
Abstract
Background:
Managing medications can impose difficulties for patients and families which may intensify towards the end of life. Family caregivers are often assumed to be willing and able to support patients with medications, yet little is known about the challenges they experience or how they cope with these.
Aim:
To explore patient and family caregivers’ views of managing medications when someone is seriously ill and dying at home.
Design:
A qualitative design underpinned by a social constructionist perspective involving interviews with bereaved family caregivers, patients and current family caregivers. A thematic analysis was undertaken.
Setting/participants:
Two English counties. Data reported in this paper were generated across two data sets using: (1) Interviews with bereaved family caregivers (n = 21) of patients who had been cared for at home during the last 6 months of life. (2) Interviews (n = 43) included within longitudinal family focused case studies (n = 20) with patients and current family caregivers followed-up over 4 months.
Results:
The ‘work of managing medications’ was identified as a central theme across the two data sets, with further subthemes of practical, physical, emotional and knowledge-based work. These are discussed by drawing together ideas of illness work, and how the management of medications can substantially add to the burden placed on patients and families.
Conclusions:
It is essential to consider the limits of what it is reasonable to ask patients and families to do, especially when fatigued, distressed and under pressure. Focus should be on improving support via greater professional understanding of the work needed to manage medications at home.
Keywords
Managing medications at home can be a complex task involving ordering, collecting, organising, storing and taking medications correctly.
Medication work must take place alongside ongoing management of household tasks, the physical and emotional labour of caring for someone who is dying and the impending loss of that person.
Family caregivers are often assumed to be willing and able to take on the role of supporting patients to manage their medications at home, yet many are themselves older adults with serious health problems or adult children with many other conflicting roles and responsibilities.
Knowledge of the ways that managing medications add to the considerable burden of care and work that must be undertaken when someone is seriously ill and dying at home.
Family caregivers are increasingly expected to undertake complex and technical medication tasks formerly carried out by professionals, but with little if any training, supervision or support; this trend has been exacerbated by COVID-19.
The work of managing medications is critical to enabling patients to remain at home at the end of life.
Health care professionals will benefit from a greater understanding of the complexities of medications management undertaken by patients and families in order to identify and tailor the support they can provide.
Substantial reduction in the complexity and bureaucracy of Health and Social Care services is needed for them to can be navigable for patients and families managing medications at the end of life.
The lack of presence of Community Pharmacists in this research suggests there may be a greater role for them in supporting patients and families to manage medications at home.
Background
The tasks of managing medications in the home are complex and various and can impose substantial practical and lifestyle difficulties for patients and their families.1–7 These tasks include attending appointments, keeping track of medication use, ordering prescriptions, organising and storing medications in the home, developing an understanding about the purpose, use, dose and side effects of medications as well as taking medications, as and when, prescribed.1,8–10 In conjunction with this practical work many patients and their families contend with an emotional burden resulting from concerns about loss of health, personal autonomy and the adverse effects and potential toxicity of taking powerful medications over the long term.11,12 These elements can be exacerbated towards the end of life when the number of medications prescribed may increase.13,14 Even with moves towards deprescribing15–17 there can still be considerable ‘potentially inappropriate prescribing’ and ‘problematic polypharmacy’.13,18,19
Research evidence has reported that up to 50% of patients do not take their medication as prescribed.20,21 However, accounts of how patients and family caregivers undertake the work of medications management suggest that non-adherence is often unintentional rather than deliberate and may be a common consequence of attempts to manage complex medication regimens.1,20–22 Adhering to a medication regimen becomes increasingly difficult towards the end of life whilst confronting the considerable challenges and vulnerabilities of old age, serious illness, frailty and incapacity within a bewilderingly complex and bureaucratic health system.1,6,18,23 Some of the pragmatic challenges faced by patients managing their medications at home are highlighted in Notenboom et al’s 4 study. Their participants, aged 70 and over, identified a number of issues around physically taking medication, handling packaging as well as reading and understanding instructions for use and how this impacted on adherence. 4 Brown and Bussell 20 highlight the problematic nature of the term ‘adherence’ as it presumes the patient is a passive consumer who agrees with the medication regimen. The term does not encapsulate the complexity of the relationships between patients and prescribers, the practical and lifestyle issues that medications may impose on patients nor the limitations of their understanding of their regimen. 20
It is often assumed that family caregivers are available, able and willing to take on the burdens and responsibilities of supporting patients to manage their medications.2,24,25 Professional focus on medication prescribing and adherence may result in a lack of awareness of the concerns which patients and family caregivers frequently have about medications, and the burden and practical difficulties involved in taking them.6,23,24 Our literature review of carers’ experiences of managing medications for patients dying at home identified that family caregivers face increasing demands of care, but there is limited professional knowledge or understanding of the challenges they experience, how they cope with these, or how they can best be supported. 24 Drawing on previous work by Corbin and Strauss 26 and Cheraghi-Sohi et al. 27 we use the concept of ‘work’ to frame the interpretations of our findings around the nature and extent of medications management required by patients and family caregivers towards the end of life.
This paper draws on findings from an NIHR funded UK study to explore the management of medications for patients who are approaching end of life. 28
Design
The study employed a qualitative design underpinned by a social constructionist perspective.29,30 Data reported in this paper were generated across two data sets (1) semi-structured single interviews with bereaved family caregivers, and (2) interviews included within longitudinal case studies31,32 with patients and current family caregivers. The interviews with bereaved family caregivers were reflective accounts across the whole experience including their relative’s death. Comparatively, the use of case studies allowed the examination of the complexities of real-world situations from a variety of perspectives.32,33 Rather than a cross-sectional snapshot provided by single interviews, longitudinal follow-up permitted exploration of experiences and processes over time. The underlying premise was to include those people taking a key role in the management of medications at home, hence it is important to note that each ‘case’ was different. This paper presents data from the patient and family caregiver interviews.
Setting
The study took place in two English counties of similar size and demographic makeup with a range of urban and rural areas, levels of affluence, ethnicity and population age and density. In both counties, palliative care was provided by generalist and specialist palliative care teams, in peoples’ homes and in the hospice setting.
Data sets
1. Single interviews
Participants: Bereaved family (or friend) caregivers.
Eligibility: Bereaved caregivers of patients who had been cared for at home during a substantial part of the last 6 months of life.
Recruitment: Bereaved family caregivers were identified through GP practices, palliative care registers, hospices and via community and specialist palliative care team caseloads. They were approached between 8 weeks and 6 months after the death of their relative by a healthcare professional known to them. Having been given an information pack, they were then able to contact the research team directly or return a reply slip if they were interested in taking part.
2. Interviews included within longitudinal case studies
Participants: Current family caregivers and patients were interviewed as part of family focused case studies and followed-up over a period of up to 4 months.
Eligibility: Patients were recognised as likely to be in the last 6 months of life and to be experiencing issues with medications management. Where appropriate, current family caregivers (including friends) were nominated by the patient as someone taking a key role in supporting their medication management.
Recruitment: Patients were identified by a member of their clinical team. A purposive sampling strategy was applied to promote recruitment of a socially diverse sample of patients with a range of conditions and their family caregivers. Clinical teams were asked to focus on patients who have one or a combination of: more than 10 medications prescribed; are using more than one route of administration; have multiple PRN or ‘as needed’ medications, are using opioids, have management aids for their medications, are known to be struggling with compliance or managing medications at home.
A ‘case’ was considered to be a patient and one or more family caregivers. However, the flexible nature of the qualitative case study approach meant that each case was different. Where a patient did not wish, or was not able, to take part directly (e.g. because of poor health) the key participant was a family caregiver, and patients could participate without a caregiver. The number of follow-up interviews varied. For example, in one ‘case’ a patient with Motor Neurone Disease, his son and wife took part in a joint interview. During the follow-up phase, the son initiated some email correspondence and when his father subsequently died, he offered to continue participating and took part in a further telephone interview.
Data collection and recording
Single, semi-structured interviews were conducted with bereaved family caregivers to explore their experiences and perspectives of looking after their deceased relative and the management of their medications. All interviews were conducted face-to-face, predominantly in their own homes, with two conducted at the University.
The key participant in each case study was interviewed once and, in most cases also on at least one further occasion over a period of 3–4 months. This could be the patient, or the family caregiver, and in some cases, both, in joint interviews. All interviews took place in participants’ own home and were predominantly face-to-face. However, one patient chose to participate solely by telephone and two follow-up interviews with family caregivers were also conducted in this way.
EW, GC, NT and KP carried out data collection between August 2017 and November 2018. An interview schedule was used as a guide and all interviews were tailored to the individual. Participants gave written or recorded verbal consent. With permission, all interviews were recorded. We experienced one failed recording of a telephone interview with a case participant where the recorder was not properly connected, and one other case participant requested not to be recorded. Comprehensive field notes were made after each interview.
Analysis
All interviews were transcribed verbatim and fully anonymised. The qualitative software programme NVivo12© was used to facilitate a thematic analysis of the data sets based on the principle of constant comparison.29,34 For each data set analysis was carried out through an initial process of open coding. At least two team members coded each transcript. As each case was singular with variable composition, a narrative account was developed to provide a clearer view of the key elements in participants’ living situation, care input, support and medications. Data from follow-up interviews enabled understanding of how medications at end of life were managed over time. Within the case studies the parallel data sets, that is of patient and family caregivers, were subject to separate, then comparative analysis. Cross case comparison was also undertaken.
EW, GC and KP developed individual coding frames for each data set through an iterative process of reading, coding and discussion of the data to identify, compare and link ‘themes’ occurring within data sets. The legitimacy of categories was reviewed with the wider project team. Several transcripts were also read and coded by our Patient and Public Involvement (PPI) co-applicant (Alan Caswell) for an additional perspective, transparency and comparison. An example case study was reviewed and themes discussed by six members of the University Faculty PPI group and in June 2019 findings were presented at two workshops for healthcare professionals and members of the public for feedback and comment. Once themes were established for each data set a more refined and selective process was undertaken to explore, differentiate, reorganise and relate the themes. A process of comparison across the data sets was then undertaken. This process explored similar and disparate themes to enable an understanding of the key issues relating to medication management for families and the degree of difference, overlap and mutual understanding that existed between the two data sets. This cross-data analysis highlighted the similarities in the identified themes resulting in some reconfiguration, merging and renaming to establish one of the key themes as ‘work’ and its four subthemes presented below.
Ethical approval
NHS Research Ethics Committee (REC) approval was obtained in March 2017 (Rec Ref: 17/EM/0091).
Ethical issues
The key ethical issue for this study centres on the potential for vulnerable participants to experience the research as distressing or intrusive. The study was carried out by researchers with considerable experience in qualitative data collection in palliative and end of life care. At all times participants were aware that they could stop, pause or withdraw from the interview. There is increasing evidence that participants affected by serious illness can find research interviews to be a positive experience.35–37 Researchers remained sensitive to participants’ emotional expression throughout the interviews. However, there were no instances when participants expressed a wish to stop an interview or when it was felt necessary to provide individuals with additional support.
Results
Participants were 21 bereaved family caregivers: 15 women and 6 men, predominantly spouses of patients who had been cared for at home (Table 1). Thirteen of the patients described in the bereaved family caregiver interviews had a primary diagnosis of cancer, although multi-morbidities were common and a wide range of conditions were represented including Heart Failure, Renal Failure, Dementia, Diabetes, Parkinson’s disease and stroke.
Bereaved family caregiver’s relationship to the patient (n = 21).
A total of 20 case studies were completed involving single interviews with 13 patients and 15 family caregivers, and a further 15 interviews with the patient and one or more family caregiver together (total n = 43). All but three of the patients in our study lived with a family caregiver who supported their care and medication needs. In 7 of the 20 cases the family caregiver was the key participant in the study. The 20 case studies focused on the care of 12 males and 8 females and included 3 male and 16 female family caregivers. Characteristics of the cases, including patient demographics and number of interviews per case are summarised in Table 2.
Case characteristics and number of interviews per case.
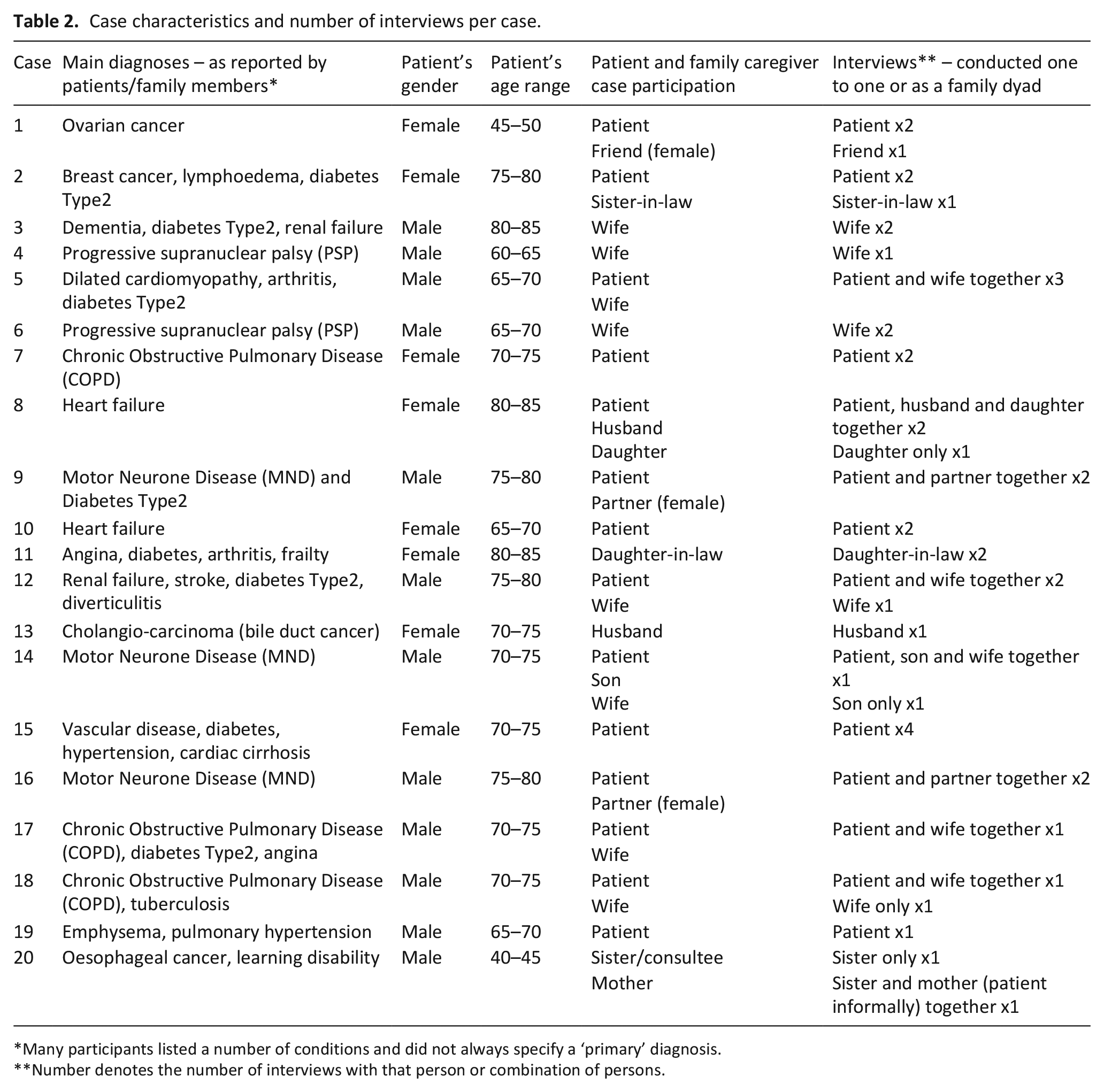
Many participants listed a number of conditions and did not always specify a ‘primary’ diagnosis.
Number denotes the number of interviews with that person or combination of persons.
Findings show that when someone is seriously ill and dying at home the work of care can be considerable. Participants in our study reported undertaking a multitude of tasks such as washing, dressing, toileting, cooking, laundry, cleaning, moving the patient, prompting eating and medication taking, being ‘on call’, providing emotional support, liaising with healthcare professionals and attending appointments alongside the management of medications. Patients, and often family caregivers, reported bearing the brunt of this workload, taking on substantial practical, physical, emotional and knowledge-based aspects of managing medications all at the time when they already have strained physical and emotional resources. For the participating families, these interlinked types of medication work took place in the context of exhaustion, anticipated loss of a family member, limited support and social isolation. This paper focuses on ‘the work of managing medications’ as a central theme across the bereaved family caregiver, patient and family caregiver narratives. As reported by Cheraghi-Sohi et al. 27 we also found that participants’ accounts of medication management work could be categorised in terms of practical, physical, emotional and knowledge work; each is presented in turn.
Administrative work
The administrative work of managing medications involved ordering, organising and keeping track of medication use. On average patients in the cases had 12 prescribed medications with a range from 6 to 20. These were prescribed in a range of formulations including tablets, injections, liquids, inhalers and patches. Opioid analgesics were the most frequently prescribed medications. The medical aspects of care slowly encroached on the home environment and additional space was often needed for storage, especially for bulkier items such as boxes of convenes, food supplements, oxygen cylinders and specialist equipment including beds, stools, commodes, chairs and stair lifts. Patients and family caregivers often deployed management techniques by locating different medications in different places throughout the house.
In the evening, if we started on the twenty-four hour circle, before bed, I used to put out the group of drugs that she had to have in the morning, and they were sort of, all in one place. I also used to put out at night the group of drugs that she may need in the night, and they were somewhere else. Then I used to put out the drugs that sort of, were ready for the rest of the day, at different stages.. . .So, at any given time, I knew which pile to go to. . . .There was no recommendations of a system, it was just something I worked out. (Mr Butcher - bereaved family caregiver)
They used to come once a month, in a big bag and I used to put them all in dates . . .in the cupboard in there so I knew I’d got the right date for the right pills. Oh god it was, no wonder [patient] got confused. (Mrs Bruce - bereaved family caregiver)
Most had developed their own systems for organising and storing medications. Spreadsheets and tick logs were also common.
Physical work
The physical work of managing medications involved tasks related to the collection of medications, and sat alongside other physical work such as cooking, cleaning, laundry and moving and handling tasks such as getting the patient upstairs or in/out of a car. Family caregivers were also often older and had disabilities and frailties of their own, placing great demand on their physical resources.
I can’t wash my feet, I can’t wash under my arms because of my shoulders. But I force my body, I always have, to do things, and that makes it worse I suppose. [Patient] is always hollering at me, but if I don’t water the flowers nobody else will. If I don’t clean the conservatory. . . (Mrs. Cooper - family caregiver)
The physical aspects of managing medications could also include visits to collect prescriptions and medications from GP surgeries or pharmacies. These could involve multiple trips, and sometimes long and difficult journeys.
I went to the chemist . . .at that point only walking 100 yards was [difficult], so [it took] half a day. And it’s just that annoying thing that I can’t do things without getting out of breath now. (Mr. Campbell - Patient)
So then I go to the chemist and I say I’ve asked for a prescription and it hasn’t come . . .then she said if you come back on Monday we’ll get it sorted out. . . .So I went on Monday and that wasn’t any good, because we hadn’t got a letter from the hospital yet. . . so I have to go back on Tuesday with the letter. So how many times have I been now? I thought it was four. But it might be five. . . .and then I have to go back again to pick them up. (Mrs. Connor - family caregiver)
Disability and illness could also cause multiple issues for physically handling medications. Family caregivers noted certain junctures at which patients could no longer independently manage their own care, for example, as regimens became more complex, or as they developed physical difficulties with eyesight, swallow, tremor or dexterity. Furthermore, medications themselves, and conditions such as dementias, could cause memory loss, drowsiness and confusion.
Initially she would deal with it by herself. But there came a point in time when there was so much medication she was taking clearly she was getting confused . . . it’s a multiple of things – which can be difficult for her especially because her English was not great . . .she couldn’t read the back of a box or something and say ‘OK this is how much I’m supposed to take’. And she couldn’t tell the difference of medications if there was a slight difference in the shape of the pill or something. (Mr. Bhuta - bereaved family caregiver)
Some patients seemed to devolve responsibility for their medication to family caregivers with little resistance. Others preferred to maintain as much control as possible and only engaged minimal support with medication tasks until quite close to their death.
Emotional work
Supporting patients in managing their medication could involve considerable emotional work for family caregivers. They often reported the unwelcome task of surveillance, prompting and making sure patients took their medication, providing reassurance and reiterating the reasons why the medication was needed as well as remaining vigilant to the occurrence of side effects and being constantly ‘on call’ to provide help when needed. Many of those involved in administering medications reported this to be a stressful and sometimes frightening experience involving a heavy burden of responsibility. This kind of work sits alongside the emotional distress of losing a loved one.
I looked through it and wrote it down and I was very careful . . .because I’d never done anything like this before, I was terrified of overdosing [him]. . . . I was terrified of getting his medication wrong, because I didn’t really know, you’re not instructed how to give it and everything, it’s just, you get it and you look at the leaflet and the instructions on the box and hope that’s how it goes. (Mrs. Baker - bereaved family caregiver)
Emotion work was often heightened by limited knowledge and information about medications, their use and side effects.
Knowledge work
Knowledge work involved understanding what each medication was for, as well as how and when to take them and what the side effects might be. Some patients and family caregivers reported being given little information about medications. Even when information was given, reinforced and checked some recognised that verbal information alone was not sufficient. Family caregivers reported not being able to absorb information and needing to refer to it later when they may be under strain, such as in the middle of the night. However, some participants developed extremely detailed knowledge of medications and worked out systems of keeping a precise record of how, and when, they had been taken.
I was still trying to keep track of what they were doing and changing so that I could say if they’re giving her something that I remembered her having before that had given her a side effect . . . So, albeit, it was in their hands, there was still a little bit of feeling like I needed to be there whenever the doctor came in to tune into that. (Mrs. Booth - bereaved family caregiver)
Yeah, it adds to the disjointed and lack of ownership, yeah, because the matron could prescribe something, district nursing could prescribe something, the doctor could prescribe something and then [palliative care nurse] could prescribe something, all without reviewing what other medication. (Mr. Crispin - family caregiver)
Knowledge work was often drawn upon and tested when family caregivers reported giving information to health professionals, such as during a hospital admission. It also intersected with the emotional work of remaining vigilant to changes made by health professionals in order to avoid repeated health crises caused by side effects or interactions.
Discussion
Main findings
Building on Corbin and Strauss’ 26 foundation of illness work and incorporating Cheraghi-Sohi et al.’s 27 themes of medication work, we have applied these to end of life care. We identified that the work associated with managing medications at home involved practical, physical, emotional and knowledge elements that require patients and family caregivers to manage multifaceted, and often potent, regimens and rapidly changing prescriptions at the end of life.23,24 This article has demonstrated that the work of managing medications can add to the considerable burden when someone is being cared for and dying at home. At times, and especially as the patient approaches death, the challenging and burdensome nature of this work could be overwhelming. For patients and family caregivers medications management is a key part of the ultimate ‘competition for resources’ 26 at the time when emotional, physical and financial resources are under enormous strain. These challenges are exacerbated by the need to negotiate complex and bureaucratic health and social care systems. 28 We suggest the need to develop professional awareness and simpler, more streamlined services to provide more effective support for families of patients dying at home.10,22,27,38
What this study adds
May and colleagues have called attention to the excessive burden which health care services impose on patients and family caregivers in complying with complex treatment regimens.2,25,39,40 Burden of Treatment Theory proposes that care, and the capacity of patients to benefit from care, must take account of the wider context of social and structural constraints in which they are embedded. Family caregivers are an increasingly essential resource within health care as the boundaries between private and professional spaces become progressively blurred.41–48 Furthermore, patients and family caregivers are asked to undertake tasks formerly carried out by professionals, but with little if any training or supervision.24,49–52
The different elements of work undertaken by participants in this study included ordering, obtaining, administering, recording and storing medications in the home as well liaising with professionals about changes, errors and problems with prescribed medication.3,9,27,50,53 Patients and family caregivers often took on the role of care coordinator, maintaining ‘hyper-vigilance’ 54 and ‘surveillance’ 27 in their dealings with services and healthcare professionals and filling in gaps in information and coordination between these. Yet healthcare professionals often had little understanding of the complexities and difficulties presented by managing medications in the home or how family caregivers felt about having to take on these roles. 23 These realities of care in the home remain hidden, alongside an idealised depiction of normative patient ‘choice’ to die at home which has become inextricably linked to the notion of a ‘good death’.47,55,56
It is important for healthcare professionals to recognise and explore the complexities of managing medications in the home with patients and family caregivers in order for them to support families in identifying tailored ways to access, store, organise and administer medications. Families need to be provided with written information to reinforce conversations and be given clear guidance on how and when to access help. We recognise that these are not new suggestions and most are included in current NHS guidance. 57 However, the systems and complexities of primary and secondary care mean that it is increasingly difficult to ascertain which healthcare professionals or service has, or should have, responsibility for supporting patients and families to manage medications at the end of life. Persistently over stretched resources often mean that time and energy is restricted to functional tasks and firefighting crises. Cycles of underfunding and professional silos are being compounded by emerging evidence of a COVID-19 induced acceleration of longstanding trends to increase the responsibility and workload of medications management for families confronting the challenges of providing care for patients dying at home.58,59
Strengths and limitations of the study
These findings are part of a larger study to explore the management of medications when someone is seriously ill and dying at home. The substantial body of qualitative data collected by the Managing Medications study enabled a very detailed account and triangulation of the experience and perspectives of patients, current and bereaved family caregivers. The views of healthcare professionals were also included and have been reported elsewhere. 23 A longer period of follow up would have deepened our understanding of families’ experience of managing medications in end-of-life care but was beyond the resources available to the project. While we were not able to include extensive diversity in terms of ethnic background or disadvantaged groups, participants did represent different conditions, disabilities and living circumstances. It was not the aim that the study findings be directly generalisable to other settings, but rather to provide in-depth insight into families’ experiences. It must be noted that while efforts were made to involve key services, we recognise that our participant group is made up of people with access to those services, and who are willing to participant in research at an exceptionally difficult and complex time in their lives. It can be noted that we were reliant on clinical gatekeepers to identify and initially approach possible participants. This is advantageous in identifying appropriate people of the study but can potentially lead to selection bias based on who they think will be willing to take part.
Our findings support and extend the knowledge provided by the limited number of previous studies from the UK and wider international literature.8,9,24,60,61 Previous studies of patients and family caregiver experiences have focused on individual elements of medication use.10,62,63 The Managing Medications study took a wider approach by exploring medications management from the narratives and perspectives of multiple key stakeholders in end of life care. Findings are, therefore, firmly situated within the context of each family, their circumstances and composition, and in relation to the resources they could mobilise through their informal and professional networks.
To date, community pharmacists have played little part in supporting medications management at home for patients receiving palliative and end of life care.6,64,65 In our study community pharmacy was notable by its absence in participants’ narratives. These findings suggest a need to further explore patient and family caregiver attitudes towards their current and future involvement in the management of medication, including greater involvement in the administration of anticipatory medication. They also highlight the scope for more effective and flexible tailoring of professional support for individual patients and their family caregivers.58,59,66
Conclusion
This paper highlights the ‘work’ of medications management for seriously ill patients being cared for at home. The challenges and effort involved are not well recognised or acknowledged by healthcare professionals. It is essential that we consider the limits of what it is reasonable to ask patients and family caregivers to do, especially when they are fatigued, distressed and under pressure. Ongoing moves to remote consultation and reduction in GP and other staff doing home visits reduces the hands-on support for patients and family caregivers and increase their responsibility and active engagement in managing medications. This trend is likely to continue long after COVID-19 and highlights the need to consider the impact on already over-stretched carers and how this can be reduced. Effective measures to systemically reduce complexity and improve coordination of care must be prioritised while on the ground, the focus should be on improving effective support via greater professional awareness and understanding of the work of managing medications at home.
Footnotes
Acknowledgements
We would like to acknowledge the contribution of PPI co-applicant Alan Caswell, Dr. Asam Latif, Professor Antony Avery, Professor Claire Anderson, Dr. Vincent Crosby and Professor Christina Faull in supporting the Managing Medicines study as members of the wider team. We would also like to acknowledge Nicola Turner (NT) for her role in data collection in the early phase of the study. Dr. Turner is a Research Fellow in the Nottingham Centre for the Advancement of Research into Palliative and End of life (NCARE) in the School of Health Sciences. She has considerable experience of undertaking qualitative interview in this field, and was seconded to the study to cover EW’s maternity leave.
Authorship
EW, GC and KP were involved in all aspects of data collection analysis, drafting the article and revising it critically for important intellectual content. KP also designed the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the National Institute of Health Research (Health Services & Delivery Research project: 15/70/101).
Disclaimer
The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Ethics and consent
Approval was granted in March 2017, by East Midlands, Derby Research Ethics Committee – 17/EM/0091. R&D approvals for each Trust were also acquired. All participants gave written or, in the case of telephone interviews, verbal consent to undertake the interviews and for anonymised sections to be used for publication and dissemination.
Data sharing
The datasets generated and/or analysed during the current study are not publicly available. Data sharing was not included in the ethical approval as the study involves personal accounts of patients’ and families’ experiences. It is essential that we maintain confidentiality and anonymity but sufficiently anonymised parts of the data are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.