
Abstract
Background:
Although guidelines recommend palliative care for patients with chronic obstructive pulmonary disease, there is little evidence for the effectiveness of palliative care interventions for this patient group specifically.
Aim:
To describe the characteristics of palliative care interventions for patients with COPD and their informal caregivers and review the available evidence on effectiveness and implementation outcomes.
Design:
Systematic review and narrative synthesis (PROSPERO CRD42017079962).
Data sources:
Seven databases were searched for articles reporting on multi-component palliative care interventions for study populations containing ⩾30% patients with COPD. Quantitative as well as qualitative and mixed-method studies were included. Intervention characteristics, effect outcomes, implementation outcomes and barriers and facilitators for successful implementation were extracted and synthesized qualitatively.
Results:
Thirty-one articles reporting on twenty unique interventions were included. Only four interventions (20%) were evaluated in an adequately powered controlled trial. Most interventions comprised of longitudinal palliative care, including care coordination and comprehensive needs assessments. Results on effectiveness were mixed and inconclusive. The feasibility level varied and was context-dependent. Acceptability of the interventions was high; having someone to call for support and education about breathlessness were most valued characteristics. Most frequently named barriers were uncertainty about the timing of referral due to the unpredictable disease trajectory (referrers), time availability (providers) and accessibility (patients).
Conclusion:
Little high-quality evidence is yet available on the effectiveness and implementation of palliative care interventions for patients with COPD. There is a need for well-conducted effectiveness studies and adequate process evaluations using standardized methodologies to create higher-level evidence and inform successful implementation.
Keywords
Patients with advanced COPD have a high symptom burden and impaired quality of life. Although guidelines recommend palliative care for patients with COPD, implementation remains often challenging and an up-to-date overview of the evidence on its effectiveness is lacking.
This review provides a comprehensive overview of evidence on the effectiveness and implementation of palliative care interventions targeting patients with COPD and their informal caregivers.
Within different care contexts, short-term palliative care assessments as well as longitudinal palliative care interventions with care coordination have been implemented. Highly valued intervention characteristics are the direct access to a professional for support, an ongoing relationship with a professional and education about breathlessness.
Few interventions have been evaluated using a controlled study design. Positive effects were found on outcomes related to advance care planning and perceived symptom control and self-management, but not on health outcomes.
Research on palliative care in COPD should focus on what is important to patients with end-stage COPD and their informal caregivers. More knowledge is needed on which outcomes best reflect their needs.
Controlled studies with sufficient power are needed to evaluate the effectiveness of palliative care on patients with COPD and their informal caregivers.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death worldwide. 1 Patients suffering from end-stage COPD experience severe breathlessness and other debilitating symptoms such as fatigue, pain, anxiety and depression, leading to poor quality of life and emphasizing the need for adequate palliative care. 2 Palliative care aims to improve the quality of life of patients with a life-threatening disease and their families by early identification, assessment and treatment of physical, psychological, social and spiritual problems. 3 Growing evidence suggests that palliative care, in general, has positive effects on quality of life and can decrease symptom burden in patients with life-limiting illnesses. Additionally, it can improve patient and informal caregiver satisfaction with care and reduces healthcare utilization. 4 However, for patients with advanced COPD, palliative care is not yet part of standard care, and discussions about goals of (end-of-life) care rarely take place, or only late in the disease course. 5 As a consequence, their severe symptoms remain undertreated, and a large proportion of this patient group inadvertently dies in the hospital.6,7 Moreover, the long disease course with declining functional capacity affects their informal caregivers. 8
Implementing palliative care for patients with COPD is challenging. Due to the unpredictable disease trajectory, healthcare professionals struggle to determine when to refer patients for specialized palliative care. 9 Further, palliative care for patients with COPD needs to be differently organized than for oncological patients because it demands integration of palliative care and disease-oriented care until the end-of-life. 10 The implementation of palliative care in COPD-care is further complicated as professionals must perform actions they are not used to, such as discussing holistic needs and end-of-life topics. 9
Although guidelines recommend palliative care for patients with COPD, there is little evidence for the effectiveness of palliative care interventions for this patient group specifically.11,12 In previous systematic reviews, the vast majority of the interventions described were designed for patients with cancer4,13,14 or focused on a single intervention component only.15–17 Research on the effectiveness of interventions that integrate multiple components of palliative care for patients with COPD is still lacking. 18 Further, it remains unclear how palliative care can be organized for this patient group and what are requirements for successful implementation. Finally, no reviews have included intervention outcomes at the level of the informal caregiver and professional.
To guide future palliative care provision for patients with COPD and to identify gaps in the current evidence-base, we, therefore, aimed to review multi-component palliative care interventions targeting patients with advanced COPD and their informal caregivers. Specifically, we aimed to:
Synthesize the characteristics of multi-component palliative care interventions targeting patients with COPD and their informal caregivers;
Review the evidence for the effectiveness of those interventions on patient, informal caregiver and healthcare professional outcomes;
Review the evidence on implementation outcomes and barriers and facilitators of implementation.
Methods
The protocol of this systematic review has been registered in the international Prospective Register of Systematic Reviews (PROSPERO) database (ID: CRD42017079962). We used the Cochrane Handbook for Systematic Reviews of Interventions to perform the review, and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for reporting.
Literature search
The electronic databases MEDLINE, Embase, Web of Science, COCHRANE Library, PsycINFO, CENTRAL and Emcare were searched for eligible studies. In the search strategy, we combined a broad range of synonyms of the search terms “COPD” and “palliative care” (Supplemental Table 1). Articles that were published between 1 January 1990 and 9 June 2020 were screened for inclusion, without language restrictions. We searched for other potentially relevant studies by screening the reference lists and citations of included studies.
Study selection
Articles reporting on primary research data of multi-component palliative care interventions targeting patients with COPD were included. The intervention described in the article needed to be referred to as a palliative care or end-of-life care intervention, program or approach. We defined a multi-component intervention as an intervention comprising multiple components which interact to produce change, following the complex intervention definition of the Medical Research Council. 19 Interventions focusing only on a single component (such as advance care planning or opioids for breathlessness) were excluded. If the study population was mixed, articles were included if at least 30% of the study population suffered from COPD. Case reports and non-primary research data, such as reviews, editorials, conference abstracts and books were excluded. We also included uncontrolled before-and-after studies, qualitative and mixed-method studies, as this (1) reflects the most frequent type of studies performed and provides a comprehensive overview of all available evidence, and (2) because we wanted to gain in-depth insight into mechanisms or elements contributing most to intervention effectiveness and successful implementation. Title and abstract screening and subsequent full-text screening was done by two reviewers independently (J.B., and J.S. or A.H.). In case of any incongruences, the in- or exclusion of an article was discussed until consensus was reached. In case of doubt, a third researcher (R.K.) was consulted.
Data extraction
Data on design, participants, intervention characteristics and all reported outcomes at patient, informal caregiver and healthcare professional level were extracted using a piloted extraction form. If necessary and possible, additional data was derived from published study protocols or supplementary documents, or requested from the authors. Data extraction of the included articles was done by two reviewers independently (J.B. as first reviewer for all articles and A.H., D.J., Y.E., or R.K. as a second reviewer). Any incongruencies were discussed until consensus was reached. Implementation outcomes and barriers and facilitators for implementation were extracted by one reviewer (J.B.) and discussed with a second reviewer who has great expertise in implementation (R.K.).
Quality appraisal
Quality appraisal was performed by two reviewers (J.B. and A.H.) independently, using the Mixed Methods Appraisal Tool. 20 After two screening questions, each study is appraised by rating appraisal criteria for the corresponding category. Any discrepancies in the quality appraisal were resolved by discussion, and if needed, a third reviewer (R.K.) was consulted. To compare study quality, we assigned four stars to a study when 75 to 100% of the criteria were positively rated (high quality), three stars for 50–75% (moderate quality), two stars for 25–50% (low quality) and one star for 0–25% (very low quality).
Data analysis
Data were analysed using narrative synthesis. 21 Study characteristics were summarized in terms of country, design, objective, study participants, inclusion strategy, intervention and organizational characteristics and outcomes. The intervention components were categorized according to twelve palliative care domains based on the Dutch Quality Framework Palliative care, 12 Clinical Practice Guidelines for Quality Palliative Care 22 and Quality standard End of life care for adults. 23 The operationalization of domains is described in Supplemental Table 2. Outcomes were classified into three categories: outcomes at patient, informal caregiver, and healthcare professional level. Quantitative results reported in studies in which no statistical testing was performed, were disregarded. The text in articles reporting on qualitative outcomes was coded phrase by phrase after which common themes were identified. 24 We categorized implementation outcomes following the proposed terminology and operationalization of Proctor et al. 25 (see Supplemental Table 3). According to Proctor et al., 25 implementation outcomes are defined as “the effects of deliberate and purposive actions to implement new treatments, practices, and services” (page 65). Process outcomes reflecting trial feasibility (and not intervention feasibility) were not evaluated. Barriers and facilitators to implementation of palliative care interventions were categorized using the framework of Fleuren et al. 26 This instrument consists of 29 determinants in four categories: determinants associated with the (a) innovation, (b) adopting person, (c) organization, and (d) socio-political context. We extracted determinants for three types of users: referrers (professionals who refer patients to the palliative care intervention), providers (professionals who provide the intervention) and patients (individuals who receive the intervention). If needed, determinants of the Consolidated Framework for Implementation Research 27 or newly defined determinants were added inductively. The codebook used is available in Supplemental Table 4.
Results
The database search yielded 5621 unique records. In total, 166 articles were excluded based on publication date. Next, we excluded 5310 articles based on title-abstract screening. The full-text versions of the remaining 145 articles were assessed for eligibility. Twenty-three of them met inclusion criteria. Screening of references and citations of included articles identified eight additional articles. A flow diagram of the study selection is displayed in Figure 1. Finally, 31 articles were included that reported on 20 unique palliative care interventions; six interventions were evaluated in more than one article.
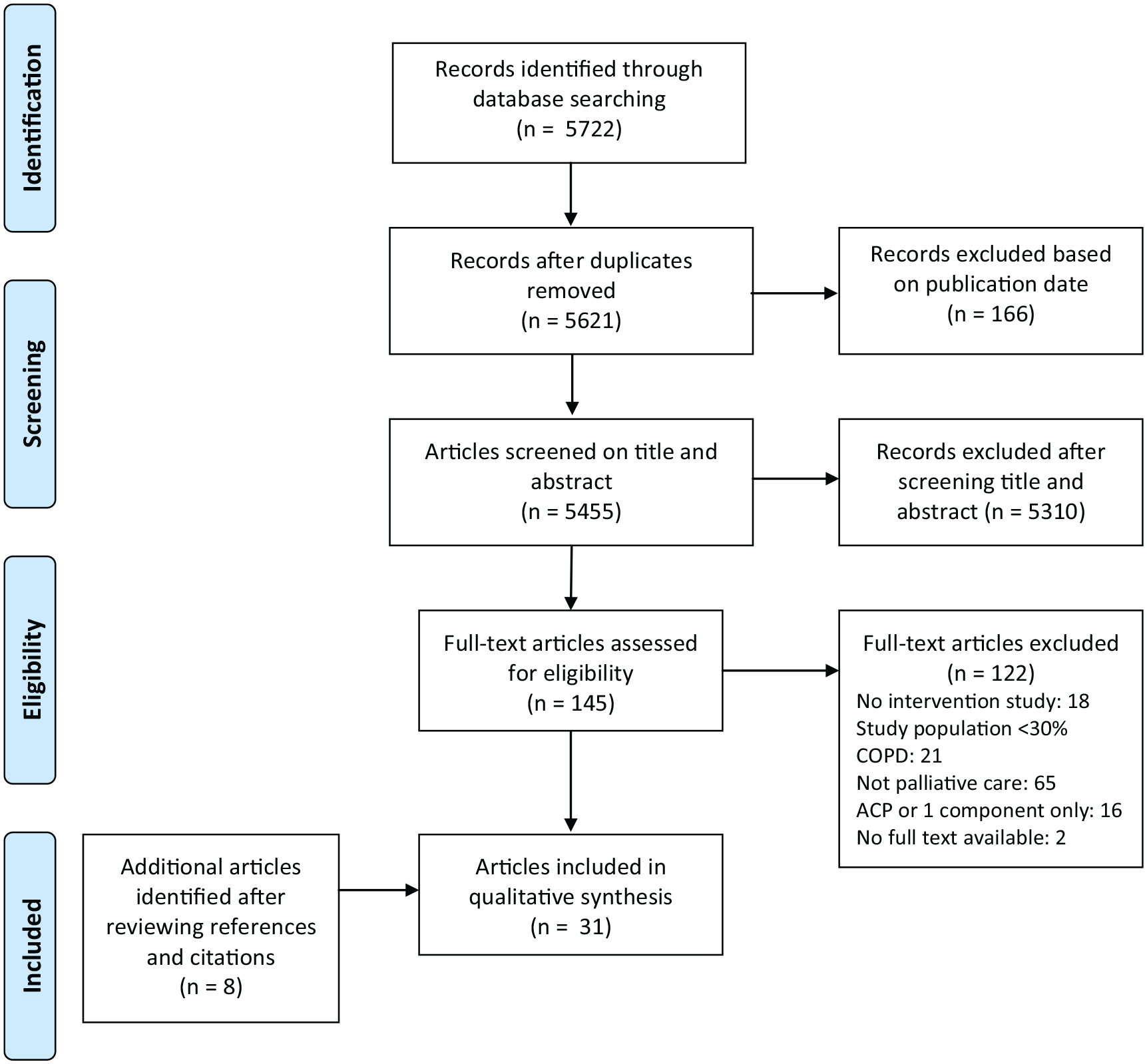
PRISMA flow diagram of the study selection process.
Study characteristics
Characteristics of included studies and interventions are summarized in Table 1. All studies took place in western countries, of which most in the USA (n = 5) and the United Kingdom (n = 4). Three RCTs,28–30 two non-randomized controlled trials,31–33 seven uncontrolled before-and-after studies,34–41 six qualitative studies,42–47 one non-comparative study, 48 and 10 pilot/feasibility studies37,49–57 were included. The study design of one article was unclear. 58 Two articles reported on the same study and were collated.32,33 Five quantitative studies30,33,35,41,48 and six pilot/feasibility studies37,50–52,54,55 also included qualitative data. Eighteen studies (60%) focused specifically on COPD. Other studies focussed on refractory breathlessness29,30,38,42,43,54 or also included patients with heart failure28,34,44,58 or heart failure and cancer.33,45 Sample sizes in quantitative studies ranged from 13 to 228 patients and in qualitative (sub)studies from 6 to 78 patients. The mean age of study populations ranged between 63 and 76 years.
Description of included studies and palliative care interventions.
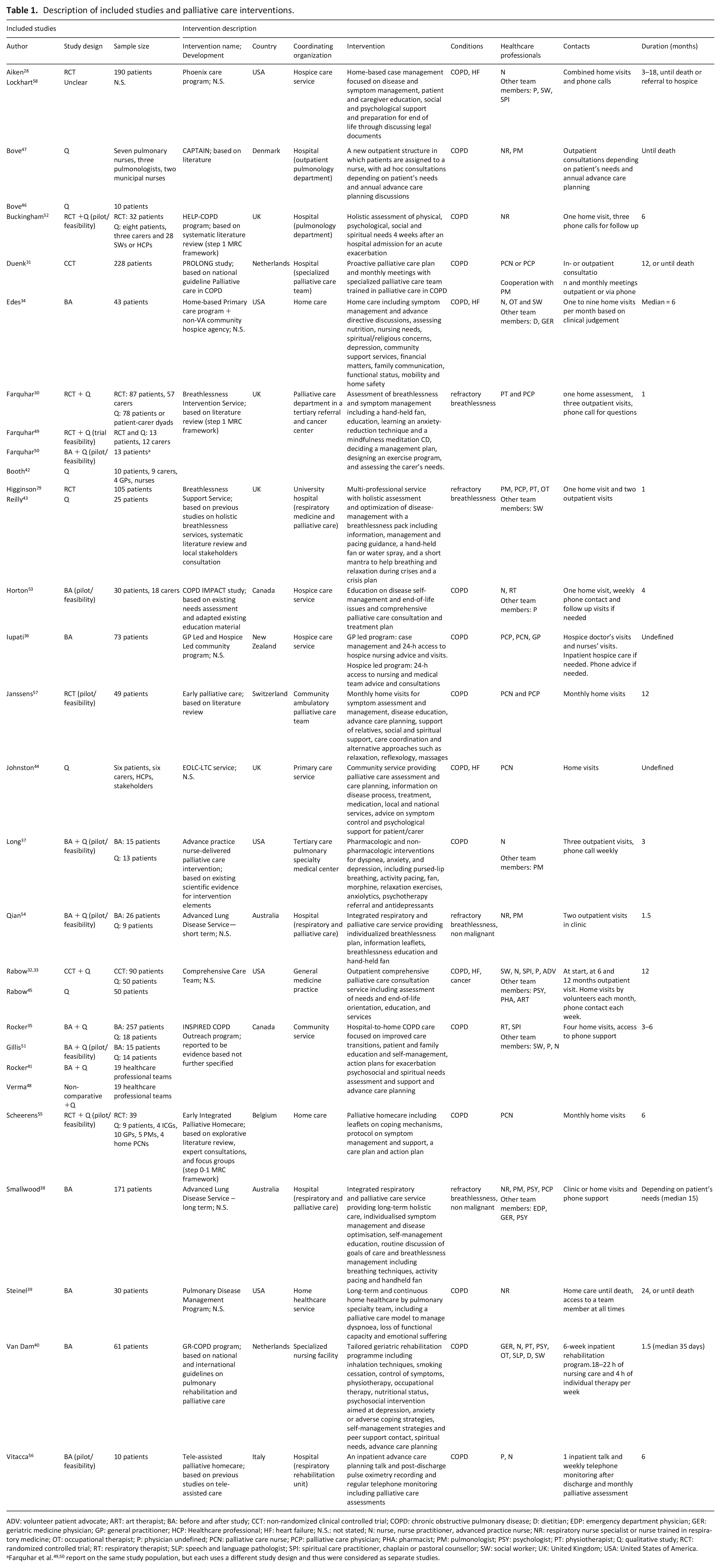
ADV: volunteer patient advocate; ART: art therapist; BA: before and after study; CCT: non-randomized clinical controlled trial; COPD: chronic obstructive pulmonary disease; D: dietitian; EDP: emergency department physician; GER: geriatric medicine physician; GP: general practitioner; HCP: Healthcare professional; HF: heart failure; N.S.: not stated; N: nurse, nurse practitioner, advanced practice nurse; NR: respiratory nurse specialist or nurse trained in respiratory medicine; OT: occupational therapist; P: physician undefined; PCN: palliative care nurse; PCP: palliative care physician; PHA: pharmacist; PM: pulmonologist; PSY: psychologist; PT: physiotherapist; Q: qualitative study; RCT: randomized controlled trial; RT: respiratory therapist; SLP: speech and language pathologist; SPI: spiritual care practitioner, chaplain or pastoral counsellor; SW: social worker; UK: United Kingdom; USA: United States of America.
Intervention characteristics
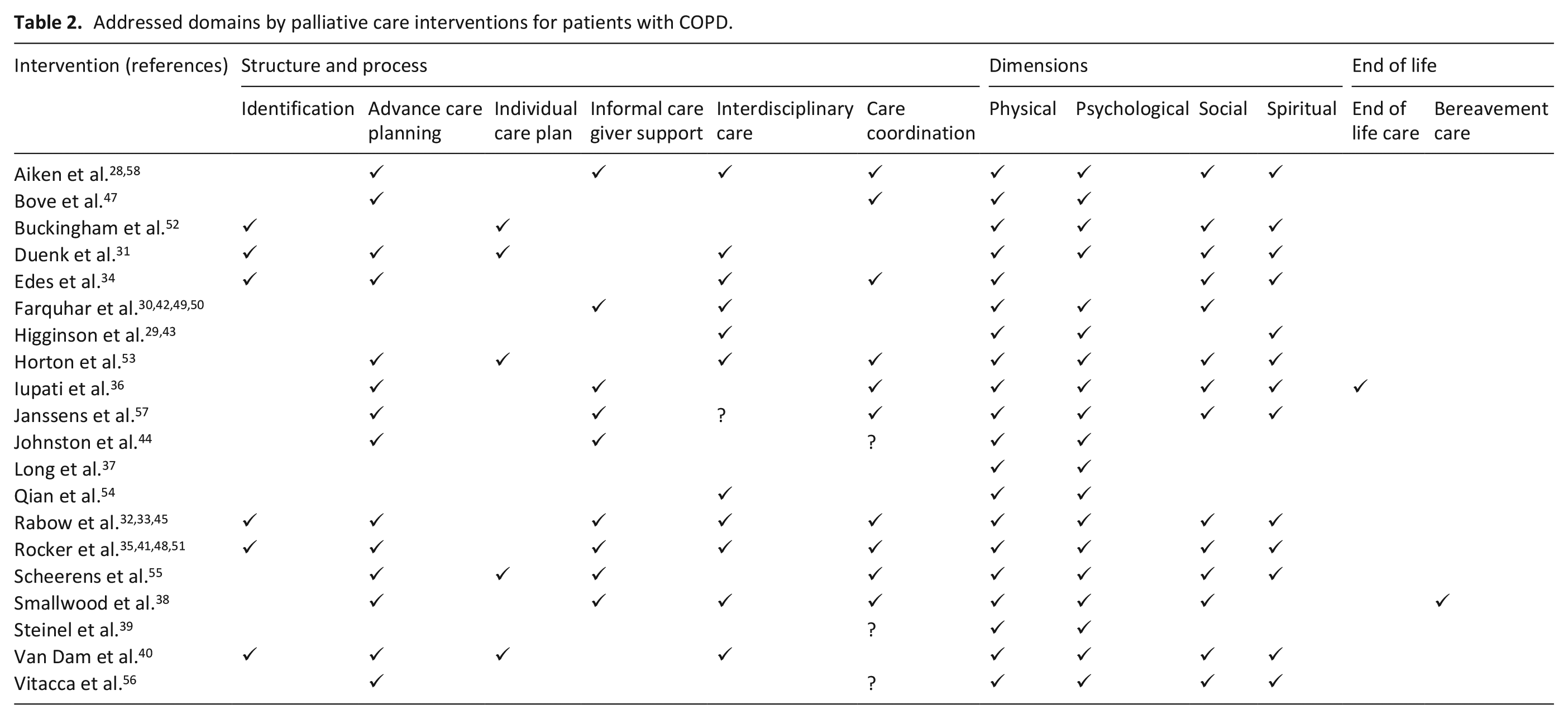
Half of the interventions were developed based on literature according to the description in the article; two were based on specific guidelines. Thirteen of the twenty interventions comprised of longitudinal care in which there was regular contact of a nurse with patients via home visits,28,34–36,39,44,55,57 outpatient visits31,33,47 or a combination of both. 38 Vitacca et al. 56 included telemonitoring. The majority of longitudinal care interventions included symptom management and needs assessments, disease education and self-management, advance care planning and care coordination (Table 2). Informal caregiver support was incorporated in eight interventions and consisted of caregiver education,28,30,33,35,38 nurse assessment of needs,28,33,44,55,57 invitation to support groups 33 and respite care 38 and was unspecified in Iupati and Ensor. 36 Most were organized by a community care organization, such as a hospice care service or home service. Six other interventions comprised of one comprehensive needs assessment with a short follow up.29,30,37,52–54 They included one to four home visits and/or outpatient visits and were mostly organized by pulmonary care and palliative care departments. Four interventions specifically focussed on the management of breathlessness29,30,37,54 and comprised of various pharmacological and non-pharmacological interventions to address breathlessness and how to cope with this symptom. Farquhar et al. also included informal caregiver education. Lastly, one intervention was a 6-week multidisciplinary geriatric rehabilitation program in a specialist nursing facility. Patients in need of palliative care were proactively identified by six interventions, by screening patients during hospitalization for acute exacerbation31,40,52 or by using a computerized screening program based on diagnosis and hospitalizations or measures of disease severity.33,34 In most other cases, patients were referred to the service by healthcare professionals.
Addressed domains by palliative care interventions for patients with COPD.
Quality appraisal
Ratings of the criteria of the Mixed Methods Appraisal Tool per study are provided in Supplementary Table 5. Quality of the studies was related to the study design used. All three RCTs were of high quality; non-randomized controlled trials and qualitative studies were of moderate to high quality; study quality of uncontrolled studies ranged from very low to moderate. The quality of pilot/feasibility studies varied from low to high. Two articles were not appraised as they did not pass the screening questions.35,58 The following reasons most frequently contributed to a negative rating: lack of information on intervention adherence in controlled trials, insufficient use of quotations that supported interpretations of results in qualitative studies, and absence of adjusting for confounding in uncontrolled studies. In studies with both a quantitative and qualitative component, there often was poor integration of the two components.
Quantitative outcomes
Quantitative results are summarized in Table 3. The most frequently evaluated outcomes were acute healthcare use, health-related quality of life and psychological outcomes. Four out of seven controlled studies reported a primary outcome: mastery of breathlessness, 29 distress due to breathlessness, 30 health-related quality of life 31 and pain. 32 Janssens et al. 57 had initially planned to measure acute healthcare use as primary outcome. However, they did not reach sufficient power to do so due to severe recruitment issues. One study found a statistically significant positive effect on its primary outcome; Higginson et al. reported a difference in mastery of breathlessness between intervention and control group of 0.58 (0.01 to 1.15).
Summary of quantitative outcomes and results at the level of the patient, informal caregiver and healthcare professional, and costs.
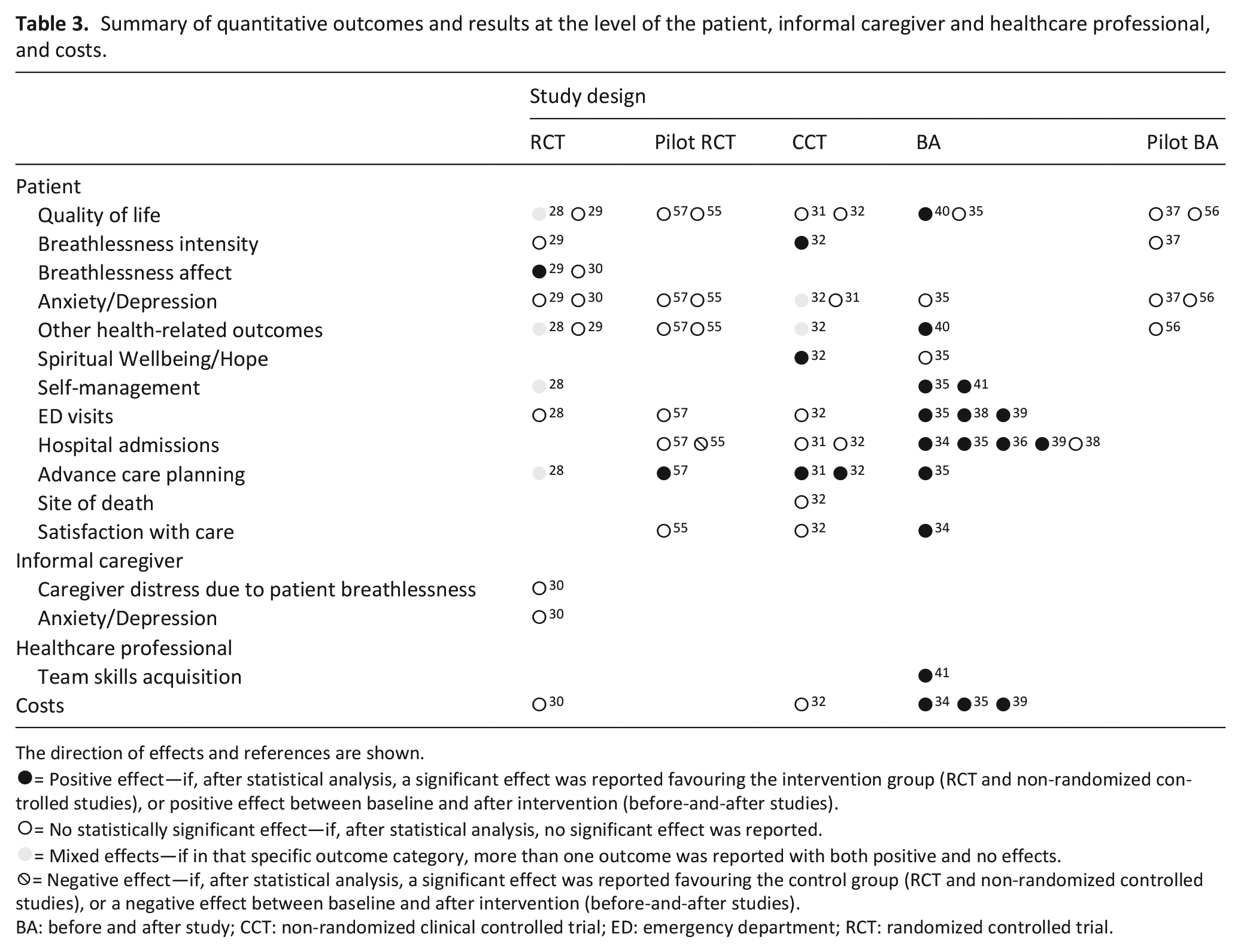
The direction of effects and references are shown.
= Positive effect—if, after statistical analysis, a significant effect was reported favouring the intervention group (RCT and non-randomized controlled studies), or positive effect between baseline and after intervention (before-and-after studies).
= No statistically significant effect—if, after statistical analysis, no significant effect was reported.
= Mixed effects—if in that specific outcome category, more than one outcome was reported with both positive and no effects.
= Negative effect—if, after statistical analysis, a significant effect was reported favouring the control group (RCT and non-randomized controlled studies), or a negative effect between baseline and after intervention (before-and-after studies).
BA: before and after study; CCT: non-randomized clinical controlled trial; ED: emergency department; RCT: randomized controlled trial.
Outcomes at patient level
Quality of life—Health-related quality of life was assessed in ten studies,28,29,31,32,35,37,40,55–57 using seven different measurement instruments. Duenk et al. 31 set health-related quality of life as their primary outcome. Their study and that of Aiken et al. 28 found significant differences between the intervention and control group on specific subscales but not on the total scale. The uncontrolled study of Van Dam et al. 40 reported an improvement on health-related quality of life; all other studies found no differences.28,29,31,32,35,37
Breathlessness—In two RCTs evaluating holistic breathlessness services,29,30 intervention patients showed higher levels of mastery of breathlessness, but only one study found a statistically significant difference. 29 No difference was found on distress due to breathlessness in one RCT. 30 In the study of Rabow et al., 32 intervention patients reported a lower degree of breathlessness interference with daily activities and limitations in daily life compared to control patients. Two other controlled studies did not find an effect on breathlessness intensity.29,37
Anxiety and depression—Rabow et al. 32 reported reduced anxiety in intervention patients, but no change in depression. Eight other studies found no significant differences.29–31,35,37,55–57
Other health-related outcomes – Aiken et al. found lower symptom distress in intervention patients at three months, but not at six months. 28 Further, positive effects were reported for the resumption of activities, 28 sleep quality, 32 functional capacity 40 and nutritional status. 40
Spiritual Well-being / Hope—In the study of Rabow et al., intervention patients reported higher overall spiritual well-being than control patients. 32 One study evaluating hope found no difference after the intervention. 35
Self-management—The study of Aiken et al. 28 revealed an improvement in illness self-management and awareness of resources, at specific time points. Rocker et al.35,41 found a positive result on the quality of preparation for self-care and need for information after program participation. 41
Health care use—Mixed results were found regarding unplanned health care use. Controlled studies showed no effect on the number of emergency department visits or hospitalizations.28,31,32,55,57 Uncontrolled studies revealed reduction in the number of emergency department visits and hospitalizations.34–36,38,39 One pilot RCT reported more hospitalizations in the intervention group than the usual care group. 55 A comparison of deceased intervention patients with other decedents showed a shorter median length of stay at the Intensive Care Unit. 35
Advance care planning—Five studies found that, for intervention patients, a personal directive and advance care planning choices were more often documented,28,31,35,57 and funeral arrangements were more likely to be completed. 32
Site of death—One controlled study examining site of death found no differences between intervention and control group. 32
Satisfaction with care—Two controlled studies found no difference between intervention and control group regarding satisfaction with care32,55; the uncontrolled study of Edes et al. 34 reported an improvement.
Outcomes at informal caregiver level
Only one study examined outcomes at informal caregiver level and found no differences in caregiver distress due to patient breathlessness, nor on anxiety and depression between the intervention and control group. 30
Outcomes at healthcare professionals’ level
Outcomes at professional level were only assessed in one uncontrolled study. A positive effect on several skills regarding quality improvement and implementation was reported. 48
Costs
Two controlled studies found no difference in healthcare costs of intervention patients,30,32 of which one also evaluated cost-effectiveness and found high costs gained per quality-adjusted life-year. 30 Three uncontrolled studies reported lower healthcare costs per patient in the period after the start of the intervention.34,35,39
Qualitative outcomes
Qualitative outcomes were derived from interviews in fourteen qualitative (sub)studies.30,35,37,41–48,52,54,55 In most studies, patients reported improved self-confidence to manage symptoms30,35,37,41,43,44,46 and positive psychological effects.30,35,37,43,45,52 Besides, in some cases, hospitalization was prevented due to earlier diagnosis and treatment.44–46 Regarding informal caregivers, increased confidence was reported because they knew how they could help their relatives with breathlessness.30,42 Regarding healthcare professionals, nurses providing palliative care got more insight in and understanding of the suffering of patients with COPD and complexities around COPD-care.47,48
Implementation outcomes
In the included studies, acceptability and feasibility were the most frequently assessed implementation outcomes. Supplementary Table 3 provides the operationalization of implementation outcomes. Acceptability was mostly assessed by interviewing patients,42,44,45,46,52,54,55 informal caregivers and referring healthcare professionals,42,44,52 but also by using a questionnaire among participants 43 or by collecting patient stories anecdotally. 58 All studies reported that patients, informal caregivers and healthcare professionals valued the palliative care intervention. Components of the interventions that were highly valued included being listened to and direct access to a professional for support,30,35,42,44,46,50,55 continuity of the relationship44,46 and education about breathlessness management.30,35,42,43,50,55 Specifically regarding breathlessness, non-pharmacological interventions such as a hand-held fan and breathing techniques were reported to be most helpful.30,42,43,54,55 Four studies reported on intervention feasibility using predefined feasibility criteria (e.g. participation rates and completion of the program).37,51,52,55 The feasibility level varied and was mostly related to specific intervention context characteristics. For instance, Buckingham et al. 52 encountered fewer actions during assessments than expected due to overlap of their service with existing discharge services. Two studies reported on the completion of program components (fidelity)37,51 and one on usefulness (appropriateness) as one of the feasibility criteria. 37 One study evaluating nationwide dissemination of their approach reported on adoption and sustainability41,48; Fifteen of nineteen teams to which the intervention was disseminated incorporated all core interventions of the program and reported sustained improvements.
Barriers and facilitators for implementation
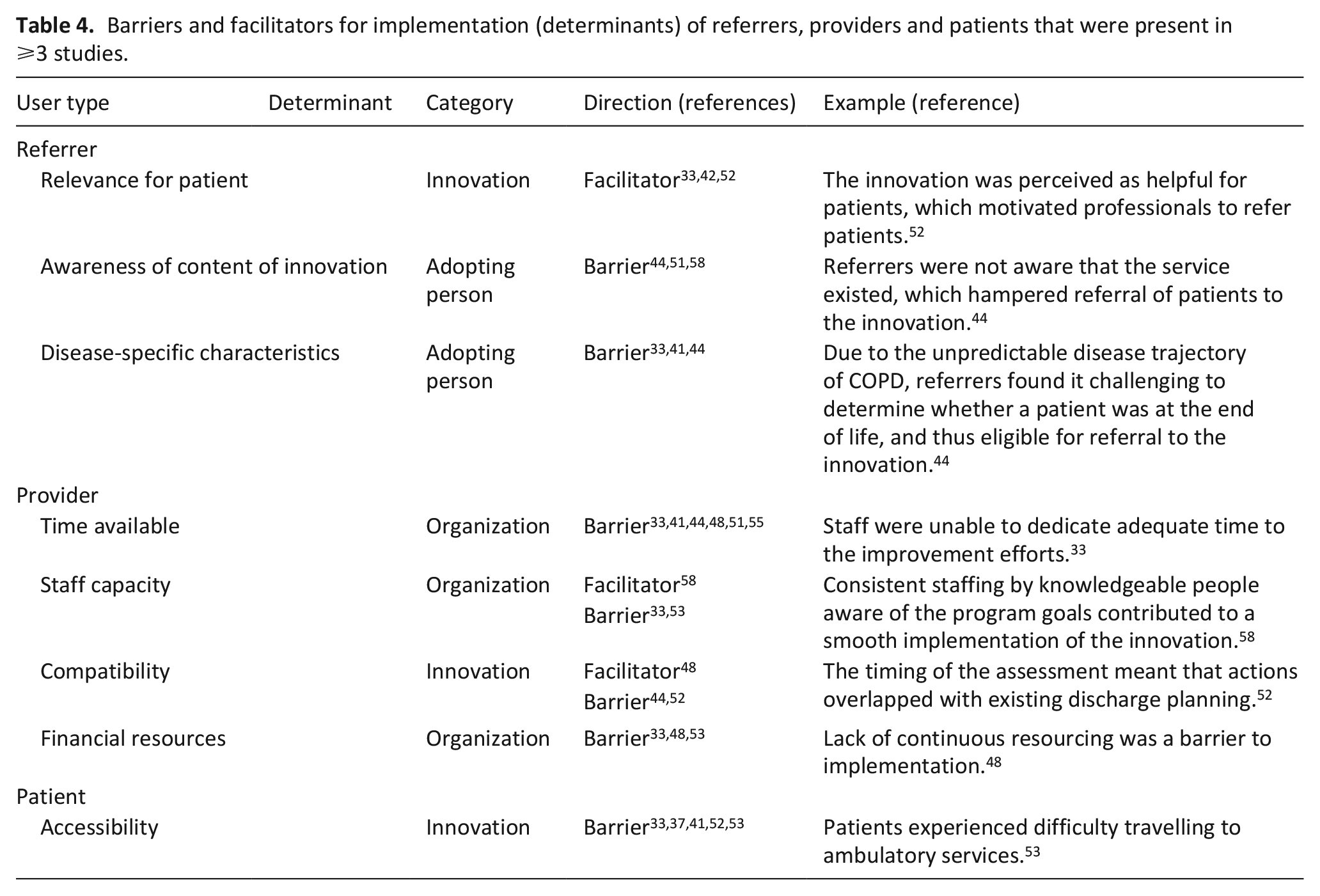
In ten articles barriers and facilitators for implementation (determinants) of nine different palliative care interventions were reported,33,37,41,42,44,48,51–53,55,58 mostly derived from interviews with referring healthcare professionals and intervention participants. Determinants for referrers, providers and patients that were present in three or more studies are shown in Table 4. All determinants are shown in Supplementary Table 6.
Barriers and facilitators for implementation (determinants) of referrers, providers and patients that were present in ⩾3 studies.
Discussion
Main findings
This study reviewed the characteristics of multi-component palliative care interventions for patients with COPD and the available evidence on their effectiveness and implementation, to provide guidance on future palliative care provision and to identify knowledge gaps in the literature. We found that a range of longitudinal and short-term interventions in different care settings has been developed to enhance palliative care provision to patients with COPD. Although the acceptability of the interventions was high among patients, informal caregivers and healthcare professionals, we found only limited evidence on their effectiveness. Quantitative and qualitative data suggest positive effects related to perceived symptom control, self-management and self-confidence. Most frequently named barriers to implementation were uncertainty about the timing of referral due to the unpredictable disease trajectory (referrers), time availability (providers) and accessibility (patients).
Interpretation of findings
The current evidence for multi-component palliative care interventions for patients with COPD is scarce and inconclusive; only four interventions (20%) were evaluated in an adequately powered controlled trial; eight (40%) were evaluated in a pilot or feasibility study only. The assessed outcome measures were heterogenous, and only a few statically significant effects were found.
Six out of seven studies found no positive effect on quality of life. This can be due to several reasons. First, just one study had quality of life set as primary outcome 31 and therefore most studies were not powered for this outcome. Second, it is very likely that interventions affect only certain dimensions of quality of life. As quality of life is often reported as one construct in which physical aspects are prominently present, effects on other dimensions are likely to be missed or underestimated. A positive effect on health status was only seen in an inpatient pulmonary rehabilitation intervention, 40 which may be due to the fact that pulmonary rehabilitation is an intensive intervention and addresses many aspects that are included in health-related quality of life questionnaires. Third, in this patient group with end-stage disease, an improvement in quality of life is possibly hard to achieve because of the progressive nature of the disease. However, in patients with heart failure and cancer, significant effects on quality of life have been found,4,59 suggesting that there are perhaps other reasons specifically related to COPD or the conducted research.
While no consistent effects were found on health outcomes, advance care planning activities were increased in all studies measuring it.28,31,32,35,57 Also, positive effects were reported on quantitative outcomes related to perceived control of breathlessness 29 and self-management.28,35 This corresponds with the consistent finding from qualitative studies that after the intervention, patients experienced increased perceived control to manage their symptoms and improved self-confidence30,35,37,41,43,44 due to increased knowledge about their symptoms and the reassurance that support was available if necessary. In line with our findings, a recent meta-analysis on holistic breathlessness interventions found positive effects in the affective domain of breathlessness, but not in level of breathlessness nor quality of life. 14
Qualitative evidence suggests that longitudinal palliative care interventions prevent emergency department and hospital admissions in some cases due to earlier diagnosis and treatment.44–46 Quantitative outcomes, however, reveal mixed results. Controlled studies showed no differences between intervention and control group, whereas uncontrolled studies showed a reduction in emergency department and hospital admissions. This difference was also present in healthcare costs, as hospitalizations are responsible for the biggest part of healthcare expenditures 60 : controlled studies reported no statistically significant differences between intervention and usual care patients, and uncontrolled trials showed lower healthcare expenses during the intervention than before. Either way, in line with previous reviews, our results suggest that adding palliative care to usual care does not increase healthcare costs.4,59
Palliative care interventions targeting patients with COPD
Two main intervention types could be identified: short-term palliative care assessments and longitudinal palliative care interventions with care coordination. Both types were regarded as acceptable and helpful to patients with COPD, and were appreciated by referring healthcare professionals since they meet the unaddressed needs of this patient group. Although the high heterogeneity of interventions and outcome measures prevents quantifying which components are most beneficial, qualitative data revealed some characteristics that were consistently valued and perceived as helpful by patients. This implies that patient and family education on breathlessness management, direct access to a professional for support and an ongoing relationship are essential components to include in future interventions. As these components are rather COPD-specific than palliative care characteristics, it seems that, with sufficient training to healthcare professionals and different care organization, these components could be integrated into regular COPD-care. This would meet the current recommendations of guidelines that integrated palliative care should be provided by generalist or respiratory care professionals, and palliative care specialists become involved only when care needs become complex.11,12
Implementing palliative care interventions
We identified several factors related to the implementation of palliative care interventions for patients with COPD. First, identifying eligible patients appeared challenging, as is also reflected by the variability in the inclusion criteria and strategies used across studies. The emergency department appeared not to be a feasible recruitment setting for a home-based program, 51 but barriers were also encountered in the ambulatory setting 53 and during computerized screening. 33 Using a natural transition point to identify patients with palliative care needs proactively, such as hospitalization for an acute exacerbation,31,35,40,52 has been recommended in previous research 61 and could possibly facilitate identification of patients. Further, palliative care can best be integrated within existing services to prevent duplication of assessments 52 and to guarantee continuity of care. To facilitate healthcare professionals to provide palliative care, a model that can be adapted to regional needs and providing access to tools showed to be practical. 41 For this vulnerable patient group with high disease burden and low socio-economic status, care needs to be easily accessible, as well in terms of physical distance as financially. This might be resolved by performing assessments during home visits and monitoring patient’s needs by phone. Lastly, general organizational conditions such as sufficient time, financial resources and personnel are required for successful implementation.
Study quality and characteristics
The heterogeneity in methodology and used measurement instruments made quantitative pooling of results impossible. Among included studies, study quality was dependent on study design used: most controlled studies were better conducted than studies with a before-and-after design. As most studies did not report a primary outcome and power calculation, the studies may have been underpowered, causing the effects to be underestimated. On the contrary, four studies evaluated many outcomes without controlling for multiple testing,28,32,35,41 leading to an increased risk of unjustified positive results. Moreover, a clear difference was found in the direction of effects between controlled and uncontrolled studies, specifically with regard to acute healthcare use and costs. In uncontrolled studies, a positive effect can falsely be attributed to the intervention, leading to an overestimation of effect, whilst in fact, it is the reflection of the normal disease course or other influences.
Furthermore, the included studies provided little information on the actual delivery of the intervention. As a consequence, it remains unclear whether or not the inconsistency of effects found is due to implementation errors.
Recommendations for future research
For future evaluations, outcomes should be chosen related to the goal of the intervention. Quality of life, although the ultimate goal of palliative care, might be a rather distal outcome measure and difficult to modify in this patient group. Qualitative research can identify which outcomes are most important to patients with end-stage COPD and can increase our understanding of the underlying working mechanisms and what works for whom and under what circumstances. Eventually, consensus on the outcome sets to be used is needed in order to compare different interventions and to be able to conduct meta-analyses. Our review revealed a striking difference between the results of quantitative and qualitative studies included. This may be due to the different focus of these two methods. Qualitative research mainly aims to examine the experiences of individuals, and not health effects. In general, additional care or attention from a professional will result in a more positive patient evaluation. That being said, the added value of palliative care interventions in COPD may just be to improve those subjective experiences of individuals in their final stage of the disease. Therefore, we argue that the discrepancy found between the quantitative and qualitative results advocates for a reconsideration of research outcome choices. Hence, we should consider what can most significantly impact the patients’ well-being and experience, and not solely focus on health effect parameters. Additionally, we were surprised to find so few outcomes at informal caregiver and professional level. We recommend to include outcomes such as informal caregiver burden and professional’s self-efficacy, to acquire knowledge on how informal caregivers can be supported and how professionals can be equipped with the necessary skills. Next, we recommend that future research includes comprehensive process evaluations to unravel requirements for successful implementation and to explore implementation strategies that enhance adoption of new care practices. Various validated tools can be used for this purpose, such as the TIDieR checklist for reporting of intervention characteristics and monitoring intervention fidelity. 62 Also, the Measurement Instrument for Determinants of Innovations framework and Context and Implementation of Complex Interventions framework have been previously used in the palliative care research field and can be used in future studies to measure implementation determinants and contextual factors.63,64
Strengths and limitations
To our knowledge, this is the first study reviewing all evidence on the effectiveness and implementation of palliative care interventions in COPD. Since we did not exclude studies based on design or quality, we were able to use all available information in literature in order to give a broad overview. We used a comprehensive and broad search strategy across multiple databases. Study selection, quality assessment and data extraction were conducted by two authors independently. Implementation outcomes and barriers and facilitators to implementation were categorized using well-established operationalizations.
This systematic review also has some limitations. Although we used a broad search strategy across databases, we included articles only if the authors referred to the intervention as “palliative.” This allowed us to use a clear and objective criterion, as there are no fixed criteria which characteristics an intervention must have in order to be labelled as palliative care, nor which patients with COPD should be labelled as “palliative patients.” As a consequence, we disregarded interventions targeting patients with severe COPD, but were not referred to as palliative. This may have resulted in the exclusion of relevant interventions with similar intervention characteristics. Due to poor reporting and inconsistent terminology used across studies, categorization of characteristics, implementation outcomes and barriers and facilitators was sometimes difficult. Since all study designs were included, there was high methodological variation between studies and variation in risk of bias. Also, there was heterogeneity in used measurement instruments. For these reasons, the results of the synthesized evidence have to be interpreted with caution.
Conclusion
Although the relevance of palliative care interventions for patients with COPD and their informal caregivers has been widely acknowledged, this study found that little high-quality evidence is available on the effectiveness and implementation of palliative care interventions in COPD-care. There is a need for well-conducted controlled effectiveness studies of sufficient power to reach definite conclusions, and that also explore which characteristics of palliative care complex interventions in COPD are especially effective and for whom. Finally, with clearer results, its implementation should be facilitated and documented with adequate process evaluations using standardized methodologies.
Supplemental Material
sj-pdf-1-pmj-10.1177_0269216320981294 – Supplemental material for Effectiveness and implementation of palliative care interventions for patients with chronic obstructive pulmonary disease: A systematic review
Supplemental material, sj-pdf-1-pmj-10.1177_0269216320981294 for Effectiveness and implementation of palliative care interventions for patients with chronic obstructive pulmonary disease: A systematic review by Johanna MC Broese, Albert H de Heij, Daisy JA Janssen, Julia A Skora, Huib AM Kerstjens, Niels H Chavannes, Yvonne Engels and Rianne MJJ van der Kleij in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank Jan W. Schoones, information specialist at the Walaeus Library of the Leiden University Medical Centre, for assisting in developing and conducting the search strategy for this systematic review.
Author contributions
J.B. and R.K. designed the protocol; J.B., J.S. and A.H. performed the study selection; J.B., A.H., R.K., D.J. and Y.E. extracted data; J.B. and A.H. appraised study quality; J.B., R.K. and A.H. performed data analysis and interpretation; J.B. wrote the first draft; All authors contributed to critical revision and agreed with the final manuscript.
This work was financed by The Netherlands Organization for Health Research and Development (ZonMw).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Data management and sharing
All relevant data are within the manuscript. Any other data are available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.