
Abstract
Background:
Fatigue affects most patients living with advanced cancer and is a symptom that healthcare professionals can find difficult to manage.
Aim:
To provide healthcare professionals with a pragmatic overview of approaches to management of fatigue in patients with advanced cancer that are commonly recommended by guidelines and to evaluate evidence underpinning them.
Design:
Scoping review methodology was used to determine the strength of evidence supporting use of interventions recommended in management of fatigue in patients with advanced cancer.
Data sources:
National or international guidelines were examined if they described the management of fatigue in adult cancer patients and were written within the last 6 years (2015–2021) in English. The Cochrane Database of Systematic Reviews (January 2011–December 2021) was searched for ‘cancer’ AND ‘fatigue’ in title, abstract or keywords. A PubMed search was also made.
Results:
Evidence indicates physical exercise interventions are effective and patients may benefit from energy conservation tactics. Evidence does not support use of psychostimulants such as methylphenidate. Limited data were found on efficacy of corticosteroids, psychological interventions, nutritional intervention, sleep optimization or complementary therapies for management of fatigue in advanced cancer.
Conclusion:
We recommend regular assessment, review and acknowledgement of the impact of fatigue. Exercise and energy conservation should be considered. Pharmacological interventions are not endorsed as a routine approach. Many interventions currently recommended by guidelines are not supported by a robust evidence base and further research on their efficacy is required.
The majority of patients with advanced cancer suffer from fatigue.
There are no universally used guidelines for fatigue management in advanced cancer.
Many healthcare professionals are unsure which approach to recommend.
Healthcare professionals wishing to develop an evidence-based fatigue management plan should promote physical activity balanced with energy conservation tactics.
Reversible causes of fatigue should be addressed if appropriate.
We do not recommend that psychostimulant medications such as methylphenidate are used.
Fatigue in patients with advanced cancer should be regularly assessed and reviewed.
Patients may benefit from acknowledgement of their fatigue and provision of information about its potential causes and management.
Additional high quality, large scale studies of efficacy and safety are needed to clarify the role of corticosteroids for fatigue in patients with advanced cancer.
Further research is needed to clarify whether psychological interventions, nutritional intervention, sleep optimization or complementary therapies should be recommended.
Background
Fatigue in cancer patients is ‘a distressing, persistent, subjective sense of physical, emotional and/or cognitive tiredness or exhaustion that is not proportional to recent activity and interferes with usual functioning’. 1 The pathophysiology is not completely understood but contributing factors can be cancer itself, medication and potentially modifiable factors such as anaemia, sleep problems, poor nutrition, physical inactivity and depression. People with advanced cancer rank fatigue as their most important symptom and up to 80% are affected. 2 A large survey of cancer patients (across all stages of cancer) found although 74% reported fatigue, the majority felt they did not get the help they wanted with the symptom. 3 Healthcare professionals can lack confidence to manage fatigue, due to a lack of evidence to guide clinical practice.
In this practice review, we aim is to provide healthcare professionals with a pragmatic overview of the approaches to management of fatigue commonly recommended by guidelines and to examine the evidence-base underpinning them.
Methods
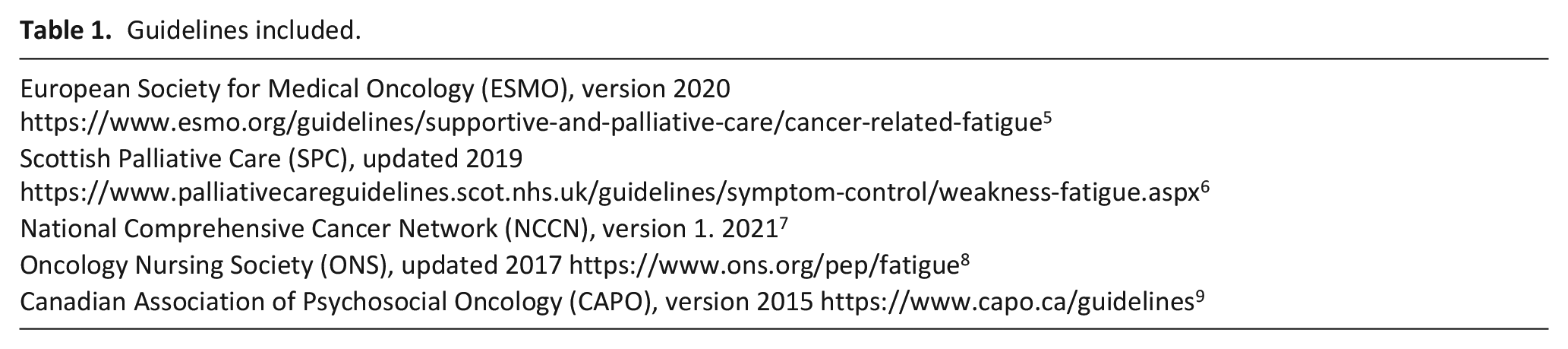
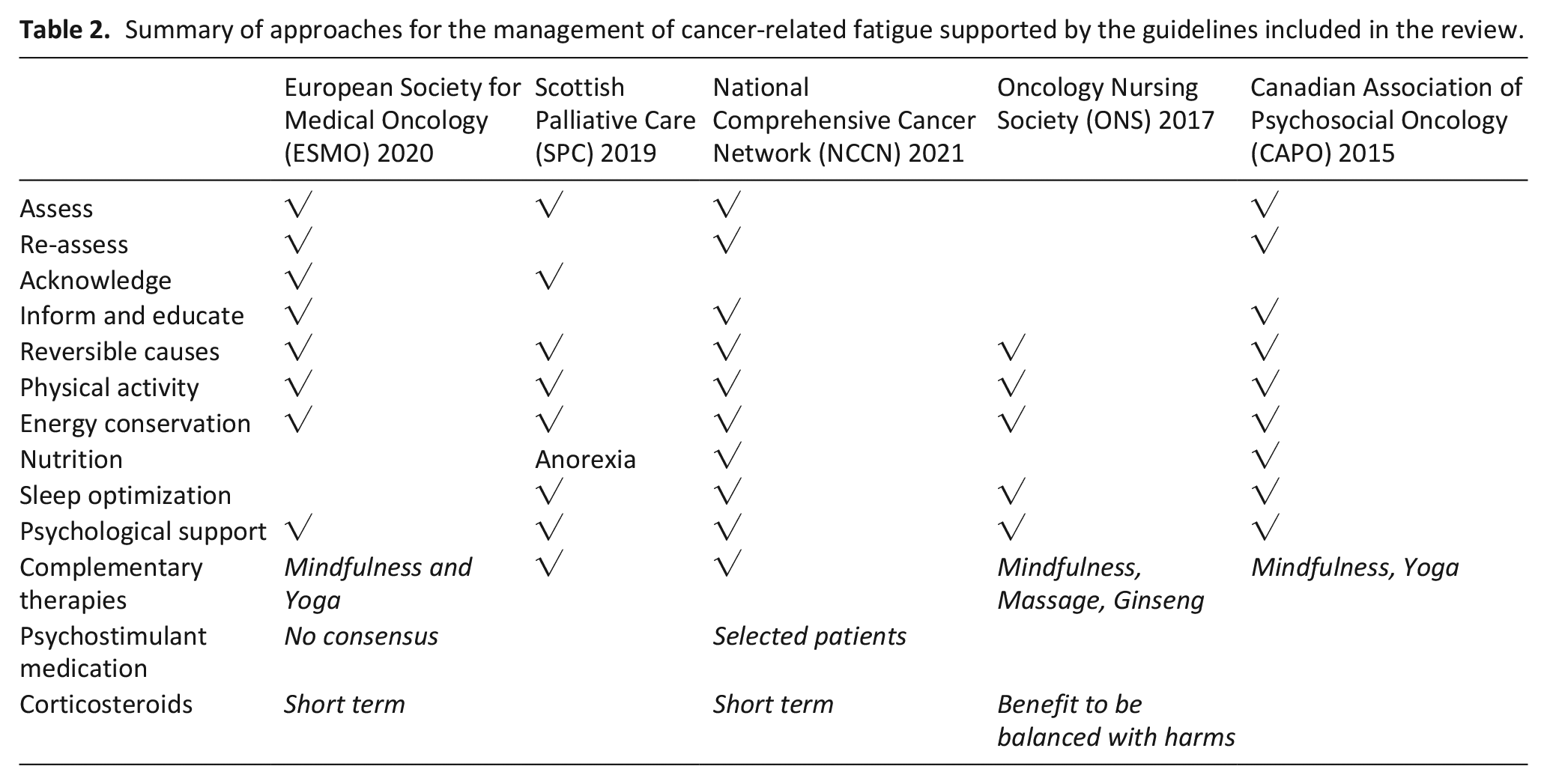
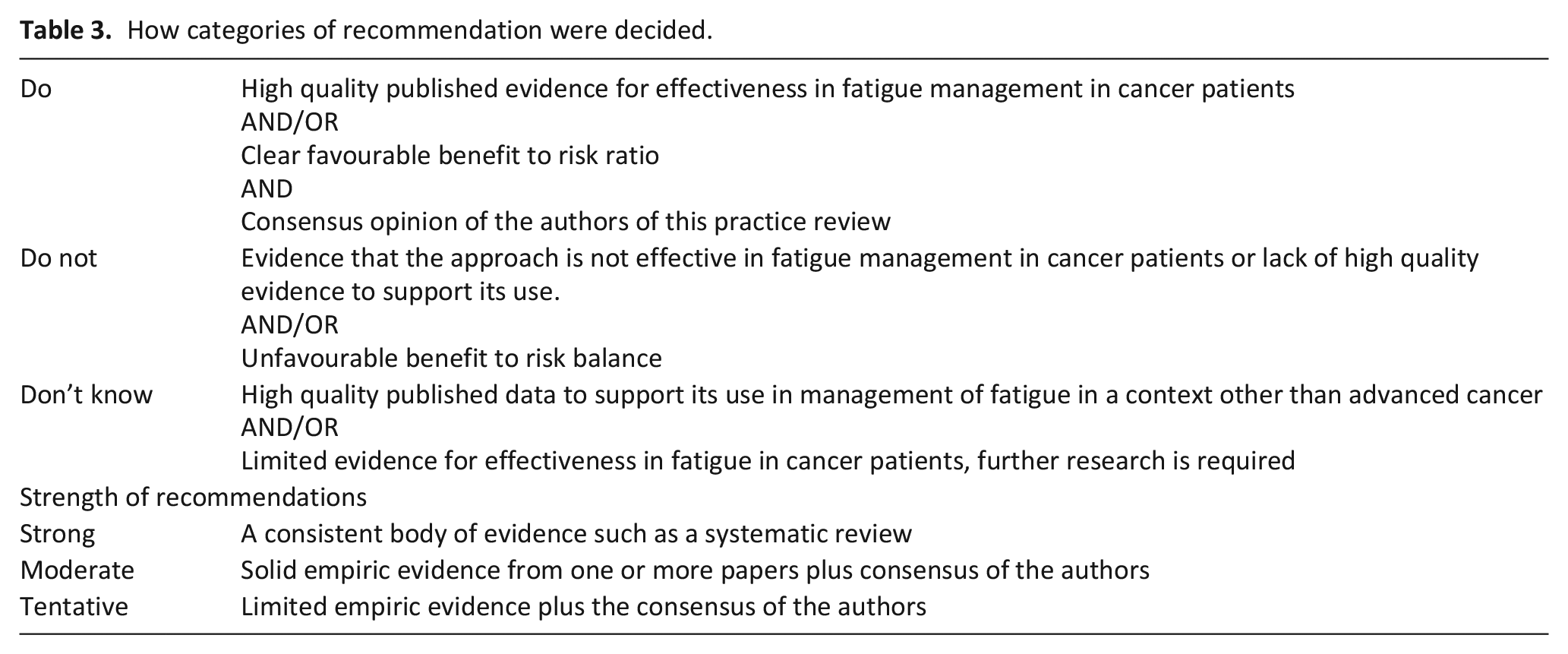
Clinical practice is shaped by guideline recommendations. We examined guidelines from national or international bodies that described the management of fatigue in adult cancer patients and were published within the last 6 years (2015–2021) in English language (Table 1) and identified interventions recommended in the management of fatigue in patients with advanced cancer (Table 2). Scoping review methodology 4 was used to collect evidence supporting the use of these interventions and identify areas where the evidence-base is lacking and further research is required. A search of the Cochrane Database of Systematic Reviews for the terms ‘Cancer’ AND ‘Fatigue’ in the title, abstract or keywords (Last search date 25/6/21, limits: April 2011–April 2021) yielded 68 reviews. PubMed searches were made for further articles to add to the evidence base for the effect of the most common interventions described in the identified guidelines (Search dates: 26/4/11–26/4/21, last search 26/6/21). Search strategies are shown in Supplemental Material 1. Search results were extracted into Excel. Titles and then abstracts were independently screened by EC and EdM and discrepancies resolved by discussion with a third author, if necessary. Selection criteria were articles detailing effect of a guideline-recommended interventions on fatigue in adult patients with incurable, advanced or in palliative care phase cancer. Articles investigating interventions not recommended by selected guidelines; without fatigue as a primary or secondary outcome; describing cancer survivors, patients under active treatment (unless described as palliative), paediatric patients; opinion pieces; protocols or where access to full text was not possible were excluded. Studies or reviews including mixed stages of cancer were excluded unless the advanced cancer patients were >50% of total. Grey literature was not searched. Additional evidence was added if authors identified relevant studies in bibliography of included systematic reviews. A PRISMA flow chart is shown in Supplemental Material 2. Results are presented in compliance with Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist (Supplemental Material 3). Strength of evidence for commonly recommended approaches was considered in accordance with the criteria listed in Table 3 and each intervention allocated to a practice recommendation category of ‘Do’, ‘Do not’ or ‘Don’t know’. Evidence used to inform review recommendations are shown in Supplemental Material 4.
Guidelines included.
Summary of approaches for the management of cancer-related fatigue supported by the guidelines included in the review.
How categories of recommendation were decided.
Results
Guidelines and common recommendations
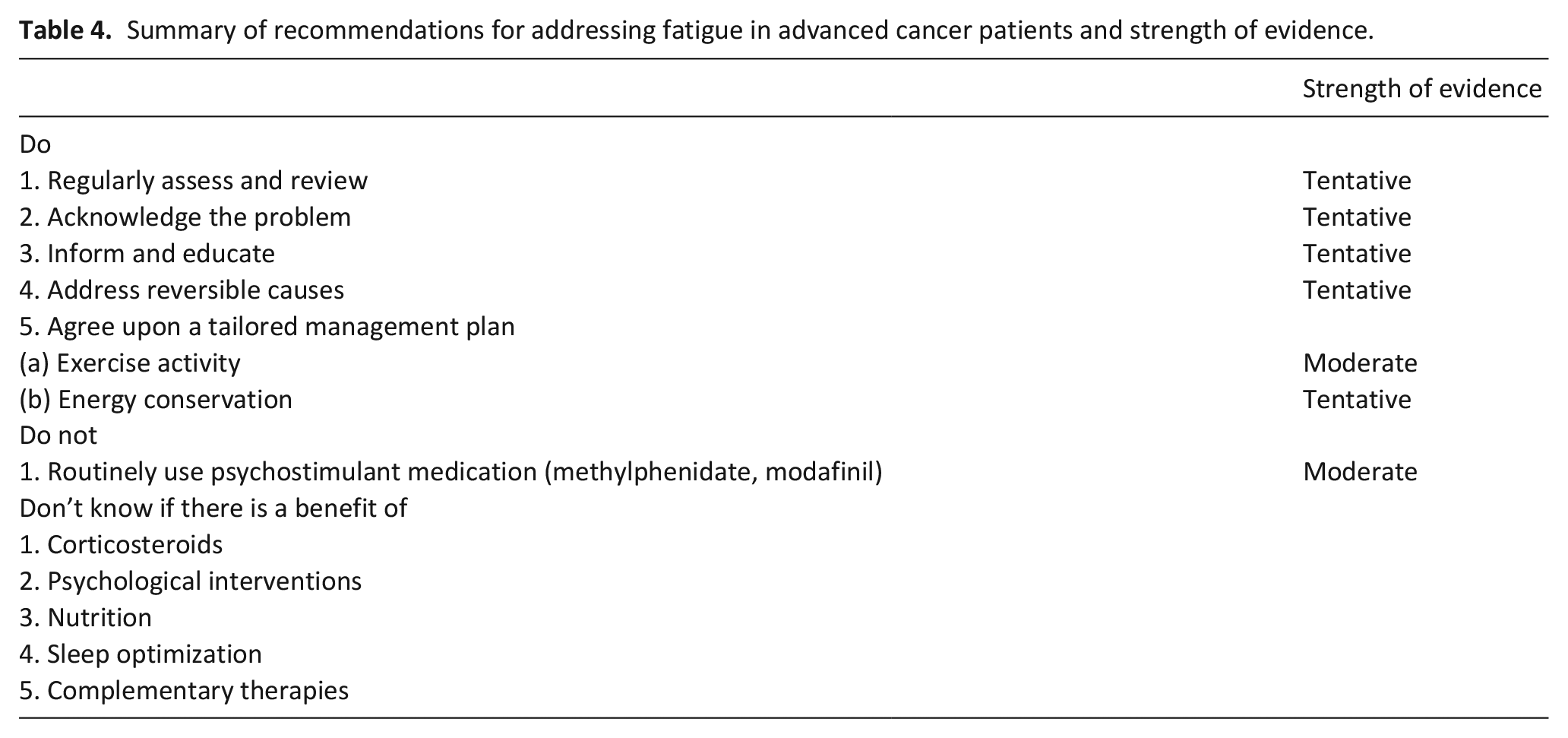
Five relevant guidelines were identified (Table 1) and their recommendations summarized (Table 2). After independent screening by EC and EdM, 37 articles relevant to this review were identified (Supplemental Material 4). Recommendations were categorized according to the criteria detailed as detailed in Table 3 and are summarized in Table 4.
Summary of recommendations for addressing fatigue in advanced cancer patients and strength of evidence.
Practice recommendations ‘Do’
Regularly assess and review (tentative)
Patients should be regularly screened for fatigue followed by a more in-depth assessment for patients with moderate to severe fatigue.5,7,9 Regular monitoring and non-pharmacological patient-tailored treatment did improve fatigue in a study of patients with advanced cancer. 10 We make a tentative recommendation in respect of this limited evidence and the low potential for harm.
Acknowledge (tentative)
Clinicians should acknowledge the burden of fatigue on the patient and their quality of life.5,6 Recent qualitative data shows healthcare professionals in hospice palliative care consider acknowledgement and validation of the impact of the symptom an important step in successfully managing fatigue (Chapman et al., unpublished data).
Inform and educate the patient and people important to them (tentative)
Guidelines recommend that the patient and their families should be informed about possible causes of fatigue and options to manage it1,5,9 and, in light of the limited potential for harm, we support this recommendation as part of good patient-centred care. Formal educational interventions encompass discussion, coaching, goal-setting, feedback and reinforcement to help patients understand and cope with fatigue. They can be delivered face-to-face, over the phone, audiotapes, on-line, as a group or one-to-one. Limited evidence to support the use of formal educational interventions comes from studies of populations of mixed cancer stage. A Cochrane review including 14 randomized controlled trials with a total of 2213 participants found low to moderate quality evidence of a small effect of educational interventions in reducing fatigue, its interference with daily life and fatigue-related distress. 11 The type, delivery modality and timing of educational interventions used in the different studies in these reviews were variable. A recent Cochrane review focussed on telephone interventions for the management of cancer symptoms. 12 Of the included studies, seven were aimed specifically at fatigue, for a total of 895 participants. Although there was some evidence of a significant effect, this was of a very low quality.
Address reversible causes (tentative)
Clinical appraisal of fatigue should consider potentially reversible factors. We specifically searched for analgesia and anaemia as they are common causes. Regular monitoring and patient-tailored treatment of physical symptoms in patients with advanced cancer led to significant improvement of fatigue over time in a small randomized controlled trial. 10 There is some evidence that satisfactory analgesia improves fatigue in patients with severe pain. 13 There is insufficient evidence to support addressing anaemia and in particular the role of blood transfusion as an approach to fatigue management. 14 Overall, evidence supporting the efficacy of addressing reversible factors on fatigue in advanced cancer is limited.
Exercise activity (moderate)
Numerous randomized controlled trials have found a positive effect of aerobic and strengthening exercise on fatigue during and after active treatment.15–18 In patients with advanced cancer, results have been inconsistent or preliminary.19,20 In a review including 16 controlled trials of exercise interventions in advanced cancer (including some patients receiving active treatment), half reported a significant improvement in fatigue 21 and a meta-analysis of 15 randomized controlled trials, which included 13 examining fatigue as a primary outcome, showed a small improvement in fatigue with exercise compared to normal care (Standardized mean difference −0.25; 95% CI −045 to −0.04; p = 0.02). 22 However, another meta-analysis of exercise in advanced solid tumours did not find a significance difference. 23 A physiotherapy programme including exercises, myofascial release and proprioceptive neuromuscular facilitation stretches significantly reduced fatigue in patients with advanced cancer compared with controls. 24 However, a Cochrane meta-analysis of exercise in patients with advanced lung cancer found no significant overall effect on fatigue. 25 Selection of physical activity for patients with advanced cancer will require careful consideration of physical capacity and underlying pathology. Gentle exercise such as walking has been shown to be acceptable and feasible for people with advanced cancer26,27 and preliminary data also suggests the feasibility of supervised aerobic or resistance exercise.28–30 Realistic and staged goals tailored to the individual are necessary to help avoid unachievable targets for physical activity that have the potential to increase psychological distress or exacerbate symptoms.
Energy conservation (tentative)
All guidelines promoted lifestyle adaptation to maximize energy conservation for beneficial activities. Patients might be advised to plan, pace and prioritize their daily tasks and activities. We make a tentative recommendation in advanced cancer based on low potential for harm coupled to some evidence of efficacy and feasibility in other cancer and chronic disease contexts.31–33
Practice recommendations ‘Do not’
Pharmacological
Psychostimulants (moderate)
Currently, we recommend psychostimulants should not be routinely used due to a lack of high-quality evidence to support their effectiveness in patients with advanced cancer. A 2010 Cochrane review combined results of five studies conducted with patients at various cancer stages found a small but significant effect of methylphenidate versus placebo. 34 However, subsequent updates to this in 2015 and 2020 concluded there was insufficient evidence to recommend any specific drug treatment for fatigue in palliative care. Interventions considered included; psychostimulants, corticosteroids, donepezil, selective serotonin reuptake inhibitors, acetylsalicylic acid, megestrol acetate, alfacalcidol and acetyl-L-carnitine. 35 Recently, a small double-blind study reported a superior effect of methylphenidate compared to placebo, 2 and 5 hours after administration 36 but methylphenidate was also shown not to be superior to placebo in randomized controlled trials, as an individual intervention 37 or in combination with a nursing telephone intervention. 38 A further randomized controlled trial of methylphenidate is currently open (https://doi.org/10.1186/ISRCTN79478762) and results are awaited. Previously, high quality randomized controlled trials had found that modafinil 39 was not superior to placebo in cancer-related fatigue.
Practice recommendations ‘Don’t know’
Corticosteroids
Begley et al. 40 reviewed use of corticosteroids for fatigue in people with advanced cancer. Four included studies reported an improvement in symptoms of fatigue but there were limitations in the quality of the data and studies evaluated mostly short term use. Some other randomized controlled trials support the use of corticosteroids to manage fatigue in patients with advanced cancer, 41 whereas others do not. 42 In light of mixed conclusions and that little evidence is available regarding optimal dose and duration of treatment, in accordance with European Society for Medical Oncology, National Comprehensive Cancer Network and Canadian Association of Psychosocial Oncology guidelines and considering the potential for adverse effects, our position is that further evidence is needed to clarify whether there is a benefit of routine or long term use of corticosteroids. Corticosteroids might be considered for short term use in selected patients, such as people whose fatigue strongly impacts on quality of life and other approaches have failed.
Psychological support
Psychosocial support is recommended by all guidelines examined but evidence is mixed. A Cochrane systematic review and meta-analysis of 12 studies, including 535 participants receiving cancer treatment with palliative intent, did not show an improvement in fatigue after psychosocial intervention. The review examined approaches such as cognitive behavioural therapy, expressive therapy and energy conservation with activity or sleep management. However, quality of studies was evaluated as very low due in part to small sample size. 43 A systematic review of diverse psychotherapeutic interventions for women with advanced breast cancer was unable to conclude the effect on fatigue, due to lack of evidence. 44 Four relevant studies were included in a recent systematic review of acceptance and commitment therapy, with non-significant changes in fatigue reported. 45
Nutrition
Anorexia occurs in the majority of patients with advanced cancer and decreased nutritional intake can be a cause of distress for informal carers and patients.46,47 A small randomized controlled trial reported a significant improvement in fatigue in cachexic patients receiving a nutritional supplement in addition to nutritional and exercise counselling. 48 Oral nutritional supplements improved European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 score for fatigue, −16.3 ± 7.1 versus 2.93 ± 5.88 for non-intervention group in a small trial of pancreatic and bile duct patients (most of whom were receiving palliative chemotherapy). 49 In a systematic review of combined nutritional and exercise support in patients with incurable cancer, there was low quality evidence of improvement in fatigue. 50 In light of a lack of large-scale research to support the role of nutrition in modulating fatigue in advanced cancer, we make a ‘Don’t know’ recommendation. Professionals should reiterate to patients and families that supporting eating and drinking has varying roles including providing patients with enjoyment and social interaction.
Sleep optimization
Sleep disturbance has been correlated with fatigue in patients with advanced cancer. 51 In patients with advanced cancer, sleep may be targeted by interventions designed to target symptom clusters 52 but evidence is mixed as to whether this correlates with improved fatigue.53,54 It is currently unclear whether intervening improve sleep would improve fatigue in people receiving palliative care for with advanced cancer.
Complementary and alternative medicine
The guidelines examined specifically recommended mindfulness, massage and Ginseng and we conducted searches for evidence supporting these. Overall, quality of research studies included in reviews of complementary therapies is often limited, and very few studies recruited only patients with advanced cancer. A small feasibility study of art-based mindfulness in 10 hospitalized patients with advanced cancer found a medium effect on fatigue. 55 However, another pilot study in outpatients with advanced cancer found no effect on tiredness. 56 There remains a lack of high quality evidence to evaluate the role of massage to relive fatigue in advanced cancer. 57 Despite some evidence supporting its use in patients undergoing treatment, Panax Ginseng was not superior to placebo in a double-blind randomized trial in patients with advanced cancer, 58 and, interestingly, both treatment and placebo resulted in a perceived significant benefit.
Limitations
This was a practice review produced using scoping review methodology, therefore a systematic review of the full evidence base for each intervention was not performed. The quality of evidence sources was not appraised. There may be additional guidelines and relevant literature that we have not examined.
Conclusions
Managing fatigue in advanced cancer patients requires an individually tailored multimodal approach. This review may assist healthcare professionals in recommending evidence-based approaches and aid discussion of options for fatigue management with patients. Current evidence supports screening for fatigue and acknowledging its impact upon the patient and people important to them. Potentially reversible causes should be considered, including minimizing adverse effects of existing medications. Evidence supports routine use of physical exercise and lifestyle adaptations to maximize energy conservation. Current evidence indicates that psychostimulants should not be routinely prescribed. Evidence is lacking to make recommendations regarding, corticosteroids, psychological, nutritional or formal educational interventions, sleep optimization or complementary therapies.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211046754 – Supplemental material for Practice review: Evidence-based and effective management of fatigue in patients with advanced cancer
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211046754 for Practice review: Evidence-based and effective management of fatigue in patients with advanced cancer by Emma J Chapman, Erica Di Martino, Zoe Edwards, Kathryn Black, Matthew Maddocks and Michael I Bennett in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163211046754 – Supplemental material for Practice review: Evidence-based and effective management of fatigue in patients with advanced cancer
Supplemental material, sj-pdf-2-pmj-10.1177_02692163211046754 for Practice review: Evidence-based and effective management of fatigue in patients with advanced cancer by Emma J Chapman, Erica Di Martino, Zoe Edwards, Kathryn Black, Matthew Maddocks and Michael I Bennett in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163211046754 – Supplemental material for Practice review: Evidence-based and effective management of fatigue in patients with advanced cancer
Supplemental material, sj-pdf-3-pmj-10.1177_02692163211046754 for Practice review: Evidence-based and effective management of fatigue in patients with advanced cancer by Emma J Chapman, Erica Di Martino, Zoe Edwards, Kathryn Black, Matthew Maddocks and Michael I Bennett in Palliative Medicine
Supplemental Material
sj-pdf-4-pmj-10.1177_02692163211046754 – Supplemental material for Practice review: Evidence-based and effective management of fatigue in patients with advanced cancer
Supplemental material, sj-pdf-4-pmj-10.1177_02692163211046754 for Practice review: Evidence-based and effective management of fatigue in patients with advanced cancer by Emma J Chapman, Erica Di Martino, Zoe Edwards, Kathryn Black, Matthew Maddocks and Michael I Bennett in Palliative Medicine
Footnotes
Authorship
Emma J Chapman (EC) is a senior research fellow in the Academic Unit of Palliative Care; Erica Di Martino is a research fellow in the Academic Unit of Primary Care; Zoe Edwards (ZE) is a senior research fellow in medicines optimization and a pharmacist; Kathryn Black (KB) is a research nurse at St Gemma’s hospice; Matthew Maddocks (MM) is a reader and specialist physiotherapist; Michael I Bennett (MIB) is the St Gemma’s professor of palliative medicine, director of the St Gemma’s Academic Unit of Palliative Care at the University of Leeds. Original idea by EC and MB. Identification of guidelines and preparation of manuscript by EdM, EC and KB. The Cochrane database of systematic reviews was independently screened by EC and EdM. All authors contributed content to the review, developed consensus on practice recommendations and revised the final submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Yorkshire Cancer Research programme grant L412, RESOLVE ‘Improving health status and symptom experience for people living with advanced cancer’.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.