
Abstract
Background:
The Integrated Palliative care Outcome Scale is a newly developed advancement of the Palliative care Outcome Scale. It assesses patient-reported symptoms and other concerns. Cognitive interviewing is recommended for questionnaire refinement but not adopted widely in palliative care research.
Aim:
To explore German- and English-speaking patients’ views on the Integrated Palliative care Outcome Scale with a focus on comprehensibility and acceptability, and subsequently refine the questionnaire.
Methods:
Bi-national (United Kingdom/Germany) cognitive interview study using ‘think aloud’ and verbal probing techniques. Interviews were audio-recorded, transcribed verbatim and analysed using thematic analysis and pre-defined categories. Results from both countries were collated and discussed. The Integrated Palliative care Outcome Scale was then refined by consensus.
Setting/participants:
Purposely sampled patients from four palliative care teams in palliative care units, general hospital wards and in the community.
Results:
A total of 15 German and 10 UK interviews were conducted. Overall, comprehension and acceptability of the Integrated Palliative care Outcome Scale were good. Identified difficulties comprised the following: (1) comprehension problems with specific terms (e.g. ‘mouth problems’) and length of answer options; (2) judgement difficulties, for example, due to the 3-day recall for questions; and (3) layout problems. Combining the results from both countries (e.g. regarding ‘felt good about yourself’) and discussing them from both languages’ perspectives resulted in wider consideration of the items’ meaning, enabling more detailed refinement.
Conclusion:
Cognitive interviewing proved valuable to increase face and content validity of the questionnaire. The concurrent approach in two languages – to our knowledge the first such approach in palliative care – benefited the refinement. Psychometric validation of the refined Integrated Palliative care Outcome Scale is now underway.
Outcome measures need to be specifically developed in palliative care populations to reflect the concerns of advanced illness and ensure minimal respondent burden.
The Palliative care Outcome Scale (POS) and Palliative care Outcome Scale–symptom module (POS-S) are brief, valid and reliable questionnaires developed for this population.
However, there is some overlap, and patient and clinician feedback indicates scope for further refinement.
Cognitive interviewing is recommended for questionnaire development but not adopted widely in palliative care research.
In response to patients’ and clinicians’ demands, we present a refined measure (Integrated Palliative care Outcome Scale (IPOS)) that has been shaped by the patients’ perspectives.
This study demonstrates once more the importance of cognitive interviewing in the refinement of outcome measures and that it can be done effectively in a palliative care population.
The concurrent use of cognitive interviewing in two languages – for the first time in palliative care – provided additional valuable information, resulted in wider consideration of the meaning and context of each item and led to a better overall refinement of the IPOS questionnaire.
IPOS is now available for clinical use; it is one of the few brief measures validated in this population that covers all relevant domains.
The refined version of the IPOS is currently undergoing phase II of validation in Germany and the United Kingdom to demonstrate the psychometric properties.
Wider awareness and use of cognitive interviewing in measure refinement in palliative care is crucial, and cognitive interviewing in more than one language can have added value.
Background
Patient-reported outcome measures (PROMs) are questionnaires completed by patients to measure their perceptions of their functional status and well-being. 1 The Integrated Palliative care Outcome Scale (IPOS) is a PROM and a newly developed advancement of the Palliative care Outcome Scale (POS) which assesses symptoms and other palliative care (PC) concerns as perceived by the patient. There are versions for patients and healthcare professionals.
The POS was developed in 1999 with the involvement of patients and has been validated in a variety of settings: hospice in-patient care, day care, home care, hospital in-patient care and community and outpatient services. 2 It has been used to inform clinical practice, to monitor service interventions, to evaluate and improve the quality of care and as a research tool.3,4 The POS team has currently endorsed 11 translations, and POS is being used in over 20 countries.4,5 To describe the impact of PC-specific symptoms, a symptom module (the POS-S) was developed as an addition to the POS. Requests from clinical colleagues to merge POS and POS-S triggered the development of IPOS (see Figure 1). The IPOS is based on POS and POS-S, with changes to the wording of certain questions and response options. The 10 questions cover patients’ main concerns, common symptoms, patient and family distress, existential well-being, sharing feelings with family, information received and practical concerns.
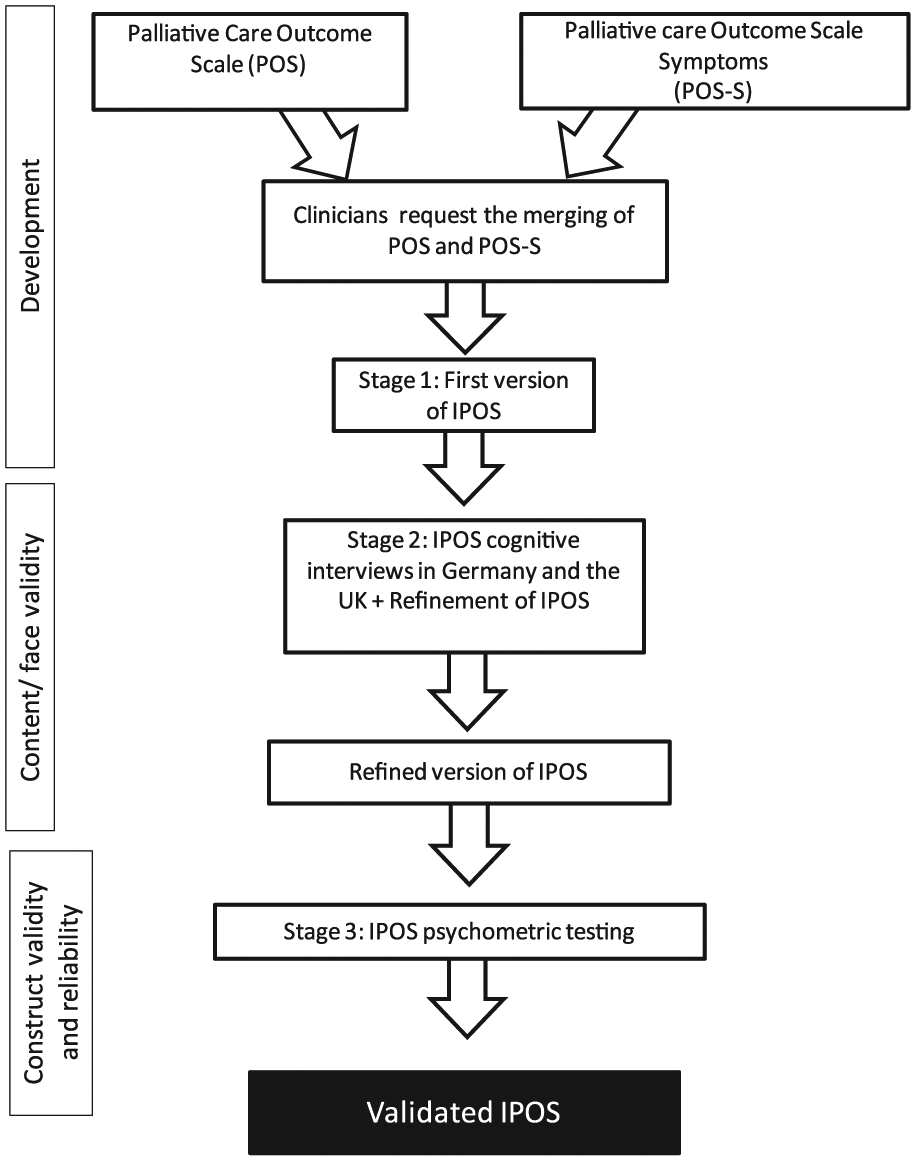
Design stages of the IPOS.
Adopting a recommended quality criterion for questionnaires,6,7 we aimed to involve patients in the questionnaire development through cognitive interviewing to ensure face and content validity and acceptability. Cognitive interviewing is increasingly used as a step in the refinement of survey questions and PROMs. 8 A complex cognitive process takes place when research participants answer questionnaires. This includes comprehension of the question, retrieval of information from memory, judgement processes to estimate an answer and formulation of a response.9,10 The European Organisation for Research and Treatment of Cancer (EORTC) guidelines for questionnaire development recommend cross-language pre-testing. 11 Accordingly, we aimed to base the IPOS refinement on views from German- and English-speaking patients and have the refined questionnaires available for concurrent psychometric validation in both countries.
Methods
Design
Cross-sectional, qualitative, bi-national and multicentre study enrolling purposively sampled PC patients in Germany and the United Kingdom, using cognitive interviews.
Setting and participants
In Germany, patients were recruited from a university hospital PC unit and its associated hospital support and community PC teams. UK patients were recruited from a university hospital support team. Inclusion criteria were as follows: age 18 years or above, capacity to give consent and sufficient fluency in written and spoken English or German language to answer the questionnaire. Exclusion criteria were as follows: being too unwell or distressed to participate as judged by the clinical team. Participants were purposively sampled according to the following criteria in order to achieve variation across key characteristics: gender, over and under 65 years, high, medium and low functional status as measured by the Australia-modified Karnofsky Performance Status (AKPS) scale 12 (see Table 1) and malignant/non-malignant main diagnosis. It was not aimed to have equal numbers in all cells, but to include participants with all characteristics. Screening took place at multidisciplinary team meetings or handovers, and a clinical team member asked whether the patients were interested and provided an information leaflet. Interested patients were approached by the researcher – except five who had deteriorated or been discharged. Of the 29 approached patients, 25 gave their informed consent.
Demographic and clinical details of participants.
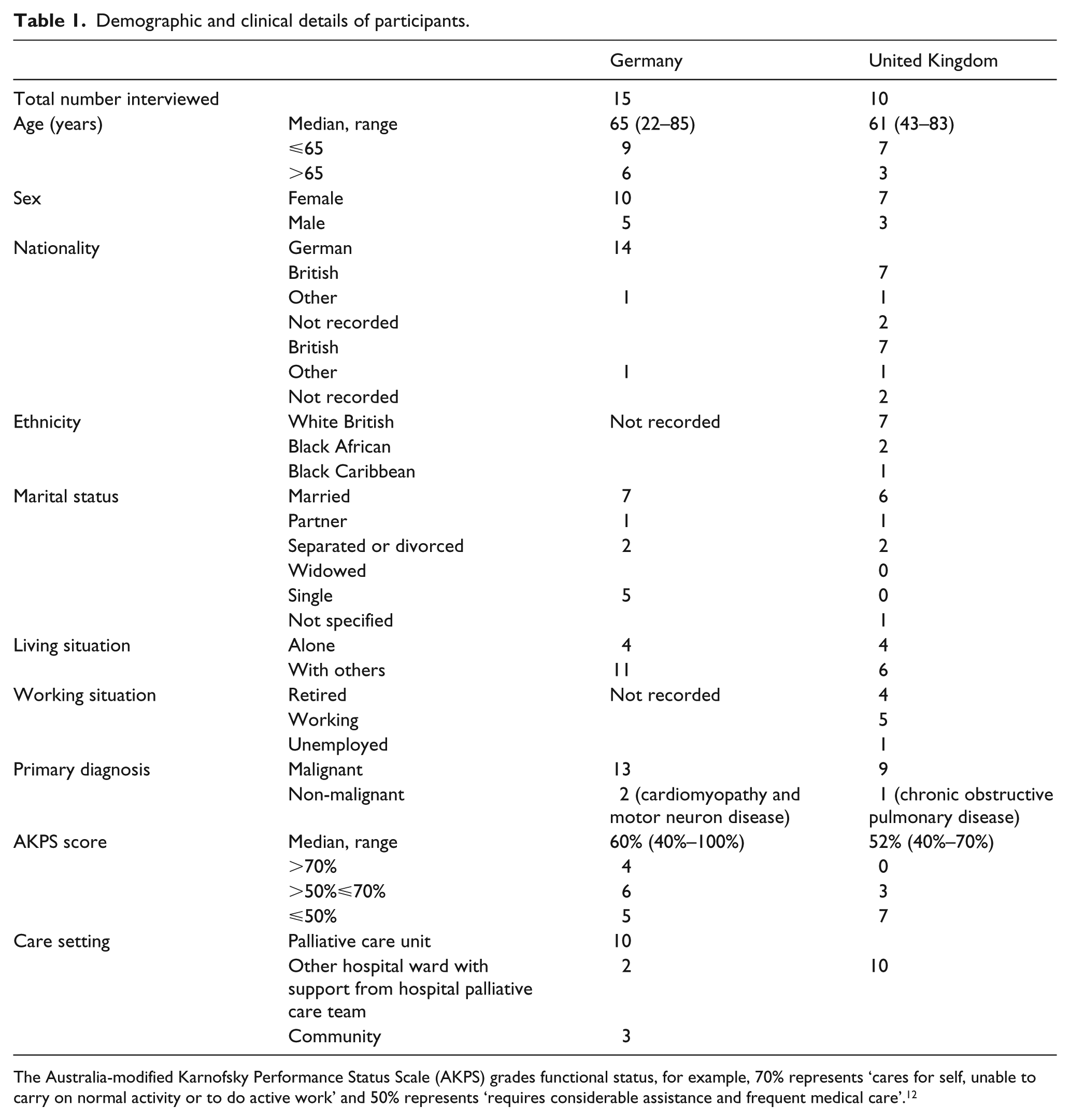
The Australia-modified Karnofsky Performance Status Scale (AKPS) grades functional status, for example, 70% represents ‘cares for self, unable to carry on normal activity or to do active work’ and 50% represents ‘requires considerable assistance and frequent medical care’. 12
Cognitive interviews
Formal translation of the IPOS from English to German had previously been conducted using standard techniques. 13 The interviews were conducted in the participants’ current care setting, that is, on the ward or in the participants’ home. Participants were asked to complete the questionnaire, using a combination of ‘think aloud’ and concurrent verbal probing techniques to elicit problems or comments regarding the completion.14,15 ‘Think aloud’ techniques (uttering the thoughts during question answering) were demonstrated by the interviewer at the start of the interview. Probing techniques were both spontaneous, to explore verbal or non-verbal utterances like hesitations or irritation, and stand-ardised according to an interview guide (see Appendix 1). This was based on the four-stage question response model as described by Tourangeau 10 (comprehension, retrieval, judgement and response formulation). Probes were developed for each of the four stages, and additional questions related to layout, missing aspects in the questionnaire and burden associated with its completion. The interviews were audio-recorded and transcribed verbatim.
Analysis of the interviews and refinement of the IPOS
Interviews were analysed by two independent researchers in each country using thematic analysis as described by Willis. 14 In accordance with the interview guide, the transcript was also categorised following Tourangeau’s 10 question response model (comprehension, retrieval, judgement and response formulation). Additional categories included the following: layout, acceptability/questionnaire burden and additional aspects. Results of all participants were compared and aggregated for each question and each category in both countries to identify the reasons for difficulties in answering the questionnaire and other emergent themes.
The German results were translated. Results from both countries were then collated and discussed between the research teams and the IPOS was refined accordingly, based on consensus. The German version was adapted according to the refined English version, taking German-language-specific results into account.
The study was approved by the relevant ethics committees (Ethikkommission of Ludwig-Maximilians-Universität Munich, reference number 169-13; National Research Ethics Service (London–Dulwich Committee) reference number: 13/LO/0573).
Results
Demographics
A total of 15 German and 10 UK interviews (16–54 min long) were completed between July 2013 and July 2014. The median age was 65 years in Germany (range 22–85 years) and 61 years in the United Kingdom (range 43–83 years). In Germany, 10/15 and in the United Kingdom, 7/10 participants were female. The predominant primary diagnosis was cancer. A third of the participants in Germany and two-thirds in the United Kingdom had an AKPS score of 50% or lower, which is defined by requiring ‘considerable assistance and frequent medical care’. 12 The majority of participants were in-patients. Details are shown in Table 1.
Findings from the interviews and IPOS refinement
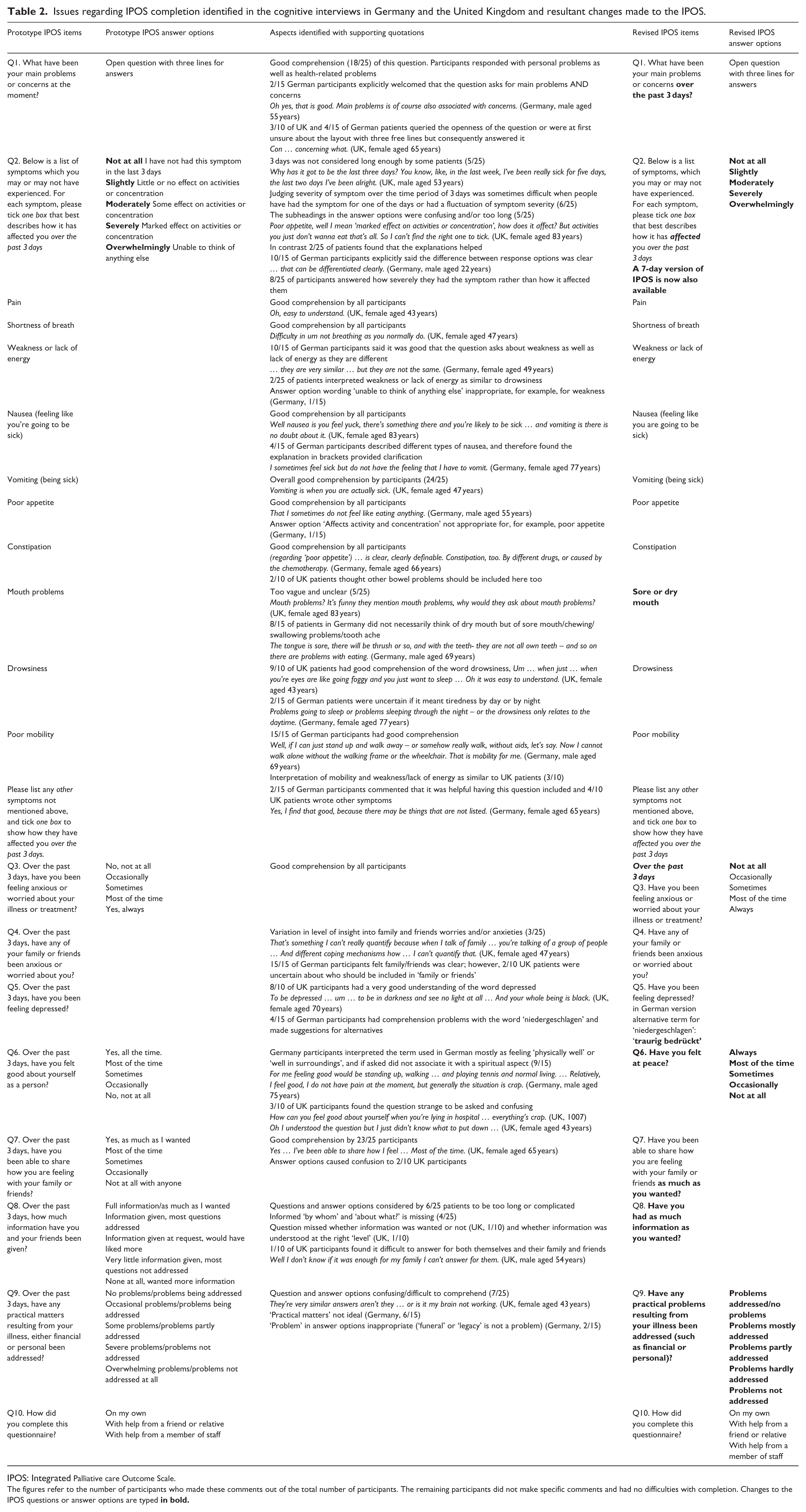
The interviews in both countries demonstrated that for the majority of participants, most questions and answer options worked well. The identified difficulties were mainly comprehension problems and some pertained to judgement. No problems were identified with retrieval or response formulation. The interview results and the changes made based on them are shown in Table 2. The revised questionnaire can be found on the POS website. 5
Issues regarding IPOS completion identified in the cognitive interviews in Germany and the United Kingdom and resultant changes made to the IPOS.
IPOS: Integrated Palliative care Outcome Scale.
The figures refer to the number of participants who made these comments out of the total number of participants. The remaining participants did not make specific comments and had no difficulties with completion. Changes to the IPOS questions or answer options are typed
Comprehension
Patients were certain about their main problems and concerns (question 1), and many described these as the things that are always on your mind. Positive comments about the symptom list in question 2 included the following:
Oh, easy to understand. (United Kingdom, female aged 43 years)
and
I think question 2 is good, that it is all dealt with in a very ‘compact’ way. (Germany, female aged 25 years)
‘Pain’, ‘shortness of breath’, ‘nausea’, ‘poor appetite’ and ‘constipation’ listed in question 2 were well understood by all participants. Comprehension of question 3 (anxiety/worries) was also good for all participants.
Some comprehension problems were identified in both countries. First, difficulties arose with the wording of specific questions. For example, the term ‘mouth problems’ in question 2 was regarded as too vague, and in contrast to the intent of the question, many patients did not think of dry mouth when answering it. Furthermore, comprehension problems concerned answer options which were regarded as too long or complicated in question 2 (symptom list), question 8 (information received) and question 9 (practical matters). In addition, a third of patients in each country rated the severity of the symptom instead of the degree of being affected by it in question 2 (symptom list).
For some questions, interviewing in the two countries elucidated additional aspects that were important for the refinement of the IPOS: The question ‘Have you felt good about yourself as a person?’ (Q6) had been difficult to translate into German as there is no equivalent phrase that captures the same concept. The translation used for the interviews was understood by most participants as feeling physically well or feeling well in their surroundings. This complemented the comments of UK patients that this question was strange to be asked. A UK patient noted that question 8 (information needs) missed whether the received information was wanted. There were cases when comments made by the German patients diverged with those from the UK patients: Some UK patients interpreted ‘weakness and lack of energy’ and ‘mobility’ as similar, whereas all German patients had a clear understanding of ‘mobility’. Some German patients were unsure about the meaning of ‘drowsiness’, while UK patients had a good understanding of the word. In addition, there were a few translation-related difficulties commented on by the German participants, for example, comprehension problems of the German word used for ‘depressed’.
Judgement
A judgement problem was identified in both countries due to the 3-day time period over which symptoms are sought: some participants said they were unsure how to answer a question when they had a fluctuation of symptom severity; however, all answered the questions. Five participants commented that they would prefer a longer time frame, for example, 7 days. In addition, three participants said that judging the level of insight and anxiety of family and friends was difficult, but all answered the question.
Acceptability/questionnaire burden, missing aspects and layout
Overall, acceptability of the measure was good. Spontaneous comments included
Well I think it’s a good questionnaire I really do … it lets everybody like staff that they’ve only got to look at it and they know how you feel. (United Kingdom, female aged 74 years)
One patient became distressed when she talked about the worries of her family, but explicitly wanted to continue answering the questions because she thought they were important. One other patient found answering the questionnaire burdensome because she had problems concentrating. All other patients did not find it distressing or burdensome to answer the questions. In the United Kingdom, 8 of the 10 patients stated that they wanted to keep all questions in IPOS, one patient expanded on the importance and variety of all questions:
… when someone’s not well as I say it changes your whole system your whole … routine … and everything needed to be looked into properly. (United Kingdom, female aged 70 years)
One or two patients each suggested the following aspects to be additionally included in the questionnaire: ease of contacting the relevant team, experience of care, general well-being, insomnia and diarrhoea. We did not incorporate these in the refined IPOS for the following reasons: We recognise the importance of measuring patient experience of care, but intended this questionnaire to remain a PROM. The aim was to assess specific symptoms and concerns. Defining insomnia is difficult, often different types of it are described. 16 Besides, an open list is provided for patients for not-listed symptoms, for example, insomnia and diarrhoea. The group agreed that this was sufficient, as we wanted to minimise respondent burden.
Finally, layout problems were identified, especially the difficulty of staying in the right line for questions 1, 2, 7 and 8. The layout changed automatically due to the item refinements, especially shortening/aligning of answer options.
Added value of cognitive interviewing in two languages for IPOS refinement
The difficult translation of ‘felt good about yourself as a person’ (question 6) into German and the fact that the chosen translation was mainly understood by patients as physical well-being led to detailed discussions between both research teams about the question’s meaning and intention. As the intended emphasis was on spiritual well-being, the question was replaced by the respective question from the African POS ‘Have you felt at peace?’ This question is a good measure of spiritual well-being in African PC and is highly relevant across diverse cultures and beliefs. 17 Discussion in the team also helped to find concise and clear phrasing in both languages for ‘mouth problems’ (question 2) as well as for questions 8 (information received) and 9 (practical matters). The items ‘weakness or lack of energy’, ‘drowsiness’ and ‘poor mobility’ were left unchanged after extensive discussion. For this discussion, the partly conflicting results from the interviews in both languages and considerations for alternatives in both languages – which were deemed inferior to the current items – were paramount.
Discussion
The cognitive interviews conducted simultaneously in Germany and the United Kingdom showed that for the majority of patients, most questions and answer options of the IPOS worked well. The difficulties that were identified were mainly comprehension problems, which were addressed in questionnaire refinement. A judgement problem was reflected in some patients’ replies regarding the 3-day time period over which symptoms were sought. These patients found it hard to judge the score if symptoms were fluctuating. This corresponds with the findings of Bergh et al. 18 in their cognitive interview study of the Edmonton Symptom Assessment System (ESAS), where patients found judging intensity ‘now’ difficult for fluctuating symptoms. The scoring of fluctuating symptoms seems to be a challenge for patients regardless of whether they are asked to score them ‘now’ or over a period of time. In accordance with the wish of some patients for a longer time frame than 3 days, a 7-day IPOS version is now also available. Generally, this problem of scoring fluctuating symptoms on a questionnaire illustrates that any questionnaire can only be one component of a comprehensive clinical assessment. 19
Problems with retrieval or response formulation were not identified in this study. The absence of retrieval problems corresponds with the findings of a former cognitive interviewing study in PC and may be due to the short time period for which symptoms were sought. 20 However, the absence of retrieval problems is important to note for this population, which was mostly elderly and with low functional status. Another important finding was that except the two patients mentioned earlier, these PC patients with mostly poor functional status did not find it distressing or burdensome to complete the questionnaire, and that they wanted to retain all questions.
Overall, cognitive interviewing showed good comprehension and acceptability of the questionnaire, identified difficulties in its completion and helped to refine it. Enabling patients to shape IPOS greatly benefited the refinement. Cognitive interviewing of patients therefore proved a valuable method to reduce measurement error caused by misinterpretation of some questions and thereby to increase the questionnaire’s validity. Based on our findings, we want to emphasise the previously published view that cognitive interviewing is a valuable tool in questionnaire refinement and that it can be used effectively in the PC setting.20,21
To our knowledge, this is the first study in PC showing that simultaneous interviews in two languages can provide additional benefits for questionnaire refinement. Multinational perspectives have generally not been well represented in cross-national survey instruments so far. 22 This is also true for PC outcome measures despite their cross-national and international use. Studies that have used cognitive interview techniques in the development of PC outcome measurement instruments have done so in a single language.18–21 In other areas of medicine, results of cognitive interviews in several languages have been published.23,24 These studies, however, do not comment on the additional value of interviews in several languages to refine the tested outcome measures.
We want to emphasise that we still recommend cognitive interviewing in one language first for the development of a questionnaire from scratch. In this study, we wanted to refine an already existing questionnaire, the POS. The consistent results from the two countries and languages strengthened the credibility of the findings 22 and therefore the evidence to inform the changes to the questionnaire. As Lee 22 recommends, in multi-site interviews, the aim should also be to identify as many different problems as possible across different sites. As demonstrated, results that were only found in one of the countries, for example, regarding ‘felt good about yourself as a person’, and conflicting results between the countries (e.g. regarding ‘mobility’ and ‘drowsiness’) added important aspects to the common findings. Collating the findings from interviews in the two languages and discussing them from two linguistic angles resulted in wider and deeper consideration of meaning and context of each item. This helped to shape the final version of the questionnaire, based on the patients’ perspectives in both countries, to the optimum.
Methodological issues, strengths and limitations
In this study, we combined ‘think aloud’ and probing techniques as advocated by cognitive interview experts. 14 Thus, we tried to maximise the information gained – such as unanticipated information by the ‘think aloud’ technique and specific information, for example, regarding the wording of certain questions, by probing techniques – and to minimise interviewer-imposed bias. 14 As recommended for interviewing in multiple countries or languages, we used standardised probing as well as spontaneous probing, thus combining their respective advantages: 22 Standardised questions maintain a level of objectivity and consistency of interviews across countries, while spontaneous probing allows flexibility to adjust the interview to the specific situations and different communication styles and facilitates more in-depth investigation into various aspects. 22 We used concurrent probing as retrospective probing was likely to be hindered by recall problems in this elderly population. 20
It is debated whether ‘formal’ or ‘informal analysis’ of cognitive interviews is preferable. 14 In this study, we used thematic analysis as described by Willis 14 and additional coding applying the four categories from Tourangeau’s 10 question response model, that is, a formal approach. However, as argued elsewhere, questions and answer options that worked well and the main difficulties emerged without formal analysis.14,20 Analysis was performed by two independent researchers in each country to enhance the findings’ credibility.
A limitation of this study is its relatively small sample size. It is still debated what constitutes a ‘sufficient’ sample size for cognitive interviews.15,22 However, small numbers are common as this method is work-intensive and yields rich data.14,20 With our study, we met current recommendations of 5–15 respondents per language group. 22 The majority of respondents had cancer which questions the transferability of the findings to people with other life-limiting diseases. However, this reflects the still high proportion of patients with cancer cared for by specialist PC in both countries. As only three community patients were included in the study, the results mainly reflect the views of PC in-patients. However, these patients have complex PC needs – as this is by definition the reason for a referral to a PC hospital support team or PC unit. Therefore, it seems adequate to base the development of a tool that aims to assess PC concerns mainly on the views of these patients.
Conclusion
Cognitive interviewing of patients for whom the questionnaire is intended proved a valuable tool to increase its face and content validity. The concurrent approach in two languages – to our knowledge the first such approach in PC – was beneficial. The refined version is currently undergoing psychometric validation in Germany and the United Kingdom. Wider awareness and use of cognitive interviewing in measure refinement in PC is crucial.
Footnotes
Appendix 1
Acknowledgements
The authors would like to thank the patients for their engaged participation and the staff at the participating centres for their help with recruitment.
Funding
This article presents independent research funded by the National Institute for Health Research (NIHR) under the Programme Grants for Applied Research scheme (RP-PG-1210-12015) (for the interviews in the United Kingdom). The views and opinions expressed are those of the authors and do not necessarily reflect those of the NHS, the NIHR, MRC, CCF, NETSCC, the NIHR Programme Grants for Applied Research programme or the Department of Health. In Germany, this research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.