hope this edition of Palliative Medicine will make a valuable contribution to that process to clarify the way forward to achieve ‘palliative care for all’.
Footnotes
Acknowledgements
We would like to thank all members of the European Association for Palliative Care reference group in primary care who have contributed to the development of this work to refocus on the value and definition of ‘primary palliative care’. We also thank Katherine Pettus for her comments and suggestions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.