
Abstract
Background:
In order to provide responsive, individualised and personalised care, there is now greater engagement with patients, families and carers in designing health services. Out-of-hours care is an essential component of community palliative care. However, little is known about how patients, families and carers have been involved in the planning and design of these services.
Aim:
To systematically search and review the research literature that reports on how out-of-hours palliative care services are provided in the community and to identify the extent to which the principles of co-design have been used to inform the planning and design of these services.
Design:
Systematic literature search and review.
Data sources:
A systematic search for published research papers from seven databases was conducted in MEDLINE, PsycINFO, Embase, Emcare, PubMed, CINAHL and Web of Science, from January 2010 and December 2021. Reference list searches of included papers were undertaken to source additional relevant literature. A manifest content analysis was used to analyse the data.
Results:
A total of 77 papers were included. The majority of out-of-hours services in the community were provided by primary care services. The review found little evidence that patients, families or carers were involved in the planning or development of out-of-hours services.
Conclusion:
Incorporating patients, families and carers priorities and preferences in the planning and designing of out-of-hours palliative care service is needed for service providers to deliver care that is more patient-centred. Adopting the principles of co-design may improve how out-of-hours care scan be delivered.
Out-of-hours palliative care services vary across organisations, jurisdictions and countries based on availability of resources, workforce, and geographical area.
There is no one best fit model of out-of-hours palliative care service that can provide all the needed care and resources to patients with palliative care needs, their families and carers.
The involvement of patients, families and carers in planning and designing out-of-hours palliative care service continues to prove difficult to achieve in practice.
This review identified the extent to which the principles of co-design have been reported by the research literature to inform the planning and design of out-of-hours palliative care services in the community.
Palliative care patients, families or carers appear to be under-represented in research that reports on the planning and developing of out-of-hours palliative care services in the community.
Findings suggests that there may be significant impediments to end-user engagement in the co-design of services and highlights the need to involve patients, families and carers in developing out-of-hours care models to provide more individualised and personalised service.
A greater role for patients, families and carers as end-users in out-of-hours service planning and design is needed for out-of-hours palliative care services in the community.
The GP plays a critical role in caring for individuals who want to be cared for in the community. The delivery of effective patient-centred out-of-hours palliative care requires services to be coordinated and well-integrated.
Further work is required to support the co-design of out-of-hours palliative care services in ways that engage and build patient, family, carer, neighbourhood and community capacity.
Introduction
Out-of-hours service is a fundamental component in community palliative care. It is defined as care delivered during out of usual working hours, weekends and public holidays. 1 Providing such care, especially in a person’s home can be physically and emotionally challenging. 2 During out-of-hours, when less help and support is available, escalation of physical symptoms, emotional and psychological distress can increase the stress and anxiety experienced by families and carers.2–4 Increased care-related burden is often reported as patients near end-of-life. 5
In 2018, the World Health Organisation (WHO) emphasised the need for round-the-clock palliative care services to support patients, their families and carers in the community. 6 Patients, families and their carers often face issues such as unsatisfactory symptom management, insufficient consideration of personal preferences, culturally inappropriate care, unnecessary ambulance call outs and hospital admissions.7–11
To address these challenges, various models of out-of-hours palliative care services have been developed. However, health service design and planning has often been dominated by healthcare planners and professionals, a practice that may skew services away from delivering responsive care that prioritises the needs of patients, families and carers.12,13 Viewing patients, families and carers as the ‘expert of their experiences’, involving them as partners and collaborators in planning and designing out-of-hours palliative care services could be part of the solution. Whilst challenging, such an approach is consistent with the philosophy of palliative care which emphasises person and family-centred care. Patients, families and carers input can assist service providers to prioritise what services are needed and how they should be provided to achieve the best outcomes.14,15 Applying an approach to service planning that values end-user input, can enable the needs of different population groups to be better understood and optimise patient-centric, holistic, and a stronger relational approach to care.16–19
Despite this imperative, little is known about the extent to which patients and families have been engaged as co-designers in out-of-hours palliative care services or research about these services. Co-design, in this context, refers to patients and families working in partnership with staff to improve out-of-hours palliative care services.16,20 The principles of co-design include equal partnership, openness, respect, empathy, and design together. 16 To date, there have been very few studies that have reported end-users directing their palliative care needs and priorities as a part of service planning.14,21–26
Aim
This paper therefore aims to systematically search and review the research literature that reports on how out-of-hours palliative care services are provided in the community and to identify the extent to which the principles of co-design were identified and used to inform the planning and design of these services.
Methods
A systematic literature search and review was undertaken to address the research aim. This methodology combines the strengths of a critical review with a comprehensive and exhaustive search process. It involves a synthesis and analysis of knowledge about a topic.27,28 Rather than focusing on a preferred type of study design, studies included demonstrate a wide range of study designs incorporating quantitative, qualitative, multiple and mixed method approaches. This type of review provides greater flexibility on the types of studies included 29 and broadens the scope of the search to include, for example, service evaluations and outcomes based research studies on out-of-hours palliative care services.
Eligibility criteria
A set of eligibility criteria was initially determined by the authors then refined through an iterative process as articles were screened and questions were raised, discussed and resolved about the inclusion and exclusion criteria. The process of constructing the inclusion criteria was adapted from that described by Merner et al. 30 This approach uses seven eligibility categories: phenomena of interest, types of study, settings, participants, intervention, context and exclusion criteria (Table 1).
Eligibility criteria.
Search strategy
A search strategy was developed by the team in consultation with a health specialist librarian. A list of main concepts and keywords and their synonyms was compiled from journal articles about the topic, thesauri and a search of electronic database-controlled vocabulary indexes. Keywords and the application of Boolean operators, proximity operators, truncation and phrase searching was developed and their application to the search process reviewed and validated by the specialist librarian (Supplemental Appendix 1). The search was undertaken by two authors (CL and TB) through electronic databases: MEDLINE, PsycINFO, Embase, Emcare, PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Web of Science. Reference lists of all included studies were hand searched to identify additional, potentially relevant articles. The search was limited to papers written in the English language. To secure a large and robust sample, international research articles published in refereed journals over a period of 12 years, from January 2010 to December 2021, were selected. Articles located were exported to EndNote (Version 9) and duplicates removed.
Screening and study selection
At the first level of screening, titles and abstracts were independently reviewed by two authors (CL and PN). Articles excluded were all those that were clearly not related to out-of-hours palliative care services. Full-texts of the remaining articles were obtained and assessed against study eligibility criteria by two authors (CL and PN). A third reviewer, TB, was consulted in the event of disagreements as well as for any citation that required further discussion and refinement of the eligibility criteria. Reference list searches of included papers were undertaken to source additional relevant literature. The study selection process and reasons for exclusion of publications are presented using the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram 32 (Figure 1).
PRISMA 2020 flow diagram.
To explore the extent to which the principles of co-design had been used in planning and developing out-of-hours palliative care services, the team drew upon the five core principles or values of co-design proposed by the NSW Agency for Clinical Innovation (ACI) 16 : equal partnership, openness, respect, empathy, and design together. Face validity of these five principles was confirmed by cross-reference to those principles and elements described in other key policy documents including the Social Care Institute for Excellence (SCIE), 33 National Standards for Public Involvement (NIHR), 34 INVOLVE, 35 Canadian Institutes of Health Research, 36 co-design resources produced by the Australia Healthcare and Hospital Association (AHHA) 37 as well as the Australian Government Department of Health (DOH) 38 (Table 2).
Co-design principles.
Data extraction and analysis
Retrieved studies were screened to identify if they reported on the engagement of patients, families and/or carers together with researcher, healthcare providers and/or other stakeholders. This subset was further reviewed to ascertain if one or more co-design principles was described or referred to in the report. To do this, text was examined by applying manifest content analysis.39–41 In this method, textual elements, such as words and phrases, are identified that could reflect the principles of co-design. These elements are then grouped based on similar denotations as evidence of one or more of the five co-design principles.39,42
Data were extracted from the selected studies using a customised spreadsheet within Microsoft Excel tailored to address the research question. The characteristic domains included publication year, author, country of origin, setting, method & study design, participant, aim/s, intervention, outcome measured, results and recommendations. Data extraction was undertaken by CL and reviewed by TB and PN. This approach was initially trialled using five articles and minor modifications made to data categorisation through team discussion. Extracted data was subject to descriptive analysis.
Critical appraisal of individual sources of evidence
As the purpose of this review was to address broad questions about out-of-hours palliative care services, retrieved articles did not undergo quality assessment. However, the authors selected and included peer reviewed research papers based on the inclusion and exclusion criteria established for the review. Studies included in the review were selected based on their relevance to the research question rather than their research design.
Results
Search outcome
Seventy-seven articles were included. The initial search retrieved 787 articles across all databases. Removal of duplicates resulted in 384 articles selected. After title and abstract screening, 283 were excluded, resulting in 103 articles which were subject to full text screening. Twenty-five articles were located through reference lists of selected articles. Fifty-three articles were excluded because they did not meet the inclusion criteria (Figure 1).
Study characteristics
Study location
Of the 77 research papers included in this study, 30 (39%) studies were conducted in the United Kingdom, nine (11.7%) from the Netherlands, eight (10.4%) from Scotland, five (6.5%) each from the United States of America, Australia, and Canada, four (5.2%) from Denmark, two (2.6%) from India and Taiwan and one (1.3%) each from France, Germany, Norway, Sweden, Switzerland, Ireland and Japan (Table 3).
The characteristics and findings of included articles (n=77).
Abbreviations: *OOH=out-of-hours, *GPs=General Practitioners
Study period
The numbers of studies published each year from 2010 to 2021 tended to decline though on average, there were seven papers published per year (Figure 2). The largest number of publications was recorded in 2015 and 2020 (n = 10) and the lowest was recorded in 2021 (n = 1)
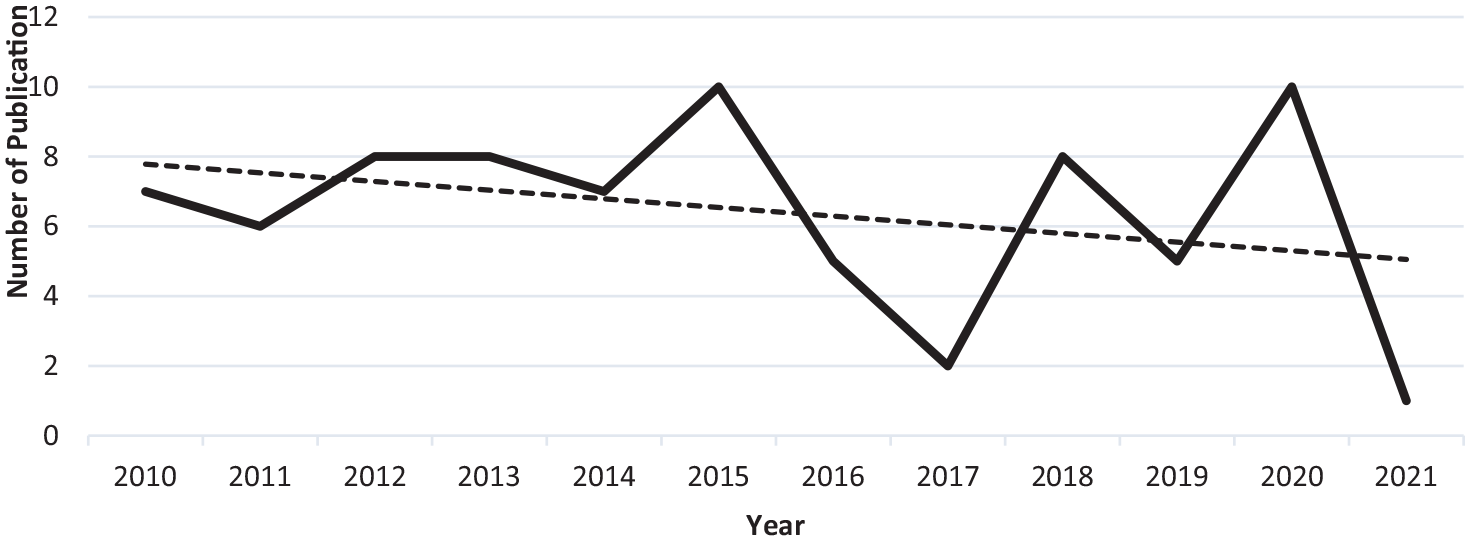
Publication distribution by year (n = 77).
Study design
A diverse range of research methods were used. Thirty-eight (49.4%) studies used quantitative methods, 25 (32.5%) used qualitative methods and the remainder, (18.2%) used mixed-methods. Of the quantitative studies, a majority used a retrospective design to identify populations with palliative care needs who had received out-of-hours services. Qualitative research approaches were used to identify and explore end-users as well as healthcare professionals’ experiences, perceptions, and opinions regarding out-of-hours services (Table 3).
Study participants and sample sizes
Across all studies, the largest grouping of participants was patients or their medical records (n = 28). Sample sizes ranged from 1 to 56,407 participants. The second largest participant group was general practitioners (n = 24), samples ranged from 1 to 5333 (n = 24). This was followed by family and/or caregivers (n = 21), ranged within 1–24 participants. Other groups of participants that have been reported on were nurses (n = 16), palliative care specialists (n = 9), and paramedics, emergency medical team and rapid response team (n = 10). Additional groups of service management teams (n = 7), pharmacists (n = 4), allied healthcare (n = 2) and community and/or public participants (n = 2) were also identified in some studies (Table 3).
Service provider
The studies included a range of service providers. Most studies reported on services delivered by primary care providers (n = 31) such as general (GP) medical practices, out-of-hours GP co-operatives, national service provider, primary care trust, clinics and hospitals. Twenty studies examined out-of-hours services delivered by hospice and/or palliative care specialists either independently or as an integrated service. There were 12 studies that included services provided by the emergency department. The pre-hospital emergency team, emergency medical team, paramedic, rapid-response team and ambulance team were also responsible for delivering out-of-hours services in the community. Across all of these studies, emergency departments worked in collaboration with the palliative care or hospice and/or palliative care unit or primary care service providers. Five studies reported the community home care as the main setting to access palliative care service during out-of-hours. Four services were provided from the hospital and two services were provided by the community pharmacy (Table 3).
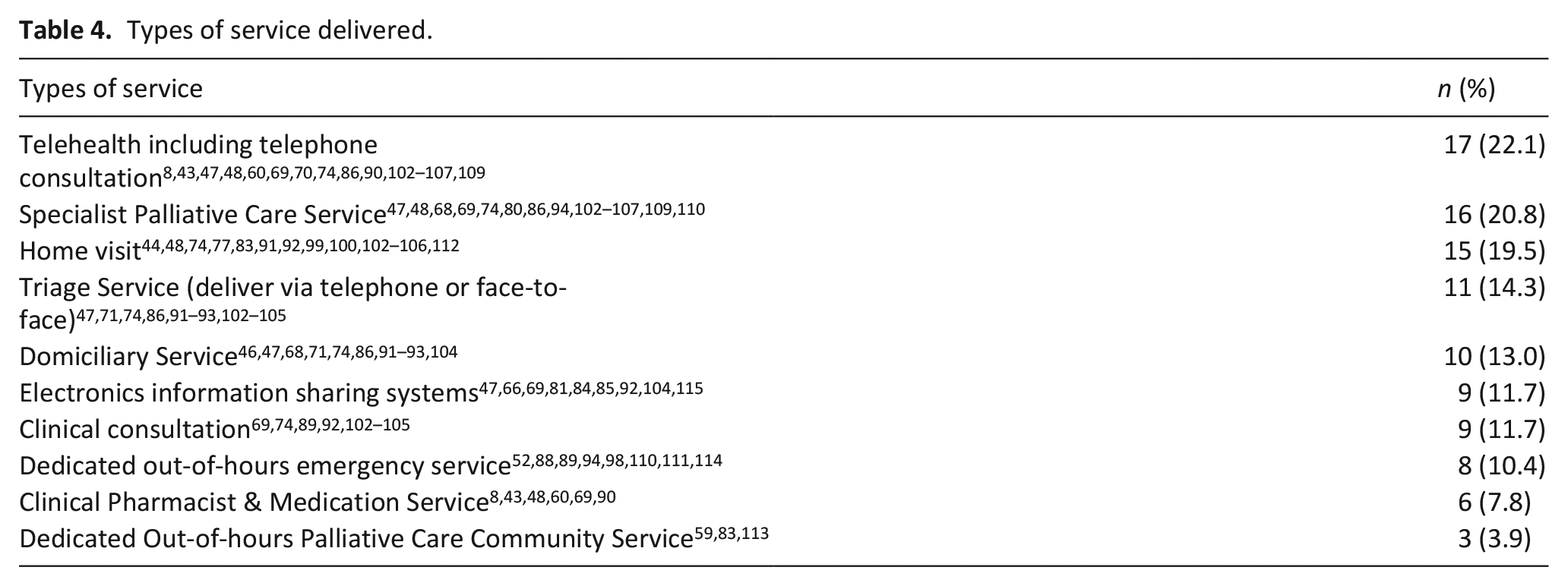
Type of service delivered
There was a range of services delivered, with many providers delivering more than one ‘type’ of service to patients out-of-hours. Telehealth consultation (including telephone helplines/advice line services) was the most common type of service reported followed by Specialist Palliative Care services and various types of home visit services. The least reported services that have been the subject of research were services about out-of-hours clinical pharmacist and medication delivery as well as dedicated out-of-hours palliative care services that specifically for community based care (Table 4).
Types of service delivered.
Recommendations for further research
The majority of the studies include recommendations for further research to be conducted into out-of-hours palliative care services and pointed to the need to prioritise end-user preferences within different service contexts. This includes investigation on end-users perspectives, preferences and partnership models to optimise the delivery of personalised out-of-hours services. Future work could also involve out-of-hours interventions on service outcomes by different healthcare providers. Other recommendations included the out-of-hours planning on care coordination and application of telehealth. Additional studies on cost benefit of services provided to different types of patients and care for wider range of terminal conditions were also proposed.
Use of a co-design approach
From the 77 reviewed studies, none clearly identified or described the application of a co-design principle. However, there were 10 studies that reported the involvement of patients, families and/or carers in addressing out-of-hours service issues. There was evidence that these studies had, to some degree, embedded at least one of the five principles of co-design (Table 2) at some stage of the research process. Only two studies reflected all five principles. ‘Design Together’ appeared to be the principle most applied by the studies identified. Other co-design principles to feature more commonly were ‘Respect’, ‘Openness’ followed by ‘Equal Partnership’ and ‘Empathy’ (Supplemental Appendix 2).
Discussion
This review aims to systematically search and review the research literature that reports on how out-of-hours palliative care services are provided in the community and to identify the extent to which the principles of co-design have been used to inform the planning and design of these services.
Out-of-hours palliative care services in the community
The research was predominately retrospective and cross-sectional, drawing on data collected by the services themselves. A majority of the reported studies originated from the United Kingdom and western European countries.
Over the study period, there was a decline of research outputs that focussed on out-of-hours care. Given that out-of-hours service is a component a 24/7 model of care, research effort may have been directed to improving the planning and management of service links with in-patient care and coordination of shared services in the community.70,117,118
In general, primary care services (primarily those provided by General Practitioners) was observed to be the predominant mechanism to access out-of-hours palliative care services. Nurses, palliative care specialists, pharmacists and increasingly, the emergency care team and other allied healthcare workers also actively contribute, though some groups appear to be reported less frequently in the research literature. Increased consumer demand and, a broader acceptance of a palliative approach to the care indicates that out-of-hours care is provided by a broader team of health care professionals and other care providers.119,120 This suggests that more research into multidisciplinary care, including that delivered in collaboration with families and caregivers with may be warranted.
The relative proportion of out-of-hours palliative care research conducted into primary care, specialist palliative care and Emergency Department services point to the research interest and importance of each area to out-of-hours service provision. Whilst some specialist services have been designed to address specific needs of out-of-hours care,52,59,83,113 primary care services clearly play a major and critical role in coordinating with secondary and tertiary care agencies to ensure continuity of care.
There was range of services provided during out-of-hours. This included home visits, outpatient face-to-face consultation and telephone and/or telehealth consultation. This suggests that interprofessional collaboration and coordination is an important component of effective out-of-hours care in the community.80,97,121 According to the WHO, 122 in order for services to deliver the highest quality of care across health system, a workforce drawn from different professions that can work together with patients, carers and communities is required. In taking this approach, out-of-hours service providers have the potential to expand the availability of palliative care services, prevent service duplication and reduce the burden on carers during out-of-hours.
In many reports, whilst there was an implicit recognition of the importance of incorporating end-user’s priorities and preferences, only a few studies demonstrated collaboration with patients, their families, and carers.
Co-design principles
For this review, we drew upon the co-design principles established by the ACI. 16 These included: equal partnership, openness, mutual respect, empathy, and the concept of design together, where in this context, patients and families work in partnership with providers to improve out-of-hours palliative care services. Whilst not an exhaustive list, these principles were quite broad and had much in common with those used internationally.
For most studies, the involvement of patients and families in out-of-hours palliative care service planning is low and was difficult to assess. If it did occur, such engagement was not often made explicit. There were only a few studies that reported how service planners had positioned themselves to engage with patients and families to inform and improve out-of-hours services using a co-design process. This was, perhaps, not surprising, given the time-limited nature of the services provided to a palliative patient. Patients who have limited life expectancy may only be able to provide input to service planning at a single point of time rather than making an ongoing contribution. Furthermore, it can be more challenging to engage patients who are receiving care if they are geographically dispersed and if these services are not well integrated. 123 Service planners may also be concerned about patients’ and families’ knowledge of services and may feel they have sufficient information about a patient’s needs through regular contact with care providers124,125 and may also source data collected through other mechanisms such as advance care plans and directives. Studies have also found that there is a lack of resources available to service providers to facilitate co-design activity. 126 Some may hold a negative attitude towards engaging end-users in service planning and design24,26 and may also exert a gatekeeper effect believing that such engagement causes unnecessary stress to the patient.124,126
How palliative care patients and other end-users can be engaged, as partners, in service design process presents a significant challenge and has not been well described in the research literature. Co-design may not be widely reported by the sector because it is resource intensive (and would negatively impact on service delivery), a relatively low priority for those investigating out-of-hours care or, has been embedded in such ways that it has proved difficult to articulate in research reports. As a consequence, there was limited advice on how to apply the principles of co-design to enhance patients and families involvement and measure the outcome of their involvement in research.127,128
It should also be recognised that many organisations obtain feedback about the services they provide through mechanisms such as case audits and carer satisfaction surveys administered sometime after a patient has died. Also, palliative care workers are sensitive to their patients’ needs and can be protective. Not wishing to burden them or impose an additional stress, they may feel confident in their ability to relate their experiences and authentically convey the wishes of their patients throughout the out-of-hours palliative care planning process.
Recommendations for future research
Co-design and the principles of co-design has been successfully applied across many areas of health care. Since patient, family and other stakeholder hold unique and valuable experiences, future research that explores their experiences may enrich and add value to out-of-hours palliative care services planning. Reporting how and in what capacity end-users are engaged in service planning and design process could be an additional quality indicator for palliative care research in this area.
Further research about the principles of co-design and application of the co-design process in the planning and development of out-of-hours palliative care services in the community is warranted. This would include investigating ways to successfully engage and collaborate with diverse range of key stakeholders, strategies to address key challenges and barriers to participation and evaluating the impact of end-user involvement on the quality of care and patient outcomes.
Strengths and limitations
Drawing on the research literature, this study outlined how out-of-hours palliative care services are provided across a number of countries, provided a summary of where this research was conducted, when published and the methodologies used. To ensure rigour, the review used established guidelines and adhered to a careful process of review throughout the selection and screening of articles. To our knowledge, this is the first review to identify the extent to which co-design principles have been reported about out-of-hours palliative care services in the research literature.
Study limitations relate to the search strategy and the selection and application of key search terms. Our approach may have excluded studies with components of out-of-hours palliative care services that were not identified. Similarly, in the initial screening of title and abstract of studies found, we may have excluded study that did not focus on out-of-hours services but may have link to services provided during out-of-hours in the community. The search was also limited to research studies in the English language published from January 2010 to December 2021. The grey literature was not searched. Policy documents, government reports, service provider accreditation reports and evaluations were not included though these could prove fertile ground for further investigation of the topic. Additionally, most of the studies reviewed in this study were related to cancer patients. A review targeted to chronic conditions and frailty may uncover additional novel findings.
Conclusion
The review found that out-of-hours palliative care service research does not report a high level of end-user engagement. Whist challenging, incorporating end-users’ priorities and preferences through the application of co-design principles in the planning and designing of out-of-hours palliative care service can help align care to the needs and values prioritised by patients and their families. Service transformation can be augmented through the co-design process by placing end-users’ needs and values at centre stage in a respectful and authentic way. Timely engagement of patients and their significant others may contribute to good quality out-of-hours palliative care service design.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221132089 – Supplemental material for Co-designing Community Out-of-hours Palliative Care Services: A systematic literature search and review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221132089 for Co-designing Community Out-of-hours Palliative Care Services: A systematic literature search and review by Christine Low, Pathmavathy Namasivayam and Tony Barnett in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163221132089 – Supplemental material for Co-designing Community Out-of-hours Palliative Care Services: A systematic literature search and review
Supplemental material, sj-pdf-2-pmj-10.1177_02692163221132089 for Co-designing Community Out-of-hours Palliative Care Services: A systematic literature search and review by Christine Low, Pathmavathy Namasivayam and Tony Barnett in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163221132089 – Supplemental material for Co-designing Community Out-of-hours Palliative Care Services: A systematic literature search and review
Supplemental material, sj-pdf-3-pmj-10.1177_02692163221132089 for Co-designing Community Out-of-hours Palliative Care Services: A systematic literature search and review by Christine Low, Pathmavathy Namasivayam and Tony Barnett in Palliative Medicine
Footnotes
Acknowledgements
All authors contributed to defining research questions, search aims, and methodology used to identify, collect and analyse data as well as to writing of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CL is a recipient of a University of Tasmania College of Health and Medicine Graduate Research Scholarship. The Centre for Rural Health receives funding from the Commonwealth of Australia Department of Health under its Rural Health Multidisciplinary Training Program.
Ethics approval
Ethics committee approval was not required for this systematic search and review because the study does not involve human subjects.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.