
Abstract
Background:
The London Chest Activities of Daily Living Scale measures the impact of breathlessness on both activity and social functioning. However, the London Chest Activities of Daily Living Scale is not routinely used in patients with advanced disease.
Aim:
To assess the psychometric properties of the London Chest Activities of Daily Living Scale in patients with refractory breathlessness due to advanced disease.
Design:
A cross-sectional secondary analysis of data from a randomised controlled parallel-group, pragmatic, single-blind fast-track trial (randomised controlled trial) investigating the effectiveness of an integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness, known as the Breathlessness Support Service (NCT01165034). All patients completed the following questionnaires: the London Chest Activities of Daily Living Scale, Chronic Respiratory Questionnaire, the Palliative care Outcome Scale, Palliative care Outcome Scale–symptoms, the Hospital Anxiety and Depression Scale and breathlessness measured on a numerical rating scale. Data quality, scaling assumptions, acceptability, internal consistency and construct validity of the London Chest Activities of Daily Living Scale were determined using standard psychometric approaches.
Setting/participants:
Breathless patients with advanced malignant and non-malignant disease.
Results:
A total of 88 patients were studied, primary diagnosis included; chronic obstructive pulmonary disease = 53, interstitial lung disease = 17, cancer = 18. Median (range) London Chest Activities of Daily Living Scale total score was 46.5 (14–67). No floor or ceiling effect was observed for the London Chest Activities of Daily Living Scale total score. Internal consistency was good, and Cronbach’s alpha for the London Chest Activities of Daily Living Scale total score was 0.90. Construct validity was good with 13 out of 15 a priori hypotheses met.
Conclusion:
Psychometric analyses suggest that the London Chest Activities of Daily Living Scale is acceptable, reliable and valid in patients with advanced disease and refractory breathlessness.
Keywords
Refractory breathlessness is common in advanced disease.
There is increasing evidence to support the role and benefit of physiotherapy and occupational therapy for patients with breathlessness due to advanced disease. Despite this, patients’ access to these services is often limited.
There is a lack of patient-reported outcome measures (PROMs) specific to breathlessness during activities of daily living (ADLs) in this patient population. Therefore, objective assessment of therapy need in this patient population is difficult.
This paper demonstrates that The London Chest Activities of Daily Living Scale (LCADL) questionnaire is acceptable, reliable and valid to assess the impact of refractory breathlessness on ADLs in patients with advanced disease.
This paper highlights the importance of asking context-specific questions regarding breathlessness during ADLs, which can facilitate onward therapy referrals/interventions.
In clinical practice, the LCADL can be used as both a screening tool to identify therapy needs and assess the impact of therapeutic interventions.
Introduction
Refractory breathlessness (RB) is defined as breathlessness at rest or on minimal exertion that will persist chronically despite optimal treatment of the underlying cause(s). 1 RB is a common and distressing symptom for people in advanced stages of disease. In particular, people suffering from chronic respiratory diseases, cancer and heart failure report RB as a significant symptom towards the end of life.2–4
Recently, we found that an integrated palliative and respiratory care service for patients with advanced disease and RB, known as the Breathlessness Support Service (BSS), improved patients’ mastery over their breathlessness, with a survival benefit for those patients who had early access to the BSS. 5 Key components to this complex intervention were physiotherapy and occupational therapy, which were individually tailored to meet the needs of these patients and their carers, delivered in the patients’ home. 5
There is increasing evidence to support the role and benefit of physiotherapy and occupational therapy for patients with breathlessness due to advanced disease.5,6 Despite this, patients’ access to these services is often limited.
Failure to access therapy services in this patient population may be due to the fact that clinical decisions including referrals to therapy services are often made on the basis of objective tests of lung function and changes thereof. Traditional measures of lung function such as spirometry are poorly correlated to breathlessness and functional impairment. 7 Furthermore, there is a lack of patient-reported outcome measures (PROMs) specific to breathlessness during activities of daily living (ADLs) in this patient population. Therefore, objective assessment of therapy need is difficult.
Potentially, the London Chest Activity of Daily Living Scale (LCADL) may be a useful PROM to assess the functional impact of RB, which may facilitate referral to therapy. The LCADL was developed by Garrod et al.8,9 to measure the impact of breathlessness on ADLs in patients with chronic obstructive pulmonary disease (COPD). The LCADL has been shown to be sensitive to change pre–post pulmonary rehabilitation in patients with COPD. 9 However, the performance of the LCADL in RB is unknown. The primary aim of the study was to examine the psychometric properties of the LCADL in patients with advanced disease and RB. The secondary aim was to investigate if diagnosis or presence of a carer influenced LCADL scores.
Methods
Design
A cross-sectional secondary analysis of data from a randomised controlled parallel-group, pragmatic, single-blind fast-track trial (randomised controlled trial) investigating the effectiveness of an integrated palliative and respiratory care service for patients with advanced disease and RB, known as the BSS. 5 Ethics approval for the study was obtained from the King’s College Hospital ethics committee (Ref. 10/H0808/17). The study protocol is registered with ClinicalTrials.gov (NCT01165034). All patients entering the study gave informed written consent.
Patients
Breathless patients with advanced malignant and non-malignant disease were studied. Patients were referred to the BSS by health care professionals in primary and secondary care. Patients suffered from RB of any cause. Optimal medical management was ensured by the referring health care professionals and patients were considered appropriate for palliative support of breathlessness. These patients were all offered access to two outpatient appointments with respiratory and palliative medicine input, and a joint home visit by physiotherapy and occupational therapy. Patients and carers also had access to a palliative care social worker. 5
Assessments
Data were collected during face-to-face interviews with patients, usually within the patient’s own home prior to randomisation. 5
Pulmonary function
Forced expiratory volume in 1 s (FEV1), slow vital capacity (VC) and peak expiratory flow rate (PEF) were measured in all patients in the seated, upright position using a portable electronic spirometer (Vitalograph 2120®; Vitalograph®, Buckingham, UK). 10 Pulse oximetry was measured at rest in all participants.
Breathlessness
A numerical rating scale (NRS) was used to assess the intensity of the sensation of breathlessness at rest and on exertion over the last 24 h. 11
Symptom-related quality of life
Symptom-related quality of life (QOL) was assessed using the Palliative care Outcome Scale (POS) and POS–symptoms to quantify palliative care symptoms in addition to breathlessness. A high total POS score is indicative of the complexity of individual patient palliative care needs; however, careful review of each component part of the POS is required when planning and evaluating treatments and interventions. 12
Activity of daily living assessment
The LCADL was used to assess the impact and severity of breathlessness on ADLs. The LCADL has been used as an outcome measure in COPD and heart failure, where it has been shown to be valid, reliable and responsive to change.8,9,13 Higher scores reflect greater breathlessness during daily activity and the tool includes an anchor question identifying an individual’s overall perception of the impact of breathlessness on their daily life.
Health – status assessment
The Chronic Respiratory Questionnaire (CRQ) was used to measure health status and was designed for the assessment of change in individuals. It comprises four component scores: Dyspnoea, Fatigue, Emotional function and Mastery. The CRQ is a multidimensional tool and is one of the most widely used measures of QOL in chronic respiratory disease. The CRQ is an interview-administered questionnaire, but a self-administered version maintains validity and responsiveness.14,15
Anxiety and depression
The Hospital Anxiety and Depression Scale (HADS) was used to assess anxiety and depression and consists of 14 items and is scored from 0 to 21, with a score of greater than 10 in either anxiety or depression representing symptoms of clinical significance. 16
Statistical analysis
Five psychometric qualities of the LCADL were evaluated according to standard methodology:17–19
Data quality was assessed by calculating the percentage of missing items (number of missing items/total number of item response possible) for each scale. Open response text fields were not included.
Scaling assumptions were examined by calculating individual item median scores. Inter-item correlations were calculated using Spearman’s correlation coefficients.
Acceptability was determined by analysing the distribution of patients’ total scores (median, range, interquartile range) and floor and ceiling effect if 15% of respondents achieved the lowest or highest possible score, respectively. 18
Internal consistency (reliability) of the LCADL was determined using Cronbach’s alpha coefficient. Internal consistency is valid only if all items form a unidimensional (sub) scale, and the set of items forms a reflective model (i.e. all items are expected to change when the construct changes). 19 A Cronbach’s alpha between 0.70 and 0.95 indicates good internal consistency without homogeneity. 18
Construct validity is the extent to which scores on an instrument relate to other measures. It is given a positive rating if at least 75% of the results are consistent with predefined hypotheses. 18 Construct validity of the LCADL was tested against items within CRQ, POS, POS-s, HADS and NRS breathlessness scores using Spearman’s correlation coefficients, according to predefined hypotheses of convergent validity (moderate and weak) and divergent validity (hypotheses and their results shown in Table 3). 19 We defined the strength of the correlation as strong (0.7–1.0), moderate (0.4–0.7), weak (0.2–0.4) and absent (0.0–0.2). Convergent validity was also tested for the total (or subscale) scores; we hypothesised that the LCADL would correlate with CRQ dyspnoea subscale, CRQ health-related quality of life (HRQL), HADS and NRS breathlessness on exertion. In addition, we hypothesised that there would be no correlation between the LCADL and lung function measures.
To investigate if diagnosis or presence of a carer influenced LCADL scores, LCADL scores were compared between the three main patient groups (COPD, interstitial lung disease (ILD) and cancer) and between patients with and without a carer present using Mann–Whitney U test. Data were analysed using the Statistical Package for Social Science for Windows, version 19 (SPSS Inc., Chicago, IL, USA). p < 0.05 was considered significant.
Data reporting
We searched http://www.equator-network.org/ for publishing guideline for validation studies for health/symptom questionnaires. No publication guidelines were returned; therefore, we report our data in line with Terwee et al.’s 18 quality criteria for reporting measurement properties of health status questionnaires.
Results
A total of 105 patients were recruited to the main study; 7 with regard to this secondary data analysis, nine patients (COPD = 4, Cancer = 3, ILD = 2) were excluded due to incomplete or missing LCADL data.
Eight patients were excluded as they didn’t have a primary respiratory diagnosis (5 = heart failure) or they had an atypical/complex diagnosis (left lower lobe collapse of unknown aetiology associated with severe symptoms; lupus, shrinking lung syndrome and rheumatoid arthritis; severe asthma and gastro-oesophageal reflux disease). A total of 88 patients were included in the data analysis for this article.
Table 1 summarises the participant demographics, pulmonary function and NRS breathlessness scores. Individual item scores for the LCADL are summarised in Figure 1. In all, 11 (12.5%) patients reported little impact of their breathing on their normal ADLs; however, the majority of patients (77 (87.5%)) reported that their breathing impacted a lot on their normal ADLs.
Participant demographics, pulmonary function and NRS breathlessness scores.
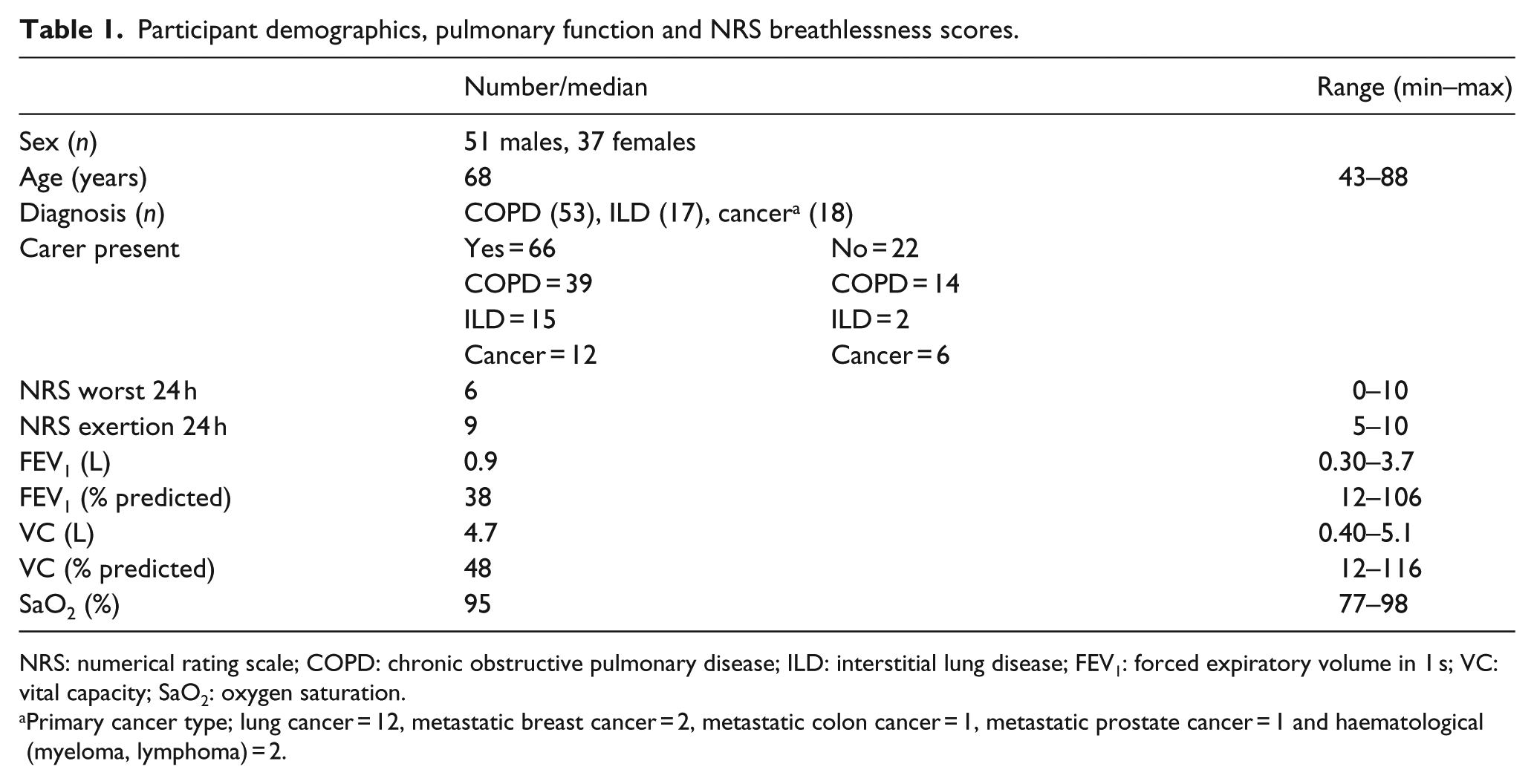
NRS: numerical rating scale; COPD: chronic obstructive pulmonary disease; ILD: interstitial lung disease; FEV1: forced expiratory volume in 1 s; VC: vital capacity; SaO2: oxygen saturation.
Primary cancer type; lung cancer = 12, metastatic breast cancer = 2, metastatic colon cancer = 1, metastatic prostate cancer = 1 and haematological (myeloma, lymphoma) = 2.
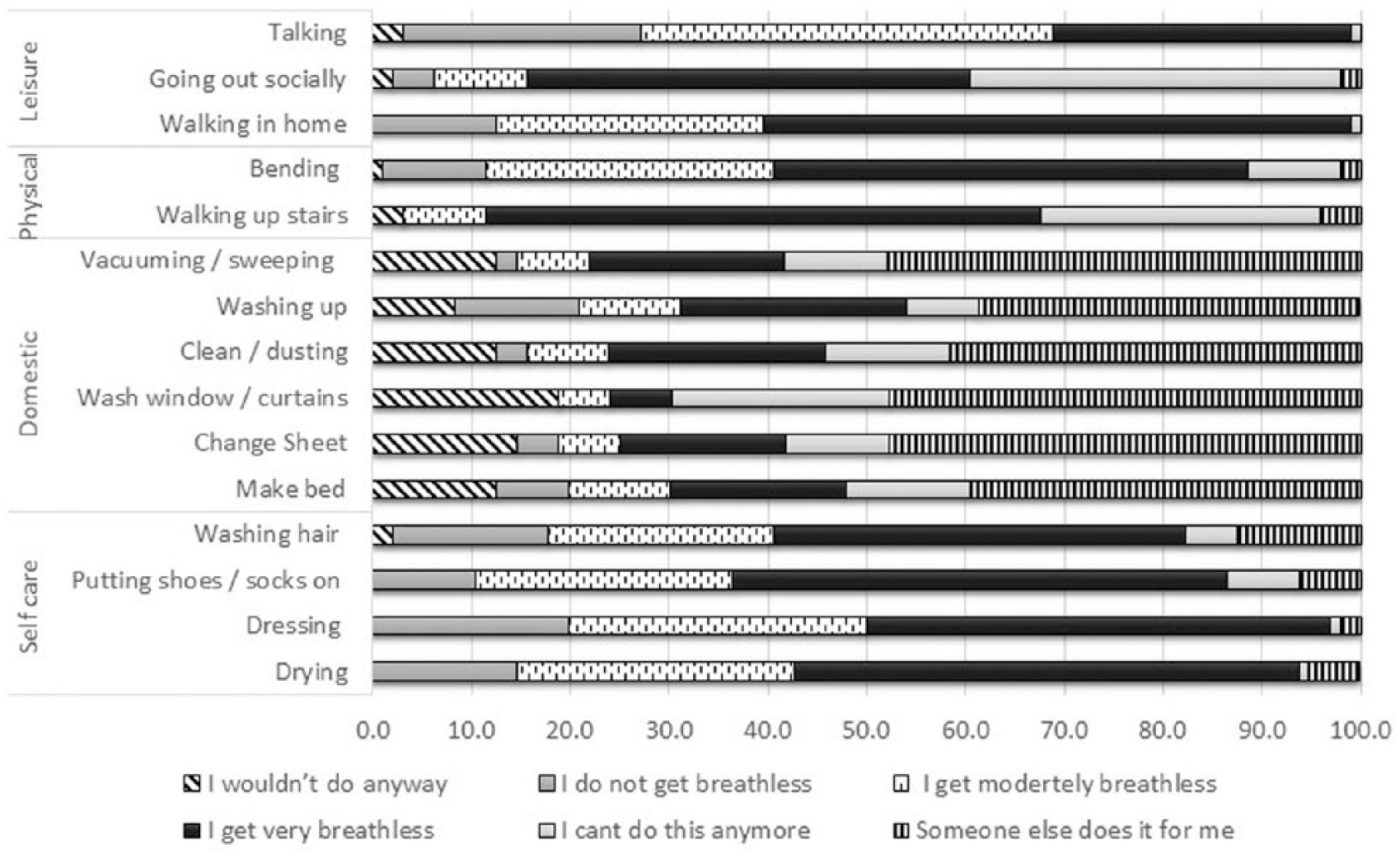
Individual item scores for the LCADL (n = 88).
Scaling assumptions
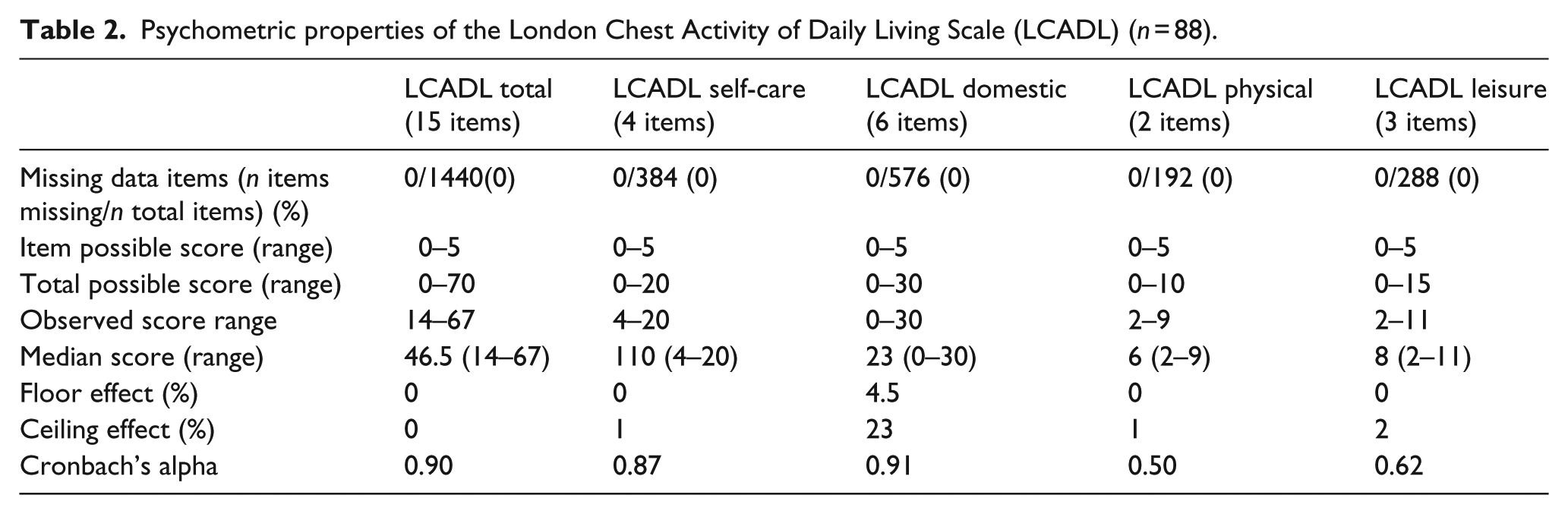
The median item score for the LCADL and subscales with the exception of the domestic subscale were around or above the midpoint (Table 2). The mean (95% confidence interval) inter-item correlation coefficient for single measures was 0.49 (0.43–0.55), p < 0.001.
Psychometric properties of the London Chest Activity of Daily Living Scale (LCADL) (n = 88).
Acceptability
LCADL total and subscales spanned a good range. No floor or ceiling effect was observed for the LCADL total score. However, the LCADL subcategory ‘domestic’ demonstrated a ceiling effect, with 23% of respondents achieving the highest possible score (Table 2).
Internal consistency
Cronbach’s alpha for LCADL total score was 0.90 and for its subscales ranged between 0.50 and 0.91 (Table 2).
Construct validity
Correlations between the LCADL and subscales were analysed according to 15 a priori hypotheses of convergent (moderate to weak) and divergent validity. Of the 15 hypotheses tested, 13 were correct (87%) (Table 3).
A priori hypothesis and results for construct validity using Spearman correlation coefficients of the LCADL and NRS breathlessness scores, CRQ, POS and POS–s, HAD and spirometry.
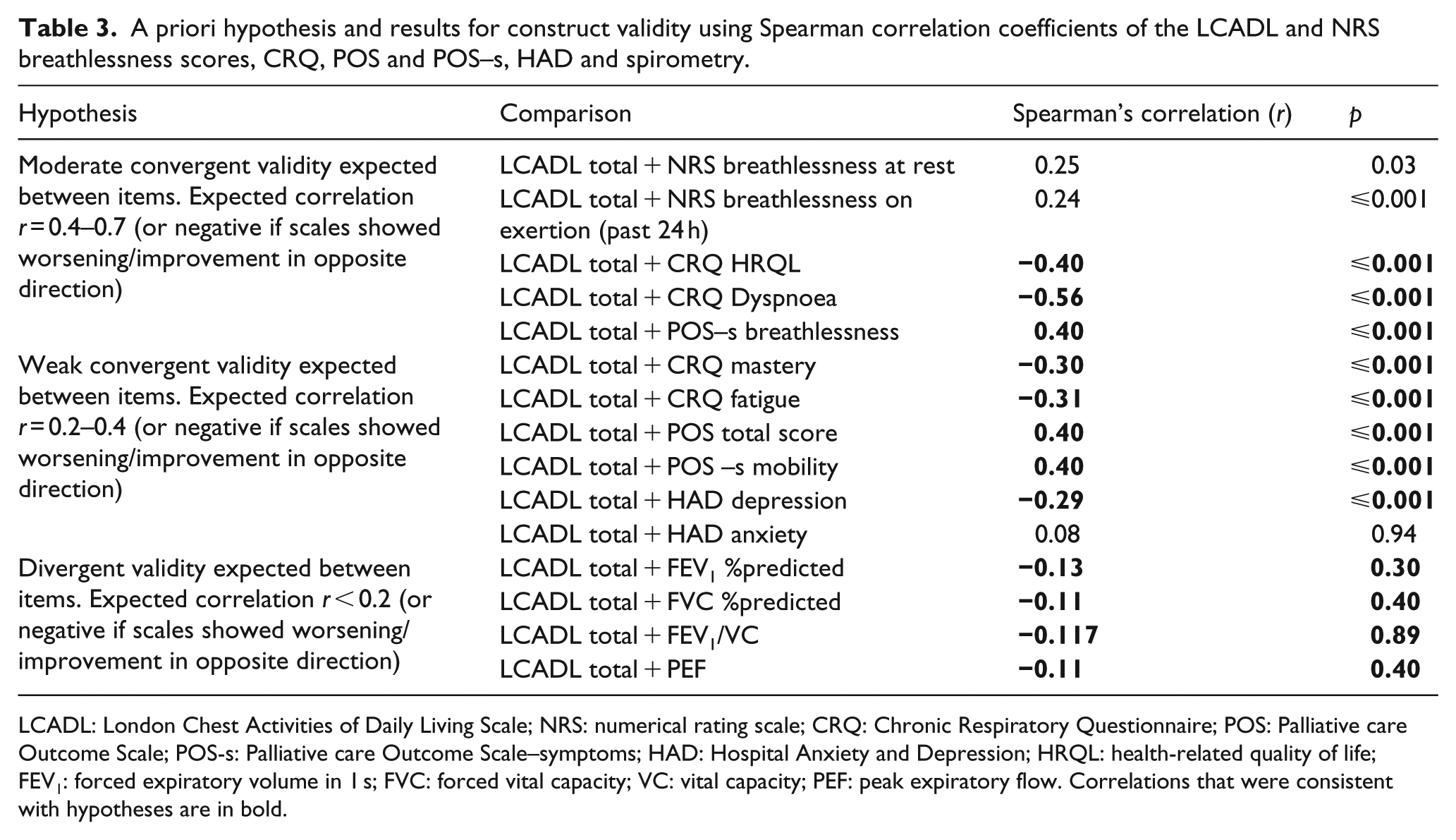
LCADL: London Chest Activities of Daily Living Scale; NRS: numerical rating scale; CRQ: Chronic Respiratory Questionnaire; POS: Palliative care Outcome Scale; POS-s: Palliative care Outcome Scale–symptoms; HAD: Hospital Anxiety and Depression; HRQL: health-related quality of life; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; VC: vital capacity; PEF: peak expiratory flow. Correlations that were consistent with hypotheses are in bold.
Influence of diagnosis or presence of a carer on LCADL scores
The median (range) LCADL score for the COPD patients was 49 (17–67); for cancer patients, it was 44 (16–61) and for ILD patients 39 (14–59). A significant difference was observed for the self-care subcategory of the LCADL between the three patient groups (p = 0.018). Table 4 summarises the LCADL total score and its subcategory scores for these three main patient groups.
Total LCADL score and its subcategory scores categorised by diagnosis (COPD, ILD and cancer) and the presence of a carer.
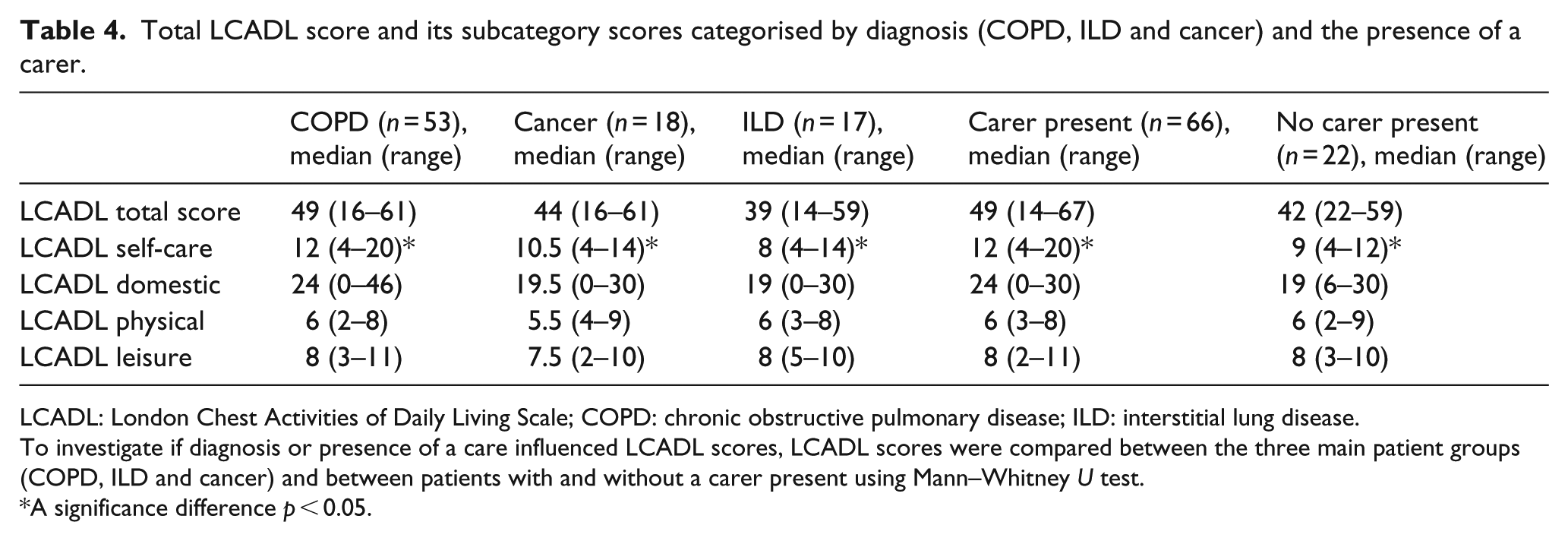
LCADL: London Chest Activities of Daily Living Scale; COPD: chronic obstructive pulmonary disease; ILD: interstitial lung disease.
To investigate if diagnosis or presence of a care influenced LCADL scores, LCADL scores were compared between the three main patient groups (COPD, ILD and cancer) and between patients with and without a carer present using Mann–Whitney U test.
A significance difference p < 0.05.
No difference in LCADL total scores was observed between those patients who had a carer present and those without. However, a significant difference was observed for the self-care subcategory of the LCADL between patients with and without a carer (12 (4–20) vs 10 (4–12), p = 0.03) (Table 4).
Discussion
The psychometric analyses of the LCADL suggest that the instrument is acceptable, reliable and valid to assess the impact of RB on ADLs in patients with advanced disease.
Significance of the findings
To test the application of the LCADL in patients with advance disease and RB, we hypothesised that the LCADL would reflect other patient-reported measures of breathlessness, symptom burden and HRQL. There was a moderate relationship between the LCADL, HRQL measured on the CRQ and its sub-domain dyspnoea. A finding consistent with previous studies in COPD7,8 and heart failure 20 was that LCADL demonstrated good relationship with HRQL, functional status and exercise capacity.
A weak correlation between NRS breathlessness intensity at rest and the LCADL was observed. This is not surprising, as we have recently demonstrated that patients with chronic respiratory disease have a blunted perception of neural respiratory drive (NRD) and breathlessness at rest, where breathlessness onset/perception is associated with physical activity.21,22,25,26 Therefore, in the clinical context, if we only assess breathlessness intensity at rest, very important clinical information about the true impact of the patient’s condition is lost.
The observed weak relationship between NRS intensity on exertion over the past 24 h and LCADL may be a consequence of patients avoiding ADLs that makes them breathless, resulting in NRS scores over the period of recall not being very high. Hence, the correlation between the functional consequence of breathlessness (impact measured using the LCADL score) and the NRS exertion (breathlessness intensity) is low. The advantage of the LCADL score over NRS breathlessness intensity scores is that it allows quantification of the functional limitation of breathlessness specific to the individual patients’ circumstance.
The LCADL was correlated to the CRQ dyspnoea domain, which rates breathlessness intensity during patient-defined activities. A limitation of the CRQ dyspnoea domain is that it only provides a global measure of dyspnoea intensity during activity.13,14
In accordance with other studies,8,23 there was no statistical correlation between pulmonary function measures and the LCADL. This supports the view that measures of lung function impairment are a poor prognostic of disability and do not reflect the burden of breathlessness perceived by the patient, particularly when considering advanced disease.
Comparison between disease groups (COPD, ILD and cancer) showed that the median scores of LCADL were not significantly different, although there was a trend towards a higher score in COPD patients. However, the subcategory ‘self-care’ was significantly higher in COPD compared with the other condition-specific groups. The COPD population reported higher scores (12) than cancer (10.5) or ILD (8). This suggests that patients with COPD may benefit from assessment of functional breathlessness limitation early in the trajectory of their disease.
The self-care component of the LCADL provides information about limitations in ADLs due to breathlessness. This component of the questionnaire is very focussed on personal hygiene activities such as washing, drying and dressing. Importantly, assessment of breathlessness limitation on ADL may specifically facilitate discussion with regard to more focused palliative therapy, approach to symptom management rather than disease orientated treatments, thus facilitating referral to therapy services.
Anxiety and depression are elevated in COPD 24 and palliative care patients, 21 and in this study, a correlation was observed between depression, the LCADL and its subcategory leisure. In all, 45% of patients reported that they become very breathless going out socially, with 38% patients reporting that they were no longer able to go out socially due to their level of breathlessness as measured on the social participation question on the LCADL, reflective of the negative downward spiral that breathlessness has on activity of daily living, subsequent loss of muscle strength, function and ability to fully participate and engage within society. 22 The LCADL may therefore be a useful tool to tease out issues concerning breathlessness in the context of activity and social role, which may facilitate discussion regarding the psychosocial impact of breathlessness and subsequent referral to physiotherapy and occupational therapy to improve social participation through interventions such as mobility aids, pacing, breathlessness management, exercise and therapeutic group activities.
The LCADL subcategory self-care was significantly higher where carer support was available. An unusual aspect of the LCADL is that it asks specifically about activities an individual can still do (but is breathless) and activities they require assistance for or have had to give up. Higher scores indicate that the individual is more affected and where help is required or an activity has had to be given up. This is reflected by the observed ceiling effect for the subcategory domestic where 23% of respondents achieved the highest possible score. Although not tested in this study, the LCADL may be a useful tool to explore unmet needs with respect to social services support or occupational therapy input.
The majority of outcome scales and scores used to quantify breathlessness measure the intensity or the symptom burden of breathlessness, but fail to measure the impact of the symptom on ADLs.
Comprehensive assessment of patients’ supportive needs in advanced disease requires sensitive questioning, inclusion of questions regarding breathlessness specifically in the context of ADLs. Potentially using the LCADL in the clinical assessment of patients with RB may aid these discussions and highlight patients who may not traditionally be considered for physiotherapy or occupational therapy, thus facilitating access to these specialist services.
Critique of the method
When interpreting these results, some limitations need to be acknowledged. We are unable to make comment on the discriminative ability of the LCADL from our current data set, and future studies could include performance status measures such as the World Health Organization (WHO) Performance status and Karnofsky which may provide useful comparators.
We did not conduct test–retest analysis on this data set, so the reliability of this tool over time in this patient population remains unknown. The LCADL control group data at 6 weeks are inappropriate for test–retest data because many patients were in the progressive phase of their disease. In the context of this patient population, a 6-week test–retest window does not reflect a stable state. Our reasoning is reinforced by the fact that the drop out due to illness or death was quite high in our control group.
Conclusion
Psychometric analyses suggest that the LCADL is acceptable, reliable and valid in patients with advanced disease and RB. The LCADL may highlight previously unreported areas of need with respect to breathlessness during ADLs and the extent of social support required which may facilitate access to services such as physiotherapy and occupational therapy.
Footnotes
Acknowledgements
We thank all the patients who participated in this research: everybody who identified and screened patients for this study, especially the Palliative Care, Respiratory Medicine and Physiotherapy Departments at King’s College Hospital (London, UK) and the Community Palliative Care teams across Guy’s and St Thomas’ Hospitals (London, UK); H. Bellas (physiotherapist), E. Brink (social worker), J. Kelly (clinical nurse specialist) and the occupational therapists for their input in the delivery of breathlessness support service, and C. Pannell and S. de Wolf-Linder (research nurses) for their support; members of our project advisory group for their advice during the course of the study and in particular J Taylor of St Christopher’s Hospice (London, UK) for allowing us to use the Breathlessness poem and J. Fuller and J. Davies for providing administrative support during this project.
Author contributions
I.J.H., C.B., C.J.J. and J.M. conceived the idea of the study and secured funding. I.J.H., C.B., C.J.J., C.C.R. and J.M. set up the study. J.M., C.C.R., C.J.J. and I.J.H. provided the intervention. C.B. and C.C.R. oversaw the study. C.C.R. checked and cleaned the data. C.C.R. and R.G. analysed the data. C.C.R., R.G. and I.J.H. produced the first draft of the paper. All authors commented on and contributed to the final draft. I.J.H. is the guarantor. All authors had full access to all of the data of the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by a National Institute for Health Research (NIHR) grant from Research for Patient Benefit (PBPG-0808-17311). This report presents independent research funded by the NIHR under its Research for Patient Benefit (RfPB) programme (PBPG-0808-17311). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. The funders of the study had no role in protocol design, collection or analysis of the data, or interpretation or writing of the results.