
Abstract
Background:
Pain of a moderate or severe intensity affects over half of patients with advanced cancer and remains undertreated in at least one-third of these patients.
Aim:
The aim of this study was to provide a pragmatic overview of the evidence supporting the use of interventions in pain management in advanced cancer and to identify where encouraging preliminary results are demonstrated but further research is required.
Design:
A scoping review approach was used to examine the evidence supporting the use of guideline-recommended interventions in pain management practice.
Data sources:
National or international guidelines were selected if they described pain management in adult cancer patients and were written within the last 5 years in English. The Cochrane Database of Systematic Reviews (January 2014 to January 2019) was searched for ‘cancer’ AND ‘pain’ in the title, abstract or keywords. A MEDLINE search was also made.
Results:
A strong opioid remains the drug of choice for treating moderate or severe pain. Bisphosphonates and radiotherapy are also effective for cancer-related bone pain. Optimal management requires a tailored approach, support for self-management and review of treatment outcomes. There is likely a role for non-pharmacological approaches. Paracetamol should not be used in patients taking a strong opioid to treat pain. Cannabis-based medicines are not recommended. Weak opioids, ketamine and lidocaine are indicated in specific situations only.
Conclusion:
Interventions commonly recommended by guidelines are not always supported by a robust evidence base. Research is required to evaluate the efficacy of non-steroidal anti-inflammatory drugs, anti-convulsants, anti-depressants, corticosteroids, some invasive anaesthetic techniques, complementary therapies and transcutaneous electrical nerve stimulation.
Pain is not adequately controlled in all patients with advanced cancer.
There are no universally used guidelines for the treatment of pain in patients with advanced cancer.
Not all guideline recommendations are evidence-based.
We provide a pragmatic overview of the current ‘state of the science’ supporting pain management practice.
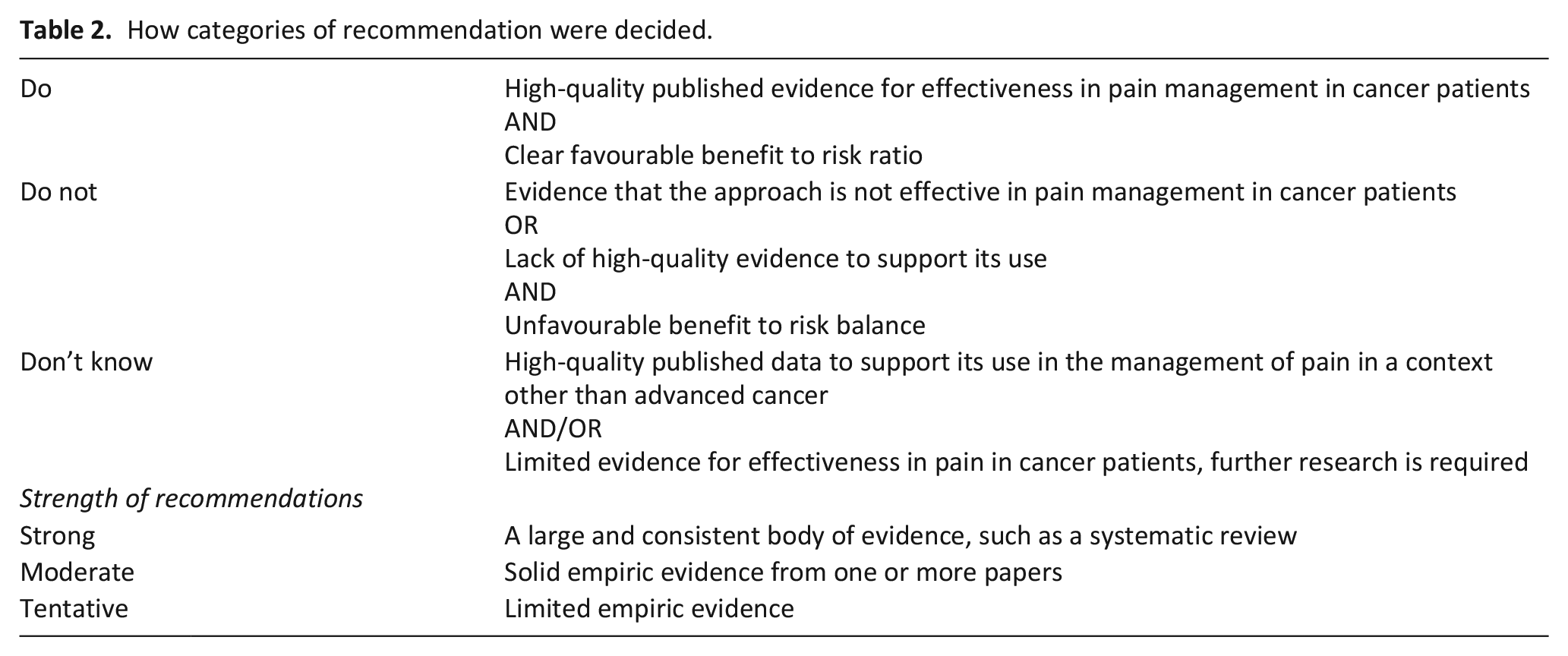
‘Do’ and ‘Do not’ practice recommendations are made based upon a set of strength recommendations, that is, strong: a large and consistent body of evidence, such as a systematic review, moderate: solid empiric evidence from one or more papers and tentative: limited empiric evidence, a strong recommendation cannot be made.
Interventions are categorised as ‘Don’t know’ where there is currently a lack or paucity of high-quality empiric evidence to support the approach in management of cancer pain but some evidence to suggest that the approach is effective in a non-cancer context. These are interventions where further research is required before the routine use of the practice can be recommended.
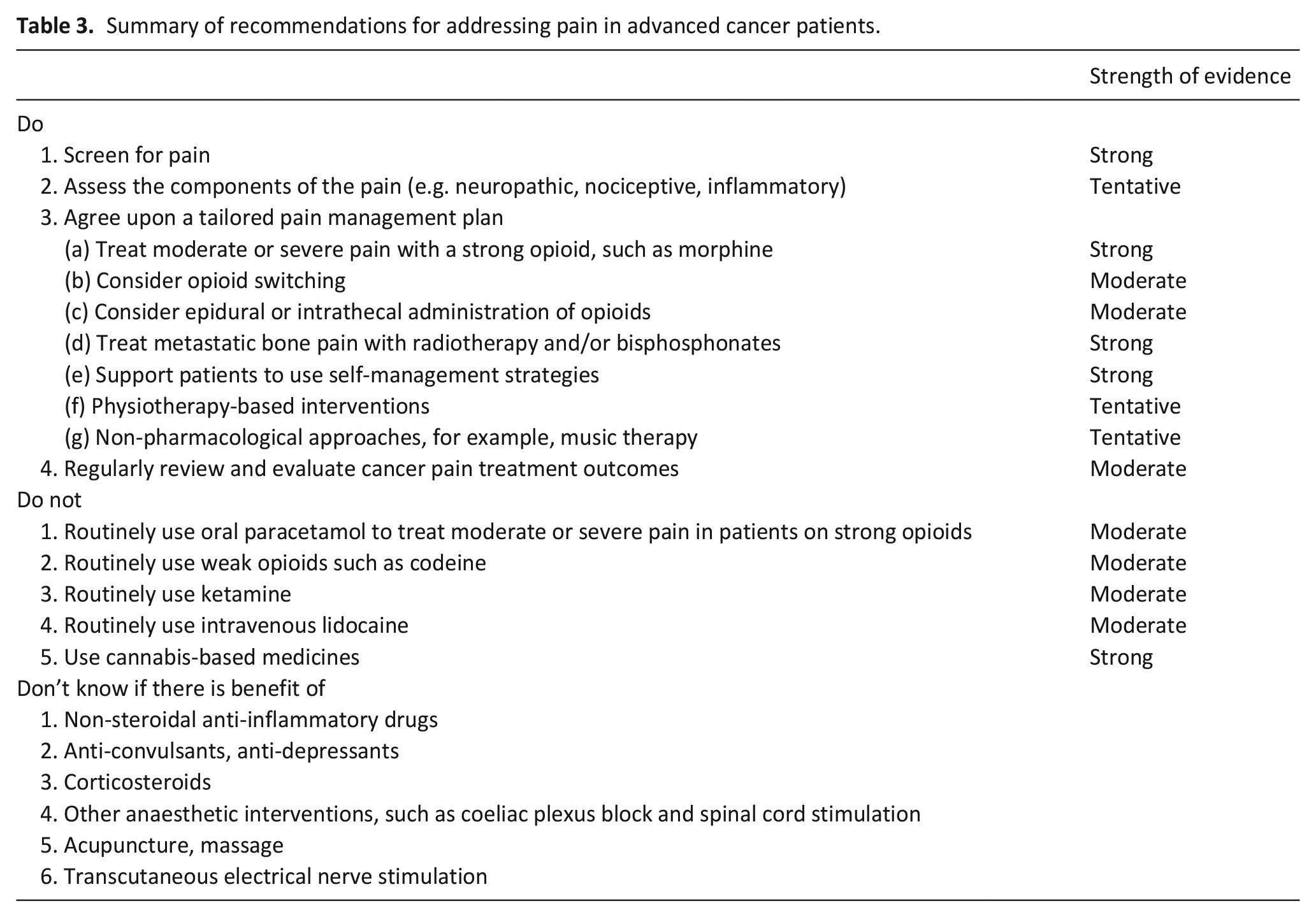
An oral strong opioid remains the drug of choice for treating moderate or severe pain in patients with advanced cancer and should be supplemented with bisphosphonates and/or radiotherapy for bone pain. Optimal management requires a tailored approach, support for self-management and regular review of treatment outcomes. There is likely a role for non-pharmacological approaches.
Oral paracetamol should not routinely be used for patients who are already taking a strong opioid to treat moderate-to-severe pain. Cannabis-based medicines are not recommended. Weak opioids, ketamine and lidocaine are only indicated in specific situations.
Further research is required into the use of non-steroidal anti-inflammatory drugs, anti-convulsants, anti-depressants, corticosteroids, some invasive anaesthetic techniques, acupuncture, massage and transcutaneous electrical nerve stimulation.
Introduction
Pain is of a moderate or severe intensity in more than half of patients with advanced cancer 1 and is undertreated in around one-third of cases. 2 Poorly controlled pain is the most common cause for community-based cancer patients to contact out-of-hours primary care services 3 and is one of the most frequent reasons for their hospitalisation. 4 Although home is the preferred place of care and death for many patients, 5 national surveys show that this is where pain control is poorest. 6 However, accessing specialist palliative care improves pain management for patients living at home. 7
There are no standardised guidelines for the management of pain in patients with advanced cancer and not all guideline recommendations are evidence-based. We set out to provide a pragmatic overview of the state of science supporting approaches commonly recommended by key guidelines rather than produce a novel consensus guideline. We also identified where encouraging preliminary results have been demonstrated but further research is required before the routine use of the practice can be recommended.
Methods
This practice review, guided by scoping review methodology,8,9 was used to determine the extent of the evidence supporting the use of interventions in the management of pain in patients with advanced cancer. Guidelines from national or international bodies were selected if they described the management of pain in adult cancer patients and were written within the last 5 years in English language (Table 1). The Cochrane Database of Systematic Reviews (January 2014 to January 2019) was searched for the terms ‘cancer’ AND ‘pain’ in the title, abstract or keywords. After independent screening by two researchers, 19 articles were identified as relevant to this review. An additional search of MEDLINE was made for further key publications that provided additional primary data to add to the evidence base for the interventions considered in Table 1 (search date: 31 May 2019). Methods were compliant with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist (Supplementary Material 1). We determined the strength of evidence for commonly recommended interventions plus some non-pharmacological approaches for which there is currently limited evidence but a low potential for harm. Each intervention was then allocated to a practice recommendation category of ‘Do’, ‘Do not’ or ‘Don’t know’ based on the direction and strength of the supporting evidence (Table 2). A ‘strong’ recommendation was made where there was evidence from a large and consistent body of evidence, such as a systematic review, a ‘moderate’ recommendation was made in light of solid empiric evidence from one or more papers and a ‘tentative’ recommendation where there was limited empiric evidence. Where ‘tentative’ evidence supports use of an intervention, the likely increased risk to the patient is considered (Table 3).
Guidelines examined and their position on the interventions recommended by this practice review.
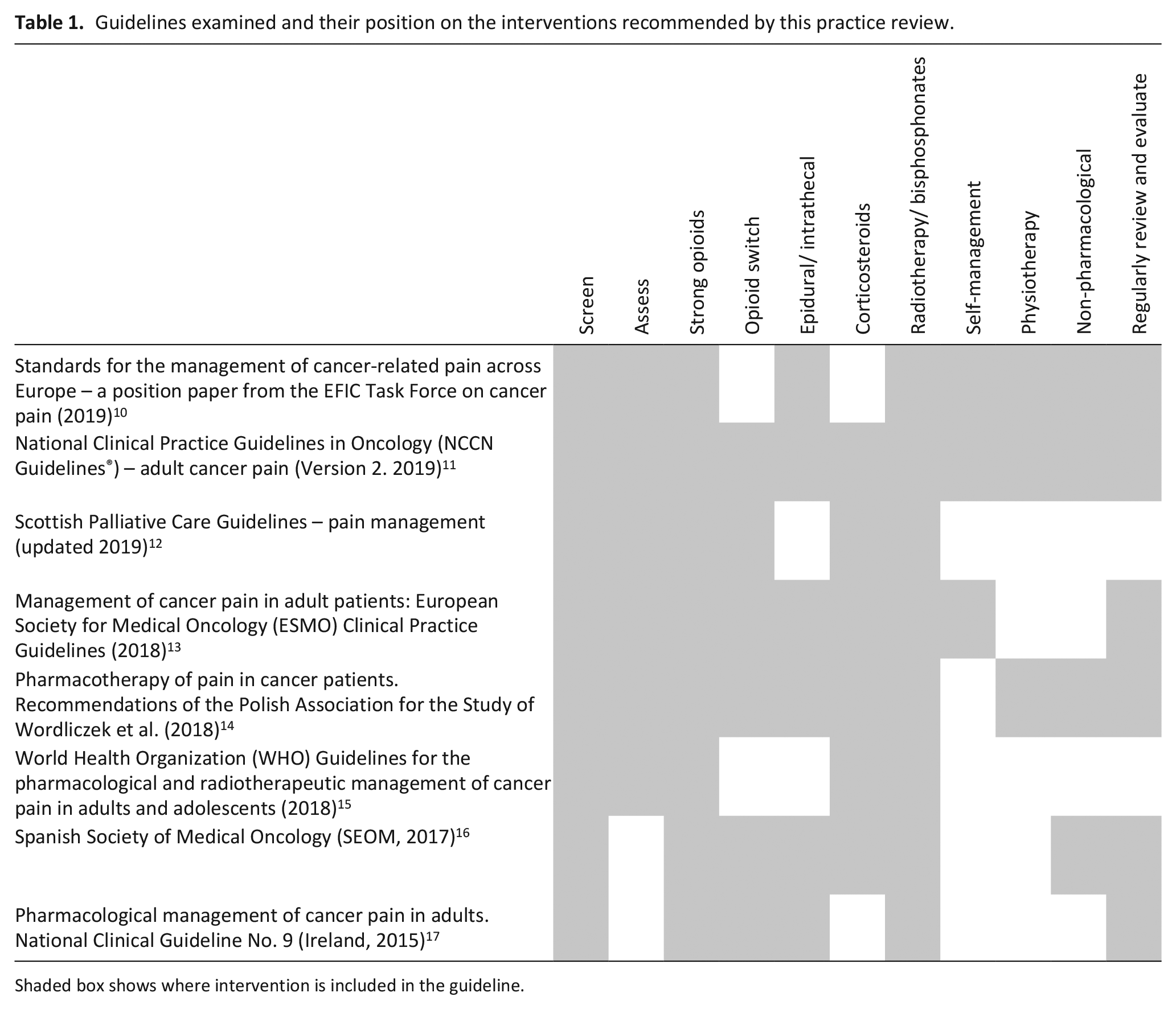
Shaded box shows where intervention is included in the guideline.
How categories of recommendation were decided.
Summary of recommendations for addressing pain in advanced cancer patients.
Practice recommendations – ‘Do’
Screen for pain at every engagement with a healthcare professional
All guidelines examined recommend that patients should be screened for pain10–15,17 and at every engagement with a healthcare professional. 10 Meta-analysis shows that using patient-reported measurements of pain reduces pain intensity in cancer patients perhaps by prompting discussion about symptoms between patient and professional. 18 A large, randomised trial found that integration of a systematic bedside pain assessment tool into cancer care improves pain outcomes. 19
Assess the components of the pain
It is widely recommended that assessment should include classification of the type and pathophysiology of the pain.10–14 Aetiology, mechanisms and impact of cancer pain should be evaluated and this information used to inform the treatment plan. 10 Identification and grading 20 of neuropathic pain are of particular importance as it is a predictor of poor pain management outcome in cancer patients. 21 A tentative recommendation is made due to the potential benefit and low risk of harm yet a lack of high-quality evidence to support a role for pain assessment in increasing efficacy of treatment.
Agree upon a tailored pain management plan
Treat moderate or severe pain with a strong opioid
Morphine remains the first-line treatment for moderate-to-severe cancer pain; all commonly used oral or transdermal opioids have similar efficacy.22,23 However, less than half of patients who die of cancer are prescribed a strong opioid, and this occurs around median 9 weeks before death.24–26 Patients with inadequately managed pain may benefit from referral to specialist palliative care at an early stage, as a longer duration of specialist palliative care is associated with increased access to opioids and improved quality of life indicators. 27
Consider opioid switching
Switching to an alternative opioid28–32 is recommended if there is inadequate pain relief or unacceptable side effects.11,12,13,14,16,17 Evidence to support opioid switching is of moderate strength, better pain relief or reduced side effects were reported in 50% of patients who switched due to sub-optimal response to another opioid in a recent four-arm, phase-IV randomised controlled trial (RCT). 33 Of note, methadone has similar analgesic actions as morphine 34 but a long and unpredictable plasma half-life, which can lead to problems with accumulation and toxicity. Methadone should only be used for cancer pain under the guidance of specialist palliative care professionals.
Consider epidural or intrathecal opioids
Spinal or epidural administration of opioids or implanted intrathecal pumps is advocated.10,11,13,14,16,17 The evidence to support this from two RCTs is judged as moderate, the complexity of running trials in this group of patients is acknowledged.35–37 Implantation of a spinal opioid infusion requires access to a specialist pain management team for ongoing review and follow-up and careful consideration of fitness to undergo the procedure in patients with end-stage cancer.
Treat metastatic bone pain with radiotherapy, bisphosphonates or both
Metastatic bone pain can be treated with radiotherapy or radioablation.11,12,13–17 A meta-analysis of RCTs found that around 60% of patients with uncomplicated bone metastases experienced pain relief in response to external beam radiotherapy and up to a quarter of these reported complete pain relief within 3–4 weeks. 38 Use of bisphosphonates is recommended11,13–17 and this treatment has a role in reducing skeletal morbidity in metastatic disease. 39 Bisphosphonates may delay the onset of pain but there was no evidence of an analgesic effect in a systematic review. 40 However, a more recent randomised multicentre trial (not included in the systematic review) provided good evidence that ibandronate had similar efficacy to radiotherapy. 41
Support patients to use self-management strategies
Supporting self- management involves helping patients make the decision to manage their pain, enhance their self-efficacy by solving problems and incorporate pain-relieving strategies into daily life. 42 Interventions that support self-management behaviour are infrequently recommended by guidelines but evidence shows that they are effective in pain control.43–48 Good communication, in particular, about opioids is key to maximising patient compliance with and therefore efficacy of treatment. 49
Consider physiotherapy-based interventions
Physiotherapy and rehabilitation medicine approaches include physical exercise (walking and home-based resistance exercises), myofascial release and proprioceptive neuromuscular facilitation techniques and are associated with reduced pain intensity in a pilot RCT, a large randomised trial of telerehabilitation, and as a symptom co-existing with fatigue.50–52
Non-pharmacological approaches, for example, music therapy
Non-pharmacological approaches are recommended.10,11,14,16 Music-based interventions had a significant effect on pain intensity based on low-quality evidence from seven studies analysed in a Cochrane systematic review. 53 Where no adverse effects have been reported, we make a tentative suggestion to consider non-pharmacological approaches, such as music therapy, as part of a holistic management plan.
Regularly review and evaluate treatment cancer pain treatment outcomes
Multiple guidelines10,11,13,14,15,16 recommend that pain intensity and its management plan should be regularly reviewed to assess treatment outcome and plan onward care. Moderate evidence shows that review and evaluation of cancer pain management at the service level improves care and allows comparison between different services for example, hospices, community services and hospitals.54,55
Practice recommendations – ‘Do not’
Routinely use oral paracetamol to treat moderate or severe pain in patients on strong opioids
Paracetamol is currently recommended for mild-to-moderate pain in guidelines based upon World Health Organization (WHO) guidance and the classic ‘cancer pain ladder’.11–13,14,15,16,17 However, patients with moderate-to-severe cancer pain that is already being treated with a strong opioid are unlikely to gain any additional benefit. A Cochrane systematic review found that there is no evidence that using paracetamol alone or in combination with opioids is of any benefit in treating cancer pain. 56 Furthermore, Cochrane systematic reviews also find high-quality evidence of no effect compared to placebo in non-cancer lower back pain 57 and recently osteoarthritis. 58 However, single-dose intravenous paracetamol is effective in acute post-operative pain 59 and may offer benefits in acute cancer pain, but this needs to be substantiated.
Routinely use weak opioids, such as codeine
Moderate-quality evidence from a Cochrane systematic review shows that there is only a little, low-quality evidence for the use of codeine in cancer pain 60 and the effectiveness of this step only lasts for about a month after which patients need to move to a strong opioid to gain sufficient analgesia. 61 In an open-label RCT of moderate cancer pain, low-dose morphine had an earlier and more adequate analgesic effect than weak opioids and a similar tolerability. 62 Nevertheless, in low resource countries and/or where morphine use may be limited, a weak opioid could still be a suitable choice for moderate pain.
Routinely use ketamine
Some guidelines include the option to use ketamine10,11,14,16 but acknowledge the lack of evidence to support its routine use. A Cochrane systematic review concluded that there was insufficient evidence to determine the benefits and harms of ketamine as an adjuvant to opioids. 63 Oral ketamine was neither superior to placebo in a RCT of patients with cancer-related neuropathic pain 64 nor when used subcutaneously as an adjunct to opioids in a randomised, double-blind, placebo-controlled study in patients with cancer pain. 65 However, ketamine should not be completely ruled out as a third-line approach because of its effectiveness in non-cancer, acute pain contexts.66,67 Ketamine might be of benefit in specific situations, such as patients with central sensitisation. 68
Routinely use intravenous lidocaine
There is limited data that intravenous lidocaine may reduce pain intensity in some patients69,70 but a lack of efficacy has been seen in other trials. 71 Use of lidocaine comes with a risk of frequent adverse effects and therefore specialist supervision is needed. Lidocaine could therefore be considered as an option for the treatment of opioid-refractory cancer pain as recommended by some guidelines.11,17
Use cannabis-based medicines
Pre-clinical experiments show that tetrahydrocannabinol (THC) enhances the anti-nociceptive effect of morphine, 72 and preliminary studies indicated a role as an adjuvant treatment for pain in cancer patients. 73 However, larger, RCTs of cannabis-based drugs as an adjuvant to standard treatment in advanced cancer patients have not confirmed any benefit.74,75 A recent systematic review 76 also concluded that very weak evidence suggests no effect of THC or oromucosal nabiximols on cancer pain that is not relieved by strong opioids.
‘Don’t know’
Further research is needed in patients with moderate and severe cancer pain because it is not clear if there is benefit of the following.
Non-steroidal anti-inflammatory drugs
Although non-steroidal anti-inflammatory drugs (NSAIDs) are recommended by guidelines,11–15,17 a Cochrane systematic review found that there is no high-quality evidence to determine their place in the management of cancer pain. 77 There is some evidence for a beneficial effect in other types of pain78,79 yet considering the potential for significant adverse effects, it is important to assess and carefully reassess the use of NSAIDs. 13 RCT’s evidence is urgently needed.
Anti-convulsants, anti-depressants
Despite evidence of effectiveness of anti-convulsants and anti-depressants in non-cancer contexts, 80 there is only very limited evidence of efficacy in cancer patients. 81 A systematic review and meta-analysis found that combining anti-convulsant drugs (gabapentin or pregabalin) with opioids did not improve pain relief in cancer patients compared with opioids alone. 82 The authors noted that due to heterogeneity of patients, a beneficial effect in some patients with neuropathic pain cannot be discounted. Currently high-quality evidence to support their use is lacking and the benefit to risk balance is unclear.
Corticosteroids
Multiple current guidelines recommend corticosteroids for some types of cancer pain,11,12,14–16 particularly where pain is related to inflammation and oedema. Evidence for their efficacy is weak, although a Cochrane systematic review found that some studies showed a beneficial effect on cancer-related pain after 1 week of treatment. 83 In light of the many well-documented adverse effects, 84 the likely benefit to risk ratio for the individual needs careful consideration.
Other anaesthetic interventions
Guidelines recommend that nerve blocks, cordotomy and spinal cord stimulation are considered in specific situations, such as refractory pain11,13,16 or as adjuvant therapy. 12 Currently there is not enough good-quality evidence to judge whether spinal cord stimulation is superior to pharmacological treatments in regards to safety and efficacy for management of pain in advanced cancer patients.35,85 RCTs are needed but the difficulty of conducting them in the relevant population is acknowledged.
Acupuncture, massage
NCCN recommend that massage and acupuncture should be considered alongside pharmacologic interventions. 11 Systematic reviews found that there is insufficient evidence to recommend the use of acupuncture 86 or massage 87 for relief of pain in cancer patients. Patients are often keen to explore complementary and integrative therapies and report a beneficial effect. Considering, the low potential for harm, further robust research into the efficacy of complementary therapies should be considered.
Transcutaneous electrical nerve stimulation
Transcutaneous electrical nerve stimulation (TENS) is categorised as an integrative intervention 11 or adjuvant therapy. 12 There is currently not enough evidence to recommend that TENS can be used for cancer pain in general or in advanced cancer patients due to a lack of power and undersizing in the studies published. 88 As a relatively simple, portable, non-invasive intervention with high safety profile, TENS merits further research in effectiveness trials.
Limitations
Limitations are acknowledged in that as this was a practice review produced using scoping review methodology, a systematic review of the evidence base for each intervention was not performed. There may be additional current guidelines and relevant primary literature that we have not examined. The source and direction of the evidence, for example, conclusion of the systematic review, was considered but the quality of evidence for each original study was not re-appraised.
Summary
After comprehensive assessment of the patient, a strong opioid remains the drug of choice for treating moderate or severe pain in patients with advanced cancer. Treatment with bisphosphonates, radiotherapy or both for bone pain is effective. Optimal management requires a tailored approach, support for self-management and regular review of treatment outcomes. Interventions commonly recommended by international guidelines are not always supported by a robust evidence base. Oral paracetamol should not be used in patients already taking a strong opioid to manage moderate or severe pain. Cannabis-based drugs are not recommended due to evidence of lack of effect. Future research should focus on defining the efficacy of NSAIDs, anti-depressants, anti-convulsants, corticosteroids and the likely role for non-pharmacological approaches in management of pain in patients with advanced cancer. Data are needed to support the appropriate selection of patients who might benefit from third-line approaches, such as lidocaine and ketamine.
Supplemental Material
Chapman_Supplementary_File_1_R1 – Supplemental material for Practice review: Evidence-based and effective management of pain in patients with advanced cancer
Supplemental material, Chapman_Supplementary_File_1_R1 for Practice review: Evidence-based and effective management of pain in patients with advanced cancer by Emma J Chapman, Zoe Edwards, Jason W Boland, Matthew Maddocks, Lucy Fettes, Catherine Malia, Matthew R Mulvey and Michael I Bennett in Palliative Medicine
Supplemental Material
Chapman_Supplementary_File_2_R1 – Supplemental material for Practice review: Evidence-based and effective management of pain in patients with advanced cancer
Supplemental material, Chapman_Supplementary_File_2_R1 for Practice review: Evidence-based and effective management of pain in patients with advanced cancer by Emma J Chapman, Zoe Edwards, Jason W Boland, Matthew Maddocks, Lucy Fettes, Catherine Malia, Matthew R Mulvey and Michael I Bennett in Palliative Medicine
Footnotes
Author contributions
Original idea, identification of guidelines and preparation of manuscript was done by E.J.C. and M.I.B.; the Cochrane Database of Systematic Reviews was independently screened by E.J.C. and Z.E; all authors contributed content to the review and revised the final submission.
Notes on contributors
Dr Emma J Chapman is a Senior Research Fellow in Palliative Care; Zoe Edwards is a Research Fellow in Medicines Optimisation and Pharmacist; Dr Jason W Boland is a Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine; Dr Matthew Maddocks is a Senior Lecturer and Specialist Physiotherapist, Ms Lucy Fettes is a Physiotherapist with experience of Pain Management Programmes in Palliative Care; Ms Catherine Malia is a Nurse Consultant at St Gemma’s Hospice, Leeds; Dr Matthew R Mulvey is a University Academic Fellow, with an interest in neuropathic pain; Prof. Michael I Bennett is the St Gemma’s Professor of Palliative Medicine, Director of the St Gemma’s Academic Unit of Palliative Care at the University of Leeds and an internationally recognised expert in Pain Management.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Yorkshire Cancer Research Programme (Grant No. L412) – ‘RESOLVE: Improving health status and symptom experience for people living with advanced cancer’.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.