
Abstract
Background:
COVID-19 public health restrictions have affected end-of-life care experiences for dying patients and their families.
Aim:
To explore bereaved relatives’ experiences of quality of care and family support provided during the last days of life; to identify the impact of factors associated with perceived support.
Design:
A national, observational, open online survey was developed and disseminated via social media, public fora and professional networks (June–September 2020). Validated instruments and purposively designed questions assessed experiences. Analysis used descriptive statistics, logistic regression and thematic analysis of free-text responses.
Participants:
Individuals (⩾18 years) who had experienced the death of a relative/friend (all care settings) within the United Kingdome during the COVID-19 pandemic.
Results:
Respondents (n = 278, mean 53.4 years) tended to be female (n = 216, 78%); over half were ‘son/daughter’ (174, 62.6%) to the deceased. Deceased individuals (mean 81.6 years) most frequently died in their ‘usual place of care’ (n = 192, 69.3%). Analysis established five conceptual themes affecting individualised care: (1) public health restrictions compounding the distress of ‘not knowing’; (2) disparate views about support from doctors and nurses; (3) challenges in communication and level of preparedness for the death; (4) delivery of compassionate care; (5) emotional needs and potential impact on grief. Male respondents (OR 2.9, p = 0.03) and those able to visit (OR 2.2, p = 0.04) were independently associated with good perceptions of family support.
Conclusion:
Despite public health restrictions, individualised care can be enabled by proactive, informative communication; recognising dying in a timely manner and facilitating the ability to be present before death.
During the COVID-19 pandemic, public health restrictions may have significantly changed end-of-life care experiences for dying patients and their families.
Being unable to visit impacted on the families’ preparedness for the death and compounded the distress of the situation, especially for those experiencing deaths within the care home or hospital setting.
Men and those able to visit were more likely to report being adequately supported during the last days of life.
Despite the challenges, there were examples of compassionate care where timely communication and being present to ‘say goodbye’ were facilitated.
Providing staff training and enabling protected time for timely, informative communication between health and social care professionals and family members needs to be prioritised during a pandemic, especially within the care home setting where this is less commonplace.
During a pandemic, it is essential that health and social care staff can recognise dying and feel confident to talk honestly with relatives about this, to enable final visits to be conducted in a timely manner.
There is a need to identify additional elements that explain differing perceptions of support during a pandemic, to help tailor support mechanisms both before and after the death.
Introduction
Following the emergence of COVID-19 in December 2019, the World Health Organisation declared a pandemic on March 11th 2020. 1 Pandemics cause increased demand for healthcare services, including those provided by palliative and end-of-life care. 2 Changing patterns of mortality are recognised with increased deaths occurring within community and hospital settings, due to both COVID-19 and non-COVID related illnesses.3,4 Staff illness and redeployment impact on the workload and skill mix of staff. Hospice services may have fewer in-patient admissions and need to shift resources to help enhance community care and provision.3,5
Natural disasters, including pandemics, have a profound impact on end-of-life care, often resulting in a ‘stark departure from a palliative care approach’. 6 Restricted visiting policies, fewer end-of-life discussions and the loss of usual death and bereavement rituals can jeopardize typical end-of-life care values and leave patients feeling isolated and fearful. 6
Additionally, the support of the family, one of the two ‘pillars’ of palliative care, can be compromised. 7 Values focused on individual needs and preferences, such as the wish for family presence and not to die alone, may be limited. 8
Few studies focus on direct service-users views during pandemics and those which have, involved seeking views about the use of telemedicine. 6 It is unlikely that COVID-19 will be the last global pandemic; we must learn from people’s experiences of the current crisis. The views of bereaved people are especially pertinent as they provide accounts of both patient care and family support. Additionally, perceptions about quality of the dying experience, along with preparedness for death, are associated with risks of complicated grief. 9
Aim
The aim of this study was to explore the experiences of individuals who had suffered a bereavement within the United Kingdom (UK) during the COVID-19 pandemic.
We present key data relating to quality of care, communication and emotional support. These represent elements within the ‘quality of dying experience’ which can affect grief and bereavement. 9 Additionally, we examined whether any demographic or clinical factors were independently associated with perceptions of adequate family support in the last days of life.
Methods
Survey development
An observational, open online survey was developed using Qualtrics online survey software and tested by the research team. The survey tool was adapted from a measure used in an affiliated, ongoing Horizon 2020 research project (The iLIVE Project: www.iliveproject.eu) to ensure relevance for deaths occurring during the pandemic and be in keeping with culturally appropriate language and practice (Supplemental File 1). The survey contained questions about demographics (deceased individual and respondents), an abbreviated version of the ‘Care Of the Dying Evaluation’ (CODE™) questionnaire 10 and relevant questions about COVID-19 and its consequences. The internationally used CODE™ questionnaire focuses on quality of care and family support during the last days of life. 11 One key outcome from CODE™ is whether or not respondents perceive themselves to be adequately supported in the last days of life. Free-text space was available for additional comments.
Five members from the online advisory panel of the Clinical Research and Innovation Office at Sheffield Teaching Hospitals NHS Trust and the lead Patient and Public Involvement (PPI) representative from the Clinical Cancer Trials Executive Committee provided feedback about the adapted tool. Their involvement was helpful for ensuring the language/questioning was appropriate, and resulted in revisions, such as the inclusion of additional response criteria, for example, adding ‘don’t know’, for respondents where visiting was not allowed at the end of life.
Study population
The questionnaire was aimed at individuals (⩾ 18 years) who had experienced the death of a family member, within the UK, during the initial part of the COVID-19 pandemic (March–September 2021) and were able to provide informed on-line consent. There were no additional inclusion or exclusion criteria. For clarity and simplicity, ‘bereaved relatives’ or ‘family member’ are used as collective terms, also representing bereaved friends and neighbours.
Recruitment
Awareness about the study and circulation of the online survey was undertaken via local and national bereavement organisations (CRUSE, National Bereavement Alliance), as well as UK professional, public and charitable networks related to palliative care and minority ethnic communities, for example, Association of Palliative Medicine of Great Britain and Ireland, All Ireland Institute of Hospice and Palliative Care, National Society of Allied and Independent Funeral Directors and Black Thrive. Organisations used email distribution lists, newsletters and/or social media; to promote accrual, the survey link was advertised via social media, press releases and personal contacts. Survey instructions asked recipients to forward links to others who may be interested in taking part, enabling snowball sampling and maximum survey reach. Data was collected between 1st June 2020 and 30th September 2020. Responses were anonymous unless respondents supplied their name and email address in the optional final field to indicate interest in further research. Additionally, respondents were invited to participate in an in-depth qualitative interview about their experiences; the results are published elsewhere. 12
Data analysis
Quantitative data were analysed using descriptive statistics within SPSS (version 26). Associations between specific respondent and deceased individual characteristics and care settings (independent variables) and whether respondents perceived themselves to be adequately supported (dependant variable) were analysed using univariate and multivariate logistic regression analyses.
Qualitative analysis of the free text data was conducted using Braun and Clarkes’ 13 principles of inductive thematic analysis. The analysis was conducted by CRM and SRM, who familiarised themselves and independently coded the data, then developed themes. They collaboratively reviewed and revised the themes, in conjunction with the quantitative data, and with the wider research team through critical dialogue. This approach was undertaken to enhance and illustrate study findings. 14
Ethical considerations
The study protocol was approved by the University of Liverpool Central Research Ethics Committee (Ref: 7761). Potential participants viewed the ‘Participant Information Sheet’ on-line, which outlined details including the study purpose, details of data storage and use and contact details for organisations which could provide bereavement support. All respondents provided informed, online consent. Due to the sensitive nature of the survey content, there was no forced response/requirement for participants to answer all questions. Additionally, a specified time period between the death and completion of the survey was not stated, allowing individuals to decide the ‘right time’ for them.
Results
Response rate
From 384 potential respondents who accessed the survey, 79 (20.6%) consented to participate in the study but did not complete the questionnaire. From the remaining 305 respondents, 27 completed demographic details only (non-respondents) and 278/384 (72.4%) completed the questionnaire (respondents). There was no statistically significant difference between respondents and non-respondents for gender (p = 0.25) or mean age (p = 0.1). The deceased individuals from the respondents’ group were predominately older in age compared with the non-respondents’ group (mean age 81.6 years (SD 12.2) vs 68.8 years (SD 18.1), p = 0.001). Free-text comments were provided by 34% (n = 104) of respondents.
Demographics for respondents and the deceased individuals
The mean age of respondents was 53.4 years (median 55.0 years, range 19–68 years). All except one respondent was from a White British ethnic group. Over three-quarters identified as female (216, 78.0%) and over half were the ‘son/daughter’ of the deceased individual (157, 56.5%).
The majority of deceased individuals died in England (179, 69.1%) and within their ‘usual place of care’ (192, 69.1%). Over half of the deaths occurred in a nursing care or residential home (162, 58.5%) (Table 1). Just under 10% (26, 9.4%) had died within a specific COVID-19 hospital ward. Almost a third of all deceased individuals (82, 32.0%) were thought to have COVID-19. Many of the deceased individuals had a chronic illness, the most common being dementia (148, 53.2%).
Demographic and relevant clinical details of deceased individuals and respondents and visiting restrictions (n = 278).
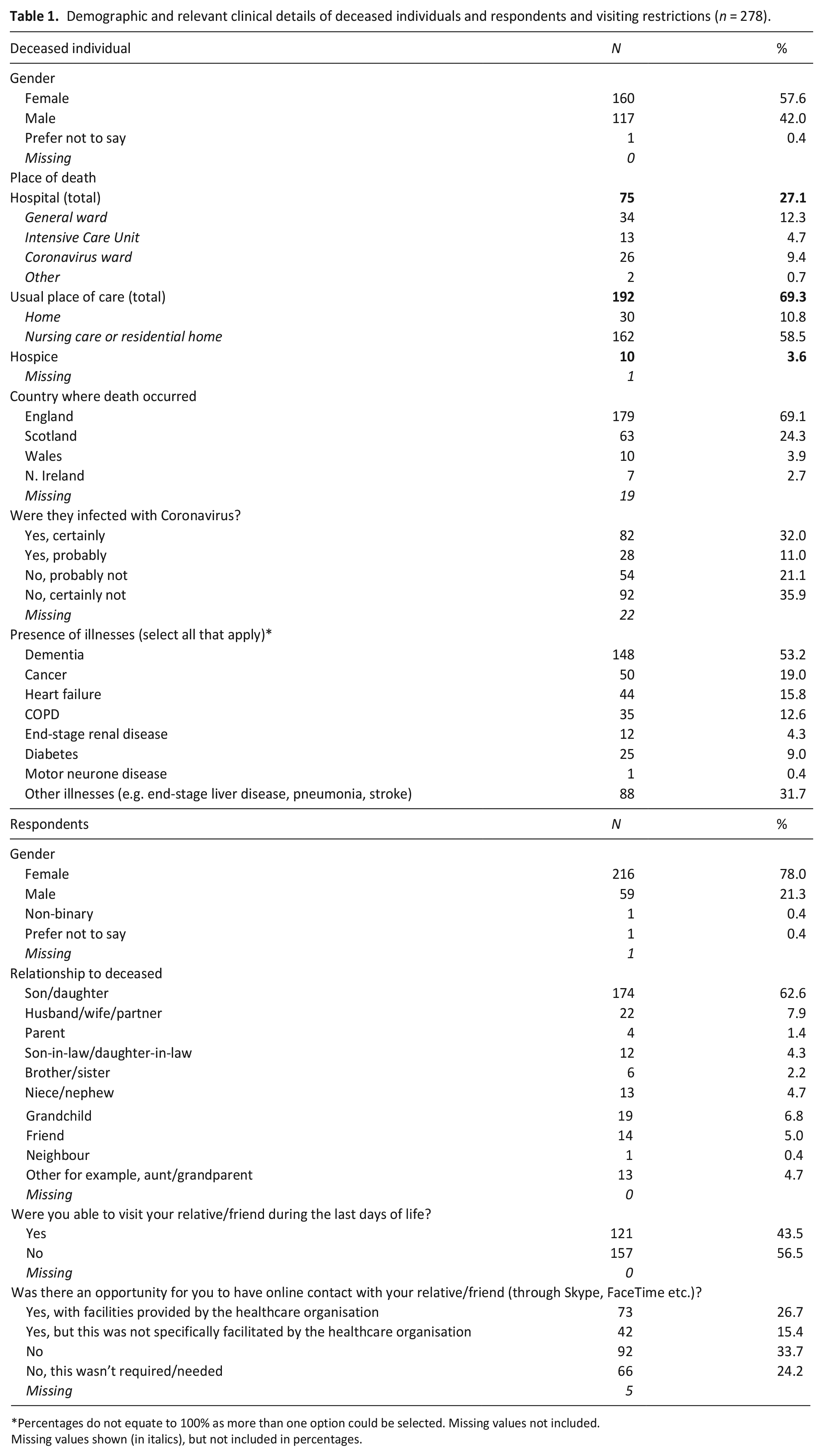
Percentages do not equate to 100% as more than one option could be selected. Missing values not included.
Missing values shown (in italics), but not included in percentages.
Themes
Using the quantitative survey data and the qualitative verbatim free-text responses, five conceptual themes were identified, linking to aspects of individualised care, under which aggregated results and analysis are presented. The themes include: (1) public health restrictions compounding the distress of ‘not knowing’; (2) disparate views about support from doctors and nurses; (3) challenges in communication and level of preparedness for the death; (4) delivery of compassionate care; (5) emotional needs and potential impact on grief.
Theme 1. Public health restrictions compounding the distress of ‘not knowing’
Pandemic restrictions meant that over half (157, 56.5%) of the respondents were unable to visit during the last days of life and a third (92, 33.7%) were unable to have any online contact (e.g. through Skype) (Table 1). Respondents clearly identified profound distress due to the impact of the restrictions, expressing sadness, guilt, anxiety, fear and feeling ‘cheated’.
‘due to visiting restrictions we were NOT allowed to visit on day of death which has lead (sic) to feels (sic) of guilt and letting my mother down. Had to ‘fight’ with care home manager to get my father and brother into visit her days leading up to her death.’ (Respondent 14, daughter, care home)
‘The NOT knowing is the worst part of all this. Not being able to see my sister on the day she lay dying when she did NOT have covid was awful’ (Respondent 31, brother, hospital)
Descriptions of the impact and effect of the restrictions were present whether or not the dying individual had COVID-19. For example, the loss of the usual level of interaction with healthcare staff meant opportunities to build supportive relationships were limited. Uncertainties about levels of care, and who was providing care, caused significant distress.
‘I have to take on trust that strangers looked after him in his dying hours.. . ..It is like you just have to put these people you have cared for and loved on a flimsy raft on the ocean and hope that their journey will be a safe one.’ (Respondent 125, daughter, care home)
Theme 2. Disparate views about support from doctors and nurses
Respondents reported a greater level of confidence and trust in nursing staff compared with doctors (Table 2). Additionally, respondents indicated nursing staff more frequently had provided care with respect and dignity. For example, almost half of respondents (119, 48.4%) perceived that nursing staff had treated their family member with dignity and respect ‘all of the time’. The same question asked of doctors received less than a third of responses (75, 31.1%) although for both groups, there was a high proportion of ‘don’t know’ responses.
Respondents’ perceptions about quality of care and communication (n = 278).
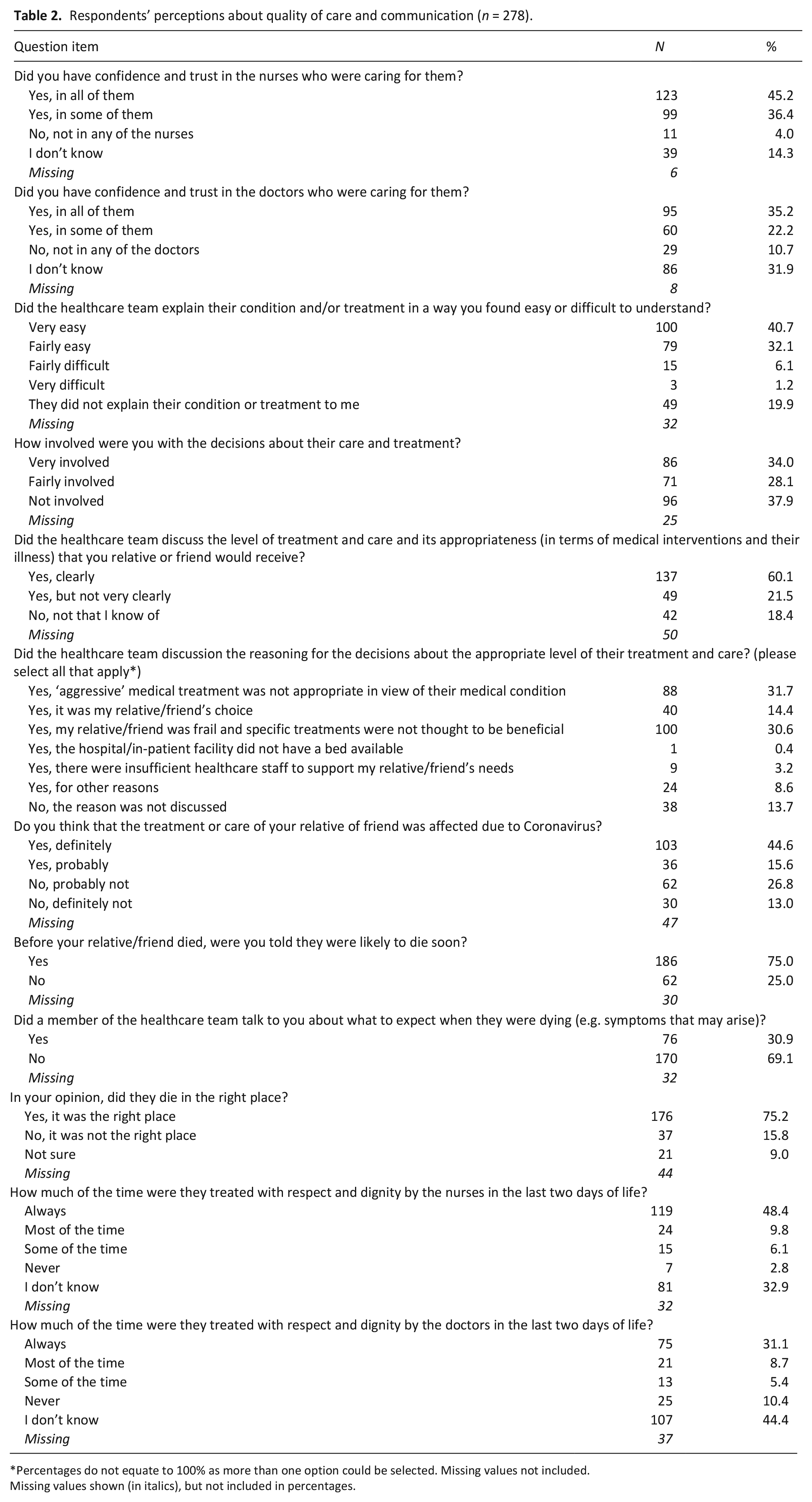
Percentages do not equate to 100% as more than one option could be selected. Missing values not included.
Missing values shown (in italics), but not included in percentages.
Respondents experiencing the death of a family member within the community setting shared differing perceptions about the level of support provided by nursing staff and doctors. They reported an absence of the usual continuity of care and visits from their General Practitioner (GP).
‘The level of care provided by the GPs was considerably less than I would have expected. There were no GP visits to the home for at least two months up to my mother’s death. The care provided by the Nurses was superb. My mother’s death was certified by a GP via a mobile telephone using a torch and Skype.’ (Respondent 180, daughter, care home)
There were many examples, however, where doctors were supportive. In situations where direct presence was possible, perceptions about the medical care were positive, with clear decision making facilitated through active family engagement to advocate wishes/preferences evident.
‘The GP was great and the treatment decisions were ‘right’ and led by me as my dads advocate. . .’ (Respondent 125, daughter, care home)
Theme 3. Challenges in communication and level of preparedness for the death
Almost half of respondents perceived their family members’ care and treatment was definitely affected due to COVID-19 (103, 44.6%) (Table 2). Nearly a fifth of respondents did not receive a meaningful explanation about their family members’ condition and/or treatment (49, 19.9%) and over a third did not perceive themselves to be involved in decisions about care or treatment (96, 37.9%). Communication with health and social care teams was reliant on remote methods, usually via telephone, which created a disconnect between families and the relevant healthcare teams. Those not identified as the immediate next-of-kin were dependent on ‘second-hand’ information. Respondents reported being frustrated by not receiving desired and required information about their dying family member, or the efforts needed to obtain reliable communication.
‘With no direct contact with my 97 yr old Welsh speaking uncle, I found communication with the hospital/staff dire. Ringing 6 times a day with no answer on the ward/nurse looking after him gone on break.. . ..My uncle was moved twice without ward informing us.’ (Respondent 58, niece, hospital)
At least three quarters of respondents were informed that their family member was likely to die soon (186, 75.0%). A much smaller proportion, however, were told about what to expect when their relative was dying (76, 30.9%) (Table 2). Communication was not always sufficiently clear or consistent when conveying that death may be imminent or what changes could be expected. Additionally, respondents perceived they were not provided with sufficient time to say ‘goodbye’, and to help prepare psychologically for the death of their family member.
‘There was a lack of communication. We were told conflicting information so could not plan for his death in the way we had always intended. We had to say goodbye on the nurses mobile via WhatsApp.’ (Respondent 117, granddaughter, care home)
Respondents reported it would have been helpful to have more regular, proactive calls with health and social care teams regarding their dying family members condition.
‘Feel very strongly that one phone call every day be made by staff to nok* with update on relative.’ (Respondent 58, niece, hospital) (*meaning ‘next-of-kin’)
Theme 4. Delivery of compassionate care
Three-quarters of respondents perceived their family member died in the ‘right’ place (176, 75.2%) (Table 2). Despite many reported challenges arising from the pandemic, respondents perceived health and social care teams were doing an ‘exemplary job’. Situations were described where kindness was shown in the personal aspects of care, such as washing and brushing hair which brought comfort. Local leadership within care homes was highlighted as having a profoundly positive impact, with intuitive thinking and timely visits prior to death being regarded as highly important.
‘In the days leading up to my Mother’s death I feel that we were lucky to have the support of the head nurse at my Mother’s care home. It was she that thought if (sic) the priest for the last rites and allowed us a visit four days prior to Mum’s death, it was also the Head nurse that allowed us to FaceTime to her personal mobile. Without her acts of kindness I believe that our experience would not have been as positive. . ..’ (Respondent 163, daughter, care home)
‘We were lucky enough to have great faith the capabilities of the Nursing Home Manager and we knew that my husband would not die until he had said goodbye, when the time was right, and she knew, I was allowed in to visit. . .. I had confidence that he was in the right place but knew he was waiting to say goodbye before he could ‘go’. (Respondent 194, wife, care home)
Theme 5. Emotional needs and potential impact on grief
Overall, almost half (110, 45.5%) of the respondents perceived that their own support was inadequate in the last days of life (Table 3). Some respondents (71, 30.1%) perceived the emotional support provided by the healthcare teams to be ‘poor’; also reflected in perceptions about the support available at the actual time of death (Table 3).
Respondents’ perceptions about their own emotional support provided by the healthcare team (n = 278).
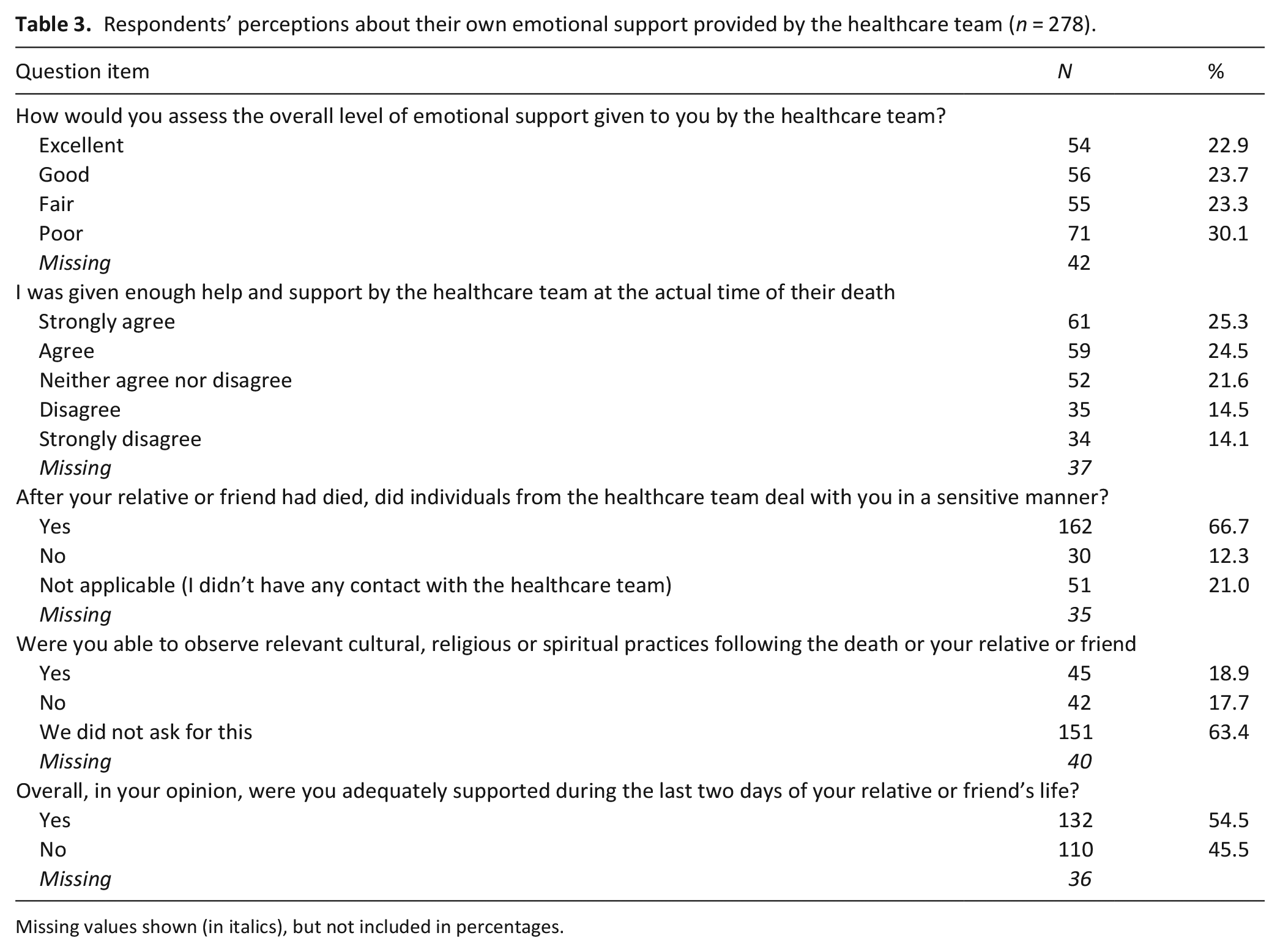
Missing values shown (in italics), but not included in percentages.
Respondents reported there was a lack of regard for meeting families’ needs and providing psychosocial support. This predominately related to the issue of social isolation, enforced by pandemic restrictions, limiting access to provide direct support to their relative, being able to visit and the opportunity to view the deceased individual.
‘However he had covid 19 symptoms and this meant that we were not able to access hep (sic) and support. We cared for him almost completely on out (sic) own.. . ..Even his body was treated disrespectfully by the funeral director when he was taken form (sic) the house, and we were not allowed to see him again.’ (Respondent 57, daughter-in-law, own home)
Respondents provided their initial reflections about the impact of the bereavement and potential issues which may arise in their grief. Experiences were described as ‘traumatic’; some being uncertain whether they would ‘ever get over it’; or struggling to make sense of their situation.
‘.. . ..very difficult not being with my father during his last days and time of death.. I had visited daily for three years up to the lockdown.. this will have a lasting impact on me and I struggle with closure’ (Respondent 171, son, care home)
Predictive factors for adequate family support in the last days of life
In order to assess whether key demographic or clinical factors independently predicted perceived support, univariate and multivariate regression analyses were conducted. The variables chosen (respondents’ age, gender, relationship to deceased, ability to visit, presence of dementia and place of death) are recognised risk factors for complicated grief (gender, relationship to deceased) 15 or are indirectly associated with levels of preparedness and support (age, ability to visit, presence of dementia, place of death) which have impact on psychological outcomes in bereavement. 15 The ‘relationship to deceased’ was categorised into ‘husband/wife/partner’, ‘son/daughter’, ‘grandson/granddaughter’, with other relationships grouped as ‘other’.
The variables univariately associated with perceived support were respondent gender and ability to visit (Table 4). Men were almost three times more likely to report being adequately supported compared to women (adjusted OR 2.9, CI 1.44–5.94, p = 0.03). Those able to visit were twice as likely to report being adequately supported during the last days of life, compared to those unable to visit (adjusted OR 2.2, CI 1.3–3.75, p = 0.04) (Table 5).
Univariate analysis of specific demographic and clinical details predicting likelihood of bereaved relatives perceiving they were adequately supported in the last days of life.
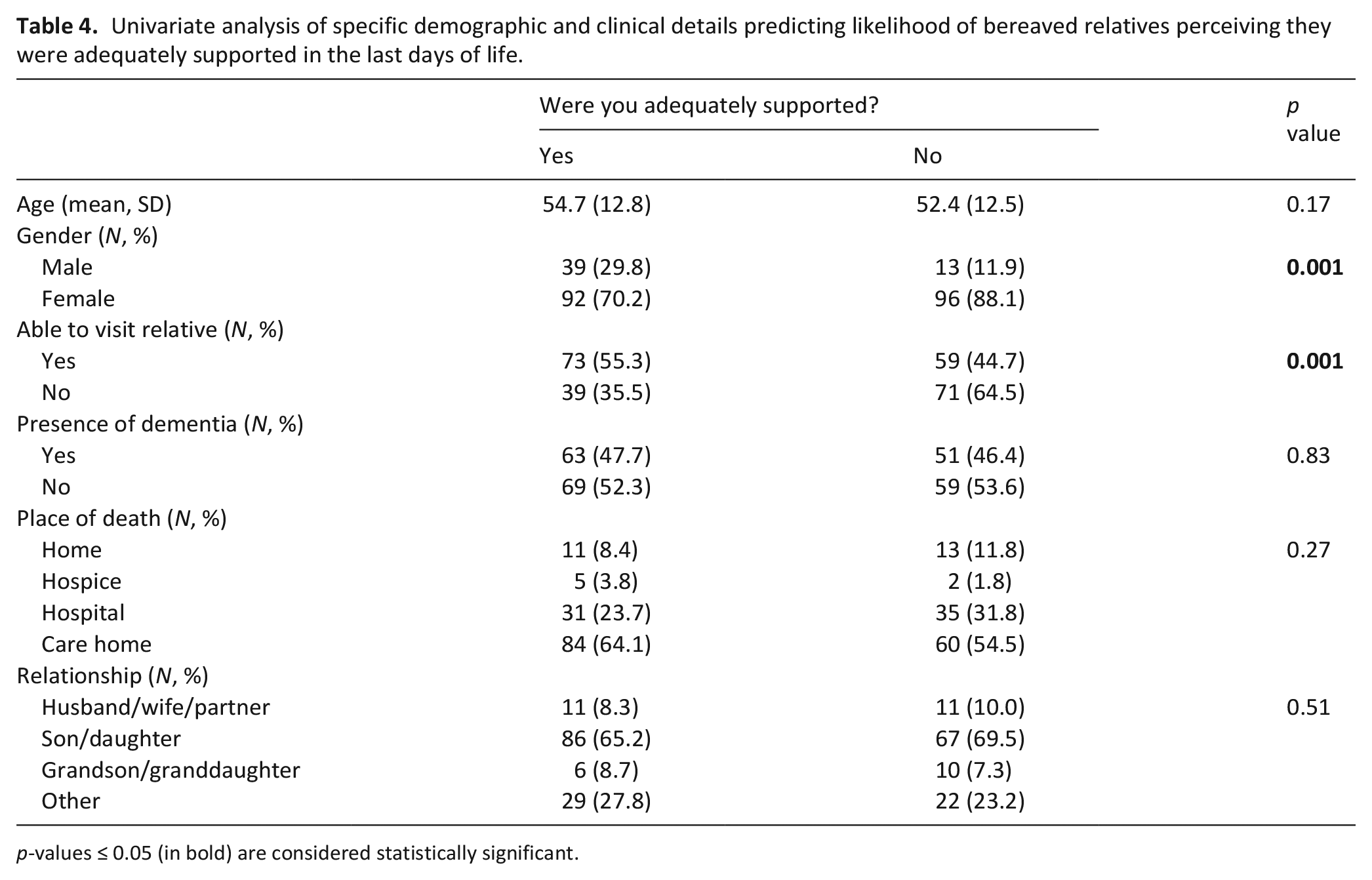
p-values ≤ 0.05 (in bold) are considered statistically significant.
Multivariate analysis predicting likelihood of bereaved relatives perceiving they were adequately supported in the last days of life.
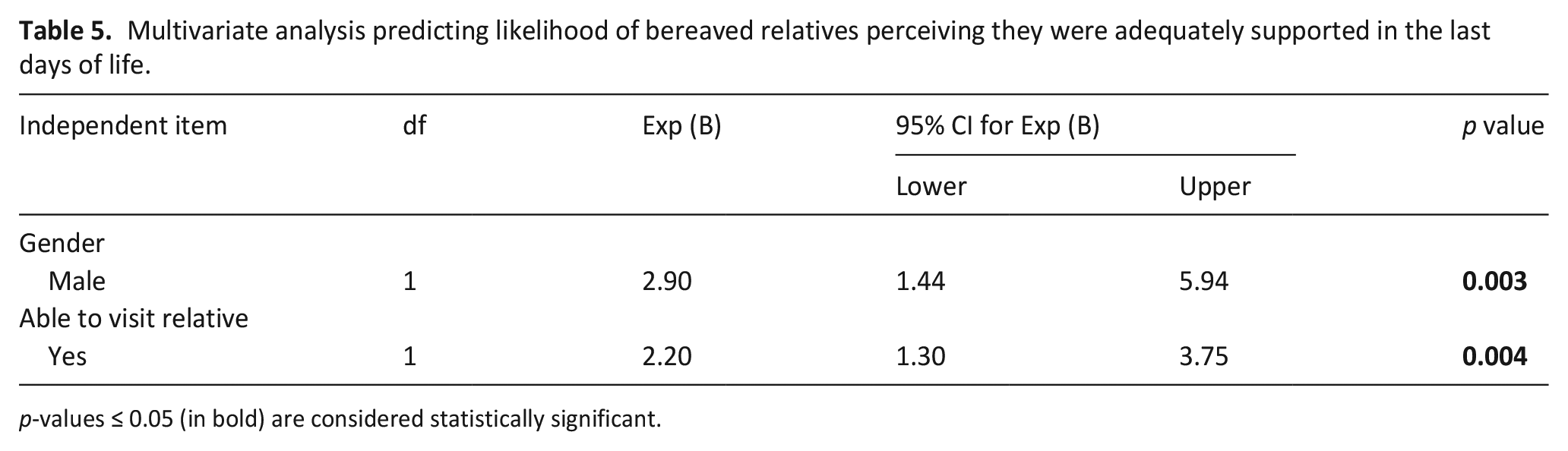
p-values ≤ 0.05 (in bold) are considered statistically significant.
Discussion
Main findings
Being unable to visit during the last days of life affected preparedness for the death, perceived levels of emotional support and compounded distress. Providing compassionate care, enabling connection, clear and timely communication and the ability to be present to ‘say goodbye’ were identified as fundamentally important in helping provide individualised care. Further, being able to visit was independently associated with bereaved relatives’ perceptions about adequate family support in the last days of life. Of interest, and anomaly, is that men were significantly more likely to feel adequately supported than women. We found no explanatory patterns for this within the qualitative data.
What this study adds
Our findings demonstrate the tensions arising between public health measures to restrict the spread of COVID-19, and the ethos of ‘palliative care values’ in providing holistic care. Indeed, poorer perceptions were expressed about dignity and respect, family support and communication, for example, what to expect when an individual is dying, compared with pre-COVID-19 studies which have used the CODE™ questionnaire.15,16 Results highlight the importance of proactive, timely and informative communication between health and social care professionals and family members, in keeping with previous recommendations. 17 This requires prioritisation, adequate training, preparation and protected time for regular patient updates. A previous study of family members’ information needs within a single end-of-life care unit under COVID-19 visiting restrictions, showed ‘information about hospital regulations/procedures’ and ‘patient health updates’ were regarded as the most important needs. 18 In order to provide holistic patient updates, information to family members include aspects of medical care and personal care, such as details and discussion surrounding individual preferences and wishes.
Our qualitative study (linked to this survey), 12 details relatives’ experiences when a family member was dying and reported how crucial it was to maintain connection, virtually or otherwise. The current study highlights this, especially within the care home setting, where restrictions had a pronounced impact on emotional well-being and the use of technology was not without issues. This current study provides a more inclusive landscape of acute and community settings (including deaths at home, nursing homes and hospices) and particularly highlights the disparate views perceived between doctors and nurses.
Recognition of the dying phase of illness is challenging, particularly for those with dementia, where disease trajectory is complex and variable. 19 The rapid and unpredictable dying phase of COVID-19 posed new challenges for clinical teams in recognising that death may be approaching. However, where local leadership anticipated changes and enabled timely visits, this had a profoundly positive affect. Further education and research focused on enabling health and social care staff to recognise dying and feel confident to talk honestly with relatives about this, should be prioritised.
Men were significantly more likely to feel adequately supported. This finding may relate to females being more prone to disclose emotional challenges in their coping. 20 Additionally, female caregivers may subjectively experience higher distress and perceive less support from others, including the clinical team. 21 The loss of the usual support networks, this may have compounded distress levels, to which future research could explore.
Strengths and limitations
This research represents the first UK study of bereaved relatives’ views about quality of care and family support provided during the last days of life and highlights the challenges and emotions experienced during the COVID-19 pandemic. COVID-19 studies from the Netherlands, United States and China,22 –25 have explored acute grief and the psychological impact during the bereavement period. This study, however, closely examines the quality of the dying experience which can have subsequent impact on grief.
Our study has limitations. Firstly, the convenience sample (with no specific sample size calculated) limits generalisability. Despite efforts to disseminate widely, respondents tended to be relatives of older individuals dying in community settings. All but one respondent was from a White British ethnic background, limiting the representativeness of the sample. Secondly, for some questions, there were a high number of missing responses; in view of the sensitive subject matter, we did not stipulate/require respondents to answer all questions, enabling respondents to contribute what they were comfortable sharing. Additionally, certain questions had a high proportion of ‘don’t know’ responses, potentially due to restricted visiting and lack of information. Despite these limitations, our findings were consistent with the results from the qualitative study, 12 adding strength to the clinical implications for practice.
Conclusion
Though challenging, public health measures in response to a pandemic can be actioned in ways that maintain high quality of end-of-life care for patients and their families. Care services must acknowledge the significance of individual deaths and ensure active approaches to support those who are bereaved. This may achieve headway in healing the barriers between what was required to limit the spread of the virus and the subsequent compromise on individualised care. Recognising dying, communicating holistic aspects of care and enabling visits whenever is possible, should continue to be priorities, during the ongoing pandemic. These approaches should be allied with risk stratification measures to help identify those in most need of bereavement support, including the identification of those unable to visit.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163211019885 – Supplemental material for Are public health measures and individualised care compatible in the face of a pandemic? A national observational study of bereaved relatives’ experiences during the COVID-19 pandemic
Supplemental material, sj-pdf-1-pmj-10.1177_02692163211019885 for Are public health measures and individualised care compatible in the face of a pandemic? A national observational study of bereaved relatives’ experiences during the COVID-19 pandemic by Catriona R Mayland, Rosemary Hughes, Steven Lane, Tamsin McGlinchey, Warren Donnellan, Kate Bennett, Jeffrey Hanna, Elizabeth Rapa, Louise Dalton and Stephen R Mason in Palliative Medicine
Footnotes
Acknowledgements
We wish to thank all the bereaved relatives who participated in this study, the contributions from the online advisory panel of the Clinical Research and Innovation Office at the Sheffield Teaching Hospitals NHS Trust and from Jacqui Gath, lead PPI representative, Clinical Cancer Trials Executive Committee. Additionally, we want to thank the many individuals and organisations who helped disseminate awareness about the study. We also wish to acknowledge Professors Agnes van der Heide and Ida Korfage for conceptualising the initial international collaborative project.
Author contributions
SRM, CRM, RH, TM, WD and KB designed the UK study. CRM led the PPI work. CRM, SRM, RH, TM, WD and KB developed the survey. All authors were involved in the survey dissemination and data collection. CRM and SRM analysed and interpreted the data with statistical support provided by SL. CRM drafted the manuscript. All authors have reviewed the article critically for clarity and intellectual content, provided revisions and have approved this version for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Catriona R Mayland is funded by Yorkshire Cancer Research ‘CONNECTS’ Fellowship scheme.
Ethical approval
The study protocol was approved by the University of Liverpool Central Research Ethics Committee (Ref: 7761). The study was conducted in accordance with the Declaration of Helsinki and all respondents provided informed, online consent.
Data management and sharing
Data sharing requests would be available on reasonable request and should be directed to Dr. Stephen R Mason,
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.