
Abstract
Background:
It is reported that, given the right support, most people would prefer to die at home, yet a very small minority of people with dementia do so. At present, knowledge gaps remain on how best to support end-of-life care at home for people with dementia.
Aim:
To identify and understand the challenges and facilitators of providing end-of-life care at home for people with dementia.
Design:
Narrative synthesis of qualitative and quantitative data.
Data sources:
The review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A systematic literature search was conducted across six electronic databases (AMED, BNI, CINAHL, EMBASE, MEDLINE and PsycINFO) and reference lists of key journals were searched up to July 2017.
Results:
Searches returned 1949 unique titles, of which seven studies met all the eligibility criteria (four quantitative and three qualitative). Six key themes were identified – four facilitators and two challenges. Facilitators included ‘support from health care professionals’, ‘informal caregiver resilience and extended social networks’, ‘medications and symptom management’ and ‘appropriate equipment and home adaptations’. Challenges included ‘issues with professional services’ and ‘worsening of physical or mental health’.
Conclusion:
People with dementia may not always require specialist palliative care at the end of life. Further research is required to overcome the methodological shortcomings of previous studies and establish how community development approaches to palliative care, such as compassionate communities, can support families to allow a greater number of people with dementia to die at home.
Public surveys report that, given the choice, most people would prefer to die in their own homes, yet people with dementia rarely achieve this.
It is recommended that a palliative care approach should be adopted when a person with dementia approaches the end of life, but many people are admitted to hospital and receive suboptimal care.
There is limited research on how best to support people with dementia to stay at home at the end of life.
A comprehensive synthesis of the evidence in relation to the factors that influence death at home in people with dementia revealed that support from healthcare professionals, carer resilience and extended social networks, support with medications and symptom management, and appropriate equipment and home adaptations all facilitated dying at home with dementia.
Challenges included issues with formal services and deteriorating physical or mental health.
The synthesis also revealed that there is comparatively little research in this area.
Inequitable access and wide disparities in end-of-life care at home for people with dementia can lead to poor coordination of care and a lack of unified standards.
In dementia, dying outside the family home appears to be the norm, but with appropriate support more families could be enabled to care at home until the end of life.
Further research with bereaved informal caregivers who supported someone with dementia at home until the end of life is required, as well as research into new public health approaches to palliative care such as compassionate community initiatives.
Background
Dementia is a life-limiting illness that is associated with a high symptom burden, particularly in the advanced stages of the disease. In 2015, it became the leading cause of death in England and Wales accounting for 11.6% of all deaths registered. 1 Worldwide, it is estimated that 46 million people have dementia, and this is expected to treble by 2050. 2 Owing to this rapid increase in prevalence, providing appropriate end-of-life care to people with dementia now poses a significant challenge to healthcare systems and societies across the world.
Place of death has been identified as an important component of high-quality end-of-life care and it is reported that, given the right support, most people would prefer to die in their own homes.3,4 In the context of death and dying, the ‘home’ often represents a feeling of familiarity, comfort and security5,6 and is associated as a contributing factor to a ‘good death’.
A review of qualitative literature on place of death for people with dementia found that a preference for home care consistently emerged. 7 Reasons for this included an inability to access hospice care, caregiver’s reluctance to place their relative in a care home for both normative and emotional reasons and a wish to avoid acute care settings. Despite this information, it is still rare for people with dementia to die in their own homes. A population study analysing death certificates between 2001 and 2010 found that only 4.8% of deaths from dementia in England occurred within the person’s own home (compared with 3.3% in Wales and 7.3% in Scotland), with 55.3% of people dying in care homes (compared with 43.8% in Wales and 54.9% in Scotland) and 39.6% in hospital (compared with 52.8% in Wales and 37.6% in Scotland). 8 Data from international sources also indicate that people with dementia are more likely to die in hospital or a long-term care facility than in their own homes. 9
Current recommendations suggest that when a person with dementia approaches the end of life, a palliative approach to care should be adopted.10,11 In recent years, there has been an increased international commitment to provide this care in community settings in order to meet patient choice, as well as reduce hospital-acquired infection, healthcare costs and inappropriate lengthy hospital admissions.10–13 However, with large variations in the provision of community-based care and a limited understanding of the dementia disease trajectory, people with end-stage dementia continue to be hospitalised and receive active treatment rather than palliative care and comfort measures.14–17 As well as being of significant financial cost to healthcare services, these burdensome admissions often have low rates of success and can hasten functional decline, morbidity and mortality.18–22 Furthermore, transitioning a person with advanced dementia from their normal surroundings can cause distress and increase confusion. 23
The success of home-based end-of-life care usually relies upon the availability and involvement of an informal (unpaid) caregiver. 24 However, as a person with dementia moves into the later stages of the disease, they typically need a more extensive level of care than their family can provide25–27 and a nursing home placement may be required. In recent years, there has been a steady increase in the amount of studies that have explored end-of-life care for people with dementia within these settings.25,28–33 While this has led to ongoing improvements for people living within these facilities, there has been comparatively little research that has explored end-of-life care for people with dementia who continue to reside in their own homes. 34 Consequently, the needs of this population, as well as their informal caregivers, are predominantly undefined and inadequately understood.
Owing to an increasing prevalence of people with dementia with end-of-life care needs and considerable strategic investment to support greater choice regarding place of death, a more in-depth understanding of the factors associated with end-of-life care at home for people with dementia is required.
Aim
The aim of this article is to identify and synthesise the literature relating to the challenges and facilitators of providing end-of-life care at home for people with dementia.
The following definitions were used:
Challenges are actual or perceived factors that negatively impact or interfere with end-of-life care at home.
Facilitators are actual or perceived factors that positively impact or enable the implementation of end-of-life care at home.
Method
Design
To identify relevant studies, a search of both qualitative and quantitative studies was conducted in accordance with the general principles recommended by the Centre for Reviews and Dissemination 35 taking a systematic approach to the search strategy and selection procedures to ensure rigour and transparency. To analyse the findings, the review adopted a narrative synthesis approach which follows the guidelines from the Economic and Social Research Council (ESRC), 36 using thematic analysis and tabulation as tools for analysis.
Search strategy
Six electronic databases were searched (AMED, BNI, CINAHL, EMBASE, MEDLINE and PsycINFO) in November 2016 and updated in July 2017. Due to the expected paucity of literature in this area, a time frame was not placed upon the search.
A comprehensive search strategy in relation to the research question and the principle of PICO 35 was applied to guide the selection of search terms. A set of keywords were identified and used to search the literature (Table 1). Subject headings were used where possible and adjusted for different databases. The same keywords were used across all databases. Additional searches were also conducted in the Cochrane database, as well as dementia and end-of-life resources such as the Alzheimer’s Society and Marie Curie libraries. A further hand search was undertaken in frequently cited journals and the reference lists of the included papers were also screened for additional sources. Experts in the field were also contacted and asked if they knew of any current studies or unpublished materials.
Key search terms.

Eligibility
Papers were included if they reported on research involving people with dementia who had received end-of-life care in their own homes. Papers must have met the following criteria:
Primary research of any design that reported upon challenges and/or facilitators to end-of-life care at home for people with dementia from the perspectives of caregivers and/or health and social care professionals.
AND/OR
Primary research that reported on the effectiveness of an intervention that sought to facilitate end-of-life care at home for people with dementia.
Papers using mixed samples (i.e. those combining data on people who had died in settings other than at home) were only included if the findings regarding care at home were reported separately in the results section.
Papers were excluded if they were
End-of-life studies not specific to dementia;
Dementia studies but not specific to end of life;
Studies about people with dementia who lived and died in a care/nursing home or hospital;
Not in English language;
Service proposals, guidelines or a synthesis of opinion with no empirical data;
Single case reports that provided anecdotal evidence.
Selection procedure
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 37 was used to guide the reporting of this systematic review (Figure 1). All titles and abstracts were screened by C.M. and excluded if they did not meet the inclusion criteria. Full-text copies of all papers that met the inclusion criteria were retrieved for further investigation. Any articles that appeared relevant but did not provide sufficient information were also retrieved and read in full. If there was doubt about the suitability of a study for inclusion, it was discussed with the supervisory team and included only if there was complete agreement.
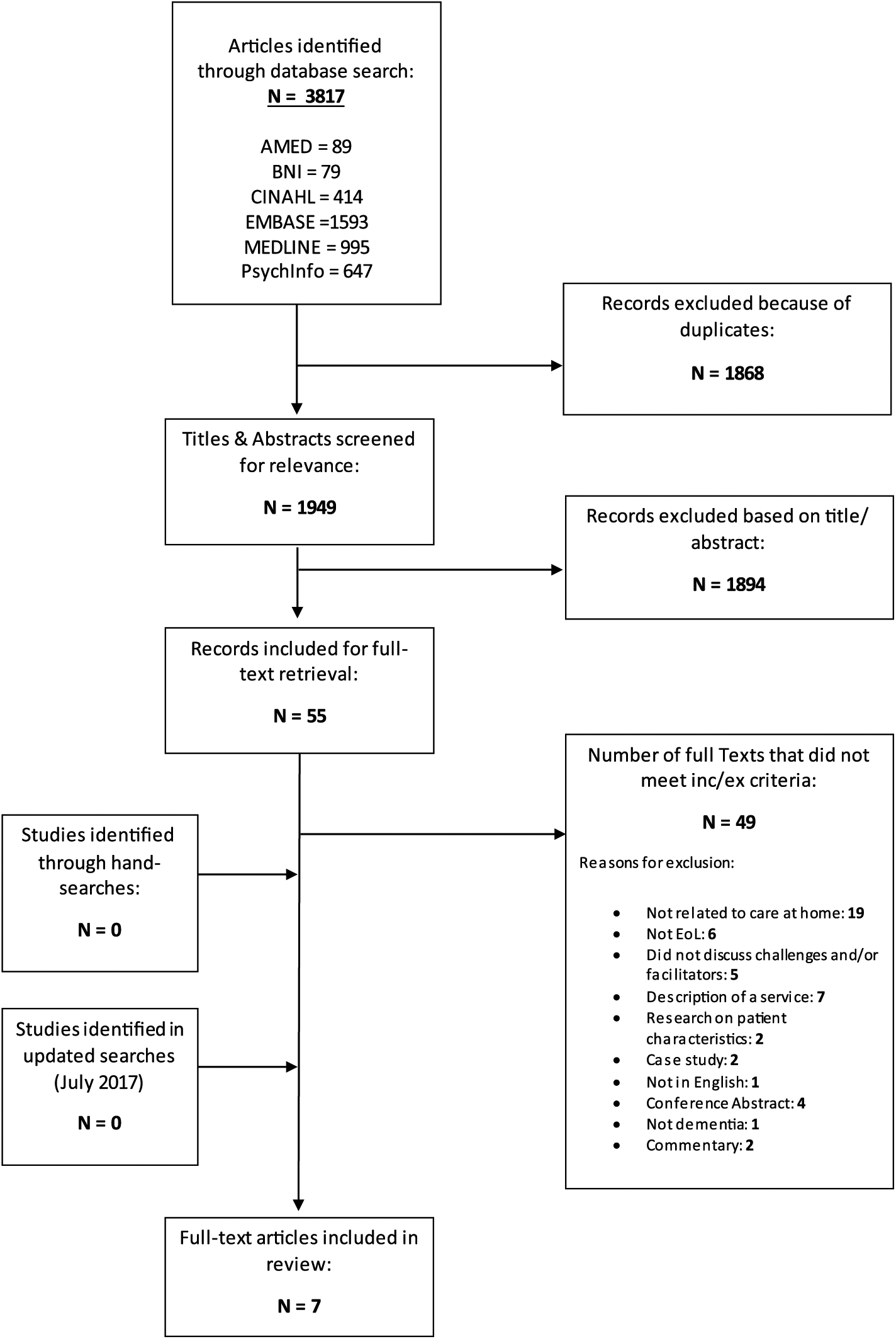
PRISMA diagram of the included studies.
To enhance the validity and reliability of the selection procedure, 10% of the excluded full-text papers and all the included papers were read and checked by a second reviewer (M.L.-W.).
Quality appraisal
All studies were assessed for methodological quality. Due to the heterogeneity of data, evidence was appraised using a checklist developed by Hawker et al. 38 who described a method of systematically reviewing research from disparate research paradigms. The tool comprises nine questions to determine the rigour, credibility and relevance of the study. The questions are designed to assist the reviewer in the evaluation by addressing the aim, methodology, design, sampling, data collection, data analysis, ethical issues, findings and value of the research. To make the results as explicit as possible, each item is rated as ‘good’, ‘fair’, ‘poor’ or ‘very poor’. Using this system, a numerical score can also be calculated for each study (10 = very poor; 40 = good) that indicates methodological rigour.
Data extraction and analysis
Due to the heterogenitey of the papers included, meta-analysis of quantitative studies and meta-synthesis of qualitative studies were not possible. Therefore, a synthesis of the results was reported narratively using a framework developed by the ESRC Methods Programme. 36 This included developing a preliminary synthesis and extracting relevant data from the included papers using a bespoke form and tabulation. Data extracted included the country of origin, primary aim of the study, design, sample, data collection method and the results that were relevant to the purpose of this review.
Results were synthesised thematically using Thomas and Harden’s 39 three-stage process: coding text, development of descriptive themes and analytical theme generation. Regular debriefing and discussion of themes among two reviewers (C.M. and M.L.-W.) and additional discussions with a third and a fourth reviewer (C.D. and K.H.D.) were used to refine and validate the findings, until consensus about the themes was reached.
Results
Seven papers were included in the final analysis (Table 2): four quantitative papers40–43 and three qualitative papers.44–46 Four studies originated from the United States,40,42,43,46 two from the United Kingdom40,44 and one from Japan. 41 Participants in all papers were bereaved informal caregivers, apart from Gabbard and McNabney, 43 which analysed retrospective data from deceased patient charts, and Hirakawa et al., 41 which collected data from questionnaires given to general practitioners (GPs) following patient deaths.
Studies (in order of methodological quality).
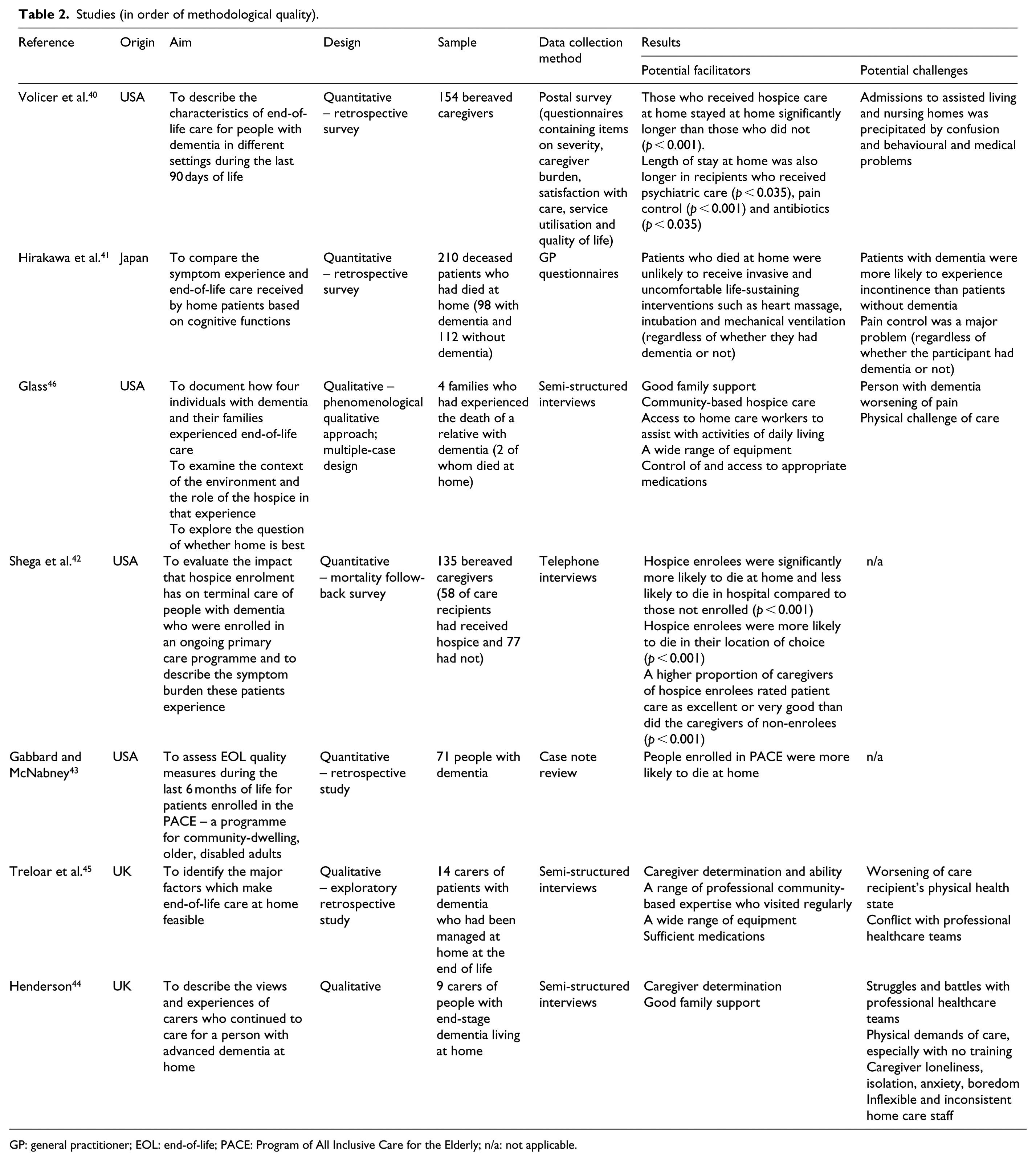
GP: general practitioner; EOL: end-of-life; PACE: Program of All Inclusive Care for the Elderly; n/a: not applicable.
The included studies covered a range of research questions and used a variety of data collection techniques. All papers presented data on the factors that could facilitate and/or challenge end-of-life care at home for people with dementia, but only two studies used this as their primary aim.44,45 The primary aims of the other studies included examining the characteristics of people with dementia who died in different settings,40,42 comparing the end-of-life experience of people with and without dementia, 41 evaluating the impact of a service, such as hospice, 42 exploring quality of life 43 and documenting the experience of caring for someone with dementia at the end of life. 46
No studies from the review were excluded based on the results of their quality appraisal. Table 3 shows the results of the quality assessment, showing domain scores and total scores for each study. Each study could achieve a score between 90 and 360, with higher scores indicating better quality studies. Studies achieved the quality scores ranging between 180 44 and 340. 41
Methodological quality of the included studies.
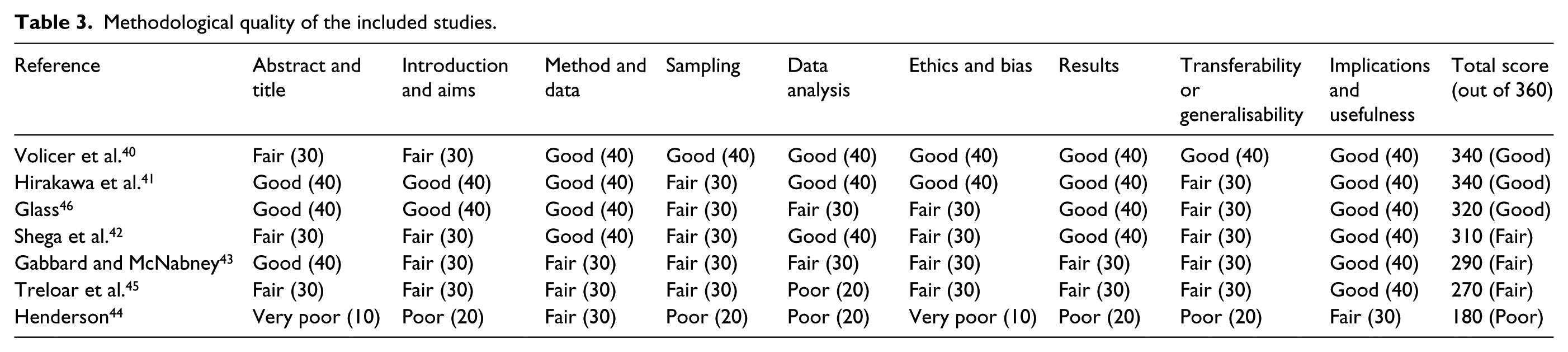
All studies used appropriate research designs for their chosen aims, although some did not describe their methodologies and failed to explain why they had chosen to use certain methods.44,45 None of the studies used randomised controlled trials or any other form of experimental design. All quantitative data were collected using standardised measures, which helped increase the internal validity of the studies. All qualitative data were collected using semi-structured interviews, but only the paper by Glass 46 reports on how the data were recorded and transcribed. None of the qualitative papers discussed reflexivity.
Sample sizes ranged from 4 46 to 210, 41 with 597 participants in total across studies. While it is likely that the small sample sizes in some of the studies represent the rare incidence of people with dementia dying at home, their results should be interpreted with caution as the findings may not generalise to a larger population. All sampling strategies were appropriate to address the aims of each study.
All quantitative studies reported a clear description of how the analyses were carried out and used appropriate statistical tests to make direct comparisons between variables. Of the qualitative papers, only Glass 46 described an appropriate justification of the theoretical underpinning for the methods chosen, which is crucial when enabling the reader to understand the lens through which the data were analysed and helps add transparency to the findings. All quantitative papers found significant results and reported their findings appropriately apart from Gabbard and McNabney 43 which omitted p values without explanation, so it is not clear what was used to determine statistical significance. Of the qualitative papers, all supported their results with relevant quotes. However, the study by Henderson 44 made only brief reference to these.
Results of the synthesis
Facilitators to end-of-life care at home for people with dementia
Support from healthcare professionals
Death at home relied heavily on the provision of formal health and social care services, and this was a theme that occurred throughout all the identified papers. Several different service models were described, including specialist community-based palliative/hospice care,40,42,46 as well as generalist packages that provided personal and nursing care.43,44 There was also evidence of older people’s psychiatry services playing an important role in assisting with end-of-life care at home40,45 as well as input from initiatives such as ‘sitting services’. 44 However, it appears that the availability and design of each service vary from country to country.
One paper which explored the effects of community-based hospice on people with dementia found that care recipients who used the service stayed at home significantly longer those who did not. 40 Another found that hospice enrolees with dementia were significantly more likely to die at home and correspondingly less likely to die in hospital than people with dementia who were not receiving hospice care. In addition, a higher proportion of caregivers of those enrolled in hospice services rated patient care as ‘excellent’ or ‘very good’ than did the caregivers of those not enrolled. 42 The benefits of community-based hospice were also demonstrated in the qualitative research, with useful components being their ability to prescribe effective medications, provide equipment and offer necessary education on how to care for a person with dementia. 46 While these specialist palliative care services were found to be successful in supporting people with dementia to stay at home until the end of life, they are more readily available in the United States and no UK-based studies on such services were identified.
Evidence from other studies demonstrated that specialist palliative care was not always necessary to enable a home death. For example, one described a service in which elderly community-dwelling patients who were certified as eligible for nursing home-level care received an interdisciplinary model of care, which enabled them to remain in the community rather than be admitted to a nursing home. 43 They found that the chance of dying at home increased significantly with the length of time enrolled in the programme, with 65% dying at home after more than 2 years enrolled compared to 15% of those enrolled less than 2 years but more than 1 year, and 20% enrolled less than a year.
Regardless of the model of care that is provided, regular contact with a healthcare professional appears to play an important role in end-of-life care at home for people with dementia. Examples of best practice included regular monitoring from Older People’s Psychiatry services to offer advice and adjust medication, as well as visits at request ‘for any reason’ 45 and the availability of additional support by telephone. 46 Domiciliary care workers or ‘aides’ were also important members of the care team at the end of life and in some cases they provided not only care for the person with dementia, but also company for the informal caregiver 46 as they often reported feeling lonely or isolated.
Informal caregiver resilience and extended social networks
Throughout the data, there is a considerable amount of detail concerning the accumulation of strains experienced by informal caregivers over time as demands grow and change. Therefore, a degree of resilience seems to be required to enable caregivers to look after a person with dementia at home at the end of life. Family caregivers often describe having to ‘skill up’ very quickly in order to adapt to the changes. 45 A strong determination to keep the individual at home was also a key factor and this was mentioned across all of the qualitative papers. For example, ‘no matter how hard [caring at home] was, he’d find a way to do it’. 46
Family caregivers with reliable and consistent sources of informal support from wider social networks also appear more likely to cope with the caring role over an extended period and studies describe how the involvement of other family members was a crucial factor that enabled the person with dementia to die at home. One study reported that family caregivers commonly received help from their children (13% ‘every day’ and 32% ‘often’), other family members (6% ‘every day’ and 22% ‘often’) and siblings (5% ‘every day’ and 15% ‘often’). They also received assistance from friends and neighbours (1% ‘every day’ and 22% ‘often’), volunteers (3% ‘every day’ and 19% ‘often’) and religious acquaintances (3% ‘every day’ and 17% ‘often’). 40
Medications and symptom management
The ability of informal caregivers to appropriately manage symptoms and administer medications to minimise the risk of care recipients suffering uncontrolled symptoms and distress was another factor that was deemed important in facilitating end-of-life care at home for people with dementia.
All included studies observed pain to be a significant symptom at the end of life and the availability of pain control was important in keeping people at home. For example, one study showed how length of stay at home was significantly longer in dementia patients who received sufficient pain control. 40 Furthermore, family caregivers in another study stated that morphine in small volumes was useful, as well as opiates in some instances. 45 Although now controversial in the field, this study also found that medications to alleviate psychiatric symptoms such as agitation were also found to be important (e.g. risperidone and olanzapine), as were antibiotics.
Family caregivers in the qualitative studies44–46 willingly assumed responsibility for treatment because it meant that they could provide immediate symptom relief. They seemed to show an awareness of what to monitor and how to interpret symptoms. For example, caregivers in one study kept records and used their own judgements about how to alter and time medications. 46
Appropriate equipment and home adaptations
The studies included in this synthesis revealed that the home environment can become more challenging as dementia progresses. Therefore, having access to appropriate equipment and adapting the home to meet the needs of the individual were seen to be integral to providing end-of-life care in the home. Caregivers in Treloar et al.’s 45 study rated items such as continence aids, commodes and wheelchairs as ‘indispensable’ and hospital beds, pressure-relieving cushions and hoists as ‘very useful’. However, the availability of these items was variable and depended on caregiver’s skills and the help they received from professionals. One study also reported that an average of $1368 was spent on home adaptation during the last 90 days of care recipient’s life. 38
Challenges of providing end-of-life care at home to people with dementia
Issues with professional services
While support from professional healthcare services was found to be the leading factor in facilitating end-of-life care at home for people with dementia, there was also evidence of poor practice, which posed a major threat. Throughout the papers, there were examples of poor working relationships with professionals and a lack of rapport, with some studies describing caregivers having arguments or ‘constant battles’ with healthcare teams.44,46
Studies from the United Kingdom reported that when care packages from social services were utilised to assist with instrumental and personal care, they could often be rigid, with several different staff members visiting. This often led to inconsistent and impersonal care, 45 which was only resolved when caregivers had financial control of care staff. The decision to pay privately for home care workers was also highlighted in other studies, 46 suggesting that statutory services do not tailor care provision to meet the needs of people with dementia and their caregivers at the end of life.
Worsening of physical or mental health
Challenges or breakdowns of end-of-life care at home for people with dementia were often exacerbated by an increase in the care recipients’ behavioural/psychiatric problems and/or a deterioration in their physical health. One study revealed that admissions to nursing homes were often precipitated by confusion and the resulting behavioural problems, as were significant medical problems. 40 Another study showed that such symptoms could also result in hospital admissions. 45
As mentioned previously, the most common symptom reported across all the included studies was pain. One study found that over 50% of caregivers reported that pain was of moderate severity or higher on average in the last 2 weeks of life. 42 Hirakawa et al. 41 also found pain to be a significant problem in the last 2 days of life. However, they also found that participants with dementia were less likely to report pain than controls (without dementia), which they concluded may be due to a limited ability to communicate. Other common symptoms across studies were incontinence, pressure sores, respiratory problems, inability to swallow, depression and agitation.
As the condition of the person with dementia worsened, greater demands for personal care and instrumental tasks were made on caregivers. If there was little support from healthcare professionals, these increasing demands were often associated with greater perceived burden as caregivers appeared to lack confidence in carrying out these tasks, reporting feeling unskilled and unable to properly deal with the issues.
Some studies concluded that caregiving was often more of a mental challenge than a physical one, particularly in relation to incontinence. 45 Others described the physical aspects of caring as the most difficult, especially without appropriate training and support. 44 Caregivers experiencing a loss of freedom, isolation and fatigue was also highlighted across studies. Volicer et al. 40 also found that caregiver burden was higher when the person with dementia experienced psychiatric symptoms.
Discussion
This article identified and synthesised the evidence in relation to the challenges and facilitators of providing end-of-life care at home for people with dementia. As there have been very few published papers in this area, a wide range of study designs were included to provide a comprehensive overview of the existing research. This mixed-method approach to synthesis helped to provide novel insights into the evidence being reviewed. While the quantitative findings offered an understanding of the factors involved in facilitating home deaths in people with dementia, as well as the strengths of these relationships, the qualitative findings helped to provide a context of how and why these factors may or may not work from the perspective of informal caregivers.
Given the complex needs of people with dementia, providing end-of-life care at home is a huge undertaking and caregivers often require a great deal of support. The papers identified reveal that no single model of end-of-life care exists. As people with dementia and their caregivers often have a range of needs in relation to practical and emotional support, they are likely to be simultaneously engaged with using formal healthcare services, as well as a range of other community-based care services and extended informal networks.
In the United Kingdom, professional end-of-life care at home for people with dementia is largely delivered by primary healthcare professionals such as GPs and District nurses and secondary services such as Older People’s Psychiatric teams. Care packages that offer domiciliary support are also frequently used. Although other services, such as respite and day care, are available for people with dementia, 47 no papers reporting on the work of such agencies were found, indicating that there has been little formal research conducted in this area. Despite this involvement of a wide range of health and social care professionals, other studies that have explored end-of-life care have found that there is little coordination or knowledge of each other’s activity or remit22,48 as well as a lack of unified standards, 49 which in turn can act as a barrier to good-quality care at the end of life.
While professional community-based support was available for people with dementia in all countries included in this synthesis, the integration of specialist palliative care into health service provision between countries was variable, with it being more readily available in the United States. The impact of community-based specialist palliative care teams on patient outcomes has been examined in several studies in non-dementia cohorts and evidence from systematic reviews has demonstrated that they can improve patient outcomes such as satisfaction with care, 50 reduce length of stay in hospital 51 and increase the odds of dying at home. 52
There is an implication that extending specialist palliative care services to people with dementia might result in better care and help more people to die at home. However, it has been suggested that this approach, which was developed for people with cancer, is not always desirable or feasible when applied to people with non-cancer conditions. 53 It is argued that most of the symptoms experienced by people with dementia at the end of life, such as pain, pressure sores or difficulties swallowing, do not require specialist intervention, but instead good-quality basic care.54,55 This is further supported by a study of family caregivers’ conceptualisations of quality end-of-life care for people with dementia by Davies et al., 56 who concluded that care does not need to be complex, but it should be tailored to the needs of the individual. This article advocates these assumptions as many of the facilitating aspects of home-based care were basic elements that could arguably be provided by palliative care generalists (e.g. symptom management and access to appropriate equipment). However, there is an ongoing debate about who should deliver this care and when it should be applied. 57
Surprisingly, none of the studies identified in this article referred to advance care planning (ACP), which is often seen as central to good end-of-life care, facilitating choice and quality of dying. 58 When used, ACP can have a significant impact on place of death as people can make an ‘advance statement’, which reflects their general beliefs and personal values about the sort of care they would like to receive in the future. 54 ACP is also reported to reduce the incidence of emergency admissions to acute care settings. 59
While the findings suggest that professional support is necessary to enable people with dementia to die at home, paradoxically there was also a sense that often it could also have a deleterious effect. Consistent with systematic reviews that have explored end-of-life care at home in other populations,5,60 informal caregivers of people with dementia expressed unmet need which was often related to reduced access and availability of services, as well as difficulties navigating the healthcare system. It was frequently reported that effective communication between the family caregiver and the health and social care provider was lacking and in some cases caregivers even described having to battle with professionals to attain appropriate care and services, which in turn added to feelings of stress and burden.
With the development of a health and social care service infrastructure in the 20th century, there is now an expectation that when someone is dying, care will be given primarily by professionals, 61 and it has been suggested that our dependency on these services has led to a widespread deskilling of communities in relation to dying, bereavement and caregiving in general.62,63 It is argued that, by professionalising the business of dying, families and communities are pushed into the peripheries as the professionals are assumed to be the primary source of support to those who are dying at home. Comparable with other studies, 48 this article found that paternalistic practice from healthcare services could be a major challenge to the success of dying at home, as it can lead families to feel incompetent and disenfranchised.
In recent years, new concepts of palliative care that focus on empowering people, families and communities allowing them to draw on their own resources and community supports to adapt and cope have been developed. 64 A range of terms exist to describe these approaches, including a public health approach, health-promoting palliative care and compassionate communities. Such community-led interventions focus on the development and delivery of a social/professional model of care and support for people living at home at the end of life by using volunteers and/or naturally occurring informal networks. The idea underpinning these models is that, by drawing on the resources of the community, it is possible to meet a person’s social and practical needs, but also to build capacity and resilience in the community and naturalise the process of care, dying, death and bereavement.65,66 They acknowledge that informal caring networks have a range of competencies in end-of-life care and urge formal services to understand their value and supplement them with their own practice wisdom and resources.48,67 In the United Kingdom, end-of-life care policy documents have recognised the significance of such approaches, 12 but it is not yet understood how they may support people with dementia.
Implications for research and practice
The findings of this synthesis suggest that people with dementia and their caregivers can suffer a contraction in their social networks and often feel unsupported at the end of life, which can lead to feelings of burden and isolation.
Given the current demands on professional health and social care services, 68 developing public health approaches to end-of-life care for people with dementia, such as compassionate community initiatives, could provide a practical and cost-effective solution for people who wish to spend their final days at home. These models could complement our existing services to ensure that people with dementia and their caregivers are receiving the additional support that they need at the end of life.
Due to the divergence in health and social care provision found across the studies included in this synthesis, it was difficult to determine which elements of such care and support are providing optimal benefits. Therefore, future research priorities should include overcoming the methodological shortcomings of previous work to identify the barriers and facilitators of providing end-of-life care for people with dementia at home, as well as developing an understanding of how caregivers of people with dementia might mobilise their social networks to support end-of-life care at home.
Limitations
While this article has endeavoured to synthesise the literature in a structured manner, there are some limitations of the methods utilised. For example, only studies published in English were included and this may have limited the scope.
There may also be limitations in relation to the quality of the identified studies and completeness of the review. Studies where titles, abstracts or keywords omitted the selection criteria wording may have been overlooked. However, electronic searching was augmented by contacting experts in the field, as well as hand searching journals and reference lists.
In addition, the transferability of the synthesis may also be limited by the nature of the included studies as most were conducted outside of the United Kingdom where health and social care systems are different. However, this identified deficit in the current literature can be considered a finding in itself.
Conclusion
This article offers evidence on the challenges and facilitators of end-of-life care at home for people with dementia and highlights the paucity of up-to-date literature in this area. It was found that while families value support from professional health and social care services, there are inequitable access and wide disparities in end-of-life care at home for people with dementia, which has led to poor coordination of care and a lack of unified standards.
Consistent with other findings within the field of home-based end-of-life care, 5 the results of this synthesis reinforce the importance of generating innovative strategies to overcome deficiencies in health and social care provision. It proposes that public health approaches to palliative care, such as compassionate community initiatives, may provide a practical and cost-effective solution by complementing our existing services to ensure that people with dementia and their caregivers are receiving the additional support that they need at the end of life.
Footnotes
Acknowledgements
C.M. was responsible for design, acquisition, analysis and interpretation of the data, and drafting and revision of the final manuscript. M.L.-W. was responsible for the conception of the paper. Both C.M. and M.L.-W. reviewed the titles and/or abstracts/full texts. All the co-authors contributed to the analysis, quality assessment and interpretation of the data; revising the article critically for important intellectual content and approval of the final version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was supported by the Economic and Social Research Council (ESRC).