
Abstract
Background:
We developed a new single point of access to integrated palliative care, respiratory medicine and physiotherapy: the breathlessness support service for patients with advanced disease and refractory breathlessness. This study aimed to describe patients’ experiences of the service and identify the aspects valued.
Design:
We attempted to survey all patients who had attended and completed the 6-week breathlessness support service intervention by sending them a postal questionnaire to self-complete covering experience, composition, effectiveness of the BSS and about participation in research. Data were analysed using descriptive statistics and thematic analysis of free text comments.
Results:
Of the 70 postal questionnaires sent out, 25 (36%) returned. A total of 21 (84% (95% confidence interval: 69%–98%)) responding patients reported that they definitely found the breathlessness support service helpful and 13 (52% (95% confidence interval: 32%–72%)) rated the breathlessness support service as excellent. A total of 21 (84% (95% confidence interval: 69%–98%)) patients reported that the breathlessness support service helped with their management of their breathlessness along with additional symptoms and activities (e.g. mood and mobility). Four key themes were identified: (1) personalised care, (2) caring nature of the staff, (3) importance of patient education to empower patients and (4) effectiveness of context-specific breathlessness interventions. These were specific aspects that patients valued.
Conclusion:
Patients’ satisfaction with the breathlessness support service was high, and identified as important to this was a combination of personalised care, nature of staff, education and empowerment, and use of specific interventions. These components would be important in any future breathlessness service.
Keywords
Refractory breathlessness is common in advanced disease;
Breathlessness services have been developed to help manage this disabling symptom, but until recently, the evidence to support such services has been limited;
Recently, we have demonstrated that our integrated palliative care, respiratory medicine and physiotherapy breathlessness support service (BSS) improves patients mastery over their breathlessness.
Patient satisfaction with the BSS was high, with many of the patients rating the care they received as excellent.
Patient free text comments identified four key themes which they valued: (1) personalised care, (2) caring nature of the staff, (3) importance of patient education to empower patients, (4) effectiveness of context-specific breathlessness interventions.
In addition to providing breathlessness support, the BSS provided information on other symptoms, e.g. immobility, pain and available services, e.g. pulmonary rehabilitation and community support.
These findings help to understand how the BSS may be working and would be key components in any attempt to reproduce the BSS
Introduction
Refractory breathlessness, that is, breathlessness that continues despite optimal treatment of the underlying condition, is a common incapacitating problem in the later stages of many diseases. 1 Studies have shown that 94% of the patients with chronic lung disease, 2 78% of those with lung cancer 2 and more than 50% of the patients with heart disease 3 suffer from breathlessness in the last year of life.
Multidisciplinary rehabilitation programmes, incorporating exercise training and education, have been shown to reduce breathlessness and improve exercise capacity in chronic obstructive pulmonary disease (COPD), heart failure and cancer.4–6 However, patients with advanced disease are often too ill to attend pulmonary rehabilitation programmes. Building upon evidence and NICE guidance, breathlessness services have been successfully developed, and evidence suggests that such services are successful in the palliation of this disabling symptom.4,6–8
Unfortunately, accessibility to breathlessness services is not uniform across the National Health Service (NHS). In response to this unmet need of our local patient population, we developed a new single point of access to integrated palliative care, respiratory medicine and physiotherapy: the breathlessness support service (BSS). Our randomised controlled trial (RCT) comparing the BSS to standard care demonstrated that patients who received the BSS had, at 6 weeks, significantly improved breathlessness mastery, quantified using the Chronic Respiratory Questionnaire (CRQ). 9
Patient experience and satisfaction are important in assessing quality of health care and can be predicative of subsequent improvements in health. 10 This study aimed to describe patients’ experiences of the BSS and to understand what aspects influenced their satisfaction with it.
Methods
Design
The study design was a self-complete postal questionnaire survey of patients who had accessed the BSS. Ethics approval for the study was obtained from the King’s College Hospital Ethics Committee (Ref. 10/H0808/17).
Setting
Data were collected as part of a randomised controlled parallel-group, pragmatic, single-blind fast-track trial, investigating the effectiveness of the BSS for the palliation of breathlessness. 9 Patients were referred to the BSS by health professionals in primary and secondary care. Patients suffered from refractory breathlessness despite optimal medical management, as deemed by the referring health-care professional. All patients were offered access to the BSS. 9 Details of the trial have been published elsewhere. 9
Sample
A total of 105 patients consented to enrol in the RCT, of which 75 accessed the BSS (fast-track = 53, delayed entry = 22) and were included in this nested study.
The breathlessness support service (BSS)
The BSS is distinct from previous services;5, 11 it incorporates respiratory expertise, widens the professionals providing care and comprises an outpatient clinic with two appointments interspersed with a home visit. At the first clinic visit, patients were assessed by respiratory medicine and palliative care clinicians, and an individualised plan of treatment was agreed. Patients received a breathlessness pack with information, management and pacing guidance, a poem (to help breathing and relaxation during crises), a hand-held fan and/or water spray and an individualised crisis plan. A home assessment after 2–3 weeks was done by a respiratory physiotherapist and/or occupational therapist that developed a tailored programme based on the domestic situation of the patient. If needed, they referred to additional services such as pulmonary rehabilitation and social work. After the second and final clinic visit (at around 4 weeks after initial assessment) further individualised actions and a discharge plan were agreed. Summaries of both clinic visits were sent to the individual, with a copy to their GP and referring health professional. Full details are published in the protocol and trial results.12, 13
Questionnaire
A self-complete postal questionnaire covering experience, composition, effectiveness of the BSS and about participating in research was used. The questionnaire built on earlier service evaluations. We sent one reminder, 6 weeks after sending out the initial questionnaire.
Questions were presented in the form of short statements, to which patients were asked to rate their level of agreement (both in the positive and negative directions). In addition, there were free text boxes for patients to comment on any aspect of the service (a copy of the questionnaire is available in the online supplement (S1)).
Procedures
The BSS questionnaire, along with a returnable stamped addressed envelope to the BSS research team, was sent to all patients after their final visit to the BSS.
Data analysis
The data collected from the returned BSS evaluation questionnaires were entered into a database using the Statistical Package for Social Science for Windows, version 19 (SPSS Inc., Chicago, IL). Data were analysed using descriptive statistics. Patients were also given the opportunity to comment on specific aspects of the BSS. These free text comments were extracted and transcribed, and themes were identified by thematic analysis. Subsequently, both the free text comments and themes were reviewed (I.J.H./C.B.), and following discussion, refinement and consensuses, the final themes were agreed.
Results
A total of 70 postal questionnaires were sent out (5 were not sent out due to an administrative error). A total of 25 patients (36%) returned the questionnaire. The baseline characteristics of patients who accessed the BSS, those who did not return (non-respondents) and those who returned the postal questionnaire (respondents) are summarised in Table 1.
Baseline characteristics of patients who accessed the BSS, those who did not return (non-respondents) and those who did returned the postal questionnaire (respondents).
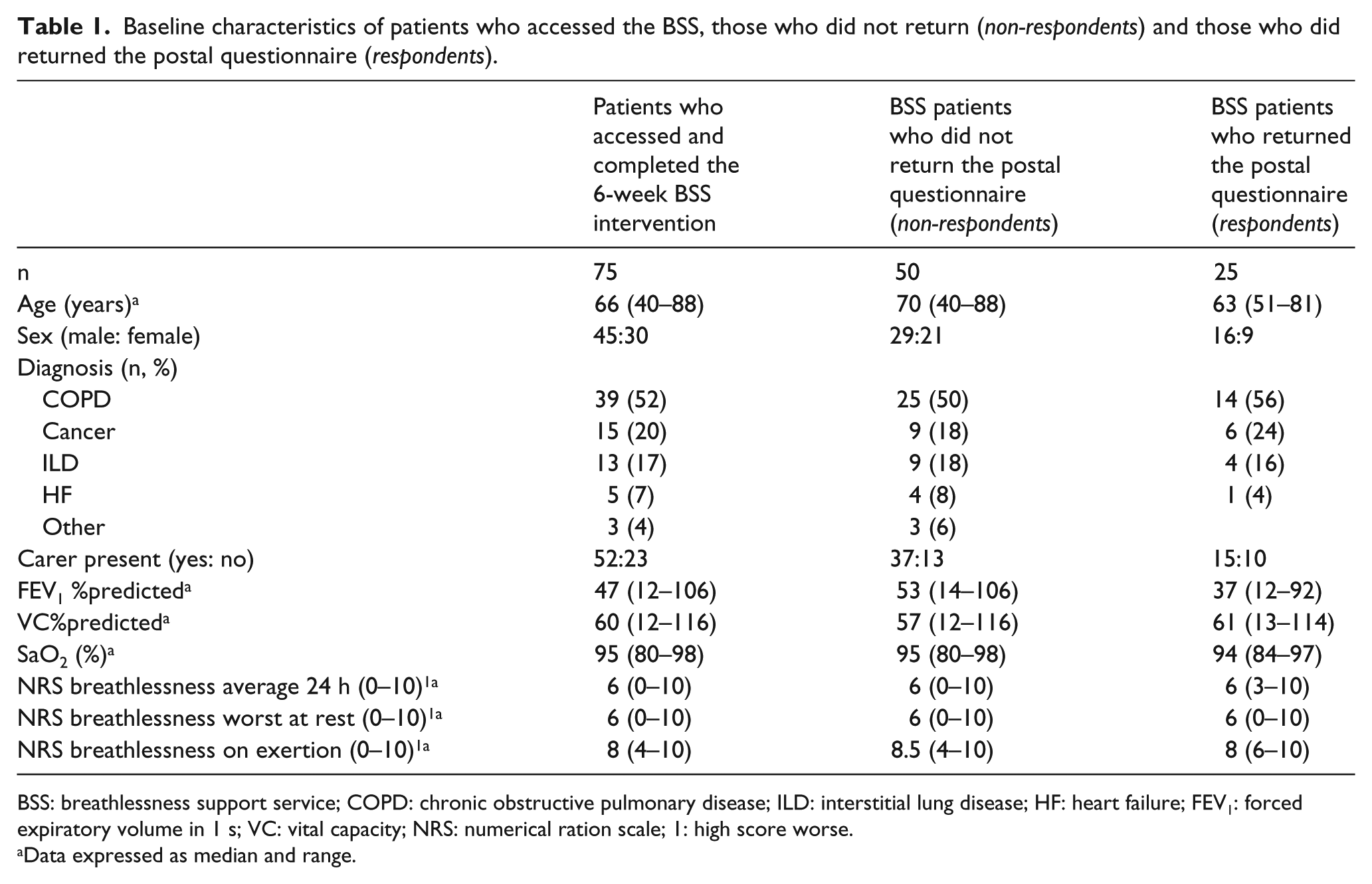
BSS: breathlessness support service; COPD: chronic obstructive pulmonary disease; ILD: interstitial lung disease; HF: heart failure; FEV1: forced expiratory volume in 1 s; VC: vital capacity; NRS: numerical ration scale; 1: high score worse.
Data expressed as median and range.
Patient satisfaction with the BSS
A total of 21 (84% (95% confidence interval (CI): 69%–98%)) responding patients reported that they definitely found the BSS helpful, with 13 (52% (95% CI: 32%–72%)) patients rating the BSS as excellent. In addition, 24 (96% (95% CI: 88%–104%)) patients reported that they found the joint physiotherapy and occupational therapy home visit useful.
The majority of patients reported that they would not change the composition of the BSS, and they valued the holistic, friendly nature of the service. One patient suggested that in addition to the current BSS: ‘Self-help or exercise groups for breathlessness patients and carers may be helpful, and promote self-management’ (65-year-old woman with COPD).
Another patient suggested that the following question should be incorporated into the BSS consultations: ‘Is there anything you cannot discuss with your family that you would like to talk about today?’ (69-year-old woman with COPD).
A total of 17 (68% (95% CI: 50%–86%)) patients reported that they did not have to wait to see a health-care professional at the BSS clinic, 5 (20% (95% CI: 4%–36%)) had to wait but reported that the wait was shorter than their regular clinic wait time and 3 (12% (95% CI: −1% to 25%)) reported that their waiting time was long but similar to their previous experience in other services. All patients reported that they would recommend the service to someone else (Table 2).
Patient satisfaction and experience of the BSS.
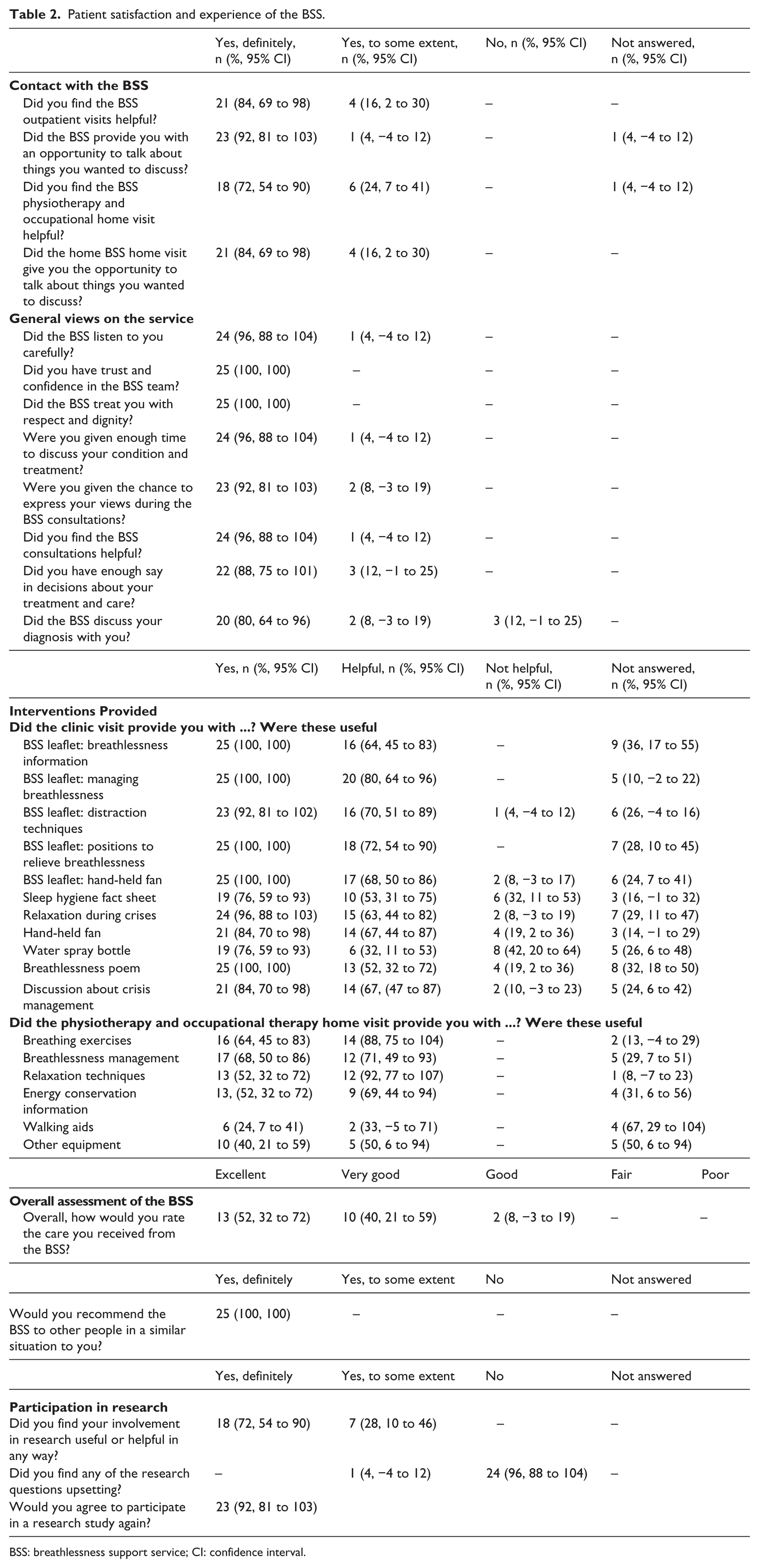
BSS: breathlessness support service; CI: confidence interval.
Benefits of the service
A total of 21 (84% (95% CI: 69%–98%)) patients reported that the BSS helped with their management of their breathlessness along with additional symptoms and activities (e.g. mood and mobility) summarised in Figure 1. A total of 21 (84% (95% CI: 69%–98%)) patients reported that the BSS provided them with additional information and support with regard to additional services (e.g. access to social services and referral to pulmonary rehabilitation), which is summarised in Figure 2.
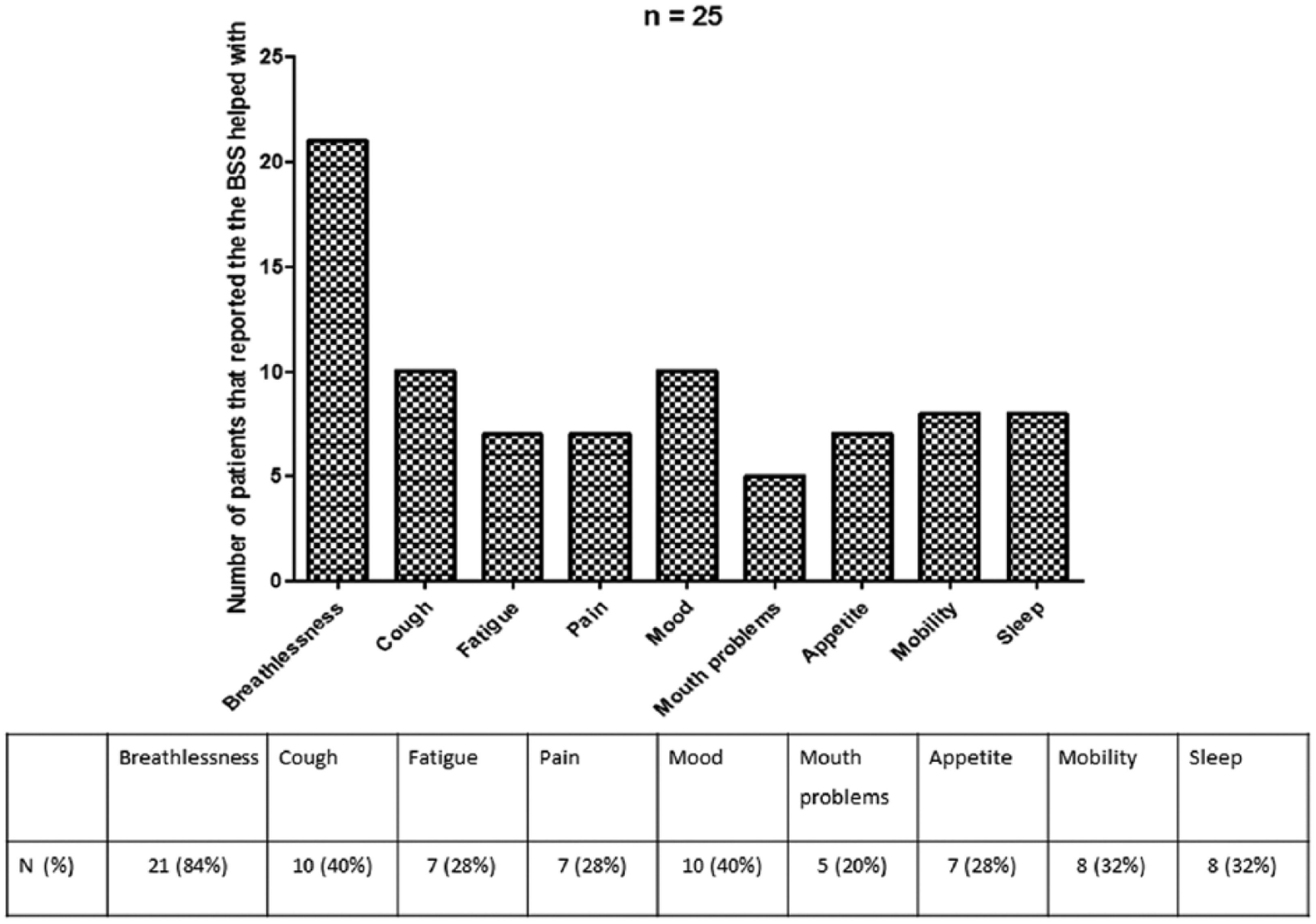
Did the breathlessness support service (BSS) help you with any of the following symptoms?
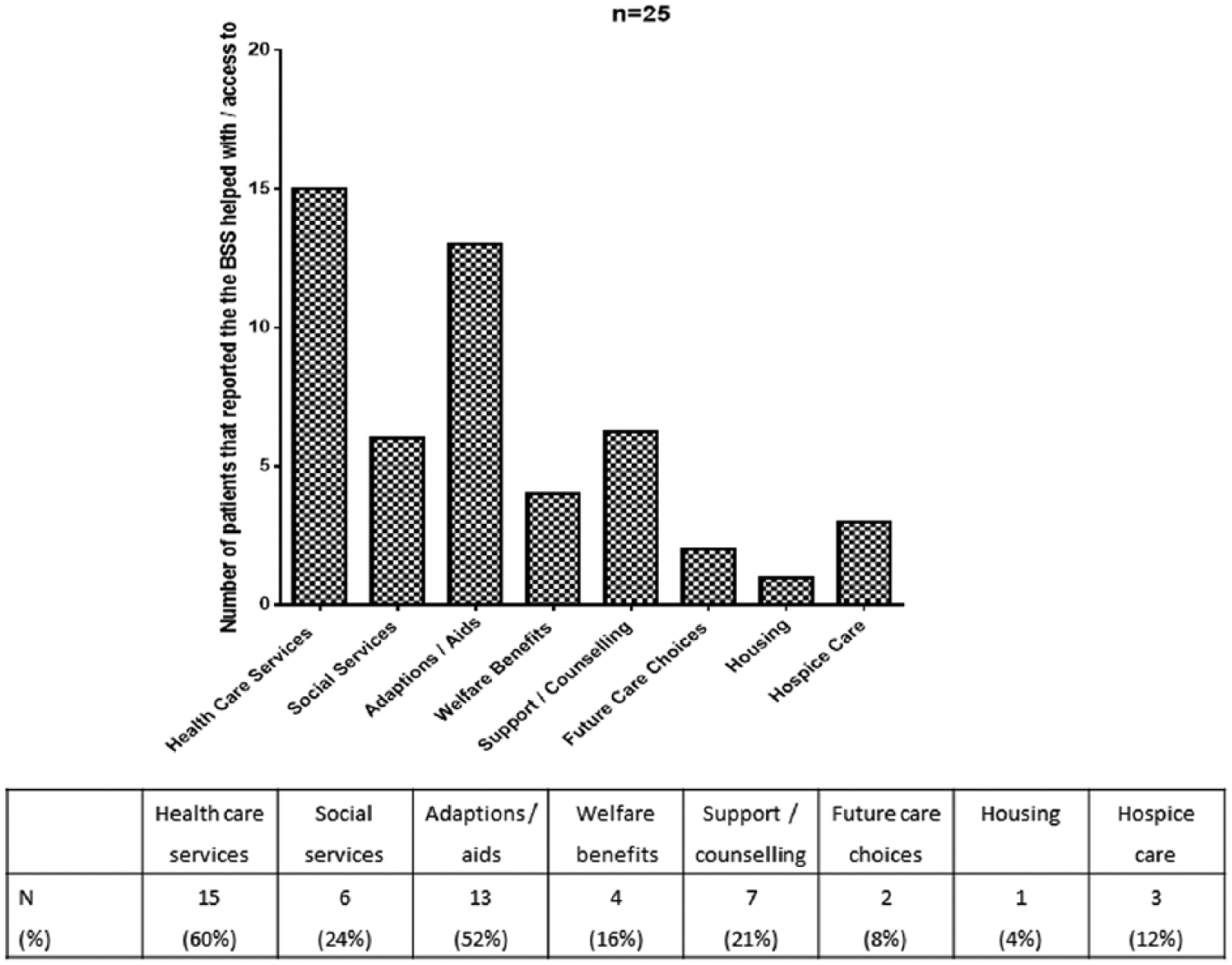
Additional help, support and information provision that patient reported they received as part of the BSS.
Interventions provided
The majority of patients reported that information provided; positions to relieve breathlessness and managing breathlessness, the hand-held fan and discussions about crisis management were the most helpful interventions offered at the clinic visit. With regard to the joint physiotherapy and occupational therapy home visit, patients reported that breathing exercises and relaxation techniques were the most helpful (Table 2).
Free text comments
From the free text component of the questionnaire, four key themes were identified as follows:
Personalised care
Caring nature of the staff
Importance of patient education to empower patients
The effectiveness of context-specific breathlessness interventions
Illustrative quotes are provided in Table 3.
Illustrative quotes about mechanisms by which the BSS improved individual patient’s mastery over their breathlessness.
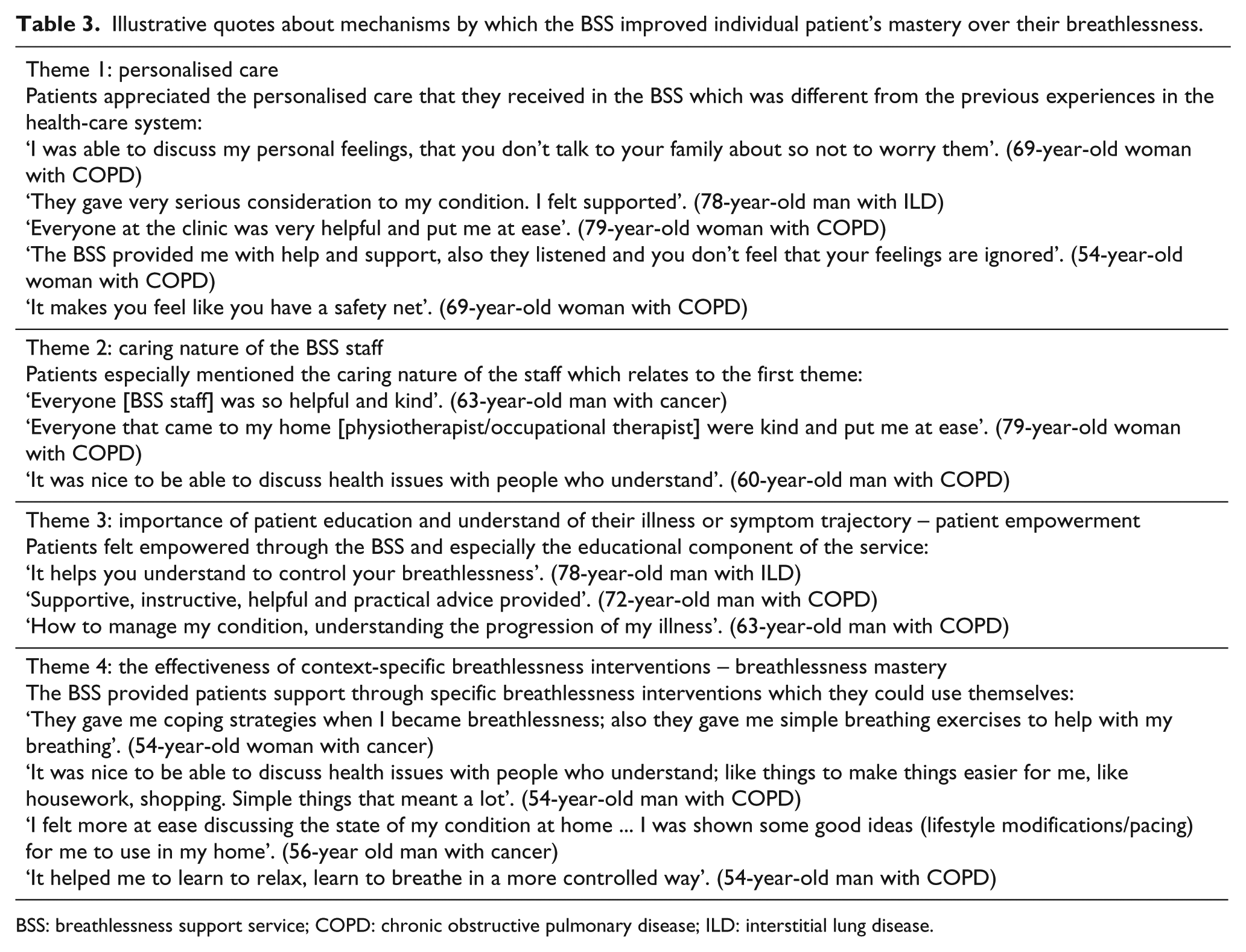
BSS: breathlessness support service; COPD: chronic obstructive pulmonary disease; ILD: interstitial lung disease.
Participation in research
When the patients were asked about participating in the research, 23 (92% (95% CI: 81%–103%)) patients said that they would definitely participate in the research again, the remaining 2 patients reported that they did not know if they would. A total of 18 (72% (95% CI: 54%–90%)) patients reported that they felt their involvement in research was a worthwhile experience.
Discussion
The main finding of this study is that the BSS was well accepted by patients; just over half of the respondent rated the care they received by the BSS as excellent. Patients reported that the BSS, through its holistic approach to the management of breathlessness, not only provided them with skills and interventions to better manage their breathlessness but also acknowledged additional coexisting symptoms, for example, pain and immobility. Moreover, the BSS provided patients with additional support and information regarding additional supportive services e.g., community palliative care and pulmonary rehabilitation.
Significance of the findings
Although this study was not designed to identify the precise BSS components that helped patients, themes identified from the free text comments and answers provided specific to the BSS interventions suggest a combination of management strategies (both education of patients and use of specific therapies) combined with a person-centred approach applied by caring and skilled staff, of the BSS. Specific components highlighted by patients included breathing exercises, education, the fan, discussions around crisis management, pacing, talking and active listening by the BSS team.
Participants identified that their treatment as individuals, coupled with the (perceived) caring nature of BSS staff, made them feel comfortable and confident (Table 3). This is a similar finding to that reported by Preston et al., 14 where patients felt both more comfortable and more confident with caring staff who were responsive to their individual needs, whereas patients reported feelings of distress (such as anxiety, unimportance and powerlessness) when care was perceived as not being personalised. The focus of management on individual concerns also responds to findings that individual breathlessness trajectories do not reflect summary trajectories. 15
In the context of advanced disease, breathless patients are likely to feel little control over their situation and future.16, 17 Offering ways that they can personally make life better for themselves is vital. 7 Patients may command a sense of control in varying ways: regaining control during breathlessness episodes, having a personal role in their symptom management and feeling more in control in the wider illness context. Increased control has been previously demonstrated to be associated with reduced distress due to breathlessness.4,5,8,18 An increased perception of control and understanding of their breathlessness symptom through patient education and context specific interventions were themes that emerged from the patients’ free text comments about the BSS. This is supported by recommendations by Syrett and Taylor. 19
The BSS did not include a core exercise component, in contrast to other breathlessness management interventions, such as those used in pulmonary rehabilitation for COPD.20, 21 For some patients, especially those who are frail and nearing end of life, formal exercise may not be an appropriate intervention. However, some patients reported that they were provided with information or interventions to help improve muscle strength to increase mobility and function, as lower limb muscle function in patients with chronic respiratory disease is of prognostic importance.22, 23
For some patients breathlessness episodes are short (termed episodic) and severe with significant differences between COPD and lung cancer patients. 24 Episodic breathlessness is associated with panic, lack of control, helplessness experiences by both the patient and carer often resulting in accident and emergency (A&E) attendances.25–27 To address this unmet need, a core intervention of the BSS was breathlessness crisis management, which patients found to be useful. This further demonstrates the holistic nature of the BSS, as breathlessness cannot be treated in isolation to its complex physiological, psychological and environmental components.
Two key points were raised by patients regarding further improvements to the service. First, with reference to the social element of the BSS, enhancement of social interaction is of great importance to participants, as illustrated by one BSS study participant, who suggested access to a local support group for patients and carers living with breathlessness to help sustain and build upon the positive effects of the BSS. Such peer-support groups have shown positive outcomes in patients with cancer and COPD, improving patient’s coping skills and overall well-being.28, 29
Second, one patient suggested that we should routinely ask ‘whether there was anything they wished to discuss during the consultation that they could not talk about with their family’. Reinforcing the importance of using open questions in the holistic assessment of these complex patients, encompassing patient and family autonomy and dignity which is the basic tenet of palliative care,30, 31 this, by necessity, places value on the patient and their family’s needs and desires regarding the patient’s illness, treatment and likely prognosis. Our findings are consistent with previous authors who demonstrated that the adoption of the palliative care approach for all patients with advanced disease reduces levels of dissatisfaction with hospital-based services. It is argued that the adoption of the principles of palliative care in all aspects of health care would greatly improve satisfaction with health-care provision. 30
Research is possible despite the debilitating nature of the advanced disease in this group of patients as for those patients that responded to the questionnaire they reported that they viewed their involvement in research, as a beneficial and worthwhile experience, a finding consistent with previous studies.32, 33 However, these findings must be interpreted in context of the low response rate. Moreover, these questions were regarding individuals’ overall experience of research and not the experimental design of the BSS RCT. Acknowledging these limitations, we feel that we have a duty to provide such patients with the opportunity to participate meaningfully in appropriate and relevant research for themselves and their families.
Limitations of the study
The low response rate and consequent small sample size of this study is a limitation of both this methodological approach and of this study. However, accepting this limitation, we feel that the patients who responded to the questionnaire are representative of the patients who received the BSS.
The aim of the questionnaire was to assess patient’s experience of the BSS; it did not include specific question regarding severity and nature of symptoms, acceptability of specific interventions provided or length of appointments. The BSS in composition is complex and individualised to patient’s individual circumstances; therefore, we built this questionnaire to measure the overall experience of the BSS and not its component parts.
We acknowledge that this study only provides information about the patient experience and satisfaction of accessing the BSS, but these data are important for service modelling and future development of breathlessness services.
Conclusion
Patients’ satisfaction with the BSS was high, with many patients rating the care they received as excellent, reporting that attending the clinic was a worthwhile and a positive experience. In addition to providing changes in breathlessness support, the BSS acknowledged the complexity of breathlessness in the presence of coexisting symptoms, an approach that patients valued.
Footnotes
Acknowledgements
We thank all the patients who participated in this research; everybody who identified and screened patients for this study, especially the Palliative Care, Respiratory Medicine and Physiotherapy Departments at King’s College Hospital (London, UK) and the Community Palliative Care teams across Guy’s and St Thomas’ Hospitals (London, UK); H. Bellas (physiotherapist), E. Brink (social worker), J. Kelly (clinical nurse specialist) and the occupational therapists for their input in the delivery of breathlessness support service and C. Pannell and S. de Wolf-Linder (research nurses) for their support; members of our project advisory group for their advice during the course of the study and in particular J. Taylor of St Christopher’s Hospice (London, UK) for allowing us to use the breathlessness poem; and J. Fuller and J. Davies for providing administrative support during this project. I.J.H., C.B., C.J.J., W.G., P.M.C and J.M. conceived the idea of the study and secured funding. I.J.H., C.B., C.J.J., C.C.R. and J.M. set up the study. J.M., C.C.R., C.J.J. and I.J.H. provided the intervention. C.B. and C.C.R. oversaw the study. C.C.R. checked and cleaned the data. C.C.R. analysed the data. C.C.R. and I.J.H. produced the first draft of this article. All authors commented on and contributed to the final draft. I.J.H. is the guarantor. All authors had full access to all of the data of the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was funded mainly by a National Institute for Health Research (NIHR) grant from Research for Patient Benefit (PBPG-0808-17311). This report presents independent research funded by the NIHR under its Research for Patient Benefit (RfPB) programme (PB-PG-0808-17311). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. Additional support for the work and interviews was from an NIHR senior investigator award and the Cicely Saunders International breathlessness programme. The UKCRC-registered King’s Clinical Trials Unit at King’s Health Partners is part funded by the National Institute for Health Research (NIHR) Biomedical Research Centre for Mental Health at South London and Maudsley NHS Foundation Trust and King’s College London and the NIHR Evaluation, Trials and Studies Coordinating Centre (NETSCC). The funders of the study had no role in protocol design, collection or analysis of the data or interpretation or writing of the results.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.