
Abstract
Background:
Effective patient–family communication can reduce patients’ psychosocial distress and relieve family members’ current suffering and their subsequent grief. However, terminally ill patients and their family members often experience great difficulty in communicating their true feelings, concerns, and needs to each other.
Aim:
To develop a novel means of facilitating meaningful conversations for palliative patients and family members, coined Dignity Talk, explore anticipated benefits and challenges of using Dignity Talk, and solicit suggestions for protocol improvement.
Design:
A convergent parallel mixed-methods design. Dignity Talk, a self-administered question list, was designed to prompt end-of-life conversations, adapted from the Dignity Therapy question framework. Participants were surveyed to evaluate the Dignity Talk question framework. Data were analyzed using qualitative and quantitative methods.
Setting/participants:
A total of 20 palliative patients, 20 family members, and 34 healthcare providers were recruited from two inpatient palliative care units in Winnipeg, Canada.
Results:
Most Dignity Talk questions were endorsed by the majority of patients and families (>70%). Dignity Talk was revised to be convenient and flexible to use, broadly accessible, clearly stated, and sensitively worded. Participants felt Dignity Talk would be valuable in promoting conversations, enhancing family connections and relationships, enhancing patient sense of value and dignity, promoting effective interaction, and attending to unfinished business. Participants suggested that patients and family members be given latitude to respond only to questions that are meaningful to them and within their emotional capacity to broach.
Conclusion:
Dignity Talk may provide a gentle means of facilitating important end-of-life conversations.
Effective patient–family communication is foundational to relationships anchored in mutual support and understanding, which can buffer emotional distress for both patients and families.
Patients with life-limiting illness and their family members often experience great difficulty in communicating their true feelings, concerns, and needs.
Numerous interventions have been developed to facilitate communication between patients and healthcare providers; however, interventions aimed at facilitating communication between palliative patients and their families are limited.
Interventions developed to facilitate end-of-life communication typically focus on patient and clinician exchanges. This study developed a list of question prompts coined Dignity Talk that may provide a viable means of facilitating important, sensitive conversations between palliative patients and their families.
Palliative patients, family members, and healthcare providers perceive Dignity Talk would be valuable in enhancing family connections and relationships, enhancing patients’ self-worth and dignity, promoting effective interaction, and attending to unfinished business.
Dignity Talk may be useful in clinical practice as a communication prompt between patients and families for important and meaningful end-of-life conversations.
Dignity Talk has the potential to enhance end-of-life experience by engendering a mutual sense of meaning for palliative patients and their families through the sharing of memories, gratitude, forgiveness, wishes, and hopes.
Introduction
Patients with life-limiting illness and their families encounter a complex array of challenges and concerns that threaten their psychological, existential, and spiritual integrity.1,2 Poor family communication can increase feelings of loneliness and hopelessness in patients with advanced cancer, resulting in increased psychosocial stress.3,4 Family connectedness can bolster patient well-being toward the end of life; 5 however, terminally ill patients and their family members often experience great difficulty in communicating their true feelings, concerns, and needs because of the desire to protect each other from being exposed to emotional distress.4,6
The quality of patient–family communication affects family members during the final phase of the patient’s illness and in the bereavement period. 7 A phenomenological study of the experience of spousal grief and bereavement suggests that meaningful communication between patient/family member dyads is important, and remembering and constructing memories during the patient’s illness is a way of helping families make sense of their experience. 8 A study of family members who had a loved one die in hospice identified regret and frustration when their loved one’s condition precluded communication. 9 Similar findings were reported in another study, which indicated that family caregivers reflected positively on their grief experience when they had been able to communicate effectively with the patient and enjoy their company despite the ravages of disease. 10
Numerous interventions such as question prompt lists and communication support programs have been developed to facilitate end-of-life communication. However, most of them are designed to facilitate communication between patients with cancer and their healthcare providers (HCPs) regarding illness and treatment,11,12 prognosis,13,14 decision making, 15 and psychosocial and spiritual issues.11,16 These interventions prompt patients to ask questions and satisfy their information needs; few demonstrate influence on psychological outcomes.11,15,17 –20 Several studies have used question prompt lists to encourage HCPs and family caregivers to discuss end-of-life issues.21,22 Recently, a Serious Illness Conversation Guide was developed to guide patient/family–clinician communication about end-of-life care goals and decisions. 23 However, interventions aimed at facilitating communication between palliative patients and their families are rarely examined. Mowll et al. 24 used the Patient Dignity Inventory (PDI) to guide couples in conversations about living with advanced cancer. The PDI-Couple Interview enabled couples to express their concerns to one another, identify differences in understanding, gave permission to speak with each other, enhanced closer communication, and helped prepare them for the challenges ahead.
Patients report that sharing their palliative care experience with supportive family members enhances their relationship and strengthens bonds. 25 The desire to feel valued by and connected to others is very important. 26 However, palliative patients and their family members are often afraid to share their feelings and needs, resulting in profoundly important issues not being broached. To help patients and their families with these challenges, we developed a self-administered intervention coined Dignity Talk, to facilitate meaningful conversations between palliative patients and their families. In this article, we described how Dignity Talk was developed and evaluated by a group of palliative patients, family members, and HCPs.
Methods
Research design
Our research team developed a list of question prompts, using the Dignity Therapy question framework as an initial template. Dignity Therapy is a brief, individualized psychotherapy, engaging terminally ill patients in a therapist-facilitated conversation designed to invoke a sense of meaning and purpose, provide patients a sense of affirmation and continued sense of worth, and fulfill generativity needs. 27 The prototype for Dignity Talk came about by way of reviewing the Dignity Therapy questions, and restating each question in a fashion that would lend itself to self-administration, hence enabling patients and families to engage in conversations. Feedback on this initial prototype was sought from five patients, six family members, and four healthcare professionals. On the basis of their input, two questions including ‘what we have meant to each other’ and ‘regret and forgiveness’ were added to the protocol. A separate set of paired questions were developed, with one version meant for the patient and the other for the family respondent. Key differences between Dignity Talk and Dignity Therapy are shown in Table 1.
A comparison of Dignity Talk with Dignity Therapy.
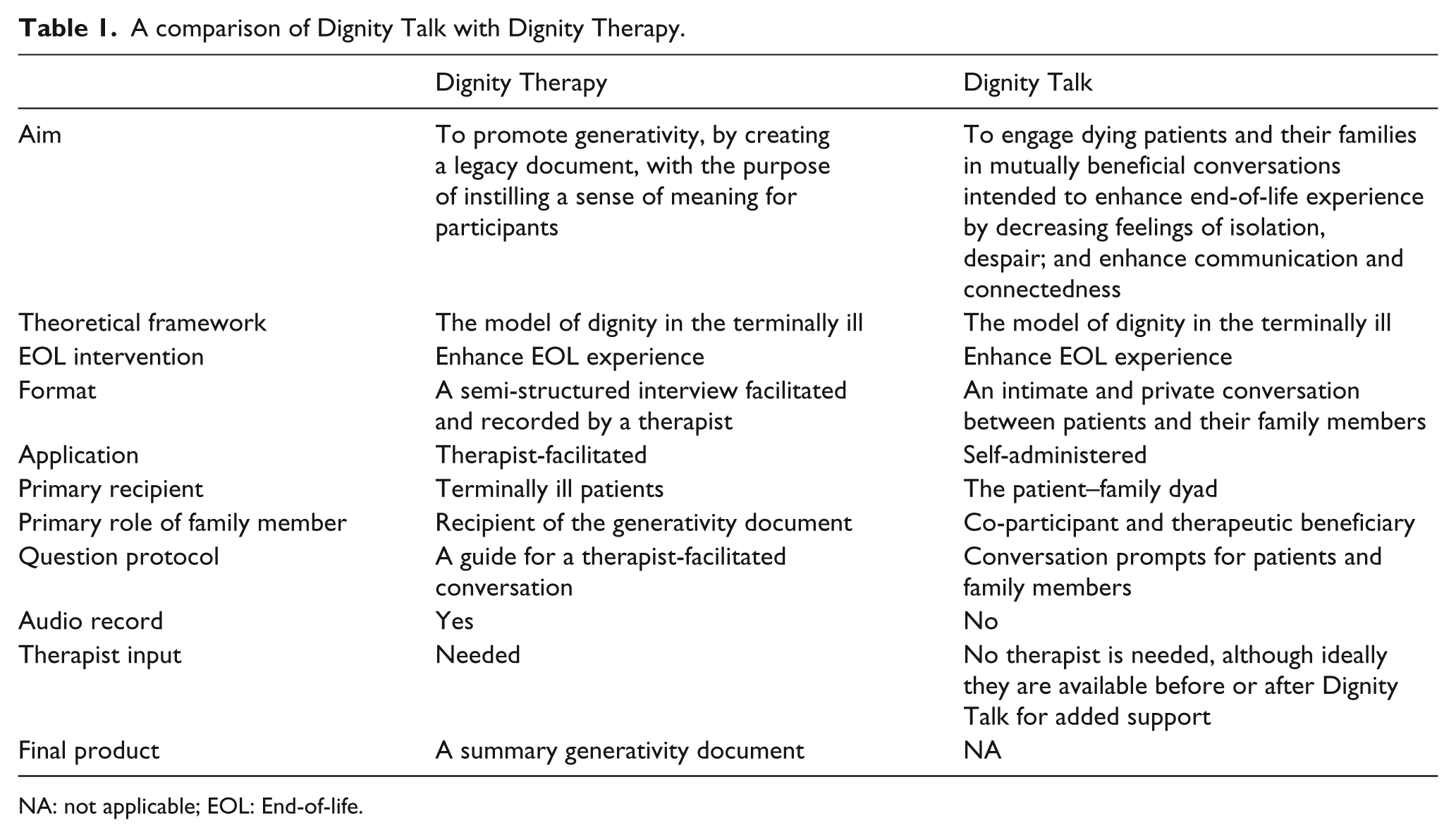
NA: not applicable; EOL: End-of-life.
A convergent parallel mixed-methods design was used for the study. 28 The Dignity Talk guidelines and questions were evaluated using both quantitative and qualitative data. Data were collected simultaneously and priority was given to both forms of data. Convenience sampling was used to recruit participants, including palliative patients, family members, and HCPs. Patients and family members were recruited from two inpatient palliative care units within the Winnipeg Regional Health Authority and were identified by staff members on the units between June and November 2013. Eligibility criteria for patients included being 18 years of age or older, able to speak and read English, having a life-limiting illness with approximately 6 months or less to live, able to provide informed consent, and showing no evidence of confusion or delirium based on clinical consensus. Eligible family members were 18 years of age or older, able to speak and read English, able to provide informed oral and written consent, and able to provide meaningful and coherent feedback regarding Dignity Talk. Eligible HCPs had to be employed on one of the two participating study units and be directly involved in clinical care. They were recruited by emails, posters, and individual invitation by the research nurse.
Data collection
Ethical approval was obtained from the University of Manitoba Health Research Ethics Board and site access from the Research Access Committee at the participating institutions. Written informed consent was obtained from all participants.
Patients and family members were interviewed individually either in person or by phone. The research nurse read each of the Dignity Talk questions to patients and family members and asked them to evaluate its clarity, sensitivity, relevance, and importance. Open-ended questions were asked to elicit concerns about Dignity Talk, suggestions for improvement, and comments about its perceived impact on patient and family experience.
Six focus groups were conducted with interdisciplinary groups of HCPs who were invited to share suggestions for improving Dignity Talk and raise concerns about its use. Each focus group consisted of 3–11 members of the interdisciplinary team, including physicians, nurses, social workers, and healthcare aides. Demographic information was collected for all participants. Patient diagnostic information was collected from the medical chart by the research nurse. Answers to open-ended questions were audio-recorded, transcribed verbatim, and summarized.
Data analysis
Descriptive statistics were used to describe demographic data. Feedback obtained from patients and family members regarding clarity, sensitivity, relevance, and importance of Dignity Talk questions were analyzed quantitatively (endorsement rate). Chi-square analysis was employed to compare the overall endorsement rate by patients and family members. Qualitative data were analyzed line-by-line using the constant comparative techniques to identify recurrent themes by the first two authors. 29 Quantitative and qualitative results were finally merged and interpreted, based on which the Dignity Talk question framework was revised. An audit trail, documenting the logic of the researchers, processes of data collection and analysis, and personal notes, was created. All authors discussed the audit trail and the emerging themes until consensus was reached.The research team included members from psychiatry, psychology, and nursing, as well as research personnel.
Results
Demographic characteristics
The final sample comprised 20 patients, 20 family members, and 34 HCPs. A total of 12 patients and 10 family members declined citing reasons of being too sick to take part, or not interested. Participants’ demographic characteristics are shown in Tables 2 and 3.
Demographic characteristics of patients (N = 20) and family members (N = 20).
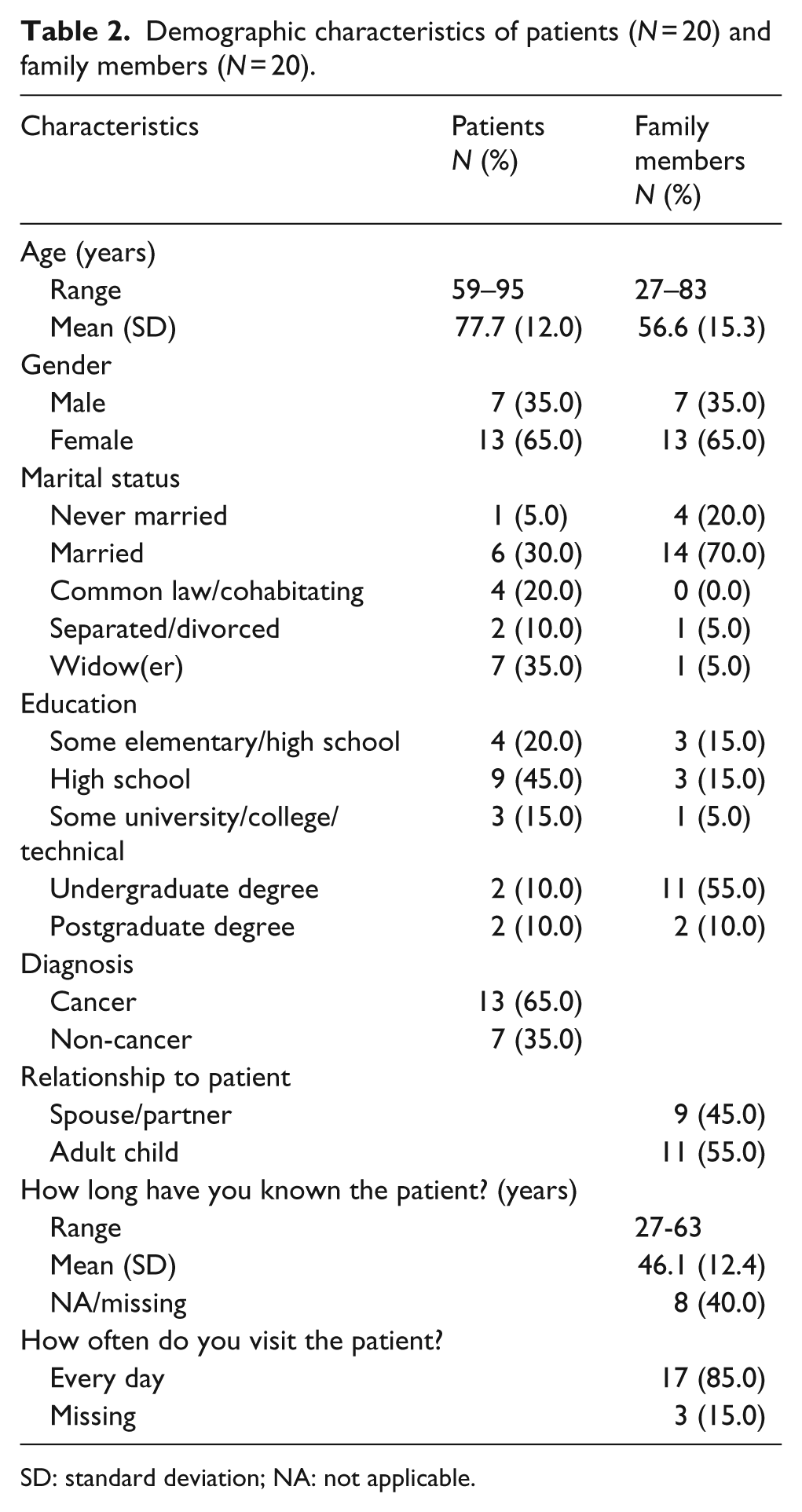
SD: standard deviation; NA: not applicable.
Demographic characteristics of healthcare providers (N = 34).
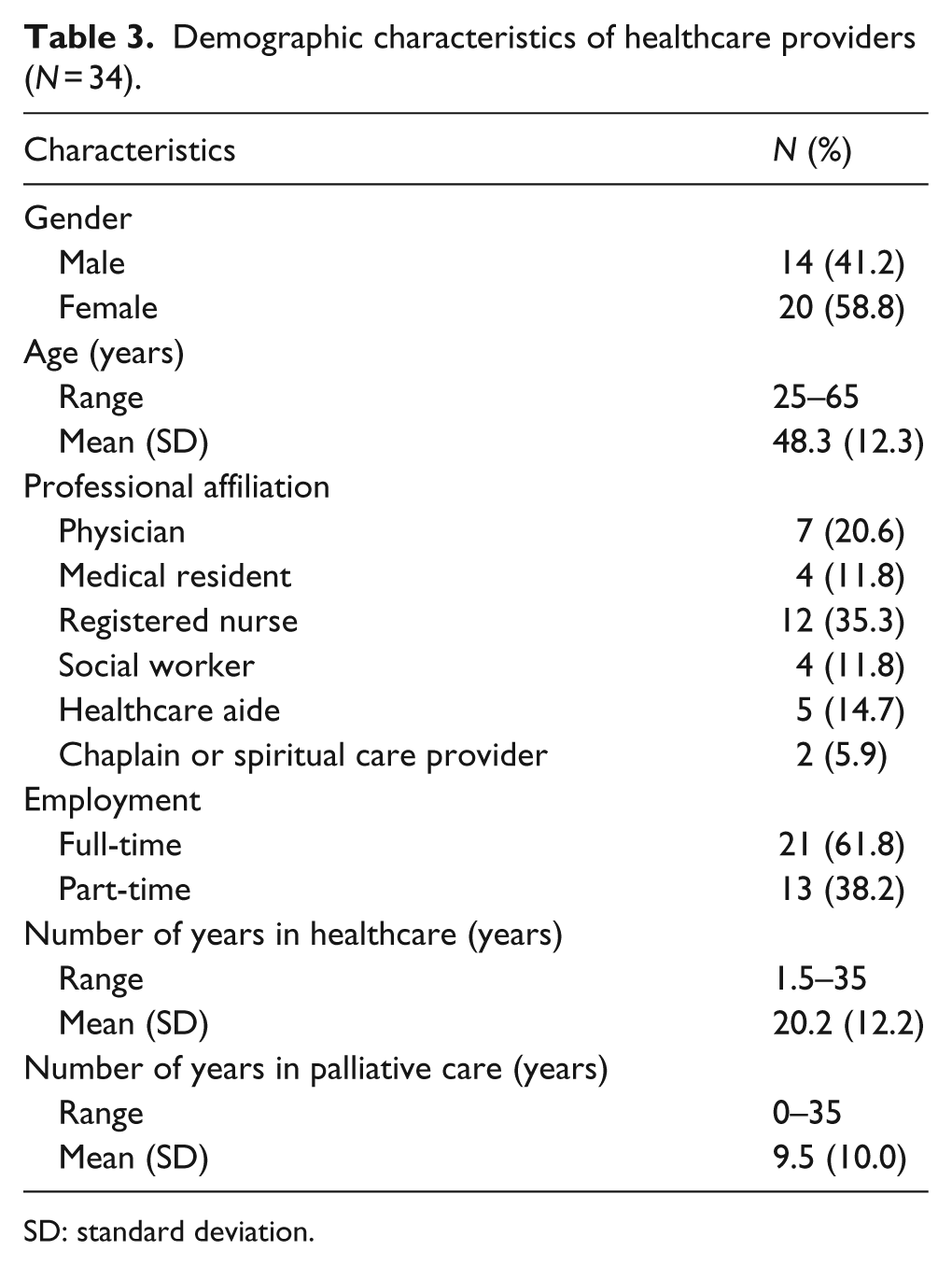
SD: standard deviation.
Endorsement of Dignity Talk questions
Table 4 shows the endorsement rate by patients and family members for each Dignity Talk question regarding clarity, sensitivity, relevance, and importance. In terms of clarity and sensitivity, all questions were endorsed by 85.0% or more of either patients or family members. In total, 10 out of 11 questions had been discussed previously by 70.0% or more of either patients or family members; 7 out of 11 questions would be discussed by 70.0% or more of either group. Six out of 11 questions were considered important by 70.0% or more of either patients or family members. In all, 10 out of 11 Dignity Talk questions received overall endorsed from 70.0% or more of patients; 8 out of 11 by 70.0% or more of family members. Question 6 regarding regrets and forgiveness was the only item receiving less than 70.0% overall endorsement by both groups.
Dignity Talk framework endorsement rates by patients (N = 20) and family members (N = 20).
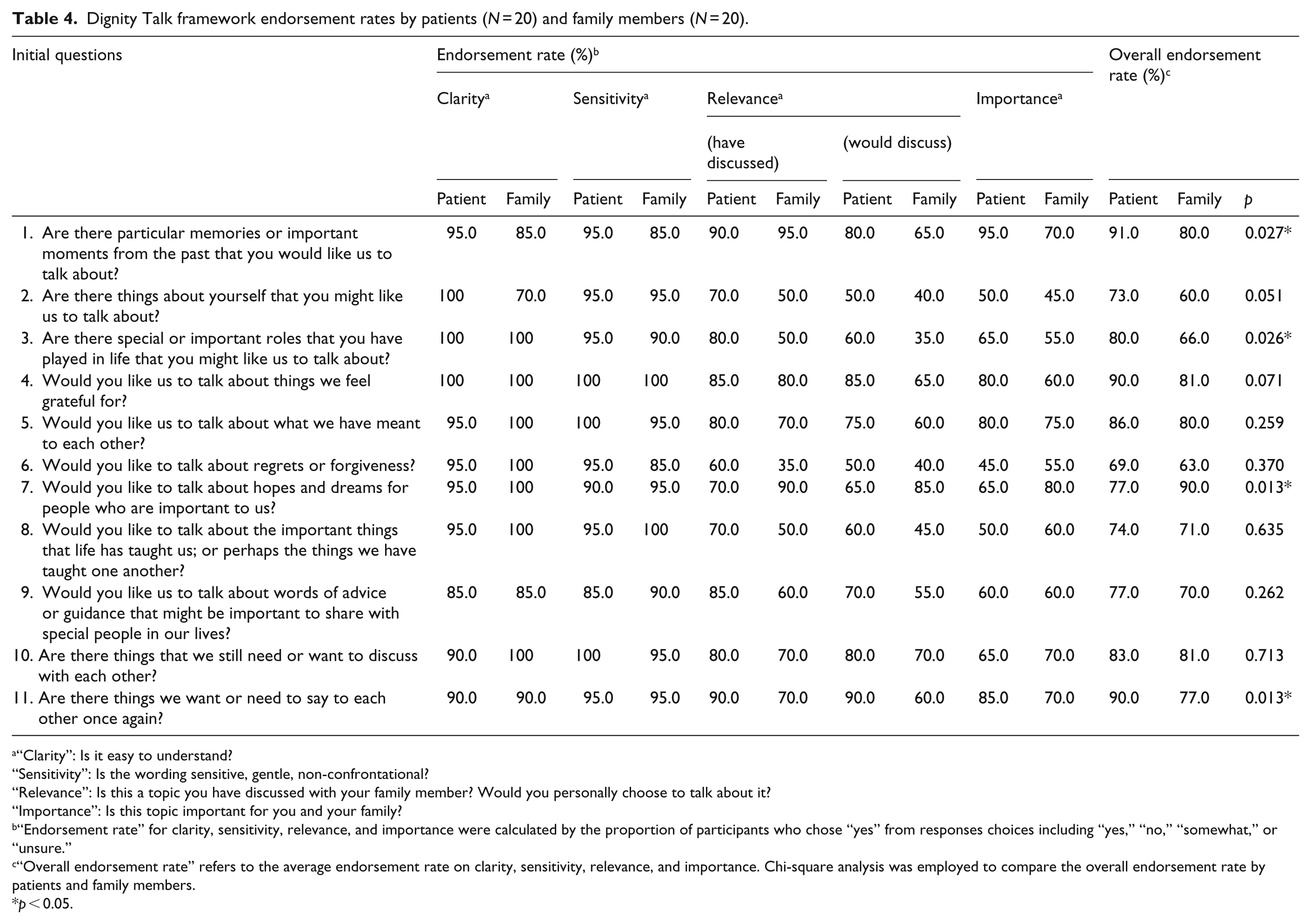
“Clarity”: Is it easy to understand?
“Sensitivity”: Is the wording sensitive, gentle, non-confrontational?
“Relevance”: Is this a topic you have discussed with your family member? Would you personally choose to talk about it?
“Importance”: Is this topic important for you and your family?
“Endorsement rate” for clarity, sensitivity, relevance, and importance were calculated by the proportion of participants who chose “yes” from responses choices including “yes,” “no,” “somewhat,” or “unsure.”
“Overall endorsement rate” refers to the average endorsement rate on clarity, sensitivity, relevance, and importance. Chi-square analysis was employed to compare the overall endorsement rate by patients and family members.
p < 0.05.
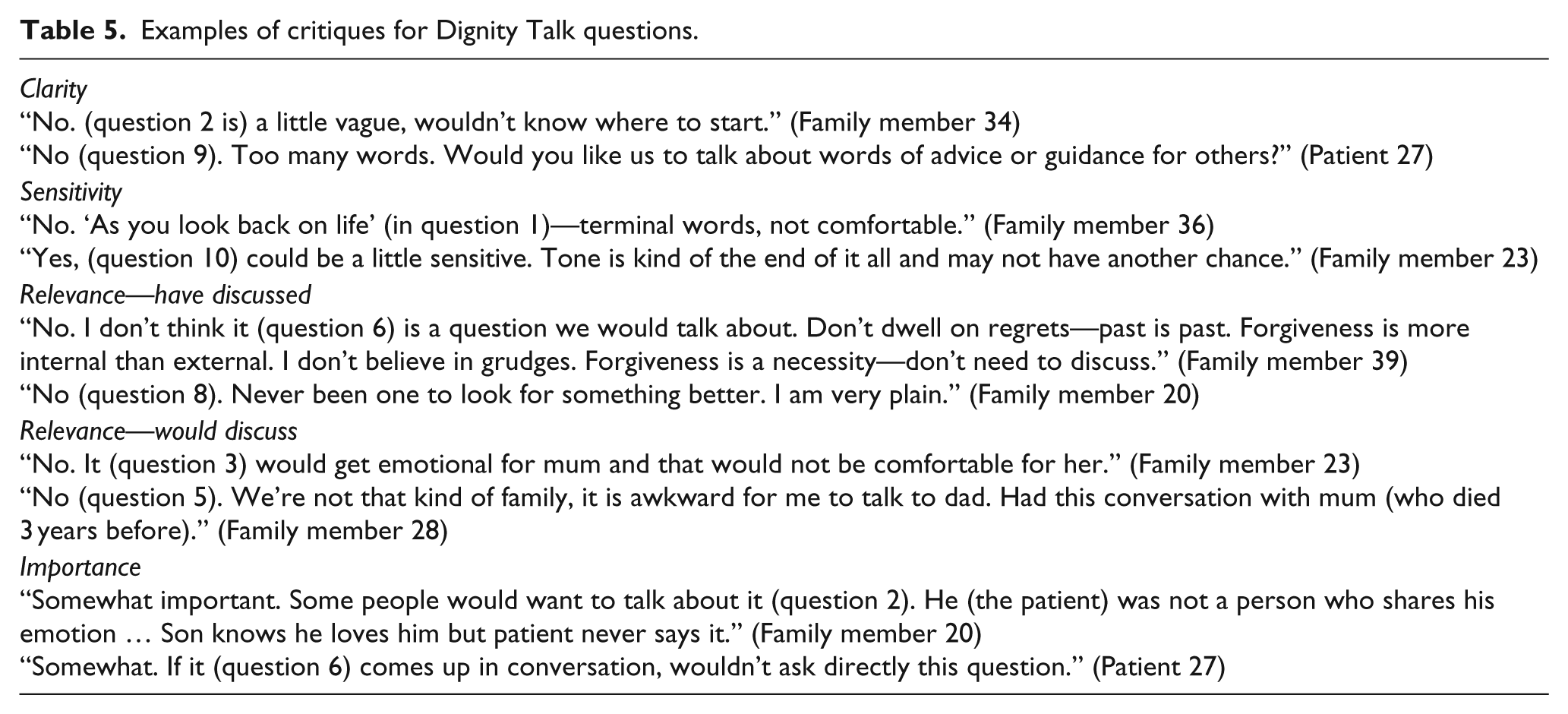
Higher overall endorsement was obtained from patients compared to family members for nearly all Dignity Talk questions. There was significantly higher endorsement among patients for question 1 regarding the sharing of memories (91.0% vs 80.0%; p = 0.027); question 3 pertaining to important roles (80.0% vs 66.0%; p = 0.026); and question 11, asking if there are still things that need to be said (90.0% vs 77.0%; p = 0.013). Family members were significantly more likely than patients to endorse question 7, inquiring about hopes and dreams for important people (90.0% vs 77.0%; p = .013). Example reasons for non-endorsement are shown in Table 5.
Examples of critiques for Dignity Talk questions.
Suggestions for improvements
Participants were asked to provide suggestions for ways to improve the Dignity Talk question framework. Qualitative analysis identified four main themes.
Appraisal of the Dignity Talk guidelines
Patients, family members, and HCPs raised three points that need to be addressed in the Dignity Talk guidelines: Explanation of the title “Dignity Talk”: A brief explanation regarding what Dignity Talk is. i.e. “Dignity Talk is a new intervention/approach developed by our research group … this will help to tie things together.” (HCP focus group 6) Flexibility in use: In guidelines may be helpful to highlight you can talk about as many or as few questions as you like. [HCP focus group 4]; “In terms of guidelines, I like the statement regarding ‘either of you may decide to stop a conversation.’” (Patient 42) Role of the patient/family: Who is taking lead, patient or family? Have to make it abundantly clear that these questions are for everybody to dialogue. (HCP focus group 6)
Conciseness and clarity
To ensure the conciseness and clarity of the Dignity Talk questions, HCPs suggested keeping questions simple and using as few phrases as possible. In addition, some patients and family members proposed that certain questions were too general or broad to respond to, while others pointed out it is good to be broad so that people can respond, but avoid things they don’t want to talk about: A general concern, keep it simple, less phrases are better. (HCP focus group 2) The question (question 2) is big enough to be vague so people could avoid some things. (Patient 11)
Wording and tone
HCPs stated that the Dignity Talk framework was worded in a respectful tone. The Dignity Talk questions were regarded as straightforward in opening up delicate and personal conversations, enabling patients and families to respond according to their own needs and preferences. The importance of using “plain language” was highlighted, so that it could be understood by participants of all educational levels: Would someone with less education understand the question? It is important to have guidelines in plain language. (HCP focus group 1) (Question 2) wording very good. Doesn’t infer that holding secrets but possibly invokes a response. (Family member 31)
Style and presentation of questions
Considering that Dignity Talk is designed to elicit patient–family conversations, participants felt that questions need to be presented less like an interview and more like an invitation to a conversation. HCPs said that numbering questions makes the questions framework seem rigid and implies they need to be gone through in order. They encouraged sensitivity to arranging questions based on how emotionally evocative they might be and starting with less evocative questions as a way of moving gently into a conversation: Numbering questions makes it seem hierarchical—i.e. some questions are more important or have to go through the list…Perhaps thematic or groupings. (HCP focus group 2) Questions 1, 8, 9 seen as easiest for people to answer—therefore maybe have them earlier in list. Don’t start with regrets/forgiveness. (HCP focus group 5) Questions would need to be presented with great care. (Family member 30)
Perceived benefits of Dignity Talk
Participants felt that Dignity Talk could serve as a conversation prompt, enhance family connections and relationships, enhance personal value and dignity, promote effective interaction, and help attend to unfinished business.
Conversation prompt
Participants stated that Dignity Talk could offer the patient and family member a chance to talk about important things, especially for those more reticent to broach some of these issues: Every single question was amazing. I would not be able to talk about these without the prompts of the question sheet. (HCP focus group 3) Talking points are helpful and I suspect most people do not talk about these things, therefore they need something like this. (Family member 30)
Enhancing family connection and relationship
Patients and family members stated that Dignity Talk could enhance family relationships by offering a chance to share stories and feelings, learn from each other, or just be together: Very very important because you hear so many occasions where families haven’t spoken really for years and this may or may not bring them together. (Patient 36) It brings family members together and brings common memories for future. (Family member 9)
Enhancing personal value and dignity
Several patients stated that Dignity Talk could offer an opportunity to pass on their memories, life learning, hopes, and advice to their family members. Family members felt that Dignity Talk could help create memories that family members can carry into bereavement: You have walked yourself and had experiences as to what have worked best [in your life]. My children want to know about my life, particularly important if young people who don’t know which way they are going in life. (Patient 2) This is important because the person is gone but their (words of advice or guidance) keep memories alive in our heart. (Family member 3)
Promoting effective interaction
Patients and families felt Dignity Talk could promote emotional interactions. They saw value in the opportunity to show appreciation to their loved ones: It is important to know how you feel about them (family). For example, my macho brother—kind and caring, I tell him how much he means to me even if it makes him uncomfortable. (Patient 36) … continue to tell each other how much we care for each other and need each other and appreciate each other. (Family member 19)
Attending to unfinished business
Patients and family members felt Dignity Talk could help them attend to unfinished business and hence die with no regrets. Similarly, HCPs felt that Dignity Talk offered patients and families an opportunity for introspection: When you know the end is inevitable like in my case, nothing is worse than someone passes away and things not clear—i.e. legal. Prepare ones that are left. (Patient 25) It (question 6) does help to have permission and allows some soul searching. (HCP focus group 5)
Perceived concerns and challenges of Dignity Talk
Concerns and challenges included applicability of some of Dignity Talk questions, patient and/or family preparation for Dignity Talk, and the potential for questions to elicit information that might be difficult to deal with emotionally.
Applicability of Dignity Talk
While the Dignity Talk questions were considered important and meaningful, not all questions are applicable to every patient or family, depending on various factors such as individual or relational characteristics, culture, or health status: Men in my culture are prideful, it is a matriarchal background. Hard for us (son and father) to share (memories). (Family member 28) Heath characteristics can impact as well—have a stroke may impact memory of events. (Patient 25)
Preparation for Dignity Talk
Although Dignity Talk is designed to be self-administered, HCPs suggested that participants will need to be well prepared prior to implementation, in terms of having a clear understanding of the intervention and how to start these conversations: Before family (and patient)gets the questions it will be important to prepare them and talk with them … They need time to “chew on it.” (HCP focus group 3) A lot of people need help opening the door … Maybe the HCP can offer support for this framework. (Family member 30)
Difficult situations
Participants noted that some questions, in some instances, could be emotional or elicit potentially harmful or difficult information. HCPs felt it was very important that participants be given complete latitude to respond only to questions that were meaningful and within their emotional capacity to engage in: I might hesitate to ask (question 10) because of what might be brought up e.g. negative. (Family member 34) … potential to be comforting for both patient and family. However, there may be potentially hurtful things that come out—may not be time for resolution—important to be mindful of this and offer safety. (HCP focus group 1)
Revision of Dignity Talk guidelines and questions
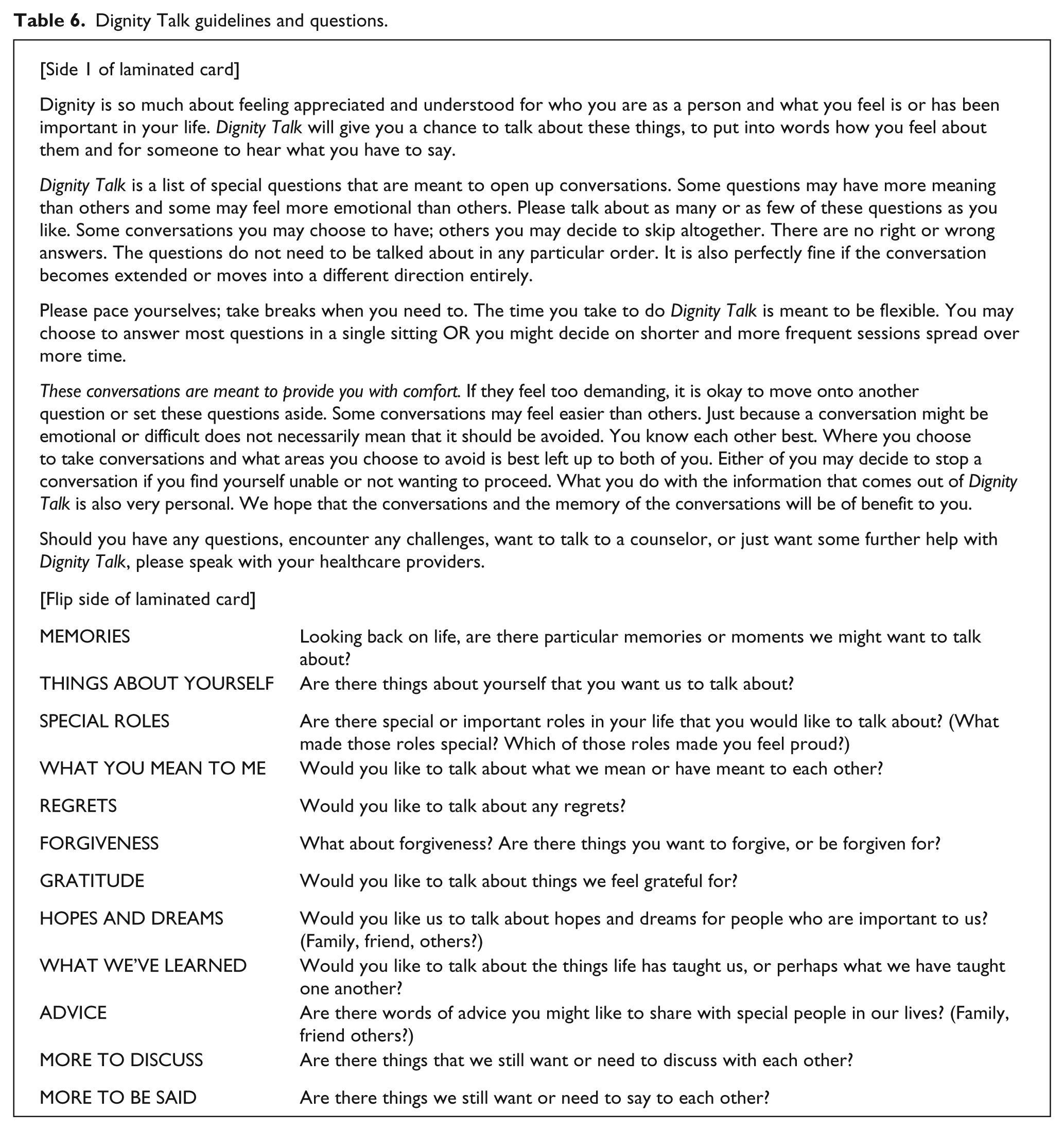
Dignity Talk was revised based on participant feedback. Revisions included a statement about the definition of dignity; an explanation that Dignity Talk is a list of questions that is intended to open up meaningful conversations between patients and their families; and a caution that some questions might be emotionally evocative. Guidelines were also revised to reflect that participants can choose to talk about as many or as few questions as they like; and that they can deviate from the question framework to talk about anything else the conversation might lead to. A statement was added instructing participants to pace themselves and take breaks as needed. Details about the time frame for completing Dignity Talk were included, stating that Dignity Talk is meant to be flexible, and can be returned to when the time feels right. To optimize emotional comfort and safety, the guidelines explicitly state that either party can decide to set aside or defer questions. Finally, the guidelines were revised to include contact information for supportive counseling following Dignity Talk, should participants feel the need to pursue this.
The original Dignity Talk question list was revised in response to feedback, rewording questions to make them less prescriptive. The final Dignity Talk communication prompt includes 12 questions. All original questions were retained, with question 6 regarding regrets and forgiveness being divided into two distinct questions: one about regrets and the other about forgiveness. Even though question 6 was endorsed by fewer than 70.0% of patients and family members, it was retained based on the feedback from HCPs such as “Question 6 is a powerful and important question and should be included, cannot have an intimate conversation if this is not on the table” (HCP focus group 4). Dignity Talk questions were re-written in plain language to assure clarity and broad accessibility. Instead of numbering, each question was labeled with a theme so that the participant can easily scan the topics and pursue those that fit best with them. While there had originally been a separate version of Dignity Talk for patients, and another for families, the feedback and refinement saw these combined into one final version of Dignity Talk suitable for both (see Table 6).
Dignity Talk guidelines and questions.
Discussion
Main findings of the study
Dignity Talk was generally well endorsed by participants, who felt it would be a valuable means of promoting family conversations, enhancing family connections and relationships, bolstering sense of value and dignity, promoting effective interaction, and attending to unfinished business. The vast majority of patients and families reported that the Dignity Talk questions were clearly stated and sensitively worded. While the rate of endorsement on relevance and importance varied across individual questions, all but one question was more highly endorsed by patients versus family members. Patients nearing death may see Dignity Talk as a final opportunity to address issues that matter most to them, speak to things they would want remembered, and complete unfinished businesses, thus achieving greater peace of mind. 27 The one exception, question 7 regarding hopes and dreams for people was more highly endorsed by family members than patients. This might reflect family members’ urge to seek guidance and input regarding the lives of people who are soon to be bereft. The question regarding forgiveness and regrets received the least endorsement, from patients and families alike, while HCPs in particular deemed it important and necessary for inclusion. That impression is supported by evidence that expression of forgiveness and regrets can improve emotional status, decrease depression and anger, improve hope and facilitate completion of life tasks for terminally ill patients, and ease bereavement for family members.30 –32
The fact that the majority of questions had already been broached by 70% or more of either patients or family members suggests that these questions are salient for patients and families anticipating end of life. The broad nature of these questions could see patients and families wanting to revisit these conversations at different points in time. On the other hand, it could be the case that a smaller minority of patients and families will use Dignity Talk to broach issues they are otherwise avoiding or find too difficult to initiate without a prompt. Enhanced communication is foundational to relationships anchored in mutual support and understanding, hence buffering emotional distress for patients and families alike. 33 Family caregivers seek existential meaning in their relationships with dying loved ones. 34 Dignity Talk offers a strategy to help them support their family member in the enactment of their caregiver role and achieve meaningful involvement. 35
Strengths and limitations of the study
Strengths of the study include Dignity Talk being developed and modified based on both qualitative and quantitative data. It is one of very few psychosocial interventions targeting patient/family dyads 36 and is meant to be self-administered by patients and families. Limitations include a relatively small sample size, although rich qualitative data were collected. Participants were recruited from two mid-western Canadian institutions; the attitudes of participants may not be representative of attitudes toward conversations elicited by Dignity Talk in other settings or cultural contexts. Collecting dyads in palliative care research is challenging, particularly given that patients are very ill and family is often preoccupied by concerns and tasks related to supporting their loved ones.
What this study adds
This study developed the Dignity Talk question framework, designed to facilitate important conversations between terminally ill patients and their family members. To confirm its role in palliative care, a Phase II clinical trial of Dignity Talk will be needed, recruiting patients and family members to examine its feasibility, benefits, and perceived value.
Footnotes
Acknowledgements
We would like to thank the patients, family members, and healthcare providers for their time and thoughtful insights. We would also like to thank our research nurse, Katherine Cullihall, for her assistance in participant recruitment and data collection. H.M.C. contributed to the conceptualization and design of the study. Q.G. and H.M.C. contributed to data analysis and interpretation of data with main contributions from Q.G. Q.G. drafted the manuscript, and H.M.C., S.M., G.T., and T.H. revised it critically for important intellectual content. All authors approved the final manuscript and have participated sufficiently in the work to take public responsibility for appropriate portions of the content. Registration: ClinicalTrials.gov Identifier: NCT01883375; data of registration: 11 February 2013.
Data management and sharing
Our study data are securely stored under lock and key in the Research Institute of Hematology and Oncology, CancerCare Manitoba. We do not have the permission from either the University of Manitoba Health Research Ethics Board or consented research participants to release or share our data, thus we cannot make it available in the public domain.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research Operating Grant (grant number MOP-123473).
Research ethics and patient consent
This study was approved by the University of Manitoba Health Research Ethics Board (H2013:024) and all participants provided informed consent.