
Abstract
Background:
Variation in the provision of care and outcomes in the last months of life by cancer and non-cancer conditions is poorly understood.
Aims:
(1) To describe patient conditions, symptom burden, practical problems, service use and dissatisfaction with end-of-life care for older adults based on the cause of death. (2) To explore factors related to these variables focussing on the causes of death.
Design:
Secondary analysis of pooled data using cross-sectional mortality follow-back surveys from three studies: QUALYCARE; OPTCare Elderly; and International Access, Right, and Empowerment 1.
Setting/participants:
Data reported by bereaved relatives of people aged ⩾75 years who died of cancer, cardiovascular disease, respiratory disease, dementia or neurological disease.
Results:
The pooled dataset contained 885 responses. Overall, service use and circumstances surrounding death differed significantly across causes of death. Bereaved relatives reported symptom severity from moderate to overwhelming in over 30% of cases for all causes of death. Across all causes of death, 28%–38% of bereaved relatives reported some level of dissatisfaction with care. Patients with cardiovascular disease and dementia experienced lower symptom burden and dissatisfaction than those with cancer. The absence of a reliable key health professional was consistently associated with higher symptom burden (p = 0.002), practical problems (p = 0.001) and dissatisfaction with care (p = 0.001).
Conclusions:
We showed different trajectories towards death depending on cause. Improving symptom burden and satisfaction in patients at the end-of-life is challenging, and the presence of a reliable key health professional may be helpful.
Although there have been many mortalities follow-back surveys of patients with cancer, few comparative analyses with non-cancer patients have been conducted.
This study demonstrates that service use and circumstances surrounding death differed significantly across different causes of death.
After adjustment, patients with cardiovascular disease and dementia experienced lower symptom burden and dissatisfaction than those with cancer.
The absence of a reliable key health professional was consistently associated with higher symptom burden, practical problems and dissatisfaction with care.
Patient trajectories at the end-of-life differ across diseases. Palliative care should be tailored and adapted to the course of these trajectories.
The presence of a key health professional might reduce symptom burden and practical problems and improve dissatisfaction with care across diseases.
Background
Rapid population ageing is a global phenomenon. The highest projected rise in serious health related suffering is among people aged 70 years (183% increase between 2016 and 2026). 1 Ageing and the consequently rising mortality rates have increased demand for palliative care, both for cancer- and non-cancer diseases.2,3
The World Health Organization proposed that palliative care is an essential component of comprehensive health services for non-communicable diseases, with an emphasis on primary healthcare and community- or home-based care. 4 With population ageing, non-cancer conditions are projected to have the greatest proportional rise in serious health related suffering, with dementia the highest (six million people, 264% increase between 2016 and 2060). 1 However, the provision of palliative care for patients with non-cancer conditions remains insufficient, globally representing 69% of people in need of palliative care. 5 Furthermore, given the different trajectories of diseases6,7 and changing palliative care practices, national end-of-life care strategies require understanding on symptom distress and system based solutions to address inequities in providing palliative care. Consequently, it is vital to understand comprehensively the experiences and quality of care among patients with cancer and non-cancer diseases near end-of-life. This understanding should be evaluated within the context of each healthcare system, considering the implications of rapid population ageing. These considerations are crucial to design effective end-of-life care policies and optimise service provision, especially in settings with limited resources.
Donabedian proposed a framework for evaluating care quality, which comprises structure, process and outcome of care. 8 Palliative care includes the places of care delivery for general and specialised services and the provision of multidisciplinary care. The outcome of care encompasses symptom burden, quality of life and patients’ and families’ satisfaction with care.9,10 However, measuring the process and outcomes of palliative care at the end-of-life using existing databases or prospective data collection is often challenging because of the vulnerability of these patients and the complexity of the palliative care delivery system. Therefore, retrospective approaches, such as mortality follow-back surveys, are commonly used. 11
Most mortality follow-back surveys focus on cancer or a single non-cancer disease, with few including several non-cancer diseases.12,13 Additionally, these surveys consider both younger and older adults. Furthermore, even when several non-cancer diseases are included, analyses are limited to comparisons between patients with and without cancer, owing to small sample sizes.14 –16 Diff-erences between causes of death have not been examined to the best of our knowledge. Therefore, in this secondary analysis, we pooled data from three studies using mortality follow-back surveys17 –20
Our aims were to: (1) gain a thorough understanding of service use, patient circumstances, symptom burden, practical problems and dissatisfaction with end-of-life care for older adults by cause of death and (2) explore factors related to symptom burden, practical problems and dissatisfaction, focussing on the causes of death.
Methods
Study design
We conducted a secondary analysis of pooled data using cross-sectional mortality follow-back surveys from three studies: QUALYCARE 17 ; OPTCare Elderly 18 ; and the Inter-national Access, Right and Empowerment 1 (IARE 1).19,20
Settings
The three studies focussed on deaths in community settings. In the QUALYCare and OPTCare elderly studies stratifying the sampling to include all deaths at home, in-patient hospice and care homes. And in QUALYCare a random sample of deaths in acute hospital. IARE1 included all places of death following discharge from acute hospital. The QUALYCARE and IARE 1, studies were conducted in London, UK providing diverse ethnic and socio-economic samples, while the OPTCare Elderly study was conducted in two diverse geographical areas in Southern England encompassing rural/urban and city.
Study population and sampling
We analysed data from bereaved relatives of individuals aged ⩾75 years whose cause of death, as identified from their death certificate, was cancer (C00–C97), cardiovascular disease (I00–I99), respiratory disease (J00–J99), dementia (F00–F03) or neurological disease (G00–G99).
The participants of the QUALYCARE survey were bereaved relatives of individuals aged ⩾18 years who died of cancer within 1 year from March 2009 to March 2010. Postal questionnaires were sent between January and July 2010, 4–10 months after the death occurred. We extracted and analysed data from those whose deceased relatives had been ⩾75 years. Four primary care trusts were selected specifically for their differing rates of cancer home deaths and levels of deprivation within London. Subsequently, the sample was stratified by primary care trust and place of death.
The participants of the OPTCare Elderly study were bereaved relatives of individuals aged ⩾75 years who died of cancer or other causes. Postal questionnaires were sent in October 2012, 4–10 months after the death occurred. The study sites included both urban and rural areas, which allowed for a comparison between different geographical areas. The Office for National Statistics randomly selected bereaved relatives of individuals who died at the designated study sites within 6-months. Additionally, death registration data were used to identify the sampling frame.
The participants of the IARE 1 study were bereaved relatives of individuals aged ⩾65 years who died of cancer or other causes and had accessed specialist palliative care services before their death. The study recruited patients who received palliative care at two hospitals in London from 2012 to 2013. We extracted and analysed data from those whose deceased relatives had been ⩾75 years. A mortality follow-back survey was conducted 4–10 months after the death occurred.
Other information about the study population and sampling procedure is described in Supplemental Table 1. More detailed information about the three original studies is provided elsewhere.17,19 –21
Approval and ethical considerations
All studies were approved by the National Health Sys-tem Research Ethics Committee, London, Dulwich (ref: QUALYCARE 09/H0808/85, OPTCare Elderly 12/LO/1367, IARE 1 12/LO/0044) and King’s College London.
Measurements
The underlying causes of death were identified based on the Office for National Statistics registry for the QUALYCARE and OPTCare Elderly studies and based on hospital records for the IARE 1 study.
The primary outcomes were symptoms and practical problems in the last week, and dissatisfaction with care. However, because the aim of this study was a thorough understanding of the circumstances of patients near death, we examined the following variables using a modified version of a questionnaire developed by Ann Cartwright, widely used to measure patients’ experiences in their last year of life from the perspective of bereaved family members.22 –25
Symptoms and practical problems in the last week before death
The Palliative Outcome Scale (POS) 26 and POS for symptoms (POS-S) 27 were used to measure patient symptom burden and practical problems experienced in the last week before death. The POS and POS-S comprise 10 and 8 items, respectively. Bereaved relatives rated the items from 0 to 4, considering time-wasted appointments (0–3) and practical matters (0–3) from their perspective. Additionally, the 18 items were classified into two components: symptoms and practical problems. 28
Dissatisfaction with care
The respondents were asked whether (Yes or No) there were any aspects of care they felt unhappy with during the last 3 months of their relative’s life.
Service use in the last 3 months
The Client Receipt Service Inventory was used to obtain information on healthcare services received by individuals in their last 3 months of life.29,30 Hospice and palliative care teams, Macmillan nurses, Marie Curie nurses and other specialist nurses were considered as specialised palliative care services. Respondents were asked about the presence of a key professional: ‘Do you feel he/she had a key contact person (health professional) he/she could rely on to get things done?’
Circumstances surrounding death
Information was ob-tained on death-related circumstances, such as place of death, patient’s awareness of their prognosis in the last week and unconsciousness or coma in the last week.
Participant characteristics
The collected data included the patient’s gender, age, religion, ethnicity, marital status, financial status and length of illness and the bereaved relative’s gender, age, relationship, religion and ethnicity.
Analysis
First, we analysed data on the participants’ characteristics, service use in the last 3 months and death-related circumstances. Using Fisher’s exact test, we compared the data by cause of death. Regarding symptoms and practical problems, we provided summary statistics of each item, as well as subtotal and total scores. We compared these scores with the causes of death using an analysis of variance. Additionally, we calculated the percentage of items with scores ⩾2 from 0 to 4, indicating a moderate, severe or overwhelming problem for each POS and POS-S item.
The factors related to symptoms, practical problems and dissatisfaction with care were explored using bivariate and multivariate analyses to identify independently associated variables. To assess symptoms and practical problems, we set the subtotal scores as dependent variables, performed a t-test or analysis of variance for bivariate analyses and conducted multiple linear regression analyses. Regarding dissatisfaction, we set dissatisfaction (i.e. unhappy experience) as the dependent variable, used Fisher’s exact test for the bivariate analyses of cases without symptoms and practical problems and conducted multiple logistic regression analyses. The model selection strategy for all multiple regression analyses was as follows: (1) bivariate analyses assessed the presence or absence of a statistical association between the causes of death and all other variables; (2) after checking any statistical interactions to determine that the association did not differ by cause of death, the causes of death and all associated variables in the bivariate analyses were included in the first model; (3) statistical variable selection was performed using a backward procedure, with the compulsory inclusion of causes of death; and (4) sensitivity analyses were conducted according to processing method of missing values. All analyses were two-sided; statistical significance and threshold for variable selection were set at p < 0.05. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
The pooled datasets contained 885 responses from the three studies (QUALYCARE, n = 328; OPTCare Elderly, n = 406 and IARE 1, n = 151). The causes of death were cancer (n = 516), cardiovascular disease (n = 172), respiratory disease (n = 104), dementia (n = 51) and neurological disease (n = 42). The study details and causes of death are presented in Supplemental Table 1.
Participant characteristics and circumstances surrounding death
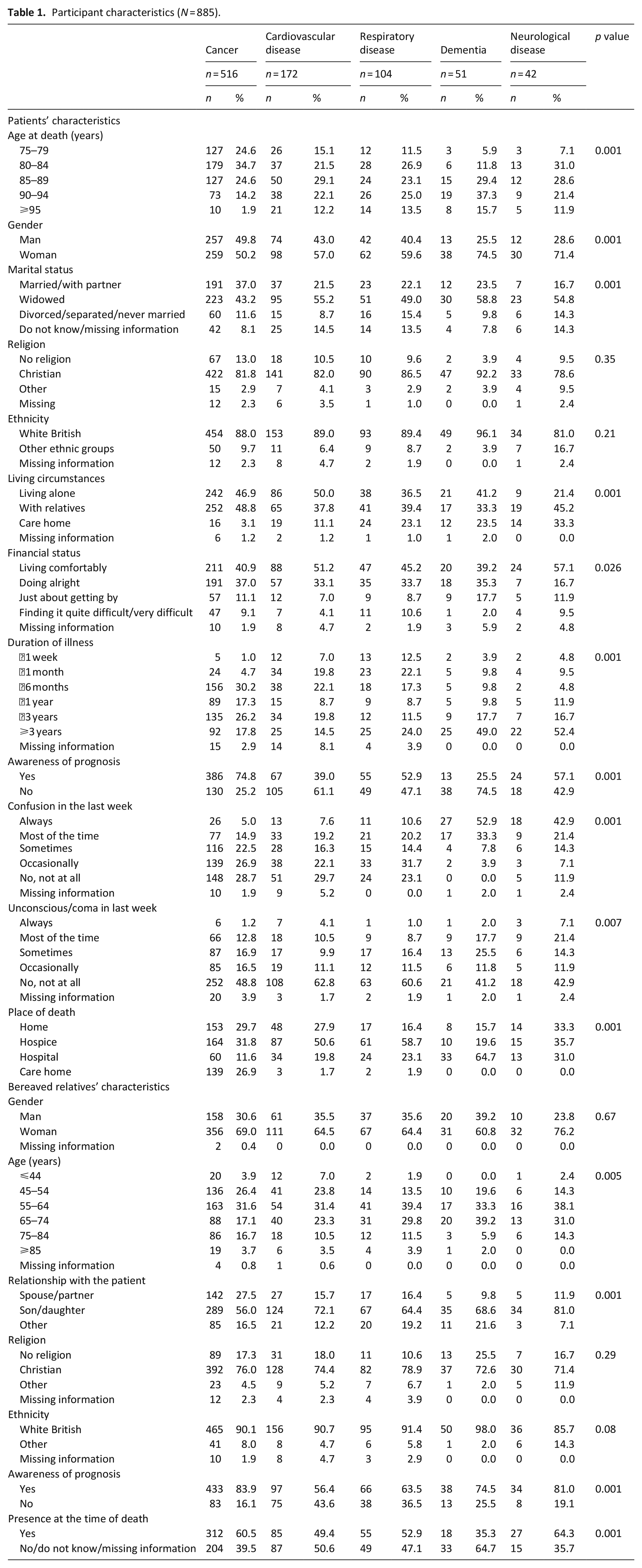
Table 1 presents the participants’ characteristics and circumstances surrounding death. Almost all variables except for religion, ethnicity and the bereaved relative’s gender significantly differed across the causes of death.
Participant characteristics (N = 885).
Symptom burden, practical problems in the last week of life and dissatisfaction
Table 2 shows the symptom burden and practical problems in the last week. Regarding symptom burden, bereaved relatives reported a ⩾30% experience of symptoms with a score ⩾2 for most symptoms. However, symptom severity did not significantly differ across causes of death except for weakness, shortness of breath, nausea and vomiting.
Symptom burden, practical problems and dissatisfaction.
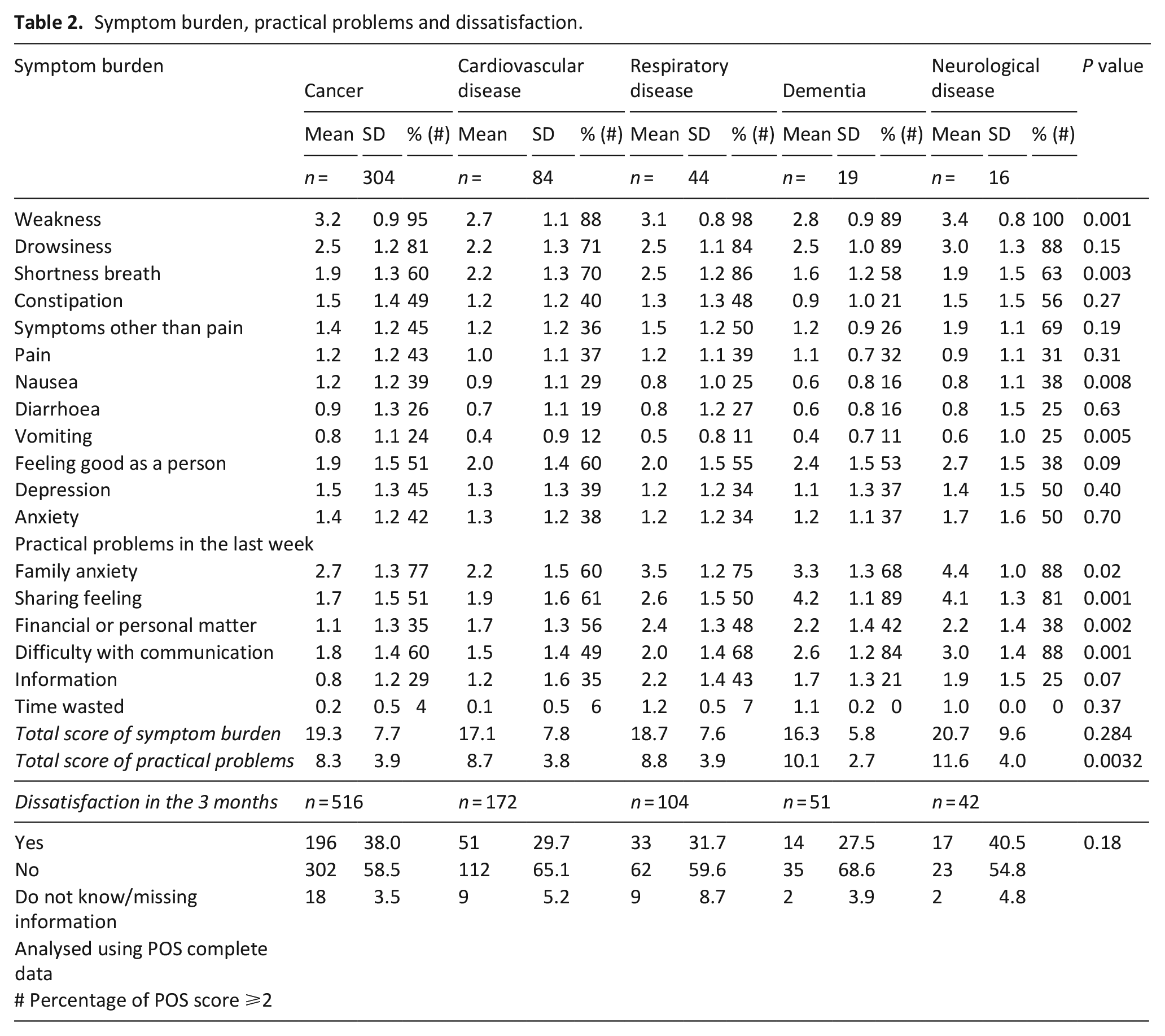
Overall, 60%–88% of bereaved relatives reported family anxiety (score: ⩾2), with family anxiety, sharing feelings, practical matters and difficulty in communication significantly differing across causes of death. Additionally, the total score for practical problems was different across causes of death (p = 0.003), but not the total score for symptom burden (p = 0.28).
Across causes of death, 28%–38% of bereaved relatives reported some dissatisfaction with care (p = 0.18).
Service use in the last 3 months of life
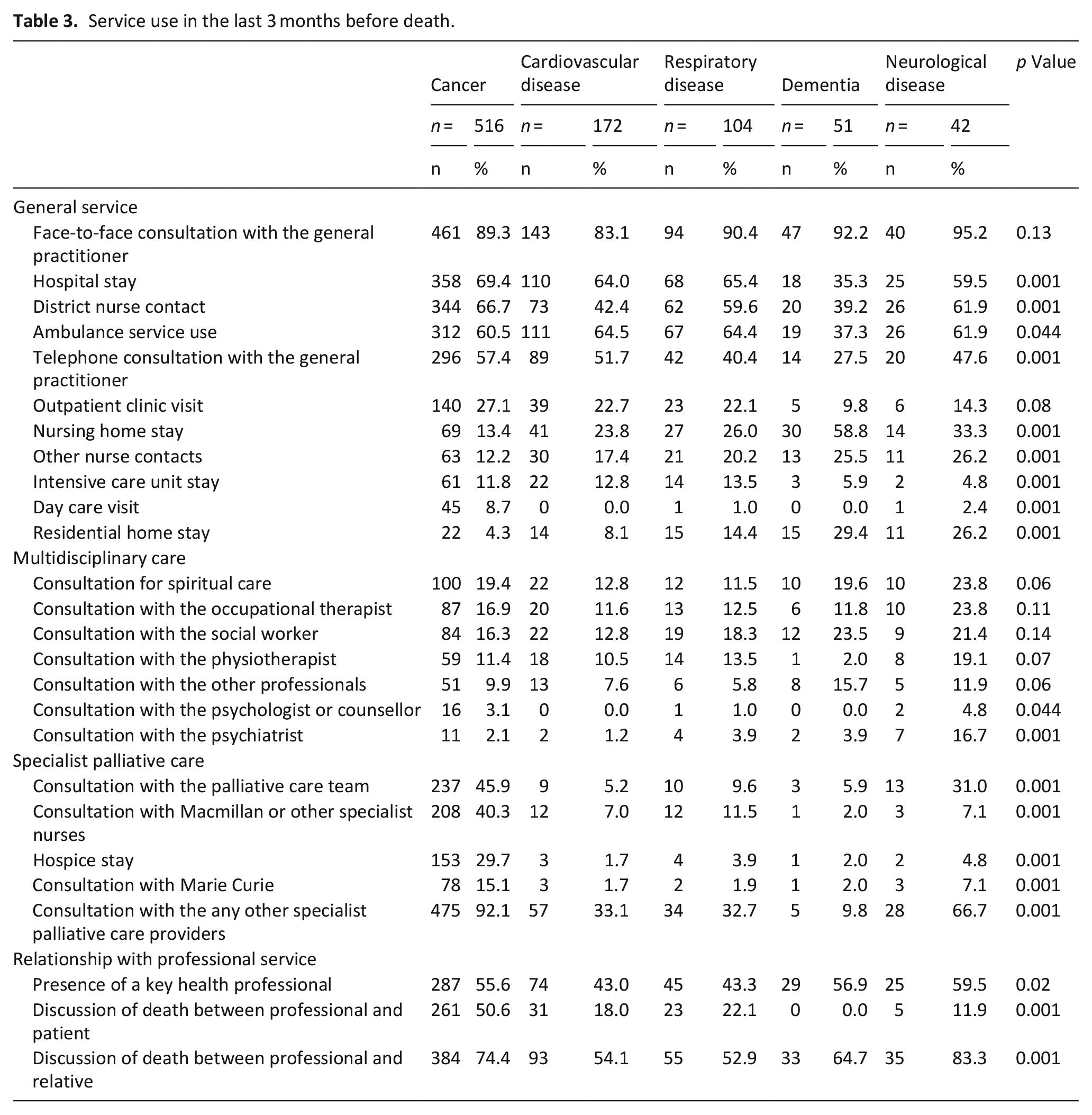
Service use in the last 3 months of life is shown in Table 3. Across all causes of death, most patients had consulted with a general practitioner face-to-face. Other commonly used services such as hospital units, district/community nurses and ambulance services had a utilisation rate of >50%, except in dementia cases. Multidisciplinary care services such as spiritual care, occupational therapists and social workers were used by <20% of patients across all causes of death. Although 92% and 67% of individuals who died of cancer and neurological disease, respectively, used any one of the specialised care services, the proportion was lower (p = 0.001) for those who died of cardiovascular disease (33%), respiratory disease (33%) and dementia (10%). Across causes of death, 43%–60% of bereaved relatives reported access to reliable key health professionals (p = 0.02). Furthermore, the types of key health professionals based on multiple answers included general practitioners (26%), nurses (19%), non-general practitioner physicians (5%) and other professionals (14%; data not shown).
Service use in the last 3 months before death.
Factors related to symptom burden, practical problems in the last week and dissatisfaction with care in the last 3 months before death
The results of the bivariate analyses are shown in Supplemental Table 2. No statistically significant interactions were found between the causes of death and any significant variables in the bivariate analyses.
Table 4 summarises the results of the final regression model of factors related to symptom burden, practical problems in the last week and dissatisfaction with care in the last 3 months. After adjusting for participant characteristics and circumstances surrounding death, individuals who died of cardiovascular disease and dementia had lower symptom burden (p = 0.007 and 0.001, respectively) and lower dissatisfaction (p = 0.04 and 0.02, respectively) than those who died of cancer. Additionally, the absence of a reliable key health professional was consistently associated with higher symptom burden and practical problems and dissatisfaction with care. Moreover, a female relative, a relative who was the patient’s child and higher practical problems were associated with dissatisfaction (p = 0.01, 0.008 and 0.001, respectively). These results were similar for different processing methods for missing data (Supplemental Table 3).
Factors related to symptom burden and practical problems in last week and dissatisfaction with care in the last 3 months.
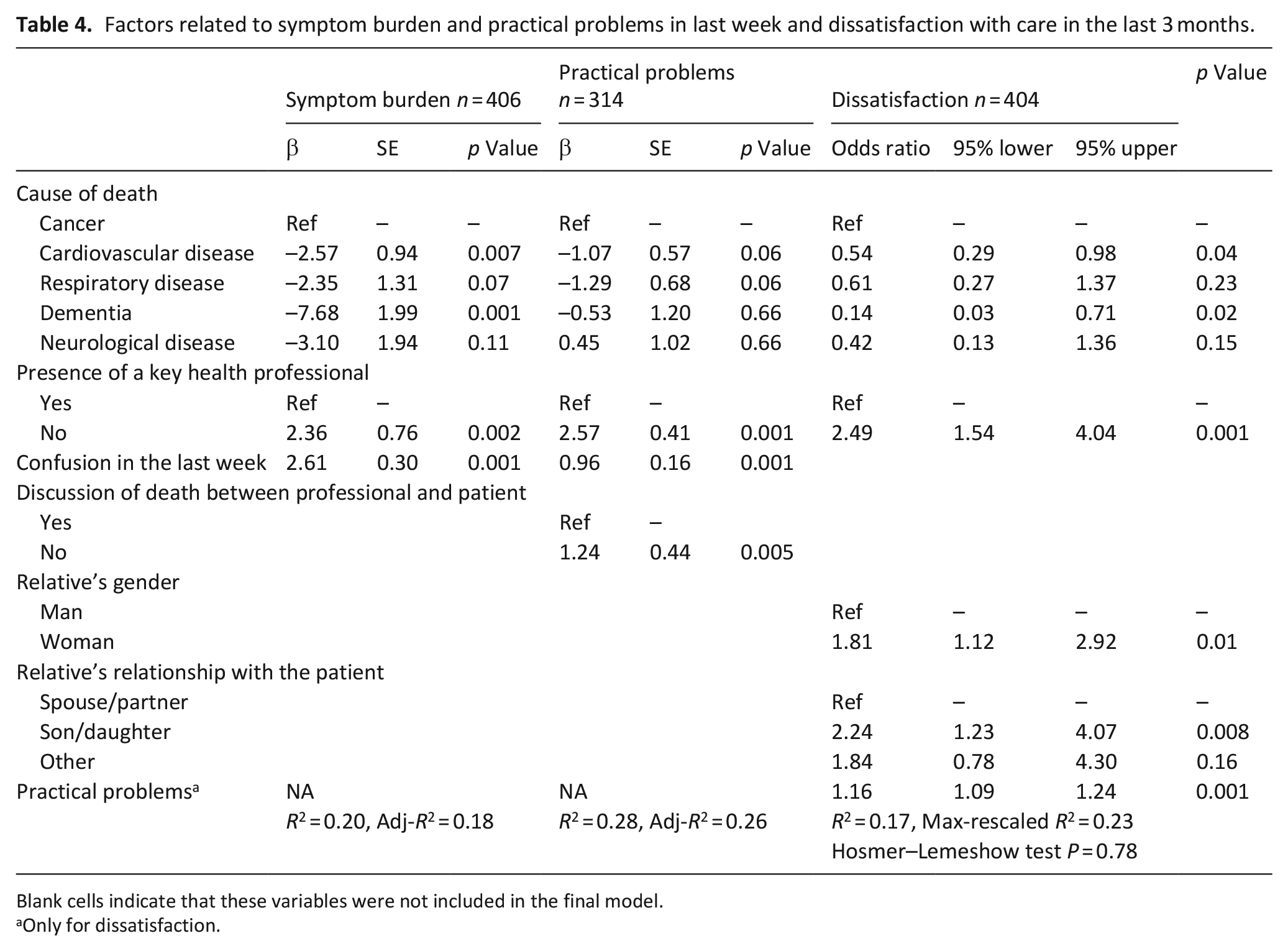
Blank cells indicate that these variables were not included in the final model.
Only for dissatisfaction.
Discussion
Main findings
First, service use and circumstances surrounding death differed significantly across causes of death. Second, after adjusting for participant characteristics and circumstances surrounding death, symptom burden and dissatisfaction with care were significantly lower in individuals who died of cardiovascular disease or dementia than in those who died of cancer. Third, after adjustment, the absence of a reliable key health professional was associated with higher symptom burden, practical problems and dissatisfaction with care.
What this study adds?
Differences in service use and circumstances surrounding death indicated different trajectories towards death according to cause. Although specialised palliative care is common among patients with advanced cancer, its provision for non-cancer conditions is highly variable.31,32 This trend is similar to that of the US data, although specialised palliative care use is more common in the US than in the UK. 13 Additionally, general practitioners, hospital units, district/community nurses and ambulance services were common end-of-life providers, except among patients with dementia. Therefore, the provision of palliative care by these general service providers is important to enhance the quality of care for all patients at the end-of-life. Particularly, the involvement of general practitioners in generalist palliative care is crucial, considering that the majority of our sample consulted with a general practitioner in the last 3 months of life. 33
Bereaved relatives reported that ⩾30% of patients across causes of death experienced symptoms with a score ⩾2, which indicates a moderate to overwhelming problem. However, the relief of physical and psychological symptoms remained inadequate for patients with cancer and other diseases. Additionally, 28%–38% of bereaved relatives reported dissatisfaction with the care services offered. This level seems high and similar to that in the US, 13 where the satisfaction levels of individuals with various diseases do not significantly differ. After adjustment, individuals who died of cardiovascular disease and dementia had lower symptom burden and lower dissatisfaction than those who died of cancer, which may be because cardiovascular disease and dementia are more common among older patients. This may reflect the older age of patients and fewer symptoms in these diseases compared with the aggressive disease of cancer.
Furthermore, the absence of a reliable key health professional was associated with higher symptom burden, practical problems and dissatisfaction with care. Additionally, the effects of key health professionals did not differ by death cause or type of professional (data not shown). Importantly, this finding was consistent across causes of death. Therefore, key healthcare professionals may contribute to better care coordination and timely referrals to appropriate services for all patients.18,21 This implies that finding a reliable key healthcare professional and coordinated care is important at the end-of-life.
Strength and limitations of the study
The strength of this study is the pooling of data from three studies with a large sample to obtain comparative and disease-specific results on palliative care for cancer and non-cancer diseases. The data were collected over 10 years ago. However, this was a novel data set that used validated measures to capture outcome and service data at the individual level, with pooled data enabling examination by respective cause of death from a diverse sample. The findings inform priority areas for policy of addressing inequities in palliative care provision, notably the importance of key health professionals to reduce symptom burden and concerns across diseases.
However, some limitations cannot be ignored. First, the distribution of service use and other variables may not be representative of the national population owing to the different sampling frameworks employed. Particularly, specialised palliative care use and home deaths may have been overestimated, although they were relatively low, except for cancer. Additionally, the surveys were conducted in London and the Southeast region; therefore, extrapolating the findings to national data for the UK and other countries requires care. Second, although we used pooled datasets from three mortality follow-back surveys, the sample sizes for dementia and neurological diseases were small, and the statistical power of the analysis for these diseases would have been low. Third, recall bias and unreliability due to proxy reporting are inherent limitations of the mortality follow-back survey34,35; family members might have overestimated symptom burden and underestimated prognosis awareness.34,35 Moreover, some symptoms such as nausea might be unreliable for people with dementia. Fourth, the causes of death identified by the registry might not reflect the true causes of death for older non-cancer patients, owing to the complexity and multimorbidity often observed in this population. Furthermore, the IARE1 study used cause of death data from hospital records, while others used the Office for National Statistics registry, potentially resulting in information bias. Fifth, we asked whether there were any aspects of care bereaved relatives felt unhappy about in the last 3 months of the patient’s life. This presented challenges in specifically identifying the services that bereaved relatives expressed dissatisfaction with. Sixth, the statistical power of statistical interaction is generally low and statistical model selection might produce biased results. However, bivariate analysis and sensitivity analysis support our analysis.
Conclusions
Differences in service use and circumstances surrounding death indicate distinct trajectories towards death, depending on the cause. Improving symptom burden and satisfaction in patients and their relatives is challenging, and the presence of a reliable key health professional may be helpful for all, regardless of diagnosis.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163241246049 – Supplemental material for Symptom burden, service use and care dissatisfaction among older adults with cancer, cardiovascular disease, respiratory disease, dementia and neurological disease during the last 3 months before death: A pooled analysis of mortality follow-back surveys
Supplemental material, sj-pdf-1-pmj-10.1177_02692163241246049 for Symptom burden, service use and care dissatisfaction among older adults with cancer, cardiovascular disease, respiratory disease, dementia and neurological disease during the last 3 months before death: A pooled analysis of mortality follow-back surveys by Mitsunori Miyashita, Catherine J Evans, Deokee Yi, Barbara Gomes and Wei Gao in Palliative Medicine
Footnotes
Acknowledgements
We thank Professor Irene J Higginson, Cicely Saunders Institute of Palliative Care, Policy and Rehabilitation, Florence Nightingale Faculty of Nursing, Midwifery & Palliative Care, King’s College London, for support throughout this study. This study was supported by three research groups, and we thank the partici-pants in all three original studies. We thank Cicely Saunders International for funding the QUALYCARE study and contributors Natalia Calanzani, Jonathan Koffman, Paul McCrone, Sue Hall, Julia Riley, Meena Valambhia, Elizabeth Davies, Peter Madden, Mike Richards, Tessa Ing, Myer Glickman, Peter Davies, Stephen Rowlands, Justine Pooley, Nada Lemic, Sarah Price, Clare Henderson, Jacqui Lindo, Ursula Daee, Kerry Hylands, Nell Dunn, Kirstie Newson, Brenda Ferns, Anita Patel, Colin Murray Parkes, Joana Cadima, Massimo Costantini, Claudia Bausewein, Despina Anagnostou, Emma Murphy, Fliss Murtagh, Lucy Selman, Marjolein Gysels, Sian Best, Thomas Osborne, Vera Sarmento, Gunn Grande and Christine Ingleton. For the OPTCare Elderly study, we thank Myfanwy Morgan, Paul McCrone, Juliet Wright, Sue Hall, Emma Gordon, Fiona Lindsay, Carla Bruni, Shamim Taherzadeh, Richard Harding, Katherine E. Sleeman, Matthew Maddocks, Helen Harris, Anita Wright, Sue Guerrier, John Barry, Lesley Talmey, Colin Vincent, Mike Bojczuk, Jack Hazelgrove, Anna E. Bone, Rowena Vohora, Katie Stone, Mark Philips, Nina Walters, Kate Porter, Claire Cox and Mendwas Dzingina. Additionally, we thank Emma Bennett, Francesca Cooper, Barbara Daveson, Susanne de Wolf-Linder, Mendwas Dzingina, Clare Ellis-Smith, Taja Ferguson, Lesley Henson, Bridget Johnston, Paramjote Kaler, Pauline Kane, Lara Klass, Peter Lawlor, Paul McCrone, Regina McQuillan, Diane Meier, Susan Molony, Sean Morrison, Fliss Murtagh, Charles Normand, Caty Pannell, Steve Pantilat, Karen Ryan, Lucy Selman, Melinda Smith, Katy Tobin, Rowena Vohora and Deokhee Yi for the IARE 1 study. Finally, we extend our gratitude to Anna Bone of King’s College London, UK.
Supplemental material
Supplemental material for this article is available online.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the original studies comprised: OPTCare Elderly was funded by the National Institute for Health and Care Research (NIHR) Research for Patient Benefit Programme (Project PB-PG-1111–26071), and Health Education England (HEE)/NIHR Clinical Lectureship held by CJE (CAT CL 10-003); QUALYCARE received funding from Cicely Saunders International (CSI, UK charity); IARE 1 received funding from Cicely Saunders International (CSI, UK charity) and The Atlantic Philanthropies. The funding organizations had no role in the design, methods, analysis, preparation, or approval of the paper. The views expressed in this publication are those of the authors and not necessarily those of the NHS, NIHR, HEE or the Department of Health and Social Care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.