
Abstract
Background:
Malignant bowel obstruction occurs in up to 50% of people with advanced ovarian and 15% of people with gastrointestinal cancers. Evaluation and comparison of interventions to manage symptoms are hampered by inconsistent evaluations of efficacy and lack of agreed core outcomes. The patient perspective is rarely incorporated.
Aim:
To synthesise the qualitative data regarding patient, caregiver and healthcare professionals’ views and experience of malignant bowel obstruction to inform the development of a core outcome set for the evaluation of malignant bowel obstruction.
Design:
A qualitative systematic review was conducted, with narrative synthesis. The review protocol was registered prospectively (https://www.crd.york.ac.uk/prospero, CRD42020176393).
Data sources:
MEDLINE, EMBASE, CINAHL, PsycINFO and Scopus databases were searched for studies published between 2010 and 2021. Reference lists were screened for further relevant publications, and citation tracking was performed.
Results:
Nine papers were included, reporting on seven studies which described the views and experiences of malignant bowel obstruction through the perspectives of 75 patients, 13 caregivers and 62 healthcare professionals. Themes across the papers included symptom burden, diverse experiences of interventions, impact on patient quality of life, implications and trajectory of malignant bowel obstruction, mixed experience of communication and the importance of realistic goals of care.
Conclusion:
Some of the most devastating sequelae of malignant bowel obstruction, such as pain and psychological distress, are not included routinely in its clinical or research evaluation. These data will contribute to a wider body of work to ensure the patient and caregiver perspective is recognised in the development of a core outcome set.
Keywords
Malignant bowel obstruction is a distressing complication of advanced cancer, having a profound impact on quality of life, prognosis, and persistent, unresolved symptoms.
Current evidence informing the palliation of malignant bowel obstruction is inadequate, and the lack of standardised clinical outcome measures for malignant bowel obstruction has resulted in inconsistent reporting and varied primary endpoints across published research in this area.
Crucially, there is a lack of data to indicate these current outcome measures reflect what is important to people with malignant bowel obstruction, and their caregivers.
This qualitative systematic review highlighted the immense symptom burden and psychosocial impact of malignant bowel obstruction on patients and those around them, with wide reaching effects on a patient’s quality of life.
We identify the lack of literature regarding lived experience of patients with malignant bowel obstruction and those around them.
Our findings demonstrate the complexities of treating patients with malignant bowel obstruction and the importance of communication between healthcare staff and these patients, and those around them.
Evaluation of malignant bowel obstruction should focus on patients’ symptoms (e.g. pain, nausea) rather than undue emphasis on physiological parameters (e.g. volume of vomit).
The psychological impact of malignant bowel obstruction on patients and their caregivers should be evaluated, and support made available as required.
Background
Malignant bowel obstruction, defined as bowel obstruction due to cancer or its treatments, occurs in up to 15% of people with gastrointestinal cancers and 50% of people with advanced ovarian cancer (15%).1–3 It is responsible for a myriad of distressing symptoms including nausea, vomiting, abdominal distension, colic, pain and constipation.3–9 Consequently, it has a profound impact on patients and their caregivers’ quality of life, and often requires hospitalisation for persistent, unresolved symptoms.4,10 It is believed to be the commonest cause of death in people with ovarian cancer. 11
Management options are limited, since most cases are not amenable to surgical intervention. Non-surgical approaches usually involve a combination of antiemetics and anti-secretory agents, often with gut drainage via nasogastric tube or venting gastrostomy.12,13 The current evidence informing the palliation of malignant bowel obstruction is inadequate; clinical guidelines favour somatostatin analogues but recommendations are based largely on case series and insufficiently powered clinical trials. 10 Recently, two adequately powered, well-conducted clinical trials of somatostatin analogue versus usual care demonstrated no objective benefit for patients, and one suggested evidence of harm.5,14 However, these studies used different primary endpoints to evaluate the efficacy of interventions; number of days from vomiting for one and proportion of patients with one or fewer episodes of vomiting per day at day 7 for the other. Four other clinical trials, albeit inadequately powered for evaluation, used a further four different primary endpoints; nausea score, absence of a nasogastric tube, number of vomiting episodes and volume of nasogastric tube drained secretions. 15 The inconsistent approach to evaluating malignant bowel obstruction has resulted in varied primary endpoints across published research. Consequently, the data is not amenable to meta-analysis and guideline recommendations vary according to methodology and interpretation.16–18 More importantly the outcome measures do not necessarily reflect the symptoms that people with malignant bowel obstruction consider most important to them. This had led to a call for a consistent approach to evaluating the severity of malignant bowel obstruction and its response to treatments in a way that is meaningful to those experiencing the condition. 15
In order to address this knowledge gap, the Research Assessment outcome measures for Malignant Bowel Obstruction (RAMBO) study was developed. The full protocol is published 19 and registered with Core Outcome Measures in Effectiveness Trials (COMET; ID:1402). 20 The ultimate aim of this programme of work is to develop standardised, measurable outcomes that can be used by clinicians, researchers and patients/caregivers. Such a core outcome set could be used to ensure that the improvement, or progression of malignant bowel obstruction is evaluated in a consistent way, be it to evaluate the impact of an intervention, evaluate a patient’s clinical status, or assess overall symptom burden. The overarching study consists of four phases: Phase I: Review of quantitative and qualitative literature, Phase II: Interviews with patients, caregivers and healthcare professionals; Phase III: Expert panel meeting to produce a list of outcomes identified through phases I and II and Phase IV: Delphi surveys to refine the outcomes, and consensus meeting to ratify those outcomes.
In this paper we report the findings of a systematic review of qualitative studies pertaining to the views and experiences of patients, caregivers and healthcare professionals, about malignant bowel obstruction. The decision to report these data separately follows recommendations of our Patient and Public Involvement partners who felt it important to ensure the patients’ and caregivers’ voices were presented clearly and not lost in the data of a larger report. The findings of a systematic review of the quantitative literature will be reported in a separate paper.
Methods
This review was conducted in accordance with the Palliative Care Evidence Review Service (PaCERS) modified systematic review methodology. 21 This review uses modified systematic review methods in which components of the review process are streamlined, in particular the time frame, which was decided upon due to the striking lack of existing literature before 2010, which was identified from a scoping search undertaken prior to the conduction of the review. The review was prospectively registered with the International Prospective Register of Systematic Reviews on 30th March 2020, ID: CRD42020176393, and is reported following the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines.22,23
Review question
The review question was ‘what are the views and experiences of people with malignant bowel obstruction, their caregivers, and healthcare professionals providing care to people with malignant bowel obstruction?’.
Search strategy
A systematic search of the following databases between January 2010 to May 2021: MEDLINE, EMBASE, CINAHL, PsycINFO and Scopus. Grey Literature: OpenGrey and CareSearch. We also carried out forward citation tracking of included studies in Google Scholar. We searched for papers published, in English language publications. To address the research question, the search strategy focussed on three concepts (see Supplemental Appendix 1 for full search strategy). Searches were conducted combining search strings for (a) bowel obstruction search terms (e.g. intestinal obstruction, bowel obstruction), (b) adult population diagnosed with malignant bowel obstruction (e.g. ovarian neoplasm or colorectal neoplasm) and (c) study types capturing views and experiences with at least some qualitative data, such as views and experiences (e.g. views, experiences, semi-structured interviews).
Study selection
Papers identified by the searches were downloaded into Endnote and duplicates removed. Criteria for inclusion/exclusion are summarised in Table 1. Following an initial screen to remove duplicate references and irrelevant articles (paediatric, non-cancer), the titles and abstracts of remaining references were independently dual-screened for inclusion (EB, MM). Disagreements were adjudicated by a third reviewer (SN). Full-text articles were retrieved, independently dual-screened (EB, MM), with a third reviewer available to adjudicate discrepancies (SN).
Inclusion and exclusion criteria.
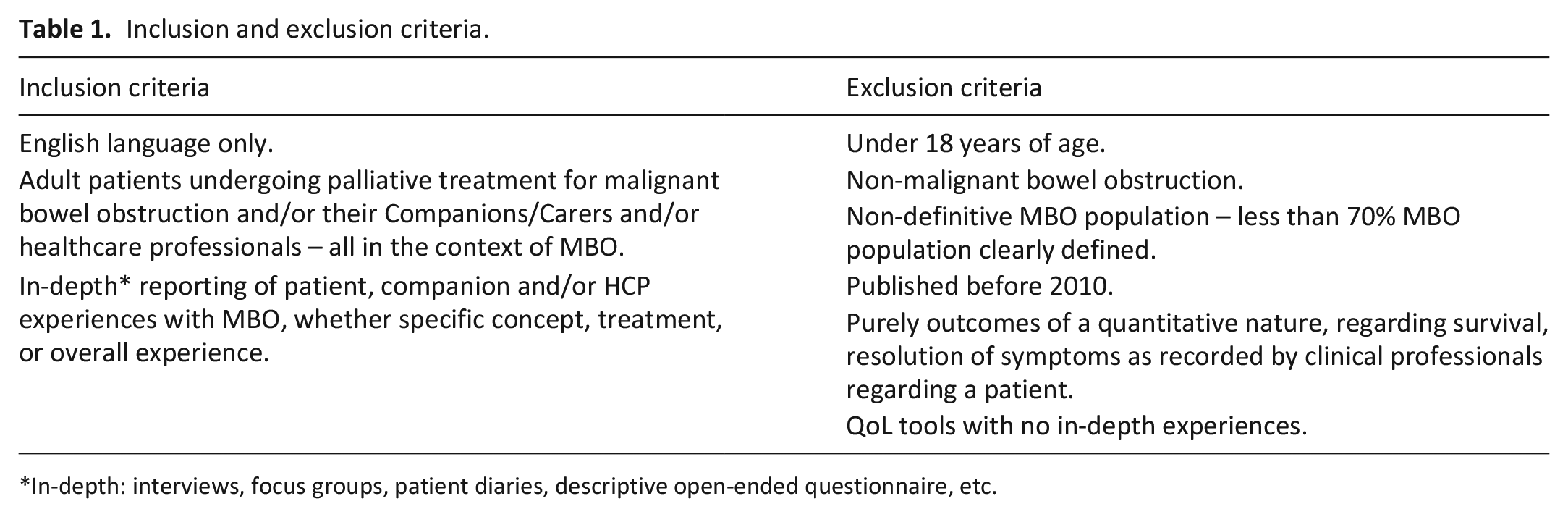
In-depth: interviews, focus groups, patient diaries, descriptive open-ended questionnaire, etc.
Data extraction
A standardised data extraction form was developed (see Supplemental Appendix 2). Data extraction was completed by one reviewer (EB) and checked/edited by a second reviewer (MM). Any differences in the data extraction were resolved through discussion, with an independent reviewer consulted where needed (SN).
Quality assessment
Included studies underwent quality assessment using the appropriate checklist from the Specialist Unit for Review Evidence. 24 Where a number of papers reported the same study, quality was assessed once for the overall study. Qualitative research papers should describe appropriate sampling, data collection and analysis. The checklist included 10 questions, relating to methods, reflexivity and ethical practice. These assessments allowed the reviewer a systematic approach to evaluating the strength and reliability of the evidence (Supplemental Appendix 3). The quality of the included papers were similar, therefore our analysis did not require weighting towards any of the papers.
Data synthesis
In view of the heterogeneity of the included studies, a narrative synthesis approach was used to integrate and describe the results. 25 Data were synthesised by comparing findings from each of the nine papers. The themes identified in the papers were preliminarily grouped, followed by analysis of specific quotations within the themes from each of the papers. These quotes and themes across all nine papers were then grouped by their similarities and their differences, with the final stage being the generation of overarching themes by the reviewers, to group specific elements covered within each of the papers of the views and experiences of patients with malignant bowel obstruction, their caregivers, and healthcare professionals. The empirical data from the ‘results’ or ‘findings’ section in the included studies were extracted and synthesised (EB and MM).
Results
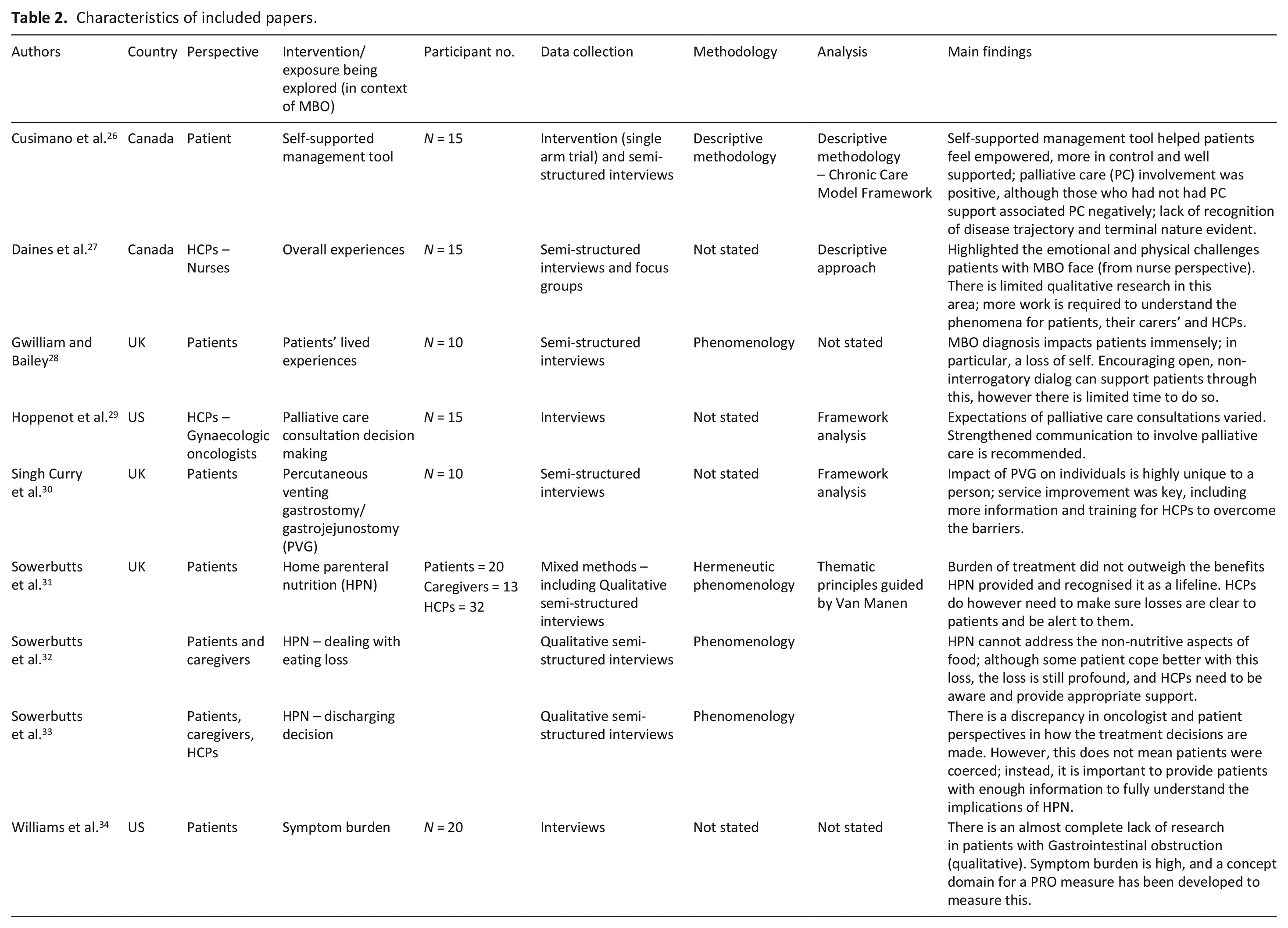
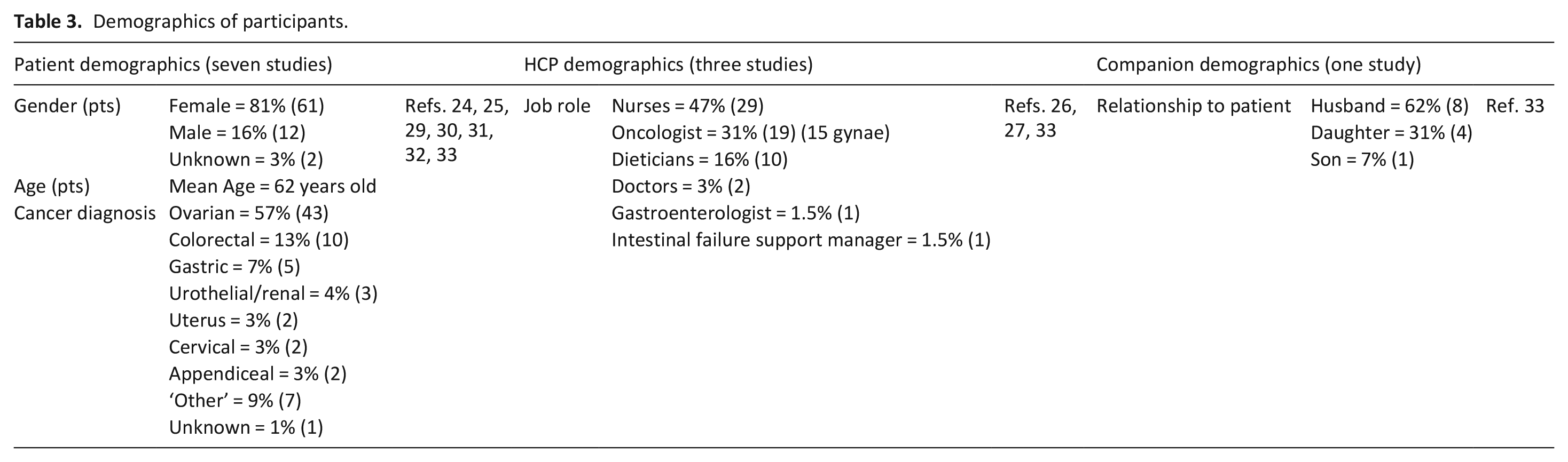
The searches generated 777 papers after removing duplicates and irrelevant articles. The search results, are summarised in a PRISMA flow diagram in Figure 1. Of a total of 16 papers screened for eligibility, seven studies (nine papers) were included in the final narrative synthesis26–34 and are described in Table 2, with a summary of study participants in Table 3. Seven papers were excluded because they did not report in-depth qualitative experiences, but instead described data from validated questionnaires or retrospective clinical note review (n = 6)35–40 and not having English language translation available (n = 1). 41 Major themes and associated subthemes of the included nine papers are summarised in Figure 2 and described in the subsequent results section below. Additional quotations are presented in Table 4.
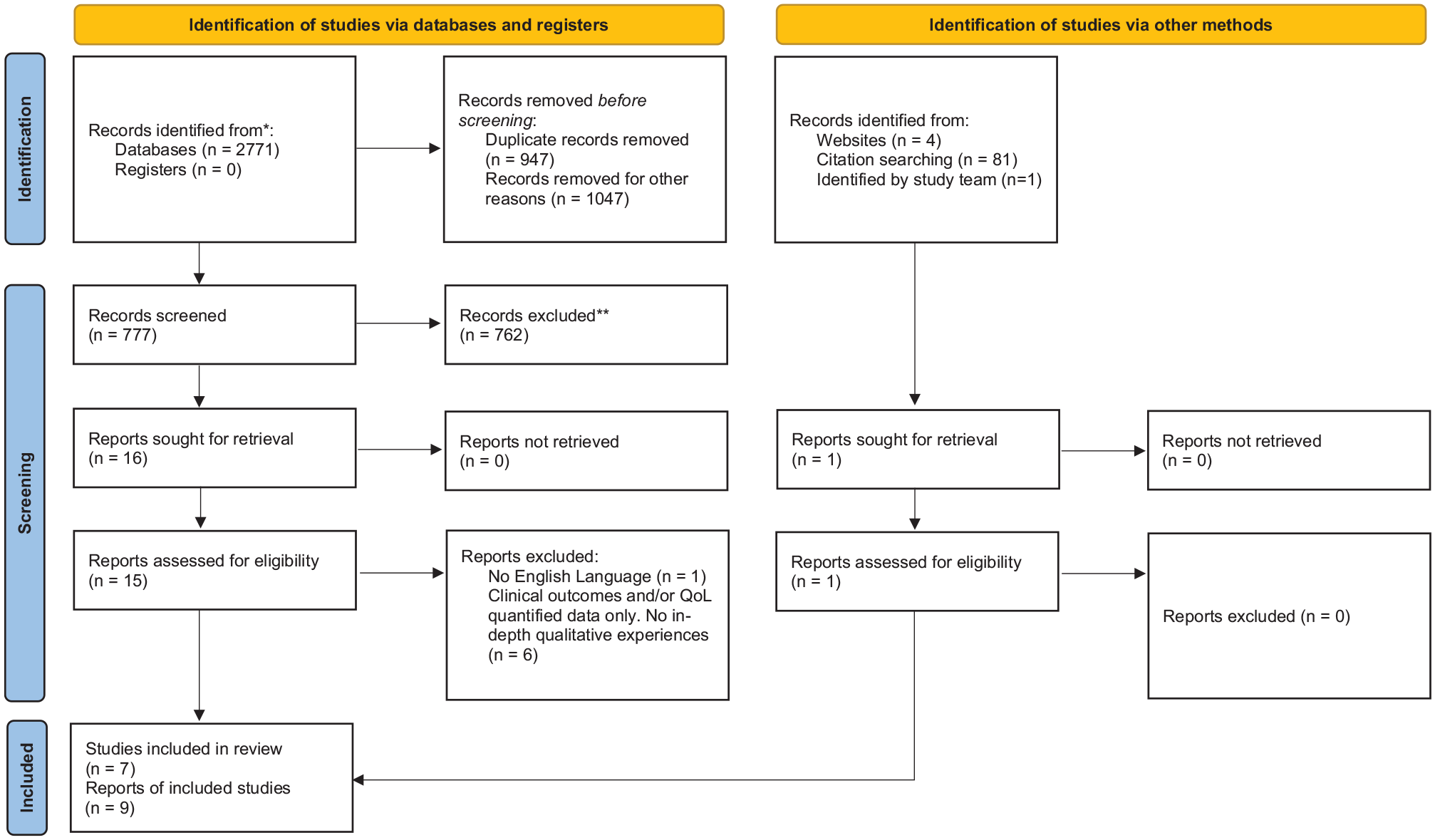
PRISMA 23 flow diagram.
Characteristics of included papers.
Demographics of participants.
Themes and associated sub-themes.
Summary of quotations.
Theme 1: Symptom burden
One paper described symptoms of malignant bowel obstruction in detail; the paper reported that ‘pain’ was mentioned by the majority of patients (18/20 participants), closely followed by ‘vomiting’ (13/20), ‘bloating’ (12/20), ‘discomfort’ (9/20) and ‘nausea’ (8/20). 34 Three other papers described the symptoms of malignant bowel obstruction in less detail but highlighted the debilitating and distressing impact that symptoms had on both patients and families, particularly symptoms of pain, nausea, and vomiting.26,27,29 For example, nurses interviewed 27 in one study identified the far-reaching impacts of these distressing symptoms on not just the patient, but their family members also: “They have pain, discomfort, nausea, vomiting and transcends to the families.” Nurse, page 596. 27 One patient described the pain they experienced as an endless, debilitating feeling “very painful. It consists of like being stuck with a knife or pin, and at times it just goes on and on.” Patient, table 3, 34 while another patient commented on the vomiting they experienced, which resulted in feelings of distress: “As soon as my stomach reached a certain point, I vomited. So, the vomiting was distressing.” Patient, table 3. 34
The data reported in detail that the ‘most common and most distressing’ issue experienced by patients was how malignant bowel obstruction impacted on eating and overall food intake. 29 This was a multifaceted and complex impact of malignant bowel obstruction, viewed as much a social and emotional loss for patients, as being considered a physical issue. Losses included greatly missing the sensation of food: “When I look at those fruit bowls. . ., and I just see these shining grapes and shining nectarines there, I just see myself biting into that nectarine. . .” Patient, page 478, 28 to the isolation felt from being unable to enjoy a meal in a social situation: “I mean, if you can’t do anything else but die, at least you expect to have a few meals with your relatives, don’t you?” Patient, page 476. 28
Fatigue and disturbed sleep were reported by six of the 20 patients interviewed in one paper. 34 Whilst not described explicitly in other papers, several studies reported general ‘weakness’, trouble sleeping and lack of physical energy.28,31,34 A patient from one paper commented on the lack of undisturbed sleep “It would be wonderful if I could have even 5 h sleep without a break.” Patient, page 6, 31 while a patient from another paper described how the pain (from cramps) and lack of food intake contributes to their fatigue: “It’s intense cramps, basically with the effect that you don’t eat, which makes you weaker. Most cramps come at night, so you get very tired. . . The whole process wears you out.” Patient, table 3. 34 However, it was difficult to establish whether these symptoms were symptoms of malignant bowel obstruction, its treatments and their side effects, or from the underlying primary malignancy itself.
While one of the papers 34 was the only paper which focussed on symptoms specifically and in detail, many of the papers identified symptoms of malignant bowel obstruction and its devastating impact. The most commonly expected symptoms, such as nausea, vomiting and pain, were prevalent in the qualitative literature. Other symptoms/side effects included eating and drinking inability, general weakness/fatigue, and inability to have a bowel movement.
Theme 2: Interventions/treatments
Four papers (reporting on two studies), offered patient, caregiver, and healthcare professional perspectives on the following interventions; percutaneous venting gastrostomy/gastrojejunostomy and home parenteral nutrition.30–33 One other paper looked at patients’ experiences of a self-management intervention; an educational tool to educate patients on malignant bowel obstruction. 25
Percutaneous gastrostomy/gastrojejunostomy
Patients described both positive and negative aspects of receiving a percutaneous venting gastrostomy/gastrojejunostomy. All participants experienced reduced or completely resolved nausea and vomiting, with some also reporting reduced pain and abdominal distension: “They explained it would be helpful for the sickness. . . stopping the sickness, which it did. I was so grateful for that because it was just projectile all the time.” Patient, page 385. 30 Another positive aspect of percutaneous venting gastrostomy/gastrojejunostomy insertion was that the nasogastric tube could be removed, thereby improving body image and comfort: “I hated that up my nose because it was so uncomfortable. It hurt me. . .” Patient, page 385. 30
Negative experiences were also described. These included leaking issues, post-procedure pain, anxiety over perceived ‘smells’ and reduced mobility, 31 which one patient described: “You can smell it though, even if it’s not leaking. I feel like. . . it smells like sewage. . .” Patient, page 386. 30 One patient described the ‘freeing’ sensation, when for brief periods, they could remove all the tubes they were attached to: “When I go in the shower and everything I can. . . take both tubes off, and I’m a different person” Patient, page 7. 31 Other negative aspects included patients considering a venting gastrostomy/gastrojejunostomy as a constant presence; some were afraid to eat, for fear of causing a blockage of the tube.31,32
Home parenteral nutrition
Patients viewed home parenteral nutrition as a ‘lifeline’, increasing both survival and quality of life. Patients mentioned being able to be at home, achieve some normality and spend time with family. 31 Healthcare professionals also felt positive towards home parenteral nutrition as an intervention and its benefit: “You are. . . giving precious time to people when there are things that they want to do and HPN allows them to do that.” Palliative Care Nurse, page 4. 33 However, home parenteral nutrition, like percutaneous venting gastrostomy/gastrojejunostomy, came with its challenges and losses. This included a profound loss of normality, limited bodily freedom and energy: “It’s difficult, yeah, especially going upstairs, because I’ve not got much energy.” Patient, page 6, 31 imposed routine and invasion of medical environment into the home. 30 One patient described the experience as more difficult than they anticipated: “It wasn’t as easy as it was made out to be.” Patient, page 7. 31
Other papers highlighted the uncertainty of success and difficulties choosing between treatments. One nurse described the ‘vicious cycle’ of interventions experienced by patients: “It seems like a vicious circle for these patients. . . they end up having all kinds of interventions. . .” Nurse, page 597, 27 whereas an oncologist highlighted the difficulties of presenting intervention options to patients, when the uncertainty of success is so high: “Having to help them decide between two options when there’s no clear answer, the emotional is higher.” Gynaecological Oncologist, table 4. 29
Overall, management of malignant bowel obstruction is described as complex when reported by healthcare professionals and intervention experiences reported by patients are mainly positive for patients in regard to symptom alleviation and perceived quality of life/quantity of life gains; however, all come with their challenges and loss to some quality of life, particularly interrupting their ability to achieve normality through simple daily activities and social interactions.
Theme 3: Impact on patient quality of life
The psychological and emotional toll of malignant bowel obstruction on patients and their family, is considerable. A major contributory factor was the uncertainty of healthcare professionals around unpredictable disease trajectory and life expectancy.
Unpredictability of malignant bowel obstruction
The unpredictable nature of malignant bowel obstruction and its uncertain trajectory led to feelings of powerlessness and fear. 26 The unpredictability of the condition, in particular, waiting around for their obstruction to resolve, or their treatment to come into effect, was a particular source of emotional turmoil within patients.27,28 One patient described their frustrations of waiting for their obstruction to resolve: “I don’t think I could face this week, I think I would go completely off me head, facing up to the weekend, to be told, ‘well, just sit tight, have your fluids.’” Patient, page 479, 28 and one nurse described patients’ worry and uncertainty of what will happen to them when they get home, with no resolution of the obstruction: “Now what’s going to happen when I go home? Am I going to be able to eat? What if I eat and I start to throw up?” Nurse, page 595. 27
One paper also identified deterioration in mental ability, inability to focus, withdrawing from oneself and also disengaging from their loved ones surrounding them: “My ability to construct. . . logical propositions, sometimes, is gone. . . I can’t be sure, when I close my eyes, whether I’m in a real situation or just something I’m thinking about.” Patient, page 478. 28
As mentioned above, fear of the unknown and what will happen next in their trajectory was a source of emotional turmoil and psychological ‘rollercoaster’ of emotions: “I feel so healthy in many ways. But then I will get this obstruction and that changes everything suddenly. It’s scary. It’s a rollercoaster.” Patient, page 478. 26 The ups and downs of the trajectory of malignant bowel obstruction and the uncertainty for healthcare professionals was particularly a source of stress: “Is this going to happen every few weeks? And my doctor said – well it can, but we don’t know for sure. So I might be fine for a while. I don’t know, they don’t know either.” Patient, table 3. 26
Family and social impact
Malignant bowel obstruction impacted on relationships within the family, including family mealtimes and other social activities. One paper highlighted the sense of burden patients feel they are weighing down on their families: “The roles and relationships really change too as they deteriorate and the families have a greater sense of burden having to take on more.” Nurse, page 595. 27 Family mealtimes and most social events revolve around eating and/or drinking, thereby resulting in impacts on the patient and the family.28,32 such as reduced social interactions: “I can’t meet my friends for a drink now and I miss them. . .” Patient, page 478 28 and avoiding family members during mealtimes: “B. has his meals in the kitchen, so I don’t go in there while he’s (eating).” Patient, page 3. 32
Several patients highlighted the social isolation that came with the condition; feeling isolated, whether from their own choice: “I laid on the bed. . . I didn’t want to move, to go in and out like I normally would, to socialise. I had people come up. I wasn’t very amenable. . .” Patient, page 478 28 or due to the way they felt: “You’re sort of isolated, on your own. You’re not, but that’s how you feel. . . you do feel. . . you do feel that you are in a little place, just left on your own.” Patient, page 479. 28
A diagnosis of malignant bowel obstruction has a profound effect on patients, who are coming to terms with a distressing condition, in addition to, and because of their cancer diagnosis. The emotional toll and impact on a patients’ mental wellbeing are overwhelming, and difficult to mitigate, due to the uncertain nature of each individual case of malignant bowel obstruction. The impact of this diagnosis on a patients’ routine, including family and social life, is shown in the literature to have been impacted severely.
Theme 4: Implications of malignant bowel obstruction and its trajectory
The trajectory or clinical course of malignant bowel obstruction is poor and indicates that the underlying cancer is most likely at an advanced stage and progressing. The deterioration can be swift, forcing patients and their families to make decisions promptly and face the limited time that they have left: “Dealing with how long they’re going to be here. . . it makes them reflect and decide what they have to do. . .” Nurse, page 597. 27
Patients appeared to struggle with the lack of instant results and the direction their condition was heading; in particular, the uncertainty even among healthcare professionals managing the condition.26–29,33 For example, one patient described the difficulty in receiving answers from healthcare professionals: “When it’s difficult to get answers. . . and they say. . . ‘we don’t know’ or there’s not answer to it. . . you feel then, that you’re just being discarded.” Patient, page 479. 28
The variability of patients is clear in that patients are highly unique, and healthcare professionals are unable to provide clear or certain information on how the patients’ condition will unfold. This appears to add to frustrations for patients.
Theme 5: Communication
Information regarding malignant bowel obstruction
Patients appreciated nurses’ help making sense of their diagnosis and condition by providing them with support and information: “They’re not just leaving you in the lurch to figure it out yourself but checking if you need anything further or have any questions.” Patient, table 3. 26
Similarly, the previously described self-management tool evaluated in one paper, 26 appeared to address support and information needs: “I have my handouts. . . it’s like my bible. I check it all the time.” Patient, table 3 26 ; it empowered patients and provided them with ways to self-manage: “I learned how to assess bowel movements to determine what is a healthy bowel movement and what is evidence that there’s possibly a problem coming up” Patient, table 3 26 but all the while knowing they instantly had the healthcare professionals’ support. 27
Information regarding proposed interventions
Patients undergoing placement of a percutaneous venting gastrostomy felt that they were given insufficient information prior to the procedure, and that details provided were sometimes conflicting: “. . . when I got down to radiology, Dr X came and explained it all to me and I was even more anxious then because I sort of then understood what was happening. . .” Patient, page 386. 30 Patients also described unrealistic expectations for the intervention, believing percutaneous venting gastrostomy/gastrojejunostomy would lead to full resolution of symptoms, a return to normal eating and prolonged life expectancy. 30
One study, exploring patients’ and caregivers’ experiences of home parenteral nutrition suggested limited understanding of the aims or process of the intervention. It was unclear whether this was due to insufficient provision of information or poor understanding of the information provided. For example, those interviewed underappreciated the complexity of home parenteral nutrition, assuming it would be simpler than they had believed: “I thought it was probably less medical than what it is.” Companion, page 5. 31 However, despite the described complexities and medicalisation, patients were reluctant to stop home parenteral nutrition if it was the only intervention available to them: “When I get to the point where I’ve got to say, ok, enough is enough, it won’t matter then, but until that point comes then I just have to fight, keep going.” Patient, page 8. 31
Overall, communication was perhaps one of the largest covered topics across the included studies. Poor communication was seen as a barrier to effective management, whereas good communication, especially between the whole care team and to the patients themselves, facilitated effective communication and therefore aided effective management and feelings of empowerment and security for patients. Some patients did have issues with information provision, including wanting more information, confusion over their management options, confusion over an intervention and what it entails, and perceived lack of involvement in the final decision for their management.
Theme 6: Goals of care
Healthcare professionals reported the complexities of malignant bowel obstruction, however when they delivered the appropriate combination of interventions, and the patient’s symptoms were controlled, they highlighted the rewarding feeling it provided: “. . . it’s just rewarding when you know that you could help somebody, and you’ve put things in place for them and for them to be comfortable. . .” Nurse, page 596. 27 While some patients still held on to the hope that there may be a cure, most patients reported more realistic goals for themselves, such as being pain free, able to spend time with family (“spending time with family when you get to, like, my stage, is the most important” Patient, page 6) 31 and having a sense of normality: it’s just wanting to get back to normal, if you see what I mean, whatever normal is these days.” Patient, page 4. 32
One study reported that as goals-of-care became complex, oncologists were more likely to involve palliative care: “I do use palliative care a lot when I think the patient and their family and I are just not on the same page at all, because I feel like they’re a good sounding board.” Gynae Oncologist, table 2. 29 However, some felt the complexities surrounding decision making and goals-of-care were too complex to involve an additional care team to the mix: “Because of the complexity of the decision making in the malignant bowel obstruction, I don’t think it’s a great idea to involve another team at the moment. Especially if the patient’s goals are not clear.” Gynae Oncologist, table 3. 29
The complexity of malignant bowel obstruction meant that the decisions for care, goals and treatment options became more complex and the nature and unpredictability of the condition was also a factor in how difficult goals-of-care can be to put forward and stick to: “You also can’t predict completely how things are going to go, so that’s really hard because you want to counsel them appropriately but sometimes things don’t go that way. So, I think the unknown for the patient is really hard, then it makes it hard for you too.” Gynae Oncologist, table 4. 29
Overall, goals-of-care appear to be complex and unique to each individual. However, this is hindered by the complexity of malignant bowel obstruction, its nature and unpredictable trajectory. Patients, for the most part, appeared to have realistic goals for themselves, such as being able to have the energy to meet family, have some normality to their lives and routine, and to be pain and symptom free in order to do this.
Discussion
Main Findings
This narrative synthesis of the qualitative literature offers confirmatory and additional information that can be used to contribute to a wider Delphi process for the development of a core outcome set to evaluate malignant bowel obstruction. Key physical symptoms that informed the Delphi process were pain/discomfort, nausea, vomiting, bloating and fatigue. Other symptoms which may be less readily considered, included distress, which was not only driven by physical symptoms, but predominantly by psychosocial domains. These included practicalities of interventions (percutaneous venting gastrostomy/gastrojejunostomy and home parenteral nutrition), loss of social norms including eating, unpredictability of the condition and the complexities of goals of care.
The findings offer valuable insights into the patients’ views and experience and identify a discordance between symptoms which are of importance to patients and those prioritised by clinicians. Even though therapeutic developments have improved survival for patients with metastatic ovarian and bowel cancer, malignant bowel obstruction remains a serious complication with no emerging new therapeutic options for two decades.42,43
Historically, studies to evaluate interventions for malignant bowel obstruction have focussed on quantitative, clinical outcomes. For example, a systematic review of the use of somatostatin analogues for the management of malignant bowel obstruction, identified six randomised control trials, each with differing primary and secondary end points. 15 The majority of the 45 pre-defined end points focussed on physiological parameters such as volume of gastric secretions, number of vomits per day etc. Whilst some studies relied on patient reported outcomes such as intensity of pain, only one clinical outcome captured data pertaining to quality of life; namely wellbeing. 14
The heterogeneity of these study end points supports a case of need for a standardised set of outcomes, to be used in clinical practice and future research. Furthermore, without some inclusion of patients’ perspectives, it will be difficult to evaluate the clinical relevance of the observations recorded. Pain, in particular, rarely featured as a clinical end point in the somatostatin randomised controlled trials, yet was the most commonly reported symptom across the qualitative studies. This correlates strongly with responses to a screening questionnaire of 37 women with advanced ovarian cancer and radiologically confirmed malignant bowel obstruction where pain, nausea, vomiting and constipation were most consistently reported. 44 In one of the only two published, adequately powered randomised controlled trials, the use of octreotide was associated with an increased requirement for hyoscine butyl bromide and by implication, increased pain. 5 With no statistical difference in the primary end point between the two groups, a greater emphasis on pain, as an outcome, might prompt a rethink about the utility of somatostatin analogues in the management of malignant bowel obstruction.
Another important finding from this review is the level of distress that is associated with a diagnosis of malignant bowel obstruction. Whilst the prognostic implications are well recognised as drivers of distress, it is clear that these worries are exacerbated when different healthcare professionals offer patients and their families mixed messages and inconsistent management plans. The challenges of living with uncertainty are well recognised and ensuring a co-ordinated and consistent approach with malignant bowel obstruction should be considered a minimum standard of care.
Strengths and weaknesses
It is appropriate to recognise the limitations of this review. Of the nine papers reviewed, three focussed on patient experience of symptoms, with the remainder reporting on experiences of parenteral nutrition, venting procedures, clinical decision making and a self-care tool. The review was limited by the timepoint of 10 years, therefore it is possible earlier papers may have been missed. However, we conducted a scoping search, which highlighted the scarcity of qualitative evidence before 2010, which has been further reinforced by the lack of qualitative studies referenced in the included studies’ reference lists, which were hand searched. The one exception was the Gwilliam paper, 28 which was referenced in some of the included studies, so it was decided the paper was to be included in the review due to it being the only qualitative paper referenced specific to malignant bowel obstruction pre-2010. Most importantly, the limited number of relevant qualitative studies illustrates how little the patient voice has been recognised in the evaluation and management of malignant bowel obstruction.
What this study adds
These qualitative data shall contribute to informing the wider study to develop a core outcome set for malignant bowel obstruction, which shall hopefully ensure future studies in the field adopt a standardised system of evaluating and reporting. 19 However, the under representation of patient experience in malignant bowel obstruction studies is of concern and should be addressed as a matter of urgency.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221081331 – Supplemental material for Symptom burden and lived experiences of patients, caregivers and healthcare professionals on the management of malignant bowel obstruction: A qualitative systematic review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221081331 for Symptom burden and lived experiences of patients, caregivers and healthcare professionals on the management of malignant bowel obstruction: A qualitative systematic review by Elin Baddeley, Mala Mann, Alison Bravington, Miriam J Johnson, David Currow, Fliss E M Murtagh, Elaine G Boland, George Obita, Alfred Oliver, Kathy Seddon, Annmarie Nelson, Jason W Boland and Simon I R Noble in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163221081331 – Supplemental material for Symptom burden and lived experiences of patients, caregivers and healthcare professionals on the management of malignant bowel obstruction: A qualitative systematic review
Supplemental material, sj-pdf-2-pmj-10.1177_02692163221081331 for Symptom burden and lived experiences of patients, caregivers and healthcare professionals on the management of malignant bowel obstruction: A qualitative systematic review by Elin Baddeley, Mala Mann, Alison Bravington, Miriam J Johnson, David Currow, Fliss E M Murtagh, Elaine G Boland, George Obita, Alfred Oliver, Kathy Seddon, Annmarie Nelson, Jason W Boland and Simon I R Noble in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163221081331 – Supplemental material for Symptom burden and lived experiences of patients, caregivers and healthcare professionals on the management of malignant bowel obstruction: A qualitative systematic review
Supplemental material, sj-pdf-3-pmj-10.1177_02692163221081331 for Symptom burden and lived experiences of patients, caregivers and healthcare professionals on the management of malignant bowel obstruction: A qualitative systematic review by Elin Baddeley, Mala Mann, Alison Bravington, Miriam J Johnson, David Currow, Fliss E M Murtagh, Elaine G Boland, George Obita, Alfred Oliver, Kathy Seddon, Annmarie Nelson, Jason W Boland and Simon I R Noble in Palliative Medicine
Footnotes
Acknowledgements
This work was supported by Marie Curie core funding of Professors Simon Noble and Annmarie Nelson’s personal chairs. Professor Fliss Murtagh is a National Institute for Health Research (NIHR) Senior Investigator. The views expressed in this article are those of the author(s) and not necessarily those of the NIHR, or the Department of Health and Social Care.
Author contributions
SN, JWB, MJ, FM, DC, GO, EGB, AN and KS were involved in the conception of the study. ALL authors contributed to protocol development. EB, MM and AB led on data collection, analyses, and writing. SN and AN provided supervision and oversight of data collection, analyses, writing and provided adjudication over study inclusion. MJ, FM, DC, GO, EB, AO, KS and JWB provided substantial contribution to the study analyses and writing. All authors read and approved the final manuscript.
Data management and sharing
The data is readily available in supplementary files/appendices.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Marie Curie Research Grants Scheme [grant number MCRGS-20171220-802].
Research ethics and patient consent
The review did not directly involve human participants and therefore required no approval from an ethics committee, however the overarching study that this review is a part of, was reviewed by the Wales Research Ethics Committee 5 (Wales REC 5) on 10th December 2019 (Ref 19/WA/0340).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.