
Abstract
Background:
Several clinician training interventions have been developed in the past decade to address serious illness communication. While numerous studies report on clinician attitudes and confidence, little is reported on individual education modalities and their impact on actual behavior change and patient outcomes.
Aim:
To examine what is known about the education modalities used in serious illness communication training and their impact on clinician behaviors and patient outcomes.
Design:
A scoping review using the Joanna Briggs Methods Manual for Scoping Reviews was conducted to examine studies measuring clinician behaviors or patient outcomes.
Data sources:
Ovid MEDLINE and EMBASE databases were searched for English-language studies published between January 2011 and March 2023.
Results:
The search identified 1317 articles: 76 met inclusion criteria describing 64 unique interventions. Common education modalities used were: single workshop (n = 29), multiple workshops (n = 11), single workshop with coaching (n = 7), and multiple workshops with coaching (n = 5); though they were inconsistently structured. Studies reporting improved clinician skills tended to be in simulation settings with neither clinical practice nor patient outcomes explored. While some studies reported behavior changes or improved patient outcomes, they did not necessarily confirm improvements in clinician skills. As multiple modalities were commonly used and often embedded within quality improvement initiatives, the impact of individual modalities could not be determined.
Conclusion:
This scoping review of serious illness communication interventions found heterogeneity among education modalities used and limited evidence supporting their effectiveness in impacting patient-centered outcomes and long-term clinician skill acquisition. Well-defined educational modalities and consistent measures of behavior change and standard patient-centered outcomes are needed.
Keywords
Effective communication with patients about their serious illness improves patient outcomes, such as reduced anxiety and distress.
Multiple interventions have been developed to support clinical skills training around serious illness communication, but little research has categorized the educational modalities used.
Data has shown that serious illness communication training has a positive impact on provider satisfaction and confidence, but less is known about the impact on clinician behaviors and patient outcomes.
Of the 64 studies identified, the most common education modalities used were a single workshop (n = 29), multiple workshops (n = 11), single workshop with coaching (n = 7), and multiple workshops with coaching (n = 5).
Clinician behavior was measured by changes in documentation (n = 19), in simulated environments using role play or standardized patients (n = 30), but rarely in real clinical settings (n = 7).
Patient reported outcomes were only assessed in 27% of studies (n = 17/64), where illness understanding (n = 12) and perceived quality of communication (n = 11) were most commonly measured.
Implications for practice, theory, and policy
Future study designs of serious illness communication training should include consistent measures of skill acquisition, behaviors in clinical settings, and patient experiences.
More research is needed on optimal education modalities for clinical behavior change and improved patient-centered outcomes.
Background
Many seriously ill people and their families wish to have honest conversations about their illness, and when clinicians proceed with discussing serious illnesses, they are consistently found to be beneficial. 1 Multiple international studies and reports have identified effective communication as a key condition for a good death, including a systematic review and the recent Lancet commission about death.2,3
Yet clinicians across all specialties struggle to communicate with their patients the implications of serious illness. 4 To address this challenge, several communication skills interventions and associated training programs have been developed over the last decade and incorporate various education modalities. Examples include the Serious Illness Care Program (SICP), 5 VITALtalk, 6 Respecting Choices®, 7 and Comskil. 8
Many education interventions focused on serious illness communication have been evaluated in prior systematic reviews.9–13 There is strong evidence that serious illness communication training improves confidence with communication, attitudes about dying, and clinician intention to change practice,14–17 though there is a paucity of evidence on its impact on health care provider behavior change and patient outcomes. One exception is a meta-analysis on end-of-life communication skills training programs that examined the impact of 11 randomized trials on clinician behavior and patient-reported outcomes. 13 However, that meta-analysis did not describe or investigate the relationship between specific education modalities on outcomes, which could be informed by non-randomized studies.
A scoping review methodology was chosen to allow exploration of the extent, range and nature of education modalities used in serious illness communication training, and to identify gaps and targets for future research. 18 The objectives were to describe what is known about various modalities and their impact on clinician behavior and patient and family outcomes.
Methods
We conducted a scoping review using guidance from the Joanna Briggs Methods Manual for Scoping Reviews. 18 The PRISMA extension for scoping reviews was used to guide reporting. 19
Information sources and search
In order to balance feasibility with breadth and comprehensiveness of the scoping review process,18,20 we focused our search on two key biomedical databases, MEDLINE and Embase, from 2011 to March 2023 using a combination of MeSH terms and key words to identify studies conducted in a population of healthcare providers in the context of serious illness communication training: “palliative/terminal/hospice care,” “end of life,” “serious illness,” “health professionals,” “physicians,” “nurses,” “allied health care providers,” “education,” and “communication training.” The search was conducted with the assistance of a health sciences librarian. The search strategy was not limited by study design or clinical discipline. An additional search was conducted for communication training reviews to identify studies that we may have missed in our initial search. For the complete MEDLINE search strategy, see Supplemental Appendix 1. We hand searched the reference lists of all original study articles and reviews identified. The results of the literature search were imported into the bibliographic reference manager EndNote 20 21 and duplicate citations were removed. Citations were then imported into the Rayyan© 2022 22 collaborative review platform, which was used for screening by the review team.
Study selection
Eligibility criteria
Articles were included if they reported on education interventions for serious illness communication applied to a population of practicing healthcare providers or postgraduate learners (e.g. medical residents or fellows) in any healthcare setting or country, were written in English, and were published since 2011. We aimed to capture the latest developments in serious illness communication training to provide recommendations that are relevant to current research trends, outcome measures and new technologies. Therefore, we focused our search following the 2011 publication of “America’s Care of Serious Illness,” 23 which led to the development of several new serious illness communication training programs that are in common use.
As the focus of the review was to explore the impact of different education modalities on healthcare provider behavior change and/or patient-reported outcomes, the Levels 3 and 4 of the Kirkpatrick training evaluation model were used to inform article selection. 24 The Kirkpatrick model is a widely used four-level model that represents different types of evidence for intervention effectiveness. Level 1, Reaction, involves evaluating learners’ reaction to the training (e.g. satisfaction, attitudes). Level 2, Learning, assesses the extent to which learners acquire knowledge or skills. Levels 3 and 4, which are the focus of this review, involve evaluating learners’ application of what they learned (Behavior) and assessing the overall impact of the training (Results, e.g. impact of behavior change). All study designs, including qualitative or quantitative methods, where there was a description of clinician behavior or patient outcomes were eligible.
Articles were excluded if they only reported on healthcare provider self-perceived satisfaction, confidence, skills, or knowledge (including provider completed knowledge tests), which reflect Kirkpatrick levels 1 or 2. Articles were also excluded if the participants were exclusively undergraduate healthcare students (i.e. medical students, nursing students, and social work students). This decision was based on the understanding that students are in the early stages of their education and careers, and therefore, may have limited clinical exposure. With serious illness communication being an advanced competency, we felt that interventions aimed at undergraduate students were unlikely to result in changes in clinician behavior or patient outcomes.
Screening, data abstraction, and collation
Study selection was conducted as a two-stage screening process: title and abstract screen, followed by full-text screening. To ensure reliability, a calibration exercise with reviewers was conducted prior to title and abstract screening, and prior to screening full-text articles. Two different reviewers from the team independently reviewed titles and abstracts, and full-text articles for inclusion. Conflicts were resolved through discussion with the team or with a third independent reviewer.
The planned analysis was descriptive in nature. For each article that met inclusion criteria, relevant data were systematically extracted by two independent reviewers using a data charting form to facilitate mapping and analysis of the data. To ensure face validity, the review team independently tested the charting form, and their recommendations were incorporated into the final version. The tool was piloted and revised after 25% of articles were screened. Items were further clarified, and agreement was achieved through consensus. All publications from included studies were reviewed and data extracted if they described provider behavioral or patient outcomes.
During the first iteration of data collection, data were extracted on study aim, research design, context of the serious illness communication training, types of learners, education intervention structure and content, and outcomes (behavior change and results) by two independent authors. In cases where multiple articles reported on findings from the same study, studies were grouped together and treated as the unit of analysis. After initial review, the team met to discuss findings and key messages. We analyzed the data by identifying various groupings for educational interventions and achieved consensus through iterative discussion. Kirkpatrick level 3 behavior outcomes included documentation and skill acquisition that was observed in either simulated environments or real clinical settings, while Kirkpatrick level 4 outcomes encompassed patient-reported outcomes and patient healthcare utilization measures. Findings were further aggregated, analyzed, and synthesized by two independent authors (JM and ML) to refine themes, concepts, trends, gaps, and areas for future research. Our research team convened to discuss and consolidate final findings and consensus was reached. Consistent with the standard scoping review methodology, our aim was to map the evidence and therefore we did not assess the risk of bias of the studies included.
Results
Literature search
Our search strategy yielded 1317 unique articles, for which we screened titles and abstracts that resulted in 208 articles identified for full-text review. A total of 76 articles met our eligibility criteria, representing 64 different studies (see PRISMA flow chart Figure 1).
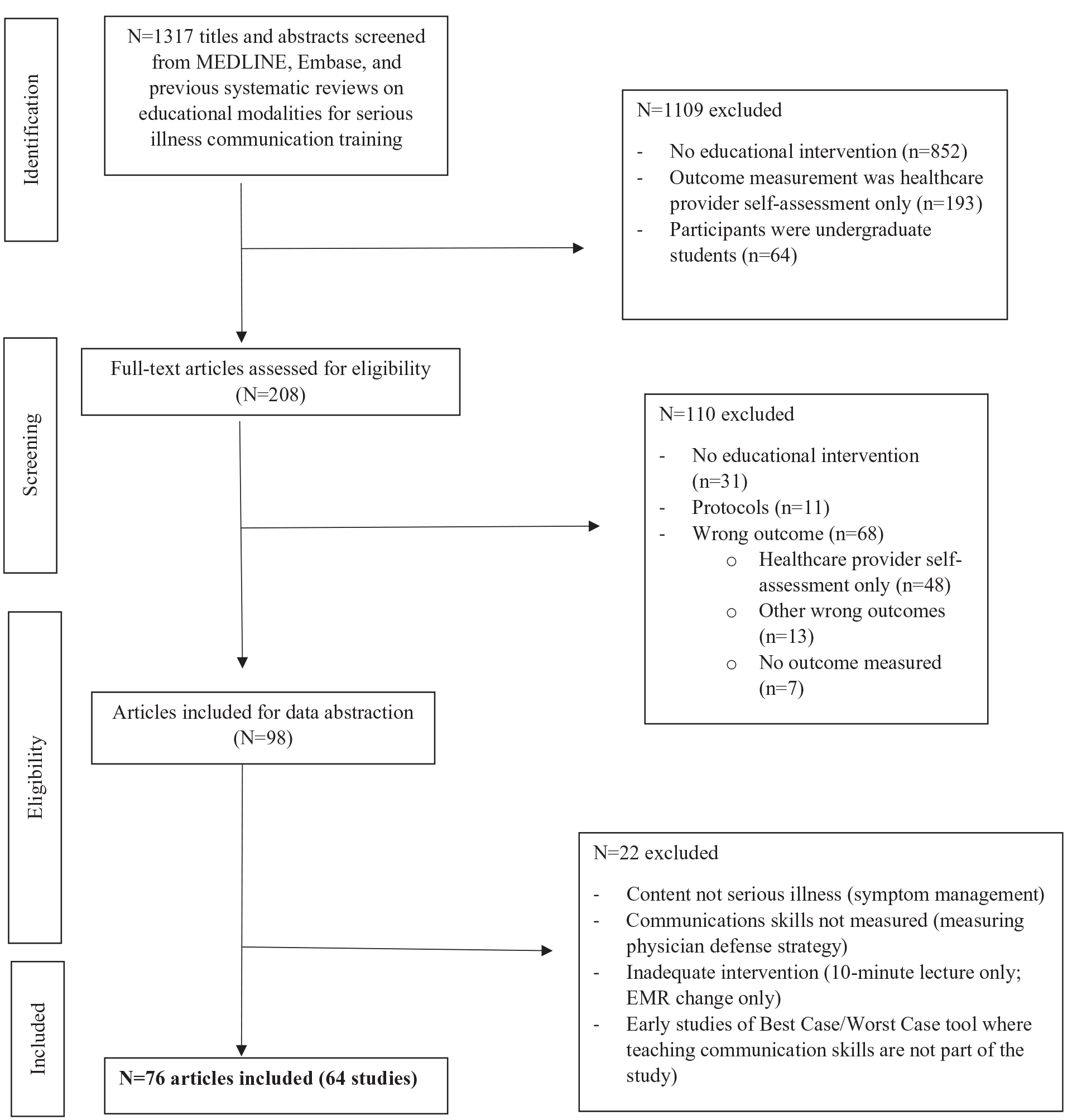
Study flow diagram of search strategy.
Characteristics of the included studies
Studies were conducted in North America (42), Europe (13), Asia (5), and Australia (4). There were 21 randomized trials, 2 non-randomized trials, 4 pilot/feasibility trials, and 37 pre-post intervention comparative studies. Twenty-one articles were published between 2011 and 2015, and 56 between 2016 and 2023. The interventions were delivered either as an embedded component of a larger quality improvement initiative or as a stand-alone experience. Only for the latter could the measured impact be directly attributed to the educational experience.
Interventions
The education interventions were delivered with four broad modalities: e-learning, single workshop, multiple workshops, and coaching (see Supplemental Appendix 2). The most common education modalities used were a single workshop (n = 29), multiple workshops (n = 11), single workshop with coaching (n = 7), and multiple workshops with coaching (n = 5). See Table 1. Nearly all interventions included a didactic component, and the majority (54/64) included some form of simulated experiential learning. Common approaches included role play using either participants or actors portraying standardized patients.
Education modalities used for serious illness communication training.
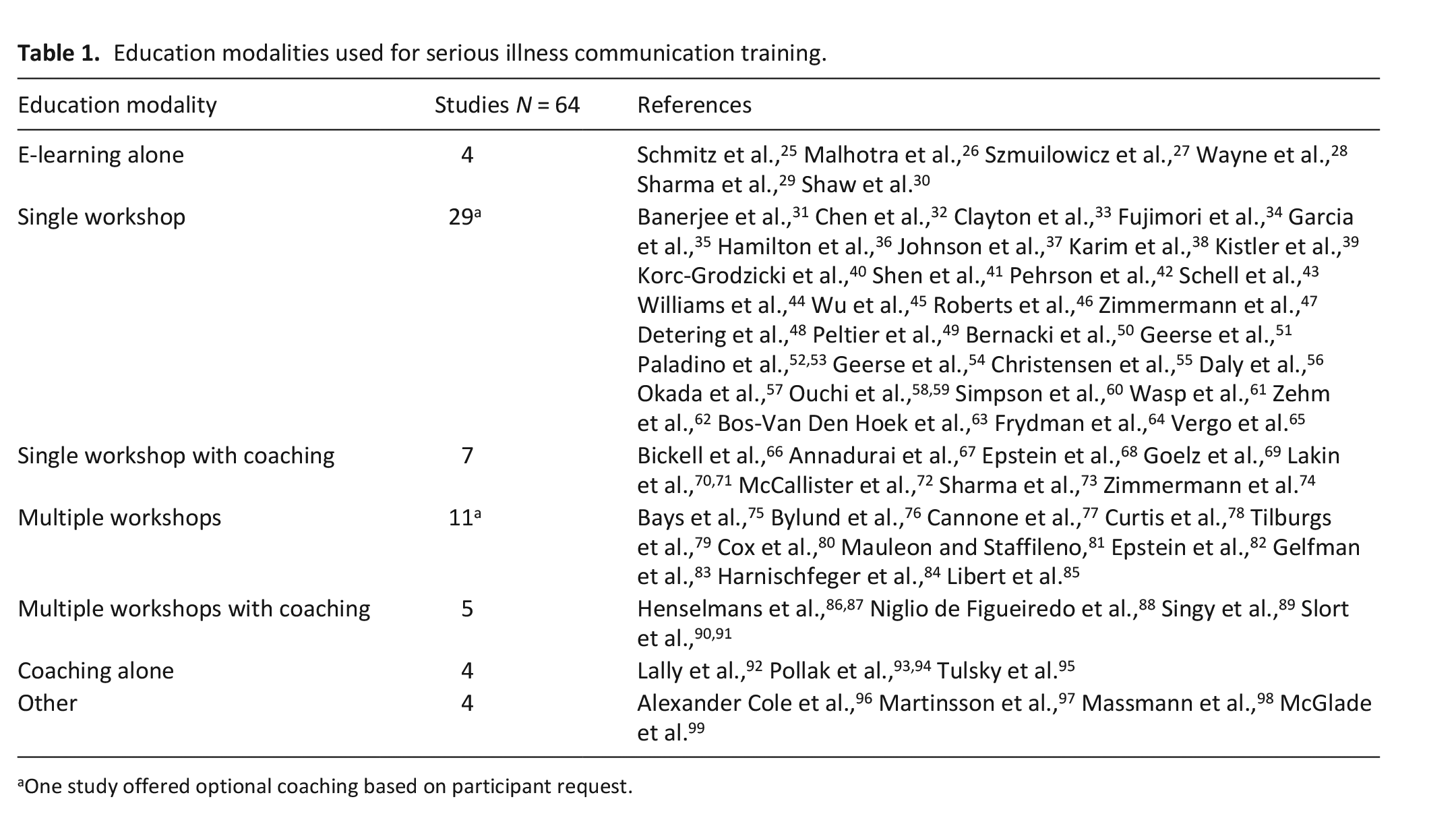
One study offered optional coaching based on participant request.
Single and multiple workshop(s)
The structure of workshops differed in how simulation was used and how they were organized temporally. Simulation techniques used involved role play, where learners (or facilitators) took on the roles of patients and healthcare providers in simulated scenarios. In this approach, one participant (or facilitator) acted as the patient, while the other participant acted as the healthcare provider. The other method involved standardized patients, who were trained actors specifically trained to portray patients with a particular health condition or history. Occasionally, single workshops were spread over one to three consecutive days whereas intervals for multiple workshops were in the order of weeks to months.
Coaching
The coaching modality was either an integral or mandatory component of an intervention or optional and driven by participant interest. Coaches used diverse methods to generate feedback and included direct observation of the participant conducting a real family meeting or seeing patients in their ambulatory clinic, review of videorecorded standardized patient encounters, audio recordings of real encounters, and documentation of conversations. Coaching components usually spanned over weeks to months.
The interventions described in thirteen studies were comprised of multiple modalities. Typically, these multimodal approaches combined single or multiple workshops with coaching. See Table 2 for more details about the education modalities.
Details on education modalities.
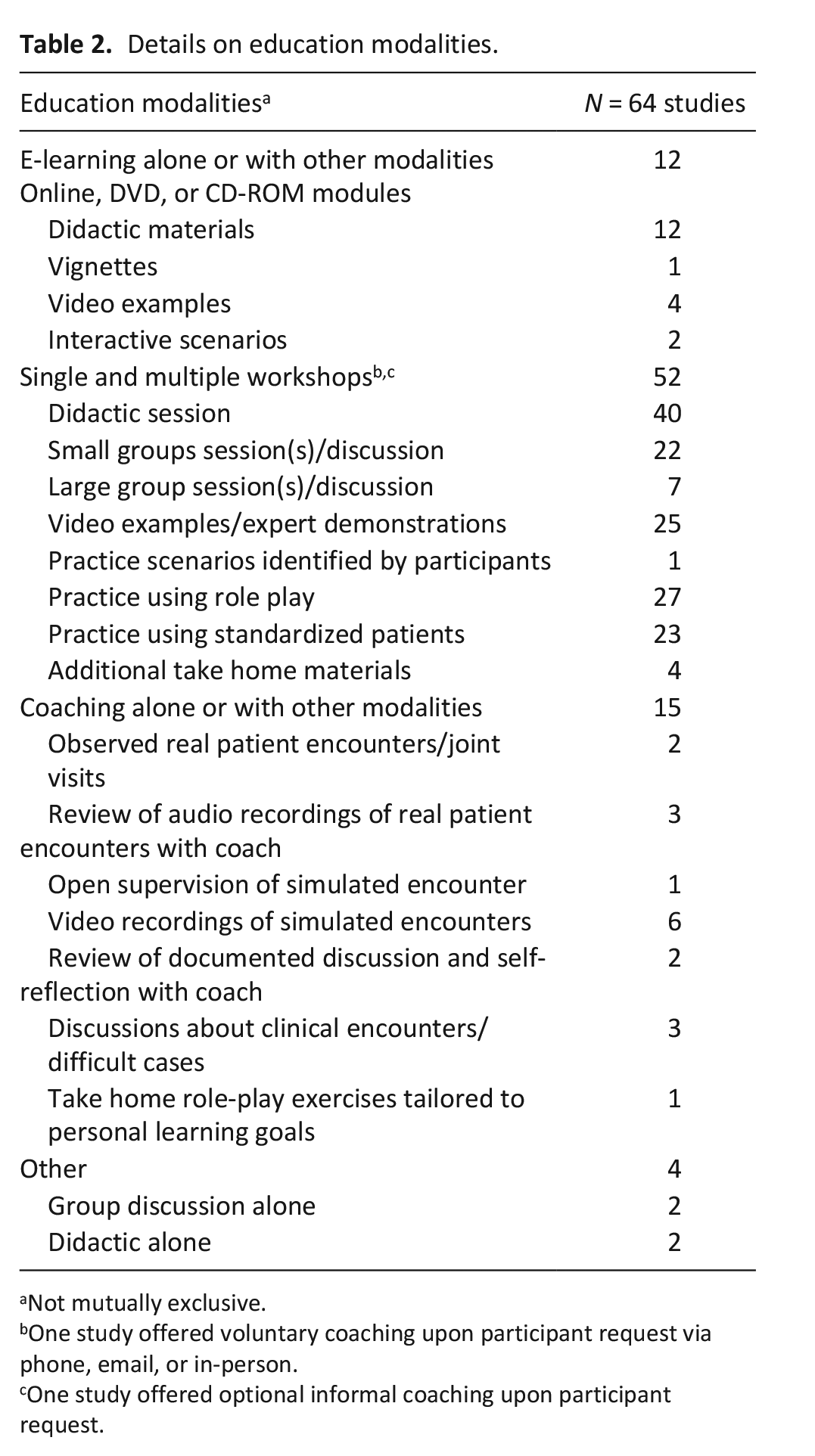
Not mutually exclusive.
One study offered voluntary coaching upon participant request via phone, email, or in-person.
One study offered optional informal coaching upon participant request.
E-learning
For this modality, interventions were comprised solely of self-directed learner experiences whereby materials would be worked through with no interaction between learners or with a facilitator. This applied to two studies in which learners completed online modules.
Target audience
Most interventions targeted specialists (56%) and only five studies (8%) specifically targeted primary care clinicians. Allied health professionals, such as nurses, occupational therapists, social workers, and nurse practitioners were the sole participants in 11 studies (17%). Additional details on target audiences and study participants are provided in Supplemental Appendix 2.
Content
Most interventions (n = 50/64) used formalized programs, including the SICP, 5 VITALtalk, 6 Com-On, Respecting Choices, 7 Comskil, 8 Best Case/Worse Case, 100 the Availability Current issues Anticipating program, 101 3-Act-Model, 45 or Shared Decision Making. 102 Content included both core communication skills and context-specific communication skills. Almost all interventions addressed similar core skills including active listening and communicating with empathy. While a common target for improvement was responding to emotions (36/64 studies), 58% either reported no improvement or did not provide results on this aspect of the intervention.
Context-specific skills included end-of-life care discussions; referring a patient to palliative care; discussing code status; discussing hospice or hospitalization; addressing patient preferences, values and wishes; how to conduct a family meeting; discussing death and dying; conveying prognosis; delivering bad news; or conducting an advance care planning discussion. None of the studies addressed cultural context as a component of their skill development.
Outcome measures and impact
When clinical behaviors were targeted, study authors regarded even minor improvements as a positive outcome, irrespective of their clinical or statistical significance. Therefore, the vast majority of these studies reported improved outcomes. Only four reported no difference in clinician behavior from the intervention.30,56,90,91 Among studies measuring patient outcomes, very few demonstrated improvement. Details on outcome measures are presented in Table 3. We describe these outcomes according to the Kirkpatrick levels 3 (Behavior) and 4 (Results) categories below.
Details on outcome measures.
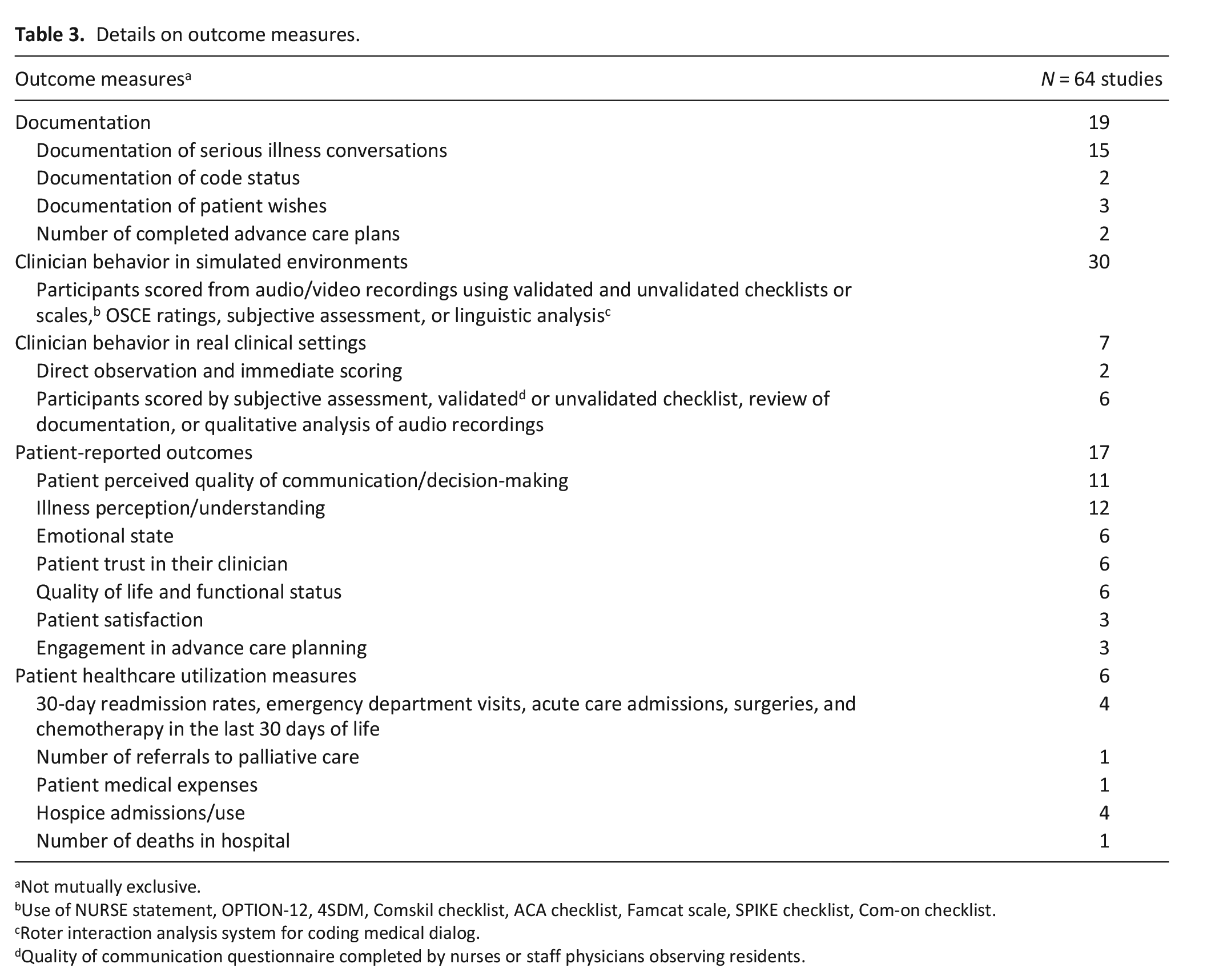
Not mutually exclusive.
Use of NURSE statement, OPTION-12, 4SDM, Comskil checklist, ACA checklist, Famcat scale, SPIKE checklist, Com-on checklist.
Roter interaction analysis system for coding medical dialog.
Quality of communication questionnaire completed by nurses or staff physicians observing residents.
Level 3—Behavior: Changes in frequency of documentation
Nineteen studies assessed the impact of the education intervention through changes in the frequency of documentation with many reporting improvements. For the vast majority, the context for the intervention was a larger quality improvement initiative and measures included documented goals of care, code status or advance care planning discussions, or completion rates of a Physician’s Orders for Life-Sustaining Treatment form.
Level 3—Behavior: Skill acquisition in simulated environments
The changes in behavior reported in two-thirds of all studies involved a pre/post assessment of specific communication skills, most often in simulated environments. Scales, checklists, predefined ratings, linguistic analysis software, or subjective evaluation were used by assessors. Several studies used validated tools such as the ComOn Check rating scale, 103 which was used in several studies evaluating the VITALTalk 6 training program. Another common instrument was the OPTION scale, 104 which was developed and validated to measure patient involvement.
Level 3—Behavior: Skill acquisition in real clinical settings
Seven interventions used the direct examination of behavior in clinical practice to capture impact. For four, patient encounters of trainees (i.e. residents, fellows, and nurse practitioner students) were directly observed by nurses or staff physicians. For the remainder, the quality of documented discussions or audio recorded clinical encounters was assessed.
Overall, almost all studies with clinician behavior outcomes reported positive effects of their intervention (i.e. 90%), regardless of outcomes being measured in a simulated or real environment. Three studies reported no improvement, one was in the quality of communication or quality of clinician skills at providing end-of-life care, 78 and two on how participants communicated about serious illness in simulated environments.25,90,91
Level 4—Results: Patient-reported outcomes
There were 17 studies that specifically measured patient-reported outcomes. All used validated instruments to measure various patient and family reported outcomes. Most studies administered more than one measurement scale or questionnaire and timing in relation to clinical encounters varied considerably. Measures that addressed the quality of the interaction with the clinician were typically administered immediately following the encounter and measures addressing quality of life and/or emotional states were administered weeks to months after encounters, most commonly at three months.
For six studies, evaluating patient-reported outcomes was the primary objective. The most common domains measured patients’ emotional state and emotional well-being, such as anxiety, depression, ability to cope, and peacefulness. However, the range of outcomes assessed varied widely between studies. Some other common elements measured were perceived shared decision making, perceived empathy, readiness to engage in advance care planning, quality of communication, satisfaction with communication, perceived therapeutic alliance, trust in the clinician, perceived competence of the clinician, concordant care, illness perception and understanding, quality of life, and quality of care. Usually, patient-reported outcomes were primarily assessed at the patient level, with the exception of one in which questionnaires were only administered to family members of patients in intensive care. 67
Most studies 12/17 (71%) that evaluated patient-reported outcomes showed no significant impact from the intervention. Five studies report having positively impacted one or more patient-reported outcomes.34,50,53,57,95 These outcomes involve a slight increase in patient perception of trust in their oncologist, small decreases in moderate to severe depression and an increased readiness to engage in end-of-life care discussions.
Level 4—Results: Patient health care utilization measures
There were six studies that evaluated patient health care utilization indicators such as hospital readmission rates, referrals to palliative care, emergency department visits, admissions to hospice, use of chemotherapy in the last 30 days of life, admissions to acute care, and death in hospital. The vast majority were large quality improvement studies. Half of the studies (three of six studies) reported improvements in health care utilization measures,71,74,93 two reported no difference,49,70 and one yielded mixed results. 81
Discussion
Main findings of the study
There have been numerous reviews in the past decade evaluating serious illness communication training, but a comprehensive review of individual education modalities and their impact has been lacking. Our scoping review is the first to report what is known about specific education modalities for serious illness communication training and their impact on clinician behavior and patient outcomes.
Several programs included a personalized education component (e.g. individualized feedback to the learner), which was identified as being beneficial by a prior meta-analysis. 13 The majority involved coaches or mentors providing individualized feedback, which was generated in a variety of contexts.
Elements of personalized education were also evident among simulation studies, where several interventions included personalized context for the clinical scenarios used. For example, using advanced cancer cases with oncology participants. In other studies, workshop content or role play exercises were developed to meet participants’ individual learning goals. Interventions with a personalized component often reported significant clinician behavior change. This aligns with what is known about authentic learning environments that allow teachers to focus on the learner’s point of view and propose alternative strategies for navigating conversations without overwhelming learners with new information.105–109 This is thought to improve receptivity and transfer of both knowledge and skill.106 –109
An important finding of this review is the collection of barriers to exploring and determining the impact of individual education modalities. A major barrier was the wide variability in the structure of each modality (e-learning, single workshop, multiple workshops, and coaching), as well as differences in overall duration and time spent on activities (didactic, demonstration, and simulation). Systematic reviews have previously highlighted the heterogeneity between studies, which limits the ability to determine the effectiveness of serious illness communication interventions.12,13 This is consistent with our experience with this scoping review as despite an in-depth examination and mapping of educational modalities, we were unable to discern clear trends or patterns. In addition this emphasizes that the relationships between educational interventions and either clinician behaviors or patient outcomes are complex.
Other barriers to assessing the impact of individual education modalities include an inability to tease the impact of different modalities apart. This was both from each other in multi-modal interventions and from the accompanying system changes when embedded as part of a larger quality improvement intervention. For several of these, a related barrier was the absence of data confirming that communication skills had improved. It is possible that quality improvement interventions will be more likely to achieve desired outcomes if study designs specifically include confirmation of improved communication skills.
Finally, while for most interventions, study designs, selection of outcome measures, and implementation processes were well described, there were several with discrepancies and inconsistencies in the reporting of results and statistical analyses. This added to the difficulty in drawing concrete conclusions about the direct impact of the modalities on outcomes. Together these barriers prevent generating concrete and practical guidance for faculty and course developers tasked with improving serious illness communication skills for their setting.
What this study adds?
Responding to a patient’s emotions is considered an essential communication skill for clinicians32 –35 and there is a clear need for this skill to be included in serious illness communication training experiences. 36 This skill was only measured in a few of the studies, which outlines a critical gap in current serious illness communication training.
Another area for further research is the timing of outcome assessment, which ranged from immediate to over 1 year. Studies in which intervention outcomes were assessed within a few weeks all reported improvements in skills. However, improvements in skill were not seen among studies where outcomes were measured months after the intervention. A key consideration beyond skill acquisition is knowledge and skill retention, and therefore, long-term outcome measures are needed to show sustained clinical behavior change. Studies evaluating life support knowledge and skill retention over time in healthcare providers report that knowledge deterioration rates are variables, ranging from 6 weeks to 2 years. 110 Multiple and distributed opportunities for learning can improve long-term knowledge retention, and in fact, both clinical experience and clinical practice have significant impact on retention.111 –113 This review included all types of healthcare providers, some of whom may have had more opportunities for communicating with seriously ill individuals in their practice than others. It is therefore unclear whether similar outcomes measures can be compared between studies, given the variability in practice among healthcare providers. Future study designs could, in part, address this challenge by confirming skill acquisition in the short term and demonstrating skill retention strategies and behavior change in the longer term.
Over the last 10 years of communication skills training experiences, few studies report improvements in patient-reported outcomes. If the aim of serious illness communication training is to improve the experiences of patients and families, programs must be designed to address this. An ideal study would be able to provide evidence of improved communications skills as well as clinical practice change and improved patient-reported outcomes. For instance, backward design is increasingly being used in medical education and is a model whereby program developers work backwards from desired outcomes to design appropriate assessment tools and curricular content. 114 It is a three-staged approach to instructional design which involves first identifying desired outcomes, followed by determining appropriate outcome measures, and then planning learning experiences and teaching methods.115,116
We found limited indication as to how education science (i.e. the application of adult learning theoretical frameworks or involvement of education scientists) informed the development of interventions or the study designs to evaluate these interventions. Study teams may have been guided by theory or included education scientists, but specific contributions were seldom clear. There has been a paradigm shift in medical education toward using evidence-based teaching and education theory to guide curriculum development which has been spearheaded by competency-based medical education research.117–119 While educational theory can provide a solid framework for designing interventions, it may not always be practical or feasible to implement in real-world clinical settings, particularly due to the structure of existing systems.117,119 However, explicit descriptions of incorporated theory and the contributions of education scientists are important gauges of quality in the design and evaluation of interventions and are a first step toward bridging the gap between educational theory and the practical implementation of communication research. 120
Strengths and limitations of the study
This scoping review has several strengths. It used rigorous and transparent methods throughout the entire process. The screening and data charting forms were pretested by all reviewers and revised as needed prior to implementation. Each citation and article were reviewed by two independent reviewers from the team who met in regular intervals to resolve conflicts. Our use of a bibliographic manager (EndNote 20) in combination with review software (Rayyan© 2022) ensured that all citations and articles were properly accounted for during the process. We included studies of all designs and completed an in-depth examination of the training interventions for which provider behavior and patient outcomes were assessed.
While we followed a systematic process to identify and review articles for inclusion, we chose to limit our search to two key databases (MEDLINE and Embase) and reference lists of published systematic reviews and did not include other bibliographic databases such as CINHAL or PsychINFO. Given the topic and nature of the research question, we reasoned that the selected databases would most likely contain nearly all relevant published articles. Our search algorithm included several different terms previously used to describe training for serious illness communication; however, other terms may also exist. Our review also excluded studies where participants were exclusively undergraduate students. Another limitation of this review is that it did not include grey literature such as conference abstracts, government and company reports due to their limited information on the methodology for delivering communication training. None of the studies addressed cultural sensitivity as a component of their skill development, which is an area for future research given the critical role that cultural context plays in shaping patient’s experiences and perceptions of illness.121–123 Finally, our data extraction of the education content and modalities is limited to the descriptions that the study authors provided. Given the heterogeneity between education formats and because several studies combined education modalities, we were unable to identify specific interventions that contribute to the greatest behavior changes or improved patient-centered outcomes.
Conclusions
This scoping review explores the literature on educational modalities for serious illness communication training and their impact on clinician behavior and patient outcomes. We found that while some studies reported improved clinician skills in simulated settings, no improvements were confirmed in clinician practice or patient outcomes. As multiple modalities were often used in larger quality improvement initiatives, the impact of individual modalities could not be determined. However, the heterogeneity among education modalities and their outcome measures limits the ability to draw conclusions about the impact of the interventions. Without standardized outcome measures, it is difficult to make recommendations for designing or implementing future interventions. To build the evidence that serious illness communication training improves patient experiences, well-defined education modalities, and standard patient-centered outcome measures are needed. For future research, a focused systematic review, that includes a critical appraisal of the identified literature, could help further elucidate the impact of different educational modalities of serious illness communication training.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231186180 – Supplemental material for Education modalities for serious illness communication training: A scoping review on the impact on clinician behavior and patient outcomes
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231186180 for Education modalities for serious illness communication training: A scoping review on the impact on clinician behavior and patient outcomes by Melissa Lavecchia, Jeff Myers, Daryl Bainbridge, Nadia Incardona, Oren Levine, Leah Steinberg, Daniel Schep, Joanna Vautour, Shilpa Jyothi Kumar and Hsien Seow in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163231186180 – Supplemental material for Education modalities for serious illness communication training: A scoping review on the impact on clinician behavior and patient outcomes
Supplemental material, sj-pdf-2-pmj-10.1177_02692163231186180 for Education modalities for serious illness communication training: A scoping review on the impact on clinician behavior and patient outcomes by Melissa Lavecchia, Jeff Myers, Daryl Bainbridge, Nadia Incardona, Oren Levine, Leah Steinberg, Daniel Schep, Joanna Vautour, Shilpa Jyothi Kumar and Hsien Seow in Palliative Medicine
Footnotes
Acknowledgements
The authors wish to acknowledge the contributions to the search strategy of Laura Banfield, MLIS, MHSc, Health Sciences Library, McMaster University, Hamilton, ON, Canada.
Author contributions
All authors listed provided substantial contributions to conception and design of the study, as well as acquisition of data. For interpretation of data, M. Lavecchia, J. Myers, D. Bainbridge and H. Seow were the main contributors, but all listed authors were involved in this process. M. Lavecchia drafted the initial manuscript, with significant contributions from J. Myers and H. Seow. All authors critically revised the article for important intellectual content. All authors gave final approval of the version to be published and agree to take public responsibility for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data management and sharing
The complete MEDLINE search strategy, study details on mode of delivery and outcomes measures are presented in the tables and supplementary materials.
Please contact the corresponding author for access to the study’s data extraction form.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent
Not applicable. There are no human participants in this article and informed consent is not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.