
Abstract
Background:
Dementia is a life-limiting disease with high symptom burden. The Integrated Palliative Care Outcome Scale for Dementia (IPOS-Dem) is the first comprehensive person-centered measure to identify and measure palliative care needs of people with dementia. However, such a measure is missing in the German health care system.
Aim:
To develop a culturally adapted German version of the IPOS-Dem and determine its content validity as a foundation for comprehensive psychometric testing.
Design:
Cognitive interview study with intermittent analysis and questionnaire adaptation. Interview guide and coding frame followed thematic analysis according to Willis complemented by Tourangeau’s model of cognitive aspects of survey methodology: comprehension, retrieval, judgment, response.
Participants:
Purposive sample with professionals (n = 29) and family carers (n = 6) of people with advanced dementia in seven nursing homes and person’s own home care in four interview rounds (n = 11; 10; 7; 7).
Results:
IPOS-Dem was regarded as comprehensive and accessible. Cultural adaption pertained to issues of comprehension and judgment. Comprehension challenges referred to the person-centered concept of “being affected by” used in the POS-measures. Judgment problems related to persons with limited communication causing challenges in assessment.
Conclusion:
Most issues of cultural adaptation could be addressed by questionnaire modifications. However, interviews unveiled fundamental challenges for using proxy reported person-centered assessments. Continuous training on how to use the instrument is imperative to integrate the person-centered approach of palliative care into nursing homes as a key provider of generalist palliative care for people with dementia. The refined version is ready for psychometric testing.
Keywords
Older people with dementia and multi-morbidities may have high symptom burden which may be undetected and therefore untreated, resulting in distress.
Person-centered outcome measures may support comprehensive assessment to improve outcomes. In people who are unable to self-report due to advancing dementia, proxy-reported measures are needed.
IPOS-Dem is a proxy-reported outcome measure allowing comprehensive assessment of symptoms and concerns experienced by people with dementia.
Cognitive interviewing is recommended for determining content validity and cultural translation, and adaptation of questionnaires.
We present a culturally adapted version of the IPOS-Dem questionnaire incorporating both cultural differences regarding German language and country characteristics as well as organizational and professional specifics on an international level.
This study demonstrates the benefit of an iterative approach of cognitive interviews for a context-specific validation and adaptation of measurement tools.
This paper identifies challenges associated with person-centered proxy assessments for persons with limited communication abilities.
Integrating a palliative care approach into settings caring specifically for people with dementia will require a mutual agreement of terms, concepts, and philosophies of care.
It is necessary to develop tailored training material to integrate the person-centered approach of palliative care across primary care settings with regards to its context.
The German IPOS-Dem is undergoing further testing to enhance its psychometric properties (validity and reliability), its practicality, and its use for clinical practice in primary care settings for people with dementia.
Background
The prevalence of dementia is projected to increase worldwide from 46.8 million people in 2015 to 74.7 million in 2030, and over 131.5 million in 2050. 1 Dementia is a progressive life-limiting disease with a relatively high symptom burden. 2 People with dementia typically suffer from multiple co-morbidities associated with advancing age. 3 Nearly all people with moderate and advanced dementia experience personality changes, cognitive impairment, and neuropsychiatric symptoms such as anxiety, depression, hallucinations, and delusions.4,5 In addition, pain, constipation, and breathlessness are common. 6 This results in high burden and psychosocial concern that negatively impact on patients’ quality of life. Palliative care is beneficial for this patient group to improve quality of life, maintain function, and maximize comfort. 2
As people with advancing dementia are often unable to express their symptoms, concerns, or wishes, it is necessary that proxies carefully assess the patients’ condition and identify potentially burdensome symptoms. However, there are few measures that allow reliable assessment of symptoms in people with advanced dementia. Available measures only focus on certain aspects or groups of symptoms. 7 Until recently, no comprehensive person-centered questionnaire covering all relevant aspects existed. 8 To fill this gap, researchers from King’s College London (KCL) developed a dementia version of the Integrated Palliative Care Outcome Scale (IPOS), the IPOS for Dementia (IPOS-Dem) which is part of the POS family of measures.9,10
IPOS-Dem is a proxy-reported outcome measure allowing comprehensive assessment of symptoms and concerns experienced by people with advanced dementia. 11 The IPOS-Dem includes questions addressing the specific needs of people with dementia and other co-morbidities common in older people. These include, for example, difficulties swallowing, communication problems, or agitation. It starts with an open question asking about main problems and incorporates 31 items, including physical symptoms and psycho-social concerns. Each item is rated on a Likert scale from 0 (no concern/never) to 4 (overwhelming/always). 9 The English version is freely available at https://pos-pal.org/.
As in the UK, there is a lack of a comprehensive person-centered outcome measures for people with dementia in Germany. Furthermore, the IPOS-Dem has been developed together with nursing staff and relatives using lay language, which makes it particularly suitable for geriatric care since employees in nursing home institutions in Germany and Europe in general have mixed levels of qualifications with moderate to low native language proficiency. 12
The quality of a questionnaire is defined by its reliability and validity. 13 This also relates to the translation of an existing measure into another language and/or culture. 14 Before psychometrically testing the translated version, cognitive interviews are recommended to determine its content validity, which allows to adapt the questionnaire to the cultural context.14–17 This ensures that the wording of the translation is appropriate and that the concept of the measure is fully understood. The resulting version of the questionnaire can then undergo psychometric testing to establish further measurement properties. The aim of this study is (a) to develop a culturally adapted German version of the IPOS-Dem and determine its content validity and (b) to develop a version of the questionnaire as a foundation for comprehensive psychometric testing.
Methods
Study design
We conducted a cross-sectional, qualitative multi-center study using cognitive interviewing techniques with “think-aloud” and concurrent probing in several rounds. 17 The measure was refined after each interview round. The study design is grounded in an interactionist paradigm, emphasizing the interpretive effort of involved actors and the interplay between “culture” and “cognition.” Epistemologically, the approach encompasses a cognitive perspective, focusing on the “underlying cognitive processes through which respondents generate their answers to survey questions.” 18
The consolidated criteria for reporting qualitative research (COREQ) guidelines were followed. 19
Participants
Purposive sampling was used to ensure variations. We included professionals with different levels of qualification (secondary and tertiary), care personnel without specific qualification, and family carers of people with dementia. All participants provided care for people with advanced dementia in nursing homes or home care. To ensure the highest possible variation, the sampling frame for selecting participants further included the following criteria: age, sex, and first language (for sampling frame see Supplemental Appendix 1). Participants had to be over 18 years and have sufficient German language skills.
Recruitment was based on suggestions of the German expert panel and by contacting care homes known to the project team from previous professional contacts. Managers of nursing homes and home care services were contacted (by FH) and asked for contacts of professional and/or family carers to participate in the study. All potential participants received a written invitation with information about the study. If they were interested in participating, an interview was arranged.
All participants provided written informed consent.
Measure
The cognitive interviews built up on the translated IPOS-Dem in German. The forward and backward translation was realized beforehand following the criteria for translation as described in the Palliative Care Outcome Scale Manual for cross-cultural adaptation and psychometric validation. 14
Data collection
The amended interview guide (see Supplemental Appendix 2) was based on the cognitive interview study for the IPOS. 20 This was developed in line with Tourangeau’s model of cognitive aspects of survey methodology. 18 According to this model, participants need to (1) understand and interpret the question (comprehension), (2) retrieve the relevant information from memory (reflection), (3) use the limited knowledge to develop an answer (judgment), and (4) formulate or select the appropriate answer from given possibilities (response). 18
The IPOS-Dem questionnaire was presented to participants and they were invited to complete the questionnaire for a person with advanced dementia they provided care for. They were encouraged to think aloud throughout the process in order to understand his/her thinking or rationale for the provided answers. The four categories named by Tourangeau were applied for each individual question. In case of unexpected statements or conspicuous nonverbal reactions, the interviewer prompted with spontaneous queries. This combination of loud reflection and methodological questions from the investigator is recommended for cognitive interviews in clinical settings.21,22 In addition, the technique of “probing” was used to pose questions about specific concepts and terms of uncertainty emerging from the IPOS-Dem translation process and previous interview rounds. 23 The interview ended with a question on the comprehensiveness of the questionnaire. Interviews were conducted by an experienced qualitative researcher (FH) and a trained and supervised medical student (HH). Interviews were audio-recorded and transcribed verbatim by a professional transcriber.
Data saturation
Data saturation in the context of cognitive interviews means that the interviews do not contain any new information regarding the need to change the tested instrument. For cognitive interviews, several rounds of 5–15 interviews per round are recommended. 24 For our study, a total number of 20–30 interviews was expected to reach saturation.14,15,17,20
Data analysis
Interview transcripts were analyzed following thematic analysis according to Willis, complemented by categories basing on the four-level cognitive model of Tourangeau.17,18 The analysis followed a deductive-inductive approach by first applying the theory based categories of Tourangeau’s model to the data deductively, followed by the process of inductively identifying underlying meanings and connections in the selected text fragments. Individual interviews were analyzed by HH and FH. Discrepancies were discussed between HH, FH, and CB. Data for each category were combined across all interviews of one interview round. After each interview round, results were discussed with members of the KCL development team of the original IPOS-Dem (CES, CJE) and a German expert-panel (including two geriatricians, one old age psychiatrist, one internist, one manager of a nursing home with geriatric nursing background, one nurse, one representative each of the German Alzheimer Society and the Bavarian Ministry for Health and Care, two representatives of patient and public involvement). Additionally, after the third round, results were discussed in an international stakeholder workshop on IPOS-Dem development and use. The results of each interview round were integrated into IPOS-Dem. The modified questionnaire was then used for the next round of interviews (see Figure 1). Microsoft Excel 2016 was used to support data management.
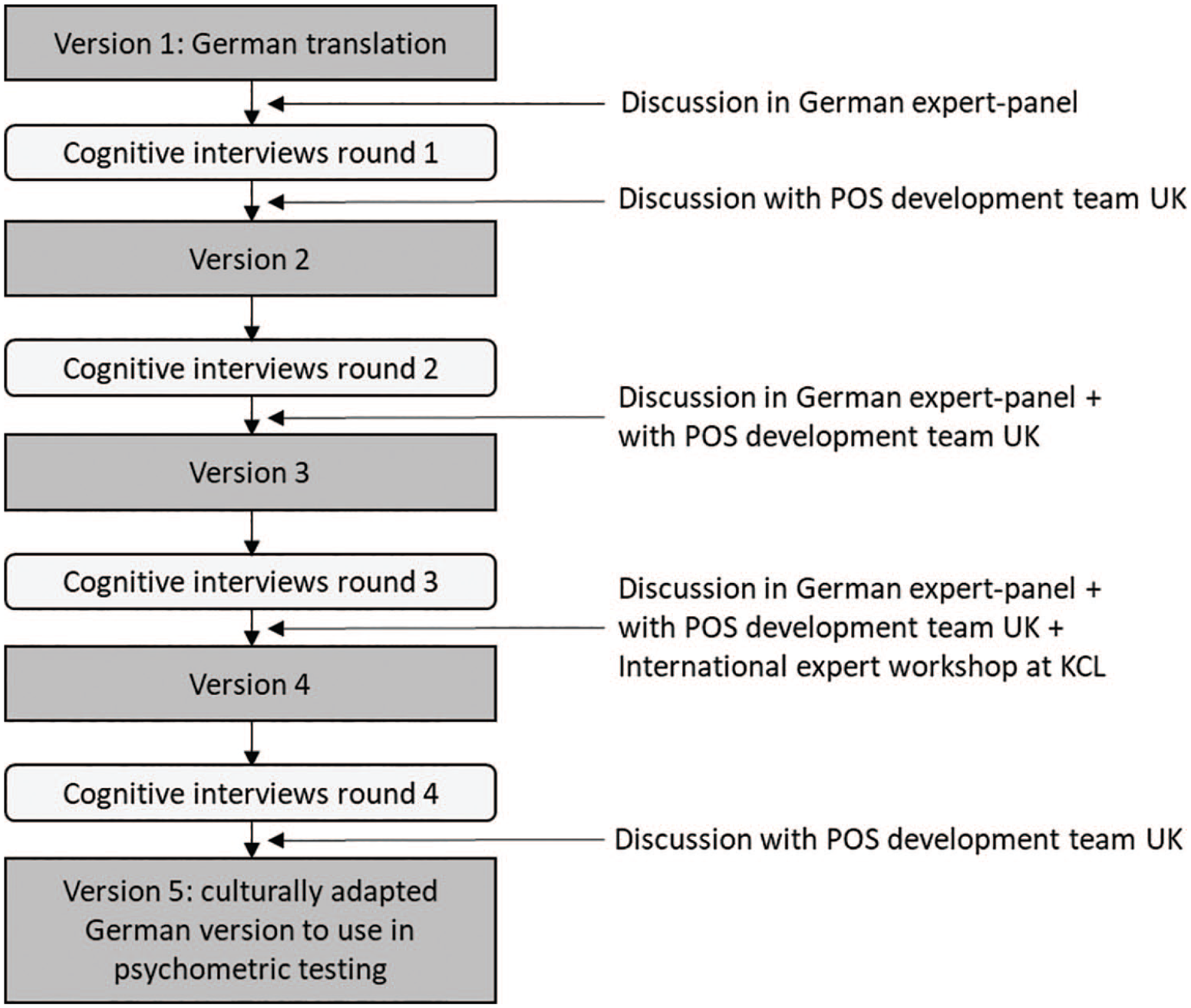
Illustration of the proceeding in the four interview rounds.
Ethics approval
The study was approved by the Local Research Ethics Committee of Ludwig-Maximilians-University Munich (reference number 17-763).
Results
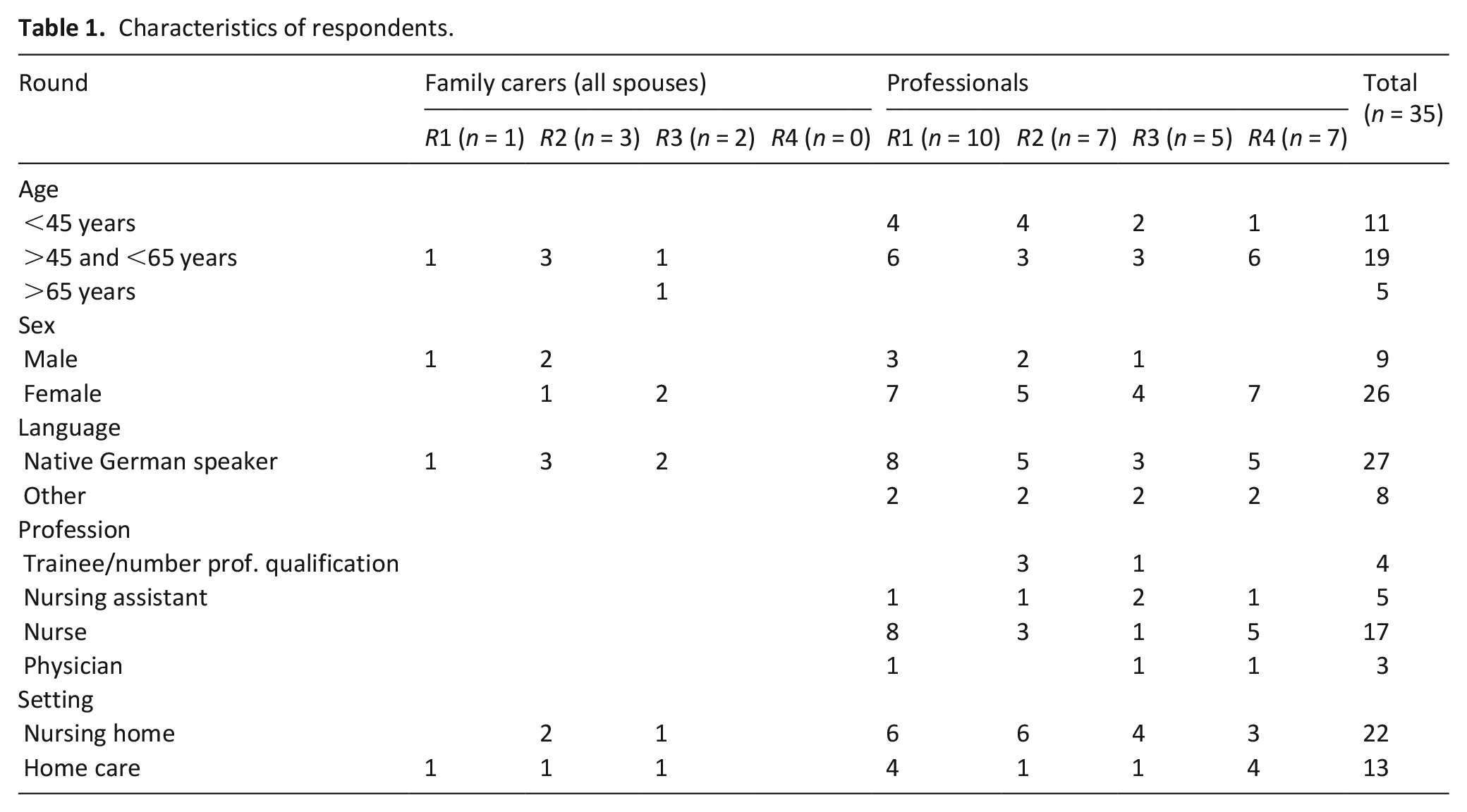
35 interviews were conducted in four rounds (n = 11; 10; 7; 7) with nurses with different qualification levels, care personnel without specific qualification, physicians from seven nursing homes or nursing services, and family carers. Interviews were conducted from February to November 2018 and lasted between 17 and 54 min. In the fourth round, only professionals were interviewed due to a specific issue arising from the third version of IPOS-Dem. Characteristics of respondents are shown in Table 1.
Characteristics of respondents.
Overall, IPOS-Dem was regarded as comprehensive and easy to use. Problems emerging from the cognitive interviews were mainly related to comprehension and some to judgment and response. Problems of response were connected to problems of comprehension and judgment and are therefore not described separately. No problems emerged regarding retrieving/reflecting the information provided by the IPOS-Dem amongst participants.
Comprehension
Problems with comprehension necessitated revision of some items. Table 2 provides an overview of the items in the initial IPOS-Dem and the modified German version (for more details on the iterative modification of items see Supplemental Appendix 3). For some items, problems were related to wording of the German translation and could easily be solved by adapting the wording (e.g. “hallucinations and/or delusions,” “Wandering”). In other items, clarifying explanations (e.g. “drowsiness,” “sleeping problems,” “difficulty communicating”) were added to improve understanding.
Overview changes between initial IPOS-Dem version and culturally adapted IPOS-Dem version.
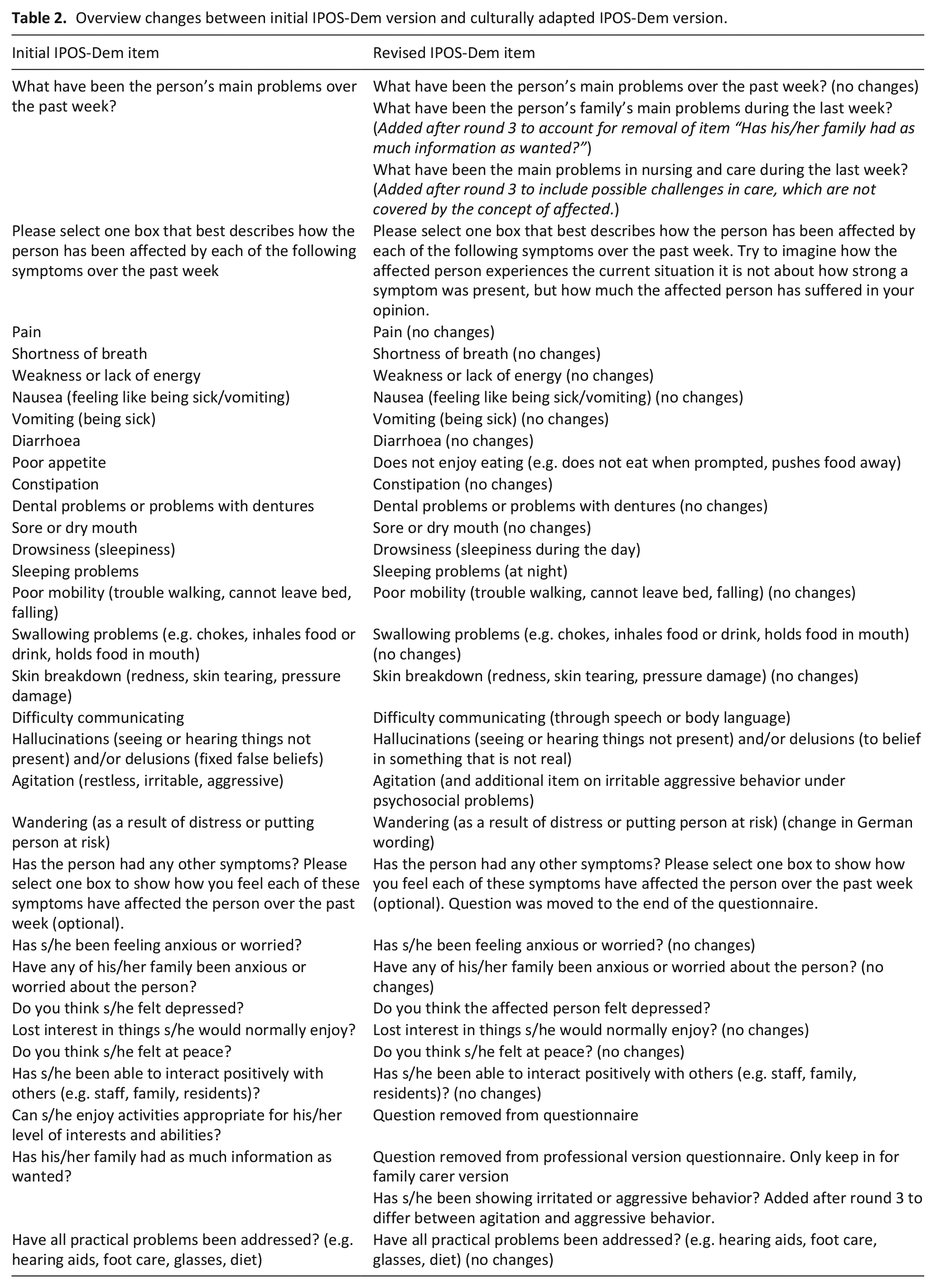
Two items were removed from the questionnaire because of poor comprehension: “Can s/he enjoy activities appropriate for his/her level of interests and abilities?” and “Has his/her family had as much information as wanted.” Also, given that the IPOS-Dem is considered to be used by professional carers, these questions would aim at self-assessment of the carers respectively or assessment by the carers of the nursing home.
The item “agitation (restless, irritable, aggressive)” was split into two items since the majority of respondents indicated (both spontaneous and prompted) that they considered aggression and restlessness as two different symptoms.
All POS measures are based on being person-centered. Hence, the leading question throughout the questionnaire is how much the person is affected by a problem or symptom. This is in contrast to other outcome measures asking about the presence and/or severity of a symptom or problem (e.g. PAINAD
25
). This concept of “being affected by” in the question referring to all physical symptoms was challenging and not understood uniformly:
: “That doesn’t make sense. Sorry to say that but in constipation and diarrhoea, “not at all” and “slightly” doesn’t fit. Constipation often, rarely, never. Diarrhoea often, rarely, never. But what does constipation severely mean?”. (R1I10)
„Well, here maybe, no idea, maybe a number would be sensible. I don’t know, zero to three hours additional to the night’s sleep, or something like that.” (R2I3)
In each consecutive round, some respondents understood the question in terms of presence/severity of a symptom and others in terms of “being affected by.” The wording was adapted and complemented with an explanation. The version tested in the fourth round demonstrated the best understanding of the concept, however still not uniformly. Furthermore, while some respondents indicated that they clearly understand the concept of “being affected,” they still had difficulty applying it in practice accordingly. A physician using the IPOS in clinical care stated “Well, what I think, what is difficult again and again is to point out that it refers to being affected (. . .) I find it, also in the general IPOS, I find it difficult to remember that this is not about symptoms I notice professionally but about the being affected.”(R3I7)
Discussions with the German expert-panel indicated that focussing on the subjective burden of a person could potentially exclude important information. Certain behavior or symptoms might not be experienced as very burdensome by people with dementia but might have major implications for their care. To account for this, an additional open question was added in the beginning: “What were the main problems in nursing and care during the last week?”
Judgment
Respondents assessed the answer options and time frame of 1 week as appropriate. Judgment problems were generally related to persons unable to communicate, resulting in uncertainty regarding the presence of a symptom/problem, or the reason behind a certain behavior.
The majority of professionals and family carers did not have any difficulties assessing symptoms in persons having difficulties or being unable to communicate. However, some respondents had difficulties judging the presence of symptoms, for example, pain, breathlessness, and nausea.
“Because I cannot observe that. But I don’t want to say, if I don’t observe it, that it might not exist after all.” (R2I5 on breathlessness).
“With many people, especially in this person, it is not possible to say, whether he, it is a man, whether he is in pain or not.” (R1I4 on the example pain).
Problems with judgment were expressed most often for the symptom “hallucinations,”
“Hallucinations, no, well things like that, we have that, but this is also related to, well they would need to be able to express themselves.”(R2I6).
The question “Lost interest in things s/he would normally enjoy?” also proved to be challenging. Some respondents found it difficult to evaluate what brings joy to people with dementia because of the limited capacity to communicate clearly.
“This is very difficult to answer in her case. No, she, well, she can speak, but she is already very limited in her life situation.” (R1I3)
Acceptability, layout, and missing items
The English version of the IPOS-Dem has numbered questions, which however do not follow a continuous order. This was perceived as confusing by respondents and numbers therefore removed from the questionnaire.
“Ah, okay, one, two, three. Three? Where is? Can I now? Where is, one, two? Eh? Alas, for god’s sake. That is one, that is two, and that is three. Okay.” (R1I10)
Respondents tended to report psycho-social symptoms such as “anxiety” in the free text question. As these psycho-social symptoms are covered in subsequent questions, the free text question was moved to the end of the questionnaire.
Additional symptoms not mentioned in the questionnaire
The majority of respondents evaluated the questionnaire as comprehensive. Symptoms mentioned to be missing were incontinence (by three respondents), motor symptoms/spasticity (by two respondents), and time distortions (by four respondents). As there is an option to address additional problems in the respective question for “any other symptoms,” no additional items were added to the questionnaire.
Discussion
This study informed about the development of a culturally adapted version of the German IPOS-Dem, resulting in a version for further psychometric testing. The adaptation followed an iterative process with the interim results being discussed not only in the German team but also with the English IPOS-Dem-development team, and international experts. This, in turn, informed adaptations of the English IPOS-Dem. Benefits deriving from an international approach were already highlighted in earlier work from the POS-development team and are encouraged by the results of the presented study. 20
The IPOS-Dem was regarded as a comprehensive and accessible person-centered outcome measurement to use by health care professionals and relatives. Insecurities in judging the persons’ presence of symptoms and challenges with the person-centered concept of “being affected by” became transparent.
Assessing subjective burden—“being affected by” instead of assessing severity of symptom
The concept of “being affected” was difficult to understand for participants and even those who understood the concept still did not apply it uniformly when answering the questions. In the German nursing care setting and its professional culture, the term “affected” has a specific meaning referring to the persons’ activities of daily living in terms of functional and cognitive limitations and is used as such in every-day work. A question using this term will most likely be understood and answered in line with this understanding, and not in the intended person-centered way. In consequence, the wording and palliative care related concept of “being affected” as used in palliative care cannot automatically be transferred and expected to function in the nursing care setting.
Furthermore, the prevailing paradigm in clinical and nursing care is still characterized by a focus on “objectifiable” symptoms, rather than the person’s lived experience. Assessment therefore usually is directed at the presence of and severity of symptoms or concerns, rather than the subjective burden experienced by the person in need of care. 26 On the other hand, it implies that person centeredness which is the core piece to palliative care is not yet well established in primary care with a generalist palliative care approach. 27 Therefore, using the IPOS-Dem systematically within a primary care population with palliative care needs, may provide a palliative care approach for people with dementia delivered by their primary care nurses and physicians.
Cultural validity within cultural context
Most problems identified in this study were related to comprehension which could be addressed by modifications of the questionnaire. The majority of modifications related to wording or specifications of items. However, the results also led to some major changes as we removed two questions (“enjoy activities appropriate for his/her level of interests and abilities,” “family had as much information as wanted”) and split one item (“agitation (restless, irritable, aggressive)”) into two. In our opinion, these changes strengthen the cultural validity of the overall measure compared to the initial German version, since they help to avoid misunderstandings, for example, due to divergent connotations of certain terms in different contexts, and hence reduce the chance of ambiguous answers in the assessment. While the respective changes were necessary to enhance the content validity of the German IPOS-Dem, these may not be applicable for versions in other languages or used in other cultural contexts.
Assessment when communication is not possible
The cognitive interviews demonstrated that professionals and family carers were overall able to assess most problems as a proxy for people with dementia. However, interviews also revealed some uncertainty as symptoms in dementia are challenging to assess because of the
Cultural adaptation
The understanding of
As stated in a Lancet Commission paper on culture and health, the
When we talk about integrating palliative care in other medical and care disciplines, disease trajectories, and care settings, we need to understand and critically reflect differences in, for example, values, symbols, practices, and language. As a discipline which per definition works with many other professional healthcare groups, palliative care needs to understand its own professional culture, and the cultures of those disciplines and working environments that it aims to be integrated into.
Methodological issues, strengths, and limitations
This study was conducted in four interview rounds. Compared to single round approaches, the iterative way to conduct interviews enabled a more in depth understanding of challenges in using the IPOS-Dem questionnaire as well as patient-centered measurement in palliative care in general. The sample of the study holds both strengths and limitations. A strength of this study is the heterogeneity of the sample in relation to professional and qualification background. However, due to an unequal composition of the study population equal distribution in terms of gender was not possible. More than 80% of nursing home staff is female. 35 As a result, women were over-represented in the sample. Even though we did not identify gender specific differences in the response behavior, we cannot rule this out.
Furthermore, we were only able to recruit 9 nursing assistants compared to 17 registered nurses. Although nursing assistants have accomplished skills in observing symptoms in people with dementia, 36 they are often not authorized to document symptoms and needs in nursing records. Therefore, they might have felt that they would not be able to contribute to our study because the measurement would be a task completed by registered nurses. 37 Reason for that may also lie within the recruitment process. Since participants were approached by managers of the participating institutions, and only upon their agreement introduced to the research team, no data on non-participation is available.
This study is part of a validation study of IPOS-Dem for use by professional carers. Therefore, the sample focused on professionals. We only included few family carers. Half of their relatives were cared for in a nursing home which means that the family carers were not able to provide care for their spouses. They were, however, still in close and frequent contact with the person with dementia, and thus to assist with the assessment their problems and concerns. As a carer version could be developed in the future, we were interested in identifying possible differences in the response behavior to learn about the necessity of separately testing the instrument. Because no differences were identified, we suggest that this version could also be used for a psychometric evaluation in family carers.
Based on the discussions of differences in professional cultures and the predominant palliative care background of the research team, findings could be challenged as being too much coined by the palliative care perspective. We addressed this by involving an expert-panel consisting of non-palliative-care professionals with a predominant geriatric and nursing home background.
Conclusion
A cognitive interview approach using several rounds of interviews proved to be useful to determine content validity in the development of a questionnaire. While the majority of problems emerging in the iterative interview rounds could be addressed by modifications of the questionnaire, interviews also unveiled fundamental challenges, and clinical implications for the use of person-centered proxy assessments such as IPOS-Dem.
Cultural adaptation of an instrument, usually related to different countries and languages, should as well be considered regarding different work and/or care settings. Also, development of training material is necessary to transfer the person-centered approach of palliative care to other care settings and cultures.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163211004403 – Supplemental material for Culture in the spotlight—cultural adaptation and content validity of the integrated palliative care outcome scale for dementia: A cognitive interview study
Supplemental material, sj-docx-1-pmj-10.1177_02692163211004403 for Culture in the spotlight—cultural adaptation and content validity of the integrated palliative care outcome scale for dementia: A cognitive interview study by Farina Hodiamont, Helena Hock, Clare Ellis-Smith, Catherine Evans, Susanne de Wolf-Linder, Saskia Jünger, Janine Diehl-Schmid, Isabel Burner-Fritsch and Claudia Bausewein in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163211004403 – Supplemental material for Culture in the spotlight—cultural adaptation and content validity of the integrated palliative care outcome scale for dementia: A cognitive interview study
Supplemental material, sj-docx-2-pmj-10.1177_02692163211004403 for Culture in the spotlight—cultural adaptation and content validity of the integrated palliative care outcome scale for dementia: A cognitive interview study by Farina Hodiamont, Helena Hock, Clare Ellis-Smith, Catherine Evans, Susanne de Wolf-Linder, Saskia Jünger, Janine Diehl-Schmid, Isabel Burner-Fritsch and Claudia Bausewein in Palliative Medicine
Supplemental Material
sj-docx-3-pmj-10.1177_02692163211004403 – Supplemental material for Culture in the spotlight—cultural adaptation and content validity of the integrated palliative care outcome scale for dementia: A cognitive interview study
Supplemental material, sj-docx-3-pmj-10.1177_02692163211004403 for Culture in the spotlight—cultural adaptation and content validity of the integrated palliative care outcome scale for dementia: A cognitive interview study by Farina Hodiamont, Helena Hock, Clare Ellis-Smith, Catherine Evans, Susanne de Wolf-Linder, Saskia Jünger, Janine Diehl-Schmid, Isabel Burner-Fritsch and Claudia Bausewein in Palliative Medicine
Supplemental Material
sj-docx-4-pmj-10.1177_02692163211004403 – Supplemental material for Culture in the spotlight—cultural adaptation and content validity of the integrated palliative care outcome scale for dementia: A cognitive interview study
Supplemental material, sj-docx-4-pmj-10.1177_02692163211004403 for Culture in the spotlight—cultural adaptation and content validity of the integrated palliative care outcome scale for dementia: A cognitive interview study by Farina Hodiamont, Helena Hock, Clare Ellis-Smith, Catherine Evans, Susanne de Wolf-Linder, Saskia Jünger, Janine Diehl-Schmid, Isabel Burner-Fritsch and Claudia Bausewein in Palliative Medicine
Footnotes
Acknowledgements
Thanks to the German expert-panel for supporting the whole validation process of the German IPOS-Dem and all the participating professionals and carers for their time and effort.
Author contributions
FH and CB obtained funding. Concept and design of the study: FH, CB. HH and FH conducted and analyzed interviews. CES and CE joined discussions in process of analysis and interpretation. JDS, IBF, SJ, SdW critically reviewed the manuscript for important intellectual content and contributed with expertise to the discussion of results. FH drafted the manuscript. CB commented the draft. All authors provided critical comments on drafts of the manuscript and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the private foundation “Ilse-Kubaschewski Stiftung.”
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.