
Abstract
Background:
Advance care planning has been defined in an international consensus paper, supported by the European Association for Palliative Care. There are concerns that this definition may not apply to dementia. Moreover, it is not informed by input from people with dementia.
Aim:
To gather the perspective of the European Working Group of People with Dementia and their supporters on how advance care planning is defined and develop recommendations for changes to the definition.
Design:
An in-depth qualitative study was conducted, analysing online focus groups and interviews using thematic analysis.
Setting/participants:
We included 12 people with dementia and 9 supporters.
Results:
Participants suggested several changes to the current advance care planning definition: mentioning people with decreasing decisional capacity; better reflecting the role of family and/or trust-based relationships; reducing focus on end-of-life/medical decisions; strengthening focus on social aspects of care. Elements of the current definition that participants suggested keeping and highlighting include the framing of advance care planning as a continuous process, that is also optional; mention of communication next to documentation of decisions; and the importance of proxy decision makers. Based on this input, we developed three overarching and 16 specific recommendations for a modified definition of advance care planning that is inclusive of people with dementia.
Conclusions:
The perspectives of the European Working Group of People with Dementia and their supporters highlighted the need for a person-centred and dementia-inclusive advance care planning definition. We provide tangible recommendations for future adaptations of the definition that reflect these perspectives.
Advance care planning has been defined in an international consensus paper.
Advance care planning is particularly relevant for people with dementia, however, the definition of advance care planning may not be applicable to them.
People with the dementia were not involved in the development of current definitions of advance care planning.
The existing definition of advance care planning should be adapted to be more inclusive and applicable to people with dementia.
A more person-centred approach to advance care planning should be highlighted in the definition, which would emphasise discussions of social aspects of care and what matters most in the future.
The definition of advance care planning should better reflect the role of families or trust-based relationships.
Using a dementia-inclusive and person-centred definition of advance care planning can lead to interventions and policies that better reflect the needs of people with dementia and their supporters.
Introduction
Advance care planning has been advocated as a process that enables individuals to make plans about their future health care. 1 Over the past decades, advance care planning has been increasingly studied and has been defined in multiple ways.1–3 Originally seen as a documentation-focused process encouraging the completion of advance directive documents, the concept of advance care planning has shifted towards a broader concept of communication about several aspects of future care and treatment planning.3,4 Advocates of advance care planning argue that it should be common practice in planning the treatment of patients with all life-limiting illnesses. 5
In a recent international consensus paper, supported by the European Association for Palliative Care, advance care planning was defined as a process that:
‘enables individuals who have decisional capacity to identify their values, to reflect upon the meanings and consequences of serious illness scenarios, to define goals and preferences for future medical treatment and care, and to discuss these with family and health-care providers. advance care planning addresses individuals’ concerns across the physical, psychological, social, and spiritual domains. It encourages individuals to identify a personal representative and to record and regularly review any preferences, so that their preferences can be taken into account should they, at some point, be unable to make their own decisions’.
2
Recommendations for the application of this definition were developed, which deal with aspects such as the readiness of the individual to engage in advance care planning, as well as the content of advance care planning and how to target it depending on the condition. 2
There are several shortcomings in this definition. It requires people to have decisional capacity to engage in the process and can thus not be applied to people who lack decisional capacity 6 such as many people with dementia. The process of advance care planning is however particularly relevant for people with dementia and people close to them, as many people with dementia gradually lose their ability to make informed decisions, verbal communication becomes more difficult and people close to them play an increasing important role in decision-making.6,7 Although loss of capacity may occur in many different conditions, especially when nearing end of life, people with dementia are particularly affected due to the extended duration over which capacity can gradually decrease. 8 Several advance care planning interventions for people with dementia have been developed to tackle this, however there is no consensus about what advance care planning for people with dementia should include. 9
The inclusion of people with dementia and people close to them in research is essential to ensure that their needs and perspectives are fully understood and considered in the development of interventions. 10 The definition of advance care planning has been developed mainly based on professional expert recommendations and a small number of patients’ relatives with experience of terminal illness and acting as patient representatives. However, people with dementia and their family members were excluded as experts by experience. 2 People with dementia have not been part of the process of describing advance care planning for their group, and more generally, their voices are missing in the scientific developments in this field. Therefore, this research addresses the gap in patient involvement in the work leading to the definition of advance care planning. We aimed to (1) obtain the perspective of a multinational group of people with dementia on how advance care planning is defined, and (2) develop recommendations for changes to the definition of advance care planning based on these perspectives.
Methods
Study design
We conducted an in-depth qualitative study (focus groups and interviews) with a multinational group of people with dementia and people close to them. We used thematic analysis to explore their perspectives on the definition of advance care planning and to formulate recommendations for the definition of advance care planning.
Participants
Our participants were being a member of the European Working Group of People with Dementia and their supporters. Members of this group are usually accompanied by a relative, friend or a member of staff from their national Alzheimer Association, and these individuals are referred to as supporters. 11 This European group is coordinated by Alzheimer Europe and composed of people with dementia who are nominated by their national associations. 11 The working language of the group is English. In the case that members are not English-speaking, their supporter can act as interpreter.
All members of the group and their supporters were invited to participate in the study by email. AD and DG, who are familiar with the working group, were the main point of contact with the participants. The main inclusion criteria were (1) being a member of the European Working Group of People with Dementia or being the chosen supporter of one of the members, and (2) participants’ expressed willingness and consent to engage in discussions related to advance care planning. All members of the European Working Group of People with Dementia are in the mild to moderate stages of dementia, and thus should have the capacity to understand what is being asked of them. Participants could have any age, dementia type, length of illness and comorbidity or could be from any country.
Our study population was limited to the size of the working group. However, we aimed to include this specific group to ensure diversity of perspectives. The European Working Group of People with Dementia is a multinational group with members from varying backgrounds, experiences, and cultural contexts. Furthermore, we used a combination of data collection strategies, that is, focus groups and follow-up interviews, which allowed us to engage in detailed discussions with all participants. This depth of engagement allowed us to explore the topic thoroughly, ensuring that we obtained rich and nuanced insights.
Data collection
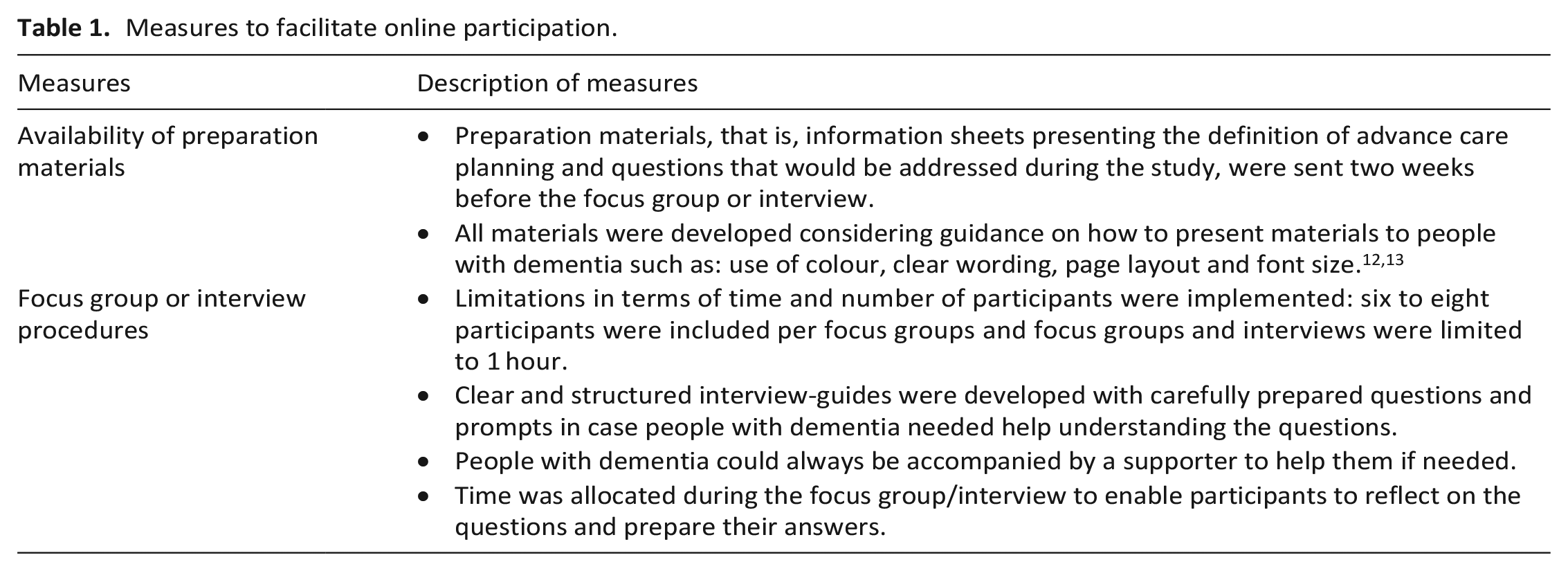
We conducted online focus groups and interviews in English. To support people with dementia during the process and facilitate online participation, we used adapted materials and procedures, which are summarised in Table 1. Supporters played a double role in the process, as they were respondents in both focus groups and interviews, but could also be asked to provide assistance to people with dementia if needed or act as interpreter for not English-speaking participants.
Measures to facilitate online participation.
Focus groups
We conducted three online focus groups in November 2020, which were led by two moderators (LP and LVdB) and an observer (FM), who assisted with technical problems, moderated the chat and took notes. AD and DG were also present as they are familiar with the members of group. We used a semi-structured topic guide and PowerPoint slides to give an overview of the extended definition of advance care planning and present the questions to participants. Specifically, the researchers presented a deconstruction of the definition into the ‘what’, ‘why’, ‘who’ and ‘when’ of advance care planning (Figure 1), which was used as visual prompt. Participants were asked to reflect on the definition of advance care planning and to what extent it reflected their experiences. They shared their ideas one after the other to ensure fair participation and then discussed their ideas as a group.
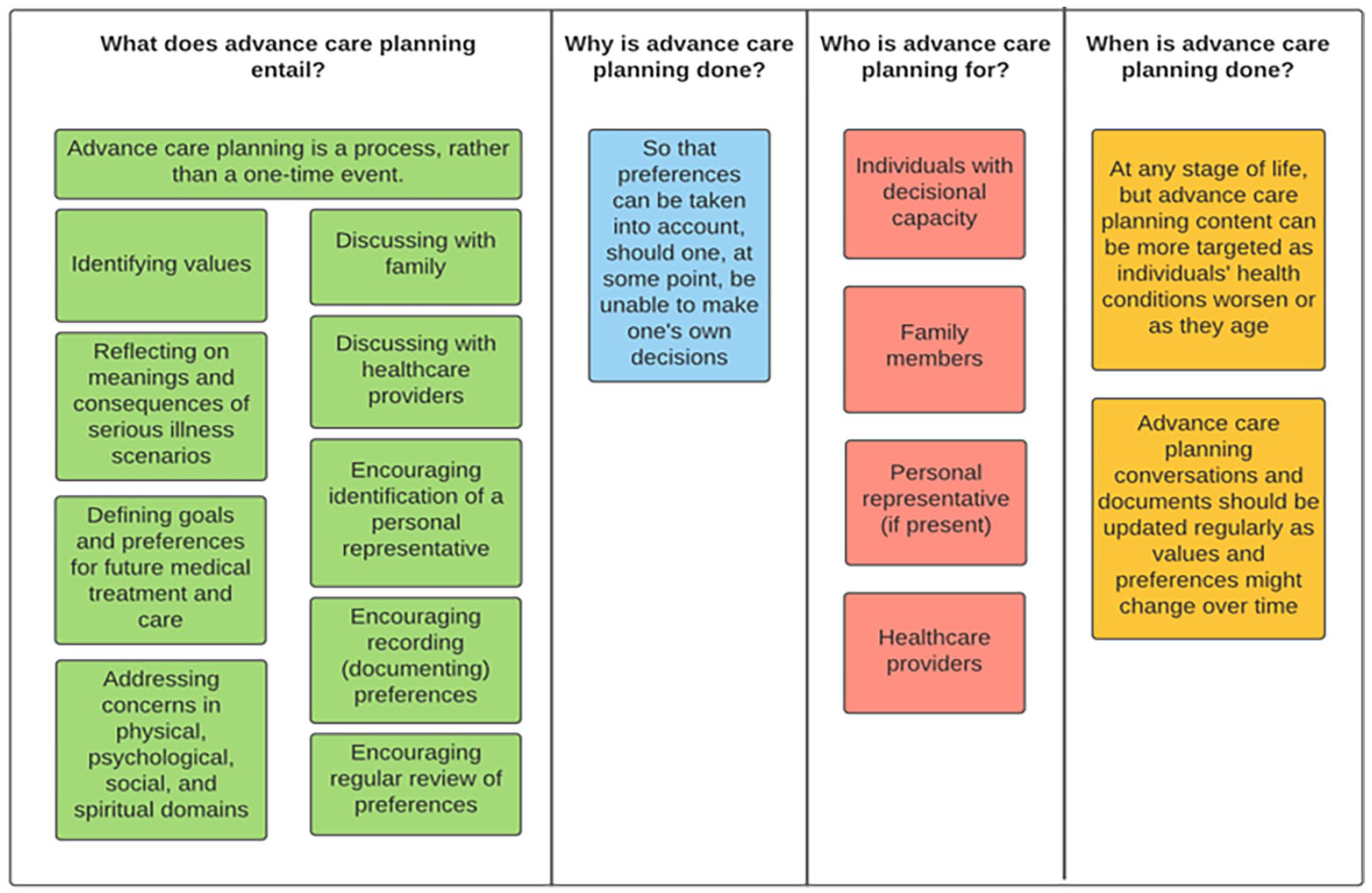
Deconstruction of the extended definition of advance care planning.
Follow-up interviews
At the end of each focus group, participants were invited to follow-up interviews. The semi-structured interview schedule was guided by the findings of the focus groups. Interviews commenced with a reminder of the definition of advance care planning using Figure 1. The interviewer (FM) invited participants to elaborate on the main three themes that emerged from the focus groups. Interviews were conducted on Zoom between June and July 2021.
Analysis
Audio-recorded focus groups and interviews were transcribed verbatim. De-identified transcripts were coded using thematic analysis, following steps recommended by Braun and Clarke, 14 and using NVivo12. Two researchers (FM and CD) first read each transcript thoroughly. The main constructs derived from the existing definition of advance care planning were used as a framework. Next to this, we also used open codes that did not fall within these pre-existing concepts but were reflective of the content resulting from the focus groups and interviews. Both researchers individually coded the data. First, they assigned pre-defined codes and then iteratively assigned preliminary open codes.14,15 This underwent several rounds of refinement, which included iterative processes of shifting between transcripts and codes while continuously revising the codes. Between these iterations, the researchers met to explore different opinions on the data and finally to agree on a list of codes. Subsequently, our attention turned towards comprehensively interpreting the content as a whole. FM organised the codes into candidate themes and subthemes, reinspected the codes within each theme and identified recurring topics within the content. Finally, FM named and presented the themes and sub-themes. Following the analysis of the focus groups and interviews, the authors developed a list of recommendations based on these findings.
Ethics
Participants received an information letter and link to an online informed consent form. This process required some adaptations in terms of formulation to make the materials as accessible as possible. Additionally, participants were asked to give verbal consent to recording. The study received ethical approval from the Ethics Review Board of the Brussels University Hospital of the Vrije Universiteit Brussel (BUN: 1432020000199).
Results
The focus groups involved 21 participants, of which 12 were people with dementia and 9 supporters. Participants were from Ireland, United Kingdom, Germany, Slovenia, Iceland, Sweden, Austria, Belgium and Portugal. Interviews were conducted with nine people with dementia and seven supporters. Four people with dementia needed their supporter to act as interpreter. Supporters were partners (n = 4), children (n = 2), siblings (n = 1) or friends/members of a national dementia association (n = 3). We identified two themes and nine sub-themes (Figure 2).
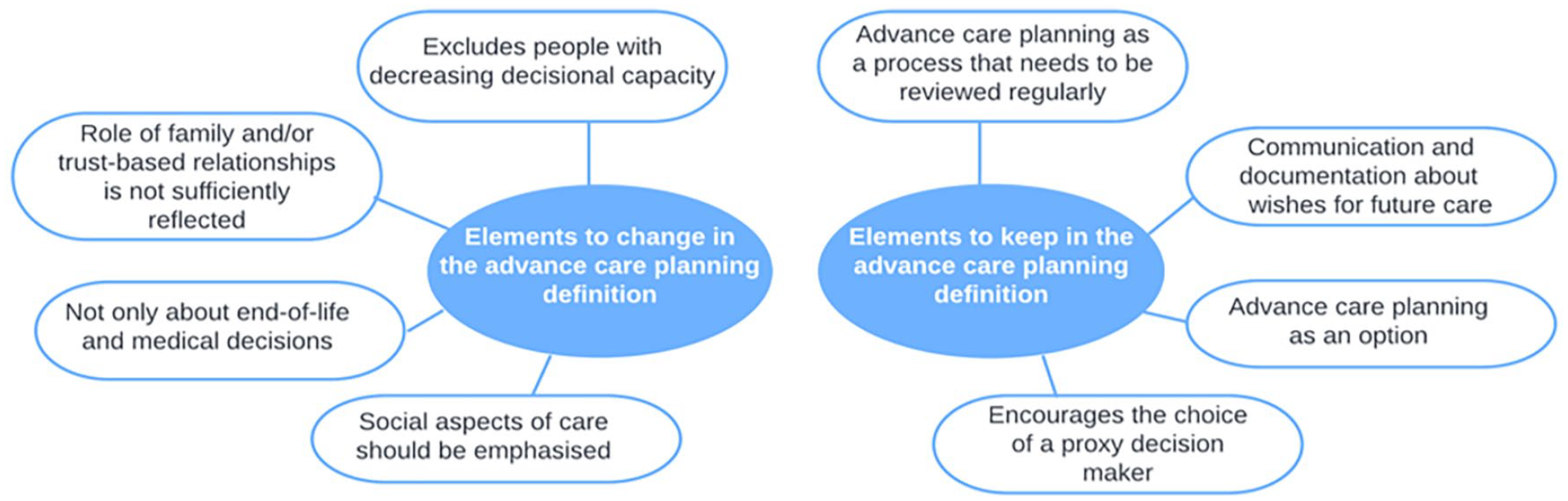
Thematic map of the findings.
Elements to change in the advance care planning definition
Several aspects of the definition of advance care planning were highlighted as either missing or not emphasised enough. Participants reflected on elements which they thought should be improved in the definition to better reflect their experiences with advance care planning. This related to who is involved in advance care planning and what advance care planning entails.
Excludes people with decreasing decisional capacity
Participants highlighted that the focus of the current advance care planning definition on individuals with decisional capacity excluded many people with dementia from the process of advance care planning. They noted that decisional capacity is a gradual process and may be dependent on the situation or the person with whom advance care planning conversations are taking place.
‘I have a friend who lost his communication skills. He stopped talking quite early on in his dementia. And everybody assumed that because he couldn’t talk that he didn’t have capacity. And he still did. He could still read, he could listen, he could think. So you know, you have to take it all into consideration’.
(Person with dementia #1)
Furthermore, participants discussed strategies to support decisional capacity and involve the person with dementia in advance care planning as long as possible. Decisional capacity was seen as knowing what one wants, knowing what one does or as understanding questions and consequences of different decisions. Some participants also reflected on the way that decisional capacity is assessed in practice, and advocated for a triangular process to this assessment, involving the person with dementia, a family caregiver and a health professional.
Role of family and/or trust-based relationships is not sufficiently reflected
Participants reflected on the fact that the definition did not show the importance of families or other trust-based relationships (e.g. friend, neighbour, family of choice) in advance care planning. Many noted that family dynamics may differ among people and that the decision of whom to involve in advance care planning concerned trust-based relationships in general rather than family ties only. Participants found that families or people whom they trust should be involved in advance care planning because of their extensive personal knowledge of the person with dementia.
‘So it’s really important as the disease progresses that the loved ones are involved in their advance care decisions. Because they know their loved ones, they know the person, they know their personality and they know what that person would prefer’.
(Supporter #5)
Participants highlighted that for the sake of clarity, it is of utmost importance that families and people whom they trust are up-to-date concerning the wishes of the person with dementia. Additionally, they also commented on the importance of discussing the potential role of family and people they trust in advance care planning, both in the present and as the condition evolves in the future. People with dementia particularly noted that considering the importance of families or trust-based relationships in the process, support systems are needed to conduct advance care planning conversations and to deal with any potential negative consequences of these conversations, such as emotional burden.
Advance care planning is not only about end-of-life and medical decisions
The members of the group and their supporters perceived an emphasis on medical decisions and end-of-life care within the definition of advance care planning. Although the definition mentions other aspects within advance care planning such as psychological, social or spiritual needs, they noted a stronger emphasis on preferences for medical treatments. Participants also found that emphasis on medical decisions was reflected in their experiences in practice, where the focus was solely on medical treatment decisions and end-of-life care preferences. They emphasised the importance of considering advance care planning as a process that enables them to identify what matters most to them in the future, including but not limited to medical decisions and end-of-life care preferences.
‘Well, I think when we talk about advance care planning there’s a concentration on how we are going to leave this world. Advance care planning to me is how we’re going to live in the world as well’.
(Person with dementia #3)
Social aspects of care should be emphasised
Participants found that social aspects of care were of utmost importance within advance care planning, and should be emphasised in the definition. They described social aspects of care as: (1) future daily activities, (2) future psychosocial interventions, (3) place of residence, (4) place of death.
‘When I think about social aspects of care, it could be for example that: my husband is a very social person and he wants to be among people even if he can’t contribute in the way somebody without dementia can. You know those types of social aspects. To do all the things he always loved doing. If he was still able to walk, he’s always gone walking. It could be seen in a care setting that he is wandering. No he’s not wandering, he’s always gone out for walks’.
(Supporter #2)
Participants also reflected on the fact that social aspects of care can be difficult to discuss, particularly with health professionals. They noted issues with recording their preferences for these aspects of care, as most advance directives may not provide this option.
Elements to keep in the advance care planning definition
Several aspects of the definition of advance care planning were positively perceived by the participants. Overall, they found that the definition was comprehensive in terms of what the process involved and when it should be done.
Advance care planning as a process that needs to be reviewed regularly
Participants supported the notion that advance care planning should be a process, rather than a one-off event. All emphasised the need to give people with dementia the opportunity to regularly review their advance care planning decisions.
‘It says advance care planning is a process rather than a one-time event. And I agree with that it’s extremely important that it is a process and that it is revised regularly’.
(Person with dementia #8)
Some people with dementia also mentioned that in many cases people may not know that they can change their wishes if they want to, and that more effort to raise awareness about the process itself should be made.
Encourages the choice of a proxy decision maker
All participants agreed with the part of the definition dealing with the choice of a proxy decision maker. They mentioned that the proxy decision maker should be a person they trust, and someone who understands the wishes of the person with dementia. Furthermore, they reflected on the difficult role of the proxy decision maker, which includes advocating for the person with dementia and advocating for his/her wishes, as well as coordinating care with families and health professionals according to what is considered in the best interest of the person with dementia.
‘ The role of the proxy decision maker is to implement as far as possible the wishes of the person who has made that decision. And it has to be as far as possible. Because you can’t always do it. But at least you have an idea, some parameters to go by. You know what they want and you do your best to do that’.
(Supporter #7)
Communication and documentation about wishes for future care
Participants highlighted the importance of: (1) communicating about advance care planning with both families or people they trust, and health professionals; and (2) documenting preferences in advance directives. They reflected that communicating about and documenting advance care planning decisions could give a sense of control to the person with dementia, less burden for the family and people they trust in moments when decisions have to be made, and finally a sense of relief for both parties.
‘[In the context of moving to a care facility] That’s going to be a tough day for me and that’s going to be a tough day for them. But they will know, if it’s done early enough, that this is what I’ve asked for and this is what I want’.
(Person with dementia #1)
Advance care planning as an option
Both people with dementia and supporters highlighted that advance care planning should remain optional, and that if the person with dementia did not wish to discuss it, they should be free not to. Furthermore, many noted that the advance care planning process should be conducted at the pace of the person with dementia, and that they should be able to stop whenever they wish to. Some also mentioned that ideally, advance care planning should be conducted as early as possible after, if not before, diagnosis.
‘As family, you can encourage, gently encourage and use some gentle persuasion to say it is for your best to discuss it. But some people with dementia are hard nuts to crack and so stubborn. So if they won’t, you cannot force the’.
(Supporter #3)
Recommendations
Table 2 summarises recommendations for the definition of advance care planning derived from the input of the European Working Group of People with Dementia and their supporters. They range from the need for a dementia-inclusive definition, elements from the current definition that should remain, to elements that should be adapted or stressed.
Recommendations for the advance care planning definition, comparison to the current extended definition, example quotes.

Discussion
Main findings
Our study reports the perspectives of the European Working Group of People with Dementia and their supporters on the extended definition of advance care planning and makes recommendations based on their input. They expressed support for several aspects of the current definition that they considered essential, such as advance care planning being a process that is reviewed regularly and that is optional. Participants also agreed that advance care planning should encourage communication and documentation of decisions about future care, and should not be limited to the completion of advance directives. The European Working Group of People with Dementia also made important and tangible suggestions for changes to the current definition of advance care planning. They highlighted the need for the definition to include people with declining decisional capacity, better reflect the role of families or trust-based relationships, and better address social aspects of care.
A central point raised by the group is the need for a dementia-inclusive definition of advance care planning. Dementia introduces specific challenges compared to other serious illnesses, such as the gradual – although fluctuating – loss of decisional capacity. However, advance care planning should be applicable to all regardless of their condition. Our participants highlighted that the main aspect excluding them in the current definition was the clear focus on people with decisional capacity only. At the same time, they emphasised that there is no need for a separate definition for people with dementia. Instead, the existing definition of advance care planning should be adapted to be more inclusive of people with dementia and applicable to people with or without conditions that influence cognitive capacities. This is consistent with the work of Alzheimer Europe calling for inclusive research and the ethical involvement of people with dementia. 16 Other approaches have also advocated for dementia-inclusive research, such as dementia-friendly communities, which aim to ensure that people with dementia are entitled to equal opportunities in all aspects of life as well as equal access to care. 17
Participants strongly emphasised the role of families and trust-based relationships in the advance care planning process, which they found to be under-addressed in the definition of advance care planning. Families or others one trusts are generally considered to have personal knowledge of the person with dementia, and they are often an important point of contact in communication and decision-making in the later stages of dementia. Our study suggests that the involvement of others should be flexible in terms of timing and extent of involvement. The importance of families and trust-based relationships contrasts with traditional conceptualisations of advance care planning or decision-making that are framed in highly individualised terms. 18 Our findings highlight the need for a more relational approach to advance care planning, but also emphasises that the person with dementia should be able to choose how others get involved.
Another clear point made by our participants was the importance of social aspects of care within advance care planning. Participants felt that the definition of advance care planning currently focuses too much on medical care, while it should include broader conversations on what matters to people in the future, on social care, and on future meaningful daily life activities. These perspectives reflect current debates about conceptualisations of advance care planning. In past conceptualisations of advance care planning, significant emphasis was placed on the written preparation process, which involves creating documents to specify end-of-life treatment preferences, as well as designating a proxy decision maker. 19 Under the impulse of public health approaches to care in the last phase of life, advance care planning has evolved to a broader concept of an iterative communication process between the person concerned, people close to him/her and health professionals, about future care and what matters most.3,4,19,20 However, our participants highlighted that this evolution is not reflected enough in the definition nor in practice. Our study provides further support for discussion about what matters most for the future as part of advance care planning. It calls for a more person-centred care planning approach to advance care planning and for the corresponding changes in its definition.
Strengths and limitations
This study filled an important gap in the involvement of people with dementia and their supporters in the work leading to the definition of advance care planning. This inclusive approach helps to ensure that the perspectives of people with dementia and their supporters are considered in the definition of advance care planning. Our study enriches the palliative care practice by shedding light on the specific needs and perspectives of people with dementia and their supporters in the context of defining advance care planning. We advocate for a more inclusive, holistic and person-centred approach that is sensitive to the unique challenges presented by dementia and provide practical guidance for adapting the definition of advance care planning. The use of a dementia-inclusive definition of advance care planning in practice could lead to interventions and policies that better reflect the needs of people with dementia and their supporters and that are more acceptable to them. Our study is also a successful example of meaningful involvement of people with dementia as participants in qualitative research. It demonstrates that this group can meaningfully participate in online focus groups and interviews. Furthermore, while interviews and focus groups were not conducted in the mother tongue of most participants, our approach allowed individuals who were not fluent in English or who felt more confident expressing themselves in their native language to actively contribute. This was made possible through the presence of their supporters who were fluent in both the native language and English and acted as trusted interpreters. This approach enhanced the quality and richness of the data collected, ensuring that the perspectives of participants who might have otherwise been excluded due to language barriers were effectively captured in our study. This study also has several limitations. The participants are members of an European advisory group, and tend to be rather politically and socially active, which may not reflect the whole of the population of people with dementia. Our study should be replicated in other populations to increase the diversity of the perspectives presented in this paper. Furthermore, it should be noted that not all participants in the focus groups took part in the follow-up interviews, which also may limit the diversity of perspectives in our study.
Conclusion
The perspectives of the European Working Group of People with Dementia emerging from our study contribute to the understanding of advance care planning in dementia and highlight the need for a dementia-inclusive advance care planning definition. Participants stressed important aspects of the current definition of advance care planning such as the description of advance care planning as an optional process that focuses on both communication and documentation and that needs to be reviewed regularly. Our participants highlight several aspects of the definition of advance care planning which should be changed or addressed in more depth, among which are the issues of decisional capacity, family involvement and social aspects of care. We provide tangible recommendations for an adapted definition of advance care planning in line with the perspectives of people with dementia and their supporters.
Footnotes
Acknowledgements
We would like to thank the members of the European Working Group of People with Dementia and their supporters for participating in this study, and Jane Ruthven for English editing.
Author contributions
Study concept and design: Monnet, Pivodic, Diaz, Gove and Van den Block. Recruitment of respondents: Diaz and Gove. Acquisition of data: Monnet, Pivodic and Van den Block. Transcribing: Monnet. Analysis and interpretation of data: Monnet and Dupont. Drafting the manuscript: Monnet. Critical revision of the manuscript: Diaz, Gove, Dupont, Pivodic and Van den Block.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research presented in this paper was carried out as part of the DISTINCT project, a Marie Curie Innovative Training Network (ITN), H2020-MSCA-ITN-2018, under grant agreement number 813196. LP is a Senior Postdoctoral Fellow of the Research Foundation-Flanders (FWO). LVdB is Francqui Research Professor (2020–2023).