
Abstract
Background:
Prospectively tracking errors can improve patient safety but little is known about how to successfully implement error reporting in a home-based palliative care context.
Aim:
Explore the feasibility of implementing an error reporting system in a home-based palliative care program in Toronto, Canada, and describe the possible factors that may influence uptake.
Design:
A convergent mixed-methods approach was used. Participants prospectively documented errors using a novel reporting tool and completed monthly surveys. Following the reporting period, we conducted a semi-structured interview exploring participants’ experiences and perceived factors influencing reporting behaviors. Error, survey, and interview data were analyzed separately, then integrated for comparison.
Setting and participants:
Thirteen palliative care physicians from a single home-based palliative care organization in Toronto, Canada anonymously reported errors between October 2021 and September 2022. Of these, six participated in the exit interview.
Results:
Participants reported 195 errors; one-third (n = 65) involved internal staff or systems. Three themes describe the factors impacting the likelihood of reporting errors: (1) High levels of cognitive burden decreases the likelihood of error reporting; (2) Framing errors as opportunities to learn rather than reason for punishment improves likelihood of error reporting; (3) Knowing that error data will improve patient safety motivates individuals to report errors.
Conclusions:
Physicians are amenable to error reporting activities so long as data is used to improve patient safety. The collaborative nature of care in a home-based palliative care context may present unique challenges to translating error reporting to improved patient safety.
Medical errors threaten patient safety, and patients receiving palliative care at home may be particularly vulnerable to experiencing errors
Prospective reporting to identify common errors and understand their root causes is an integral part of error prevention and reduction
Although common in hospitals and medical clinics, little is known whether the factors that influence the uptake of error reporting tools in these settings translate to a home-based palliative care context
Collecting and comparing quantitative error data and qualitative interview data allowed us to contrast actual error reporting practices with participant descriptions of their experiences and the perceived factors to influence error reporting behavior
Our quantitative findings suggest that home-based palliative care physicians are comfortable reporting errors and tend to document ones that are significant, preventable, involve external care partners, and occur between physician visits
Our qualitative data indicate that physicians are motivated to report errors when mistakes are framed as learning opportunities that will be used to improve patient safety
Interpreted together, we observe that the motivation of using error data for patient safety improvements conflicts with the inability to address errors that occur external to the organization, thus bringing into question the sustainability of error reporting in this setting
The collaborative nature of palliative care at home makes the translation of error data to patient safety interventions difficult and may highlight similar challenges in other contexts where inter-organizational or interprofessional collaboration is required for patient care
Error documentation and evaluation efforts should be integrated across care partners to optimize the effectiveness of patient safety interventions
Introduction
Medical errors—“the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim” 1 —are important topics of discussion in medicine because of their contribution to morbidity, mortality, patient distress, and health care costs.1 –3 Palliative care patients may be particularly vulnerable to experiencing errors due to the complex communication among interdisciplinary team members (including the patient and their caregivers), the use of high-risk medications such as opioids and benzodiazepines, polypharmacy, patient frailty, and patient cognitive decline.4 –8 Care in patients’ homes presents additional challenges to patient care that are unique from hospital settings: Decreased communication about roles and responsibilities in care can result from involvement of multiple care teams and different electronic records.9 –11 These gaps in information exchange in combination with uncontrolled home-environments and dependency on informal caregivers can have significant consequences when providing advanced medical treatments that are common in palliative care.6,10 –12 Home-care presents additional risks associated with lack of control over the home environment and dependency on informal caregivers to provide care. 12 Previous studies investigating errors in palliative care or home-care environments have focused on characterizing the types of errors that occur. These examinations of common errors (e.g. medication, communication, and symptom control)4,12 –14 and their root causes (e.g. poor communication)13,15 have described the potential and actual negative consequences on patient safety.13,16,17
Research from other disciplines suggests that prospectively tracking errors is an integral component of error prevention that may reduce the number and severity of errors. 18 Transparency when discussing errors can promote learning from others’ mistakes and enable institutions to improve patient safety.16,19 That is, identifying and examining recurring errors can highlight opportunities to intervene and prevent errors, thereby improving patient safety.
Several barriers and facilitators to error and incident reporting have been documented in family medicine and hospital-based settings: Time restrictions, forgetting to report, confusion about what to report, fear of litigation, perceived harm to professional or institutional image, personal shame, lack of proficiency in disclosure, and repetitive, infrequent, or low severity errors may reduce likelihood of reporting.20 –22 Conversely, clear benefit of reporting, anonymity, and feelings of guilt are all perceived to improve error reporting rates. 21 It is not known whether the factors identified in these settings translate to the uptake of and error reporting system within a home-based palliative care context.
Our study aims to fill this gap by evaluating the feasibility of implementing an error reporting system in a home-based palliative care context and describing the perceived factors that can modify the likelihood of uptake.
Methods
Study design
We used a convergent mixed methods approach to evaluate the feasibility of implementing an error reporting tool in a home-based palliative care context. Applying a mixed methods approach within a pragmatic paradigm, we could combine practical data collection methods and explore multiple perspectives of a singular phenomenon. 23 This combination and comparison of complimentary datasets affords a more complete understanding of the overall reporting experience than would have been possible with either data set alone. 23 Quantitative error and experience survey data provided insight about actual error reporting practices, and qualitative interviews allowed for a detailed exploration of participants’ experiences and the perceived barriers and incentives of error reporting. Quantitative and qualitative data were separately collected and analyzed, then integrated to provide insight about the error-reporting experience.
Setting
This study was conducted within Sinai Health’s Temmy Latner Centre for Palliative Care’s home-based palliative care program in Toronto, Ontario. Home-care physicians from the center collaborate with external care providers (e.g. care coordinators, nurses, personal support workers, pharmacists, and laboratory technicians) to provide interdisciplinary care. These care providers represent disparate organizations, each with their own guidelines, policies, and procedures.
Population and sample
Thirty-six physicians worked at the center (0.5–1.0 full-time equivalents) during the study period. All physicians providing home-based care, including those hired during the study period, were eligible to participate. Learners completing a rotation with the center were excluded from participation.
Recruitment
A member of the research team presented the study purpose and participation requirements at several center-wide meetings before individually inviting all physicians to participate by email. This study was approved by Sinai Health’s research ethics board (ID#21-0061-E. Approved August 25, 2021), and all participants provided written informed consent to participate.
The error reporting tool
The error reporting tool was designed by the research team with consultation from palliative care providers. The tool collected sociodemographic information about the patient involved in the error as well as information about the error (who was involved, the type of error, when it occurred, the severity, preventability, impact, and whether it was disclosed to the patient/caregiver). A full list of fields is included in Supplemental Appendix 1). No personal health information was collected. We housed the tool on the Qualtrics survey collection website 24 to allow for easy access across locations and devices. The link to the reporting tool was circulated to participants in an email and was flagged within the electronic medical record system.
Data collection
Quantitative
Participants anonymously self-reported errors between October 1, 2021 and September 30, 2022 following a 1-month test period, which allowed participants’ familiarization with the tool and management of technological or logistical concerns. Participants were instructed to document all errors that occurred, regardless of whose actions contributed to the error. Because our intention was to assess the feasibility of error reporting, we used a general definition of an error—“any deviation from perfection”—to capture the greatest breadth of error types. Aggregate error data from the previous month were presented to all staff at center-wide meetings along with reminders for the participants to continue to report. Participants completed monthly error-reporting experience surveys asking if and why any errors were not reported in the prior month, their level of comfort reporting errors, and for suggestions regarding the reporting process or tool (Supplemental Appendix 2). These surveys were terminated after 9 months of collection due to no new feedback and poor response rates.
All participant suggestions were reviewed upon receipt and iteratively integrated into the error reporting form or process if feasible. A list of changes can be found in Supplemental Appendix 3.
Qualitative
At the end of the error reporting phase, all participants were invited to participate in a semi-structured exit interview. Questions explored participants’ experiences over the past year, any perceived barriers and incentives, and general views on the utility of error reporting (Supplemental Appendix 4). All interviews were conducted virtually, audio recorded, and transcribed clean-verbatim for analysis.
Data analysis
Quantitative
We conducted descriptive analysis of the reported errors and the experience surveys. We reviewed “other” responses for the question “whose actions contributed to the error” and reclassified responses into existing or emergent categories as appropriate. Due to the large number of medication errors classified as “other,” we re-categorized all medication errors by timing: during (1) medication ordering (e.g. medication order forgotten, placed for the wrong patient, or sent to the wrong pharmacy), (2) order transmission (orders were not received by the pharmacy), (3) medication dispensing (e.g. medications were dispensed in the wrong amount, were delayed), and (4) medication administration (e.g. equipment failure, instructions were not followed).
Qualitative
We employed a Framework Analysis approach for interview analysis. This comparative form of thematic analysis utilizes summaries of each code to identify, describe, and interpret patterns across participants and generate themes within a phenomenon of interest. 25 Following an initial familiarization of the interviews, we used a modified version of Grol and Wensing’s categories for barriers and incentives to interventions in health care 26 to inform an a priori coding framework. We supplemented the original six categories (innovation, individual professional, patient, social context, organizational context, and economic and political context), with one additional category (implementation strategy) and sub-concepts informed by existing lterature 27 and group discussion. Using MaxQDA software, 28 AK, GK, and NP deductively coded all interviews, periodically meeting to compare coding, discuss conflicts, and add/refine codes as required.
Consistent with the Framework Analysis approach, we organized transcript quotes into a matrix (“Codes” by “Participants”), and generated summaries for each code. Using these code summaries, discussion and memos, the team developed themes that described the salient factors impacting likelihood of error reporting.
Data integration
Following the separate analysis of our quantitative and qualitative data, we merged our results by comparing findings to identify points of convergence, divergence, and expansion. Informed by our qualitative findings, we further categorized each error as occurring internally (to the center), externally, or both. This was done by reviewing individuals involved in the error and the error description when further clarification was required. The categorization algorithm used is presented in Supplemental Appendix 5. Utilizing a weaving narrative discussion approach, we report our quantitative findings together on a theme-by-theme basis within the qualitative data.
Results
General results
Thirteen palliative care physicians representing an equivalent of eight full-time equivalents participated in the study. Four participants completed fewer than 12 months of data collection due to joining or leaving the center during the study period (6, 7, 8, and 11 months, respectively). A total of 195 errors were reported during the reporting period, representing a monthly median of 16.5 errors (minimum = 9; maximum = 23). We received 28 error-reporting experience surveys. Descriptive frequencies for the errors are presented in Table 1 and Figure 1. Responses for the experience survey are presented in Table 2.
Descriptive frequencies of reported errors.
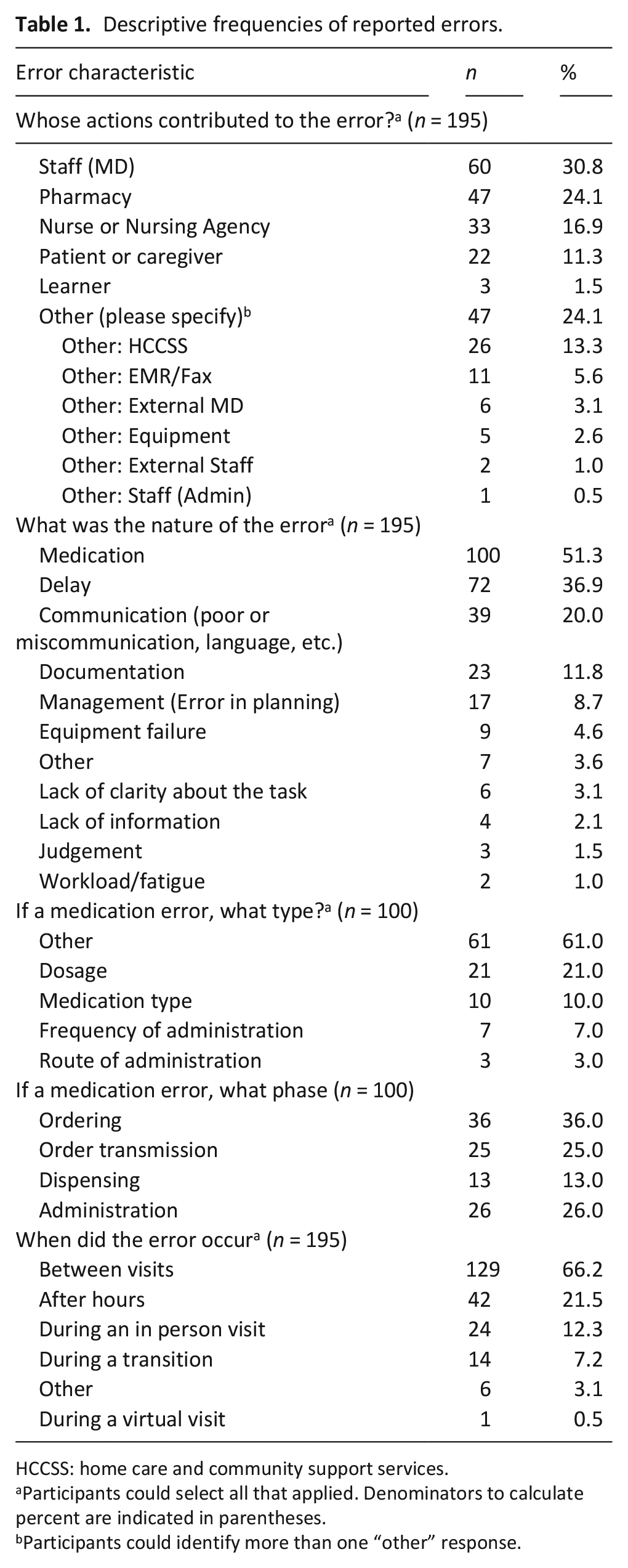
HCCSS: home care and community support services.
Participants could select all that applied. Denominators to calculate percent are indicated in parentheses.
Participants could identify more than one “other” response.
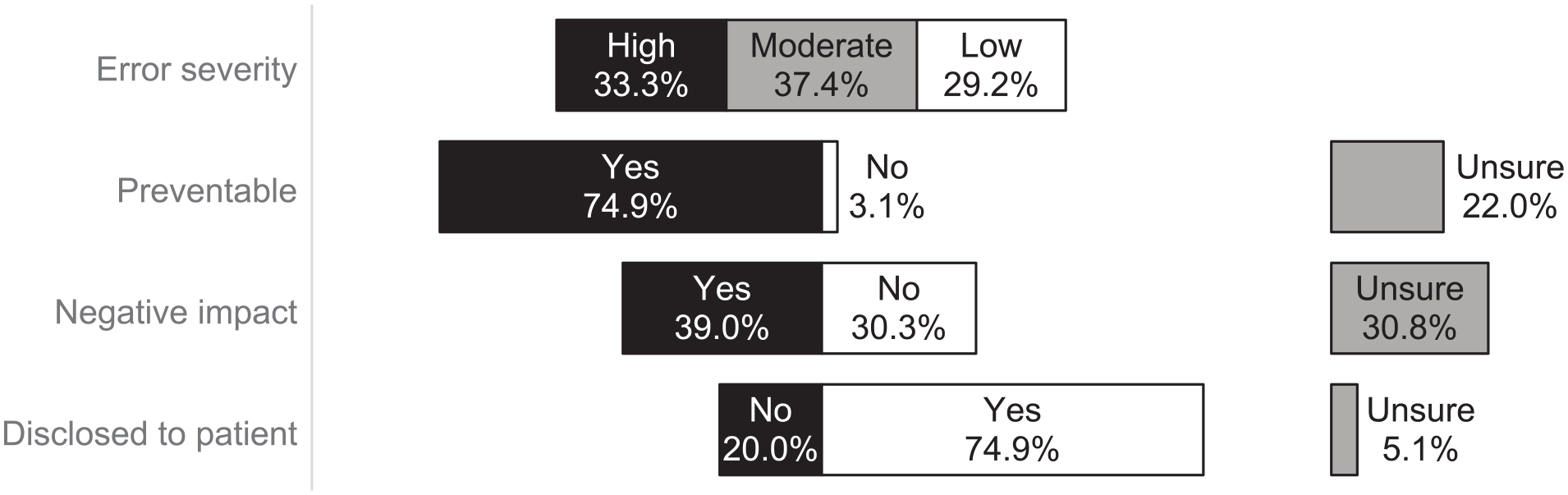
Error severity, preventability, impact, and disclosure.
Summary of experience survey responses.
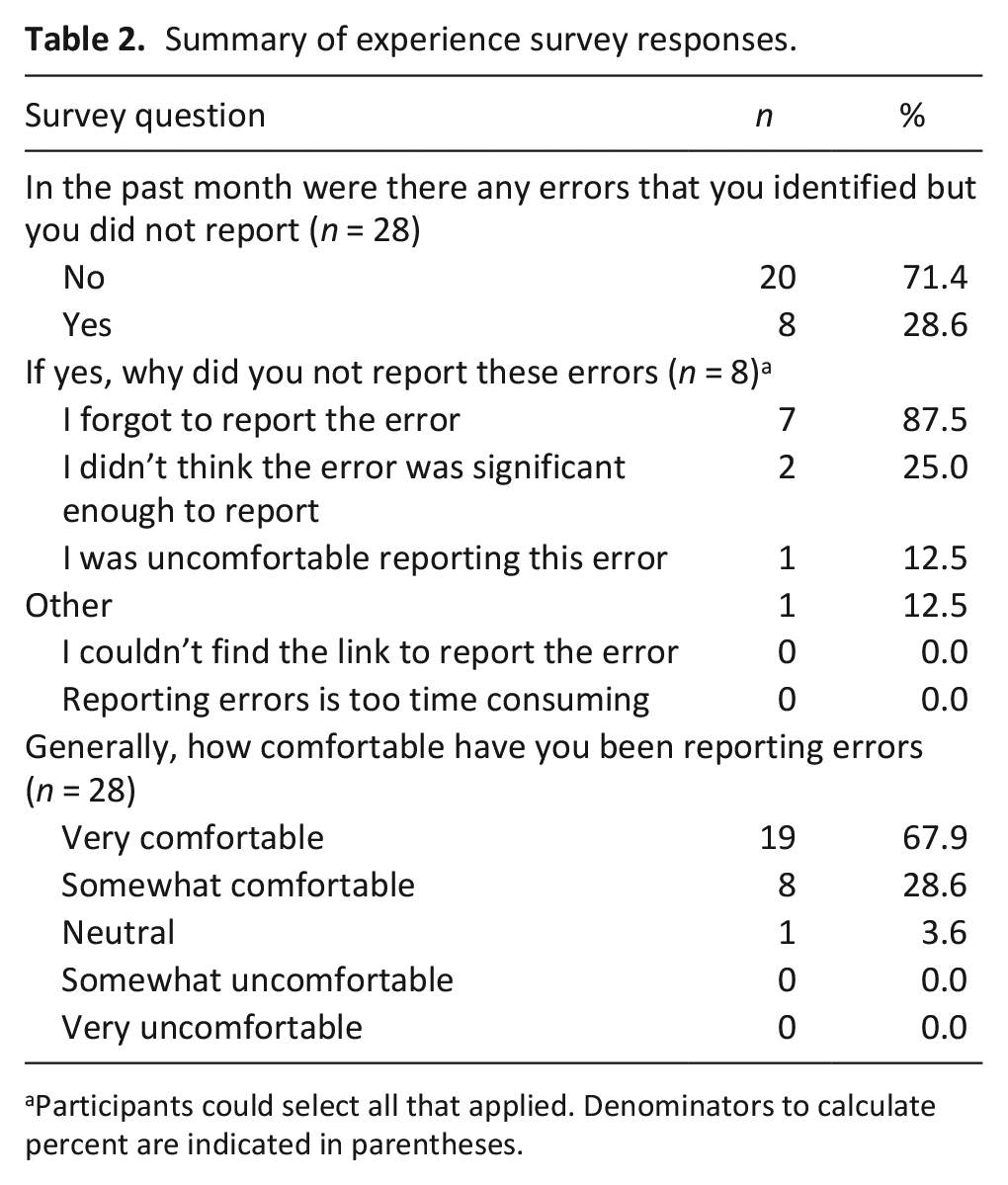
Participants could select all that applied. Denominators to calculate percent are indicated in parentheses.
Six individuals completed the exit-interview. We identified three themes that describe the factors impacting the likelihood of reporting errors and overall uptake of the error reporting system in a home-based palliative care setting: (1) High levels of cognitive burden decrease the likelihood of error reporting; (2) Framing errors as opportunities to learn rather than reason for punishment improves likelihood of error reporting; (3) Knowing that error data will improve patient safety motivates individuals to report errors.
High levels of cognitive burden decrease the likelihood of error reporting
Difficulty using the tool and lack of incorporation into participants’ usual workflow resulted in cognitive burden that reduced likelihood of error reporting. Participants identified several specific factors that were perceived to contribute to cognitive burden.
Our broad definition of an error (i.e. “any deviation from perfection”) required individuals to decide for themselves whether an event qualified as an error or not. While some found this broad definition liberating, most others found it difficult to decide, requiring thought and time. Participants suggested that standardizing or providing a clear definition of an error could improve uptake.
I like the idea of narrowing down to a specific type of error that we identify as being prevalent and then trying to hone in on that and capture that error. I think that would make capturing it a lot easier. (Participant 03)
On an individual level, participants indicated that competing priorities, such as managing large patient loads, often resulted in errors not being reported. In these instances, errors were one more thing to remember and reporting was often de-prioritized, delayed, and ultimately forgotten.
So it was one of those, things that you get busy and you’re like, ‘hey I’ll do it later’, and then that falls off your radar. (Participant 05)
This was exacerbated by participants needing to navigate away from the electronic medical record to access the tool. Deviating away from one’s routine workflow presented enough of a barrier to reduce the likelihood of reporting an error.
I think there were probably a lot of errors that I didn’t report, and it was probably because it wasn’t built into my workflow and it just didn’t occur to me. (Participant 06)
The effects of lack of integration into workflow are corroborated by error reporting survey results, which showed that participants did not report all errors that occurred, and that most un-reported errors resulted from forgetting to report the error (87.5%). In contrast, no participants selected “Reporting errors is too time consuming” as a reason for not reporting errors.
Individuals expressed becoming “desensitized” to errors that were routine or frequent, and that they were more likely to remember and report severe errors, even after a delay.
Unless it was really like a major significance it disappears from my memory very quickly. (Participant 01)
Our error and survey results support this, as 70.7% of errors were described as highly or moderately severe in nature, and of the eight surveys that indicated an unreported error, two selected “I didn’t think that the error was significant enough to report” as a reason. Conversely, errors with perceived negative impact were reported only slightly more often than errors with no negative impact (39.0% versus 30.3%, respectively).
Framing errors as opportunities to learn rather than reason for punishment improves likelihood of error reporting
When discussing their own beliefs, most participants viewed mistakes as normal and opportunities to learn. This aligned with perceptions of the error reporting activity, which was described as focused on learning and improvement and not punitive in nature. As a result, participants felt comfortable reporting their own and others’ errors because they were not afraid someone would “get in trouble.”
And there is nothing wrong with looking at errors if the aim is to fix and not punish, right? Then I’m all for it. (Participant 06)
This is reflected in the experience surveys: Nearly all (96.5%) of completed surveys showed participants as being “Very Comfortable” or “Somewhat Comfortable” reporting errors.
Some participants described feeling personally vulnerable when reporting their own errors, and discomfort or guilt when reporting others’ errors.
I just remember that time where I was reporting, so that felt like I made a mistake, it was my error and sort of thinking ‘oh, this feels weird, putting that out there into the public kind of space, even though I probably I think I explained and disclosed it to the patient, as I recall. But yeah, it still felt funny. (Participant 01)
Knowing that error data will improve patient safety motivates individuals to report errors
Seeing mistakes as opportunities to learn and improve was closely associated with the final theme. Most participants felt that in order to be a worthwhile activity, the information collected through error reporting should be used for improving patient care and safety.
I think being able to record what’s happening on the ground is always helpful. And just using it, using the data to advocate for improvement in our services. So, from like a quality improvement standpoint if there’s some errors that are consistent, you know, bringing those up in a meeting and being able to say, ‘hey, what do we think about this, how can we improve this?’ (Participant 04)
At an organizational level, participants expected that error data would be used to identify and address recurrent errors through quality improvement initiatives. Within a broader context, participants noted that the center collaborates with many external care partners and that identifying these errors presented both opportunities and limitations: On one hand, identifying external errors could be used to advocate for change at a system level, while on the other, errors involving external partners are outside the control of the center, making it more difficult to enact change.
I think the benefit is more. . . for the Centre or even beyond the Centre, right? Because a lot of the errors didn’t just occur within people in the Centre. It was it was in coordination with other groups. Where there’s 2 [Home and Community Care Support Services] organizations, there’s a number of nursing agencies, and that’s where it becomes so complicated. (Participant 06)
The error data provides some additional insights about how it can be used to improve patient safety. Although many errors were described as preventable (74.9%), the center’s physicians were involved in fewer than one-third (30.8%) of all errors reported. “Other” and pharmacy were the next commonly involved (24.1% of all errors, each). A closer inspection of errors involving “Other” individuals showed that the Home Care and Community Support Services were involved in 13.3% of all errors.
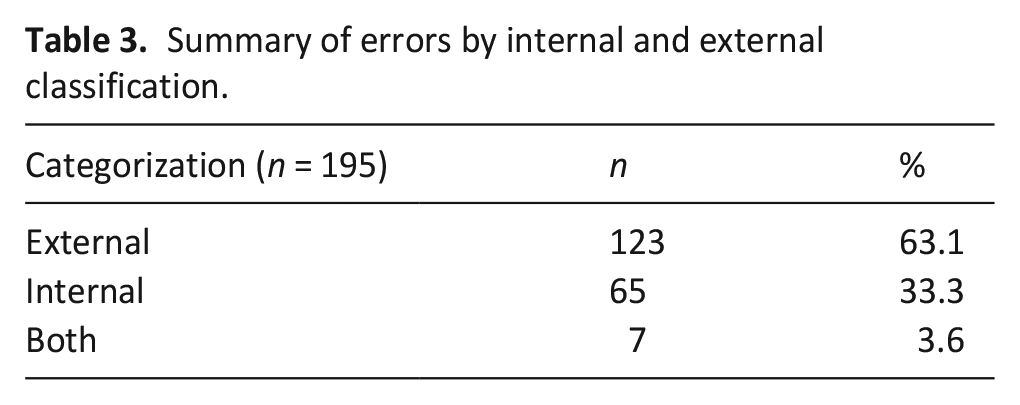
In our analysis of internally and externally driven errors (Table 3) we found that 33.3% of the reported errors involved an internal individual or system (physician, administrative staff, or medical record/fax systems), while 63.1% involved an external care partner or equipment and 3.6% involved both. Finally, 66.2% of errors occurred between visits (i.e. did not occur during an in-person or virtual visit made by the physician).
Summary of errors by internal and external classification.
Discussion
Main findings
Studies utilizing prospective error recording in medicine are rare29 –31 and to our knowledge, none exist in palliative care. This study examined the feasibility of implementing an error reporting system in a home-based palliative care program including physician experiences and perspectives about the factors that can help or hinder the uptake of such a system. Rates of error reporting and survey responses suggest that collecting error data is possible in this context and that physicians are generally amenable to error reporting. Although our rates are higher than in previous reports focused specifically on serious and medication errors in hospice and palliative care,13,32,33 we surmise that there was under-reporting of errors in this study given participant disclosure of un-reported errors.
What this study adds?
The barriers and incentives described by participants were closely aligned with error and survey data, providing insight into the conditions that need to be met for palliative care providers to engage in error reporting activities. Factors related to cognitive burden and organizational culture have been described in previous literature about error reporting uptake. 31 Confusion around what constituted an error due to our broad definition is consistent with previous literature, which has suggested there is little existing guidance or recommendations about errors in palliative care.5,21 Referring to existing literature, policies, and guidelines when defining errors, as well as their severity and preventability, may serve to minimize decision fatigue associated with reporting and can facilitate comparison of error data across institutions and regions. The poor integration into existing workflows noted by our participants has also been previously recognized as a barrier to error reporting uptake.20,34 Examining existing workflows and preferred technologies may help to integrate error reporting in a more seamless way. Finally, the beneficial effects of an organizational culture that prioritizes learning over punishment is consistent with existing literature, which highlights how climates of consequence20,34,35 and positive reporting cultures 34 that offer reassurance and support 36 can threaten or heighten error reporting, respectively.
Although several factors we identified resonate with existing literature, most previous studies were conducted in hospital and clinic-based settings. Our study focused on a home-based palliative care setting and highlights the unique considerations that need to be made within this context. Participants strongly felt that error data must be used to improve patient safety in order to justify reporting efforts.
Reporting errors is just one aspect of a comprehensive patient safety strategy, which should also include mechanisms for improvement and for disclosing errors to patients.22,37 –41
The majority of the errors in our sample were reported as preventable suggesting there may be opportunities for intervention. However, as most errors involved external care partners and occurred between physician visits, the feasibility of translating error reporting to improved patient safety may be limited. Previous investigations of medication errors, which constituted over 50% of errors reported in our study, suggest that good communication between healthcare providers, a unified electronic medical record system, and access to an onsite pharmacist can mitigate the occurrence of these errors.9,15,42,43 Implementing these strategies in our environment may not be feasible.
In our study, only 75% of errors were knowingly disclosed to patients. This rate could be increased through clear processes for and education around error disclosure. 38 Physicians may also not have disclosed others’ errors if they felt they did not have all the details, or were unsure about whose responsibility it was to disclose the error. Recommendations for disclosing others’ errors include colleague-to-colleagues communication to review error and to coordinate a disclosure plan, with oversight and support by the institution. 44 This can be challenging in the home-care setting if a patient’s other care providers are unknown, and oversight from multiple institutions is required.
Underpinning each of these areas is the need for effective information transfer between healthcare teams14,44 Within hospital settings, care providers are united by centralized processes for documenting and analyzing errors, identifying opportunities for intervention, and collaborating on solutions, thus maximizing the potential to improve patient safety within the institution. In contrast, incident reporting in the community is inconsistent and siloed across organizations with no processes that allow for sharing error data, thus making it difficult to collaborate on patient safety interventions between organizations. Patient care at home requires cooperative integration between many care providers; patient safety at home is no different. More research is needed to understand how to foster inter-organizational collaboration in error reporting and patient safety interventions.
Strengths and limitations
Prospectively collecting errors in this study may have the limited recall bias associated with asking participants to remember events, thereby generating a more representative account of the errors that occurred. Similarly, interviewing participants immediately following the reporting period may have facilitated more detailed and accurate descriptions of participant experiences, and the barriers and incentives described may be more closely rooted to actual reporting behaviors.
The anonymous error and survey data prevented us from exploring the agreement between actual and self-described reporting behaviors, and quantifying contributions to the data at the individual level. The limited number of self-identified un-reported errors impacts our ability to determine the degree of under-reporting. Majority of reported errors involved external partners, and it’s possible that, even with anonymous reporting, individuals were more likely to report others’ errors than their own. This study was conducted during COVID-19; staffing shortages, delays in care and modifications to practice may have influenced the nature and volume of errors that occurred and were reported.
The study principal investigator (MB) and co-investigator (RG) are both home-based palliative care providers who participated in the study. In order to preserve participant and error anonymity, neither had access to participant recruitment information or raw study data. Contributions to interpretation were based on aggregate quantitative data or emerging themes and isolated quotes.
Conclusions and implications
Although we found that it is feasible to implement an error reporting system in a home-based palliative care organization, the collaborative nature of care with external care partners may limit the effectiveness of translating error reporting to improved patient safety. Our findings are applicable to other areas where comprehensive patient care relies on inter-organizational collaboration. Future research should focus on implementing and evaluating inter-institutional error reporting systems in home-based contexts.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241288774 – Supplemental material for Feasibility of prospective error reporting in home palliative care: A mixed methods study
Supplemental material, sj-docx-1-pmj-10.1177_02692163241288774 for Feasibility of prospective error reporting in home palliative care: A mixed methods study by Allison M Kurahashi, Grace Kim, Natalie Parry, Vivian Hung, Bhadra Lokuge, Russell Goldman and Mark Bernstein in Palliative Medicine
Footnotes
Authors contributions
AK, NP, BL, RG, and MB participated in the conceptualization, design, and implementation of this study. AK, NP, GK, VH, and BL contributed to the collection and/or analysis of study data. AK, NP, GK, BL, RG, and MB participated in data interpretation. AK drafted the first draft of the manuscript and all authors critically reviewed and revised the manuscript and have approved it for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent
This study was approved by the Sinai Health Research Ethics Board (ID#21-0061-E. Approved August 25, 2021). All participants provided written informed consent.
Data sharing
Due to the small sample size and the risk of identifying individual participants, study data is not available. Questions regarding data can be directed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.