
Abstract
Background:
People with intellectual disabilities often present with unique challenges that make it more difficult to meet their palliative care needs.
Aim:
To define consensus norms for palliative care of people with intellectual disabilities in Europe.
Design:
Delphi study in four rounds: (1) a taskforce of 12 experts from seven European countries drafted the norms, based on available empirical knowledge and regional/national guidelines; (2) using an online survey, 34 experts from 18 European countries evaluated the draft norms, provided feedback and distributed the survey within their professional networks. Criteria for consensus were clearly defined; (3) modifications and recommendations were made by the taskforce; and (4) the European Association for Palliative Care reviewed and approved the final version.
Setting and participants:
Taskforce members: identified through international networking strategies. Expert panel: a purposive sample identified through taskforce members’ networks.
Results:
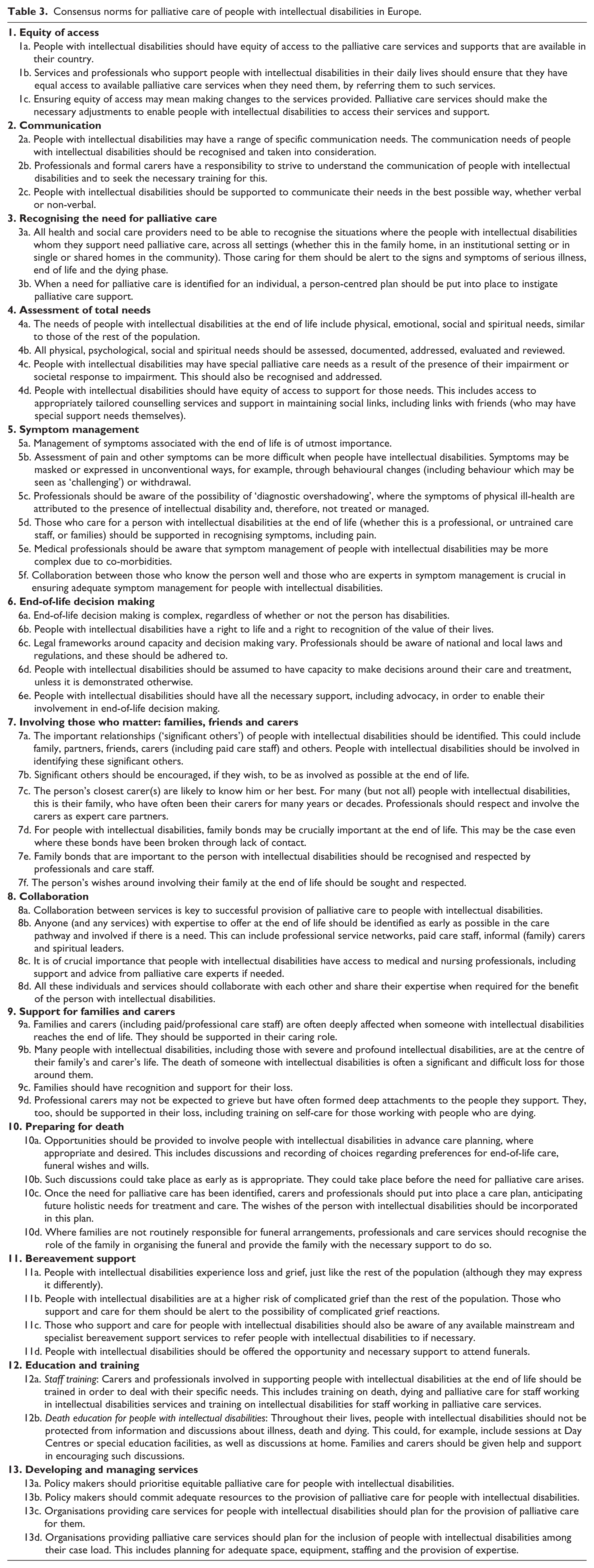
A total of 80 experts from 15 European countries evaluated 52 items within the following 13 norms: equity of access, communication, recognising the need for palliative care, assessment of total needs, symptom management, end-of-life decision making, involving those who matter, collaboration, support for family/carers, preparing for death, bereavement support, education/training and developing/managing services. None of the items scored less than 86% agreement, making a further round unnecessary. In light of respondents’ comments, several items were modified and one item was deleted.
Conclusion:
This White Paper presents the first guidance for clinical practice, policy and research related to palliative care for people with intellectual disabilities based on evidence and European consensus, setting a benchmark for changes in policy and practice.
Keywords
The UN Convention on the Rights of Persons with Disabilities states that access to health is important in enabling persons with disabilities to enjoy all human rights and fundamental freedoms. Despite this, people with intellectual disabilities lack equitable access to quality health care, including palliative care. This is compounded by a lack of population data about people with intellectual disabilities, making them a hard-to-reach group with hidden needs.
Palliative care provision is more complex for people with intellectual disabilities, due to disadvantaging issues and circumstances including difficulties with cognition, understanding and communication, complexities in decision-making processes, high levels of co-morbidities and mental health issues, and complex social circumstances.
There are few regional/national guidelines on meeting the palliative care needs of people with intellectual disabilities and no European guidelines.
The study shows that while many of the palliative care needs of people with intellectual disabilities are no different from those of the general population, focused attention and guidance are needed to ensure that palliative care services know how to adjust their services in order to make them accessible to people with intellectual disabilities.
The White Paper is the first document to provide internationally relevant guidance for palliative care of people with intellectual disabilities.
This study demonstrates that it is possible to reach full European consensus on what quality palliative care for people with intellectual disabilities looks like.
Palliative care services should actively reach out to find the population of people with intellectual disabilities within their catchment areas.
Available expertise is scarce and often isolated; therefore, there needs to be an ongoing exchange of experiences and expertise on local, national and international levels, both within and across professional specialties.
Further research should include investigations of the current state of affairs around palliative care provision for people with intellectual disabilities (including comparisons with the general population), the challenges in meeting the consensus norms across Europe, issues around end-of-life decision making for people with intellectual disabilities across Europe and development of common outcome measures.
Introduction
An estimated 1%–3% of the population have intellectual disabilities, 1 between 5 million and 15 million citizens of the European Union. 2 It is difficult to provide an overview of the scale of the issue due to a lack of explicit data on the prevalence of intellectual disability; the lack of standardisation between countries of terms and definitions; 3 and the different criteria, methods and age groups used in surveys.
‘Intellectual disability’ covers a wide range of abilities and disabilities, skills and limitations, ranging from mild to severe and profound. Despite varying definitions and inclusion criteria, there is international consensus that intellectual disability is present when the following three criteria are present: (1) a significantly reduced ability to understand new or complex information and to learn and apply new skills (impaired intelligence); (2) a significantly reduced ability to cope independently, expressed in conceptual, social and practical adaptive skills (impaired adaptive functioning); and (3) early onset (before adulthood), with a lasting effect on development.4,5
People with intellectual disabilities have increasing longevity, and many are now living into old age, 6 with an associated increased need for palliative care provision. However, there is growing concern that many people with intellectual disabilities do not have equitable access to palliative care and are seldom referred to specialist palliative care services.7–11 There are further concerns about the quality of palliative care they receive.12,13 This is part of a now well-established evidence base about the substantial health inequalities experienced by people with intellectual disabilities, leading to poorer outcomes that are often avoidable.14–17 This is noteworthy considering that palliative care has been recognised as an international human right18–20 and disability identified as an issue in need of global attention. 21 The United Nations 22 Convention on the Rights of Persons with Disabilities (which includes those with intellectual impairments) recognises that people’s impairments interact with attitudinal and environmental barriers, which may hinder full and effective participation in society on an equal basis with others.
There is a small but steadily growing body of research around the palliative care needs of people with intellectual disabilities. 23 A consistent finding is the importance of collaboration, in particular between palliative care and intellectual disability services, in ensuring that people with intellectual disabilities have the opportunity to live and die well.10,12,24–28 Specific guidance is needed to enable services and support offered to people with intellectual disabilities at the end of life to be adjusted to meet their individual and special needs.
The needs of people with intellectual disabilities towards the end of their lives are similar to those of the general population, but they often have additional and associated unique issues which can make it more difficult to meet those needs. This includes, for example, communication difficulties affecting all aspects of palliative care provision, including the assessment and treatment of pain and other symptoms;24,29 limitations in comprehension; difficulties around insight into the illness, the treatment and its consequences;30,31 issues around mental capacity and participation in decision making; high levels of co-morbidities and polypharmacy;13,32 and complexities in social circumstances, with limited social networks and high levels of reliance on elderly parents or care staff.33,34
It is against this backdrop of challenges and inequalities that the European Association for Palliative Care (EAPC) convened a Taskforce on Intellectual Disabilities in 2012, with the aim to develop consensus norms for best practice. In line with the EAPC, we define ‘Europe’ as the 53 countries within the World Health Organization (WHO) European Region. 18
There are challenges in describing norms that are relevant, acceptable and achievable across Europe, as there are huge variations in the provision of both palliative care services and intellectual disability services. Very little is known about the existing palliative care provision for people with intellectual disabilities across Europe, but anecdotal evidence gathered through this project suggests huge variations, ranging from non-existent to pockets of high expertise. However, the norms described in this official EAPC position paper present a European-wide consensus on quality goals that have to be aimed for when providing palliative care to people with intellectual disabilities. 35 As a result, they provide guidance on what good practice looks like, regardless of social and geographical setting or national and cultural differences. Additionally, this paper sets out recommendations and establishes a research agenda.
Methods
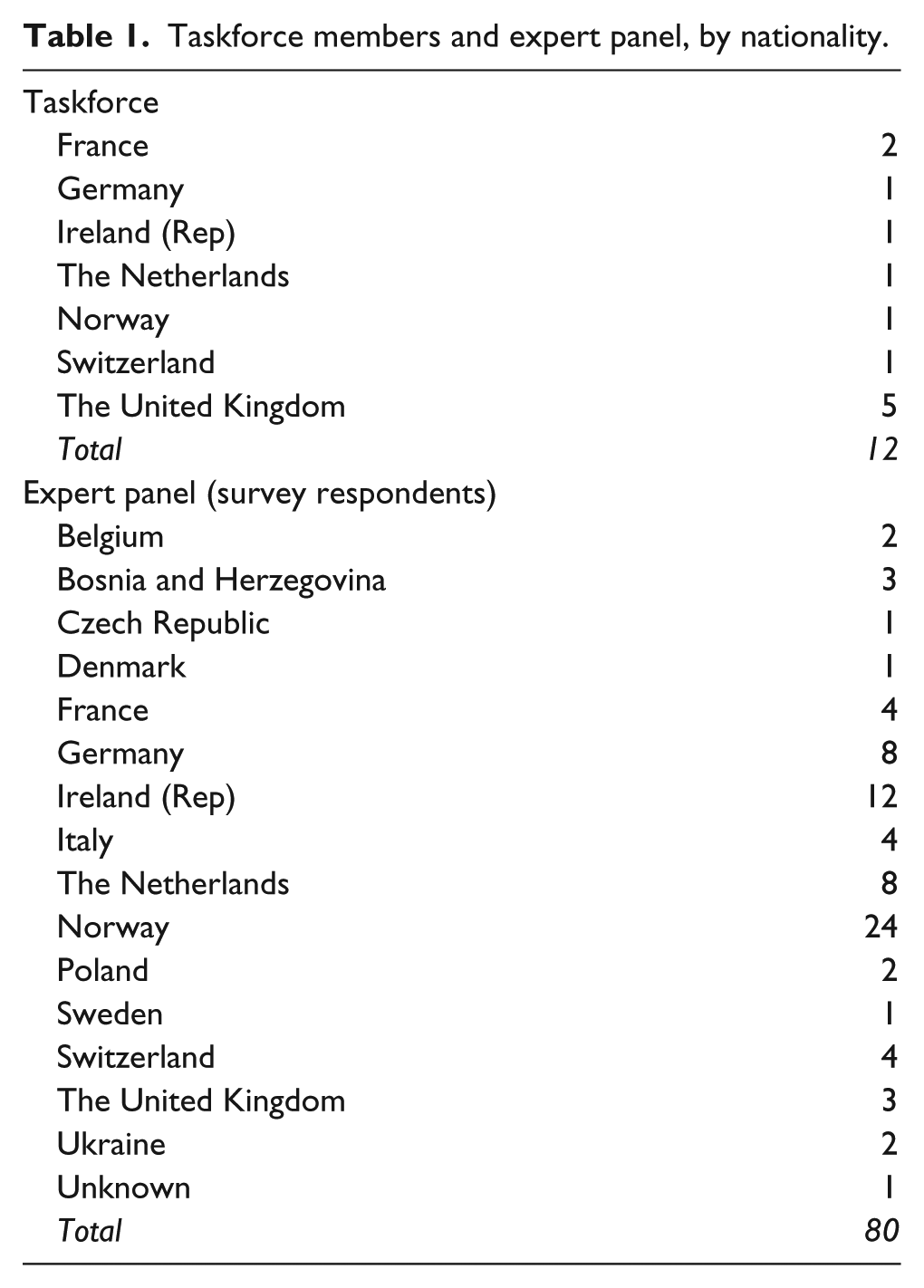
The taskforce consisted of 12 known experts in the field of palliative care for people with intellectual disabilities, comprising expertise in medicine, nursing and social work; expertise in clinical practice, education and academic research; and representing seven European countries (see Table 1). They were identified through national and international networking, such as contacting published authors and using contacts made through (inter)national conferences as well as through established palliative care and intellectual disability networks; this is a highly specialised field where most taskforce members were already aware of each other’s work.
Taskforce members and expert panel, by nationality.
The study involved generating draft norms and building systematic consensus through the use of Delphi methods in four rounds. This method uses virtual questionnaires to obtain the ideas and attitudes of people without the need for a meeting and is, therefore, ideally suited for gaining the views of a large number of geographically diverse experts. Respondents are asked to rank their level of agreement with a number of statements. If there is a substantial amount of disagreement, a further cycle of feedback may ensue. Anonymised, controlled feedback about previous rounds (including statistical group results) is given to encourage experts to review their opinion in the light of other experts’ responses. 36
The protocol was approved by the EAPC Board of Directors. As this was a consultation study, using clinicians and research professionals to comment on identified guidelines for good practice, ethical approval of the protocol was not required.
Round 1: drafting norms by a core group of experts
The first round was qualitative and unstructured. A sub-group of five taskforce members met several times to discuss and develop draft norms. A number of documents were studied and used as a starting point, including the EAPC White Paper on standards and norms for hospice and palliative care in Europe 35 and a range of regional and national guidelines for the provision of palliative care for people with intellectual disabilities.11,37 Taskforce members contributed their expert knowledge of research and practice that included involvement of people with intellectual disabilities, carers and staff. Within each norm, a number of statements were set out. The first draft of the norms was sent electronically to all taskforce members and, following two rounds of comments and amendments, agreed.
Round 2: evaluation of draft norms by an expert panel, using an online survey
The resulting statements within the draft norms were incorporated in an electronic survey (Monkey Lime Survey version 1.86, an online survey software tool) and piloted within the taskforce. For each statement, respondents were asked, ‘How much do you agree that the following statements should be part of the norms?’ They could indicate their level of agreement using the following Likert scale: ‘agree totally’, ‘agree a little’, ‘disagree a little’, ‘disagree totally’ and ‘not sure/don’t know’. They were also invited to provide additional feedback on each item in a free text box. The link to the survey was sent to a ‘group of experts’ across Europe, consisting of 34 professionals in 18 countries who had expertise in the field of palliative care, the field of intellectual disability or both. They were identified through the networks of the taskforce members and purposively invited to take part. The group of experts was asked to return the completed survey themselves and to email the survey link to expert colleagues.
Full consensus was defined as a median of ‘agree totally’ and ⩾80% agreement (i.e. the number of respondents indicating either ‘agree totally’ or ‘agree a little’); this is in line with similar EAPC European Delphi surveys. 38
Round 3: modifications, decisions and recommendations by the taskforce
All survey response scores, including all feedback comments, were collated and distributed anonymously among the Taskforce, highlighting in particular any ‘disagree’ responses. These were carefully considered, leading to several items being modified. The modifications were accepted where at least 10 of the 12 expert taskforce members agreed. Explanatory text, including background and justification, was written for each norm to form part of the White Paper and agreed following several rounds of feedback from the taskforce members.
Round 4: review and acceptance by the EAPC
The full set of norms and the explanatory text was submitted to the EAPC Board of Directors, reviewed and approved in April 2015.
Results
Round 1
Much of the early discussions centred around the ways in which norms for people with intellectual disabilities differed from those for the general population and ways in which national guidelines might be applicable (or not) in a European context. There was immediate general consensus among the taskforce sub-group about the core issues around palliative care provision for people with intellectual disabilities; these led to the definition of categories for the resulting norms. The draft norms, agreed by all 12 taskforce members, consisted of 52 statements in 13 categories.
Round 2
A total of 85 questionnaires were returned. Of these, five were blank and were excluded, leaving 80 usable questionnaires (59 fully completed and 21 partially completed) from 15 European countries (see Table 1). Two countries (Norway and Ireland (Rep)) were heavily represented due to the way the survey was distributed among large numbers of clinical experts in those countries.
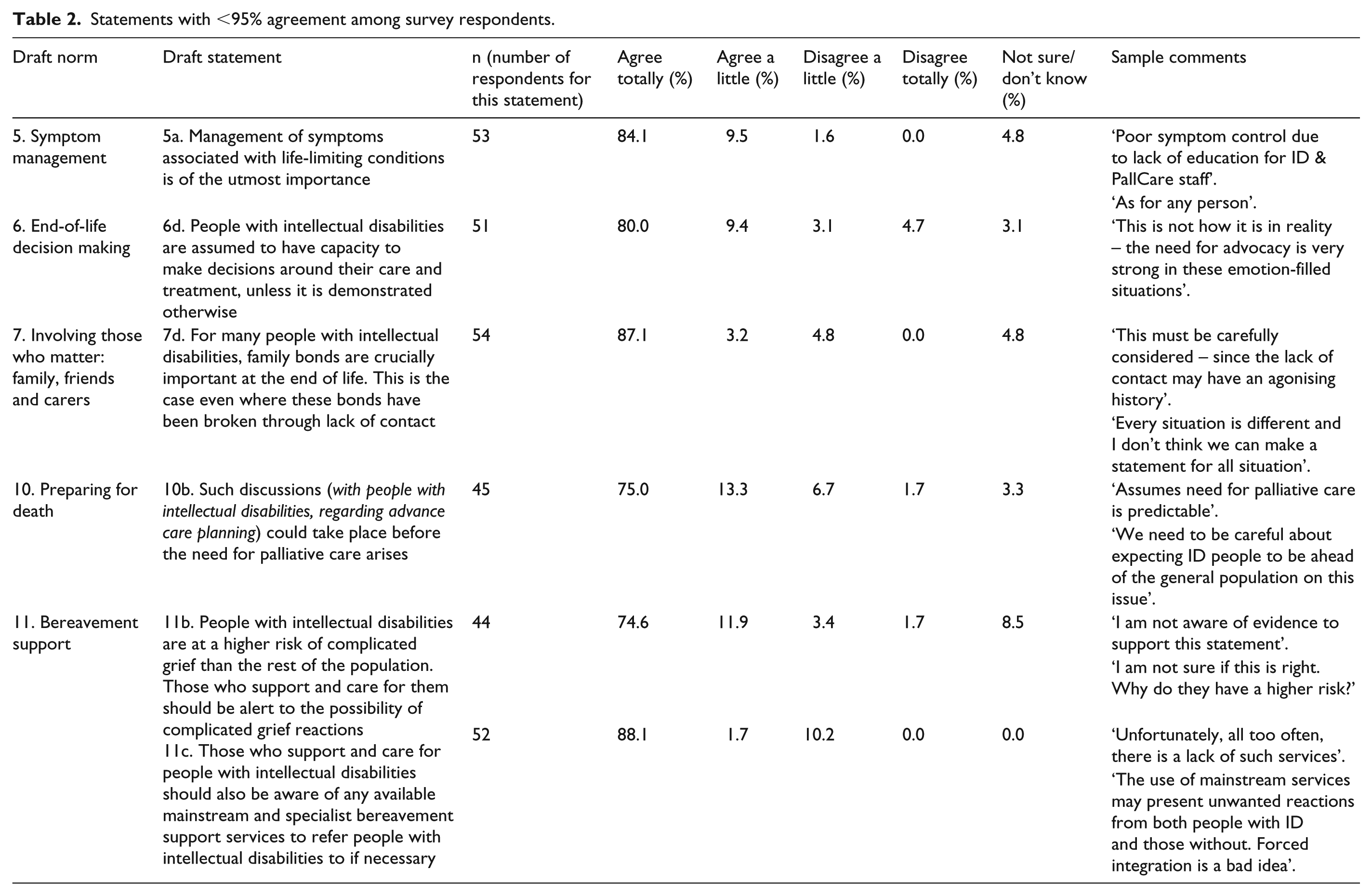
All items scored a median of ‘agree totally’. A total of 47 items scored ⩾95% ‘agree totally/agree a little’ (of these, the vast majority were ‘agree totally’). Five items scored between 86% and 95% ‘agree totally/agree a little’. No items scored <86% agreement. A total of 476 of comments on the 52 individual statements were received (range: 5–18). These clarified, to some extent, the reasons for either ‘disagree totally/a little’ or ‘not sure/don’t know’ responses (see Table 2). As there was strong consensus among the expert panel, a second round of the survey was not needed.
Statements with <95% agreement among survey respondents.
Round 3
Despite the strong consensus on all 52 statements, the taskforce re-considered each item in light of the scores and comments with the aim of optimising clarity and ease of understanding. This led to some statements being re-worded. For example, statement 7d (see Table 2) was changed marginally as follows: ‘For people with intellectual disabilities, family bonds MAY BE crucially important at the end of life. This MAY BE the case even where these bonds have been broken through lack of contact’. Background explanations and evidence were added to the final White Paper, for example, reference to the strong research evidence that people with intellectual disabilities are at increased risk of complicated grief (statement 11b).
The following statement was deleted under norm 12 (education and training): ‘General education and information available to the public should be aimed at leaving future generations less afraid of people with intellectual disabilities, and less afraid of dying’. Although this statement had 98.9% agreement among the expert panel, taskforce members thought, on reflection, that it was related to a more general need for attitudinal change within society and, therefore, fell outside the scope of the White Paper.
Round 4
The final version of the consensus norms can be found in Table 3. The full White Paper can be found on the EAPC website (http://www.eapcnet.eu/). In addition to the norms, it contains background information, research evidence, practice examples and resources.
Consensus norms for palliative care of people with intellectual disabilities in Europe.
Discussion
This is the first document to provide internationally relevant guidance that demonstrates what quality palliative care for people with intellectual disabilities consists of. The fact that these are aspirational norms, rather than standards (which would imply a minimum level below which care should not fall), is important. There might be a danger, for example, that in some regions or countries where palliative care is unavailable, even for the general population, some or all of the ‘standards’ for palliative care of people with intellectual disabilities would be dismissed as being unachievable and, therefore, irrelevant – as some of the comments from the expert panel indicated.
Challenges and limitations
Sampling bias
Collecting information through a relatively small number of invited ‘experts’ runs the risk that the data provided by these key persons could become slightly exaggerated. 18 The survey responses are skewed towards Northern Europe, with respondents from Norway and Ireland particularly overrepresented. It is worth noting that despite our best efforts, it was particularly difficult to find expert panel members from certain parts of Europe, especially countries in Southern Europe. Palliative care professionals from underrepresented countries typically commented that they had never come across a patient with intellectual disabilities and had no idea who they were or where they lived. Many intellectual disability professionals commented that in their country, palliative care was not available to people with intellectual disabilities. These findings are, of course, anecdotal, but they indicate that across Europe, there may be significant inequalities with respect to palliative care provision to people with intellectual disabilities that need to be investigated further and addressed.
Lack of population data
The difficulty in finding ‘experts’ is related to the difficulty in establishing what happens to people with intellectual disabilities when they reach the end of life, where they live and are cared for and where they die. To a large extent, this is due to the lack of population data on people with intellectual disabilities in almost all European countries. The WHO 3 has identified this as a problem, stating that the ‘major failure to recognize and support this group has led to a massive hidden population of children and adults with intellectual and other disabilities who are unknown to the official system’ (p. 5). This failure has serious implications, including the fact that palliative care services will struggle to identify which of their patients have intellectual disabilities There is a risk that the needs of a hidden population are not seen as a priority or even as a problem. This makes it much more difficult to engender system changes that would ensure all people with intellectual disabilities have access to palliative care support and services that meet their specific needs.
Involvement of people with intellectual disabilities and carers
Although the development of the norms was informed by the contributions of people with intellectual disabilities in relevant research and local guidelines, they have not been directly involved in the development and writing of the White Paper.
What is unique about providing palliative care for people with intellectual disabilities?
There are many overlaps between the norms in this paper and generally recognised best practice in palliative care.39,40 However, it is clear that people with intellectual disabilities face specific barriers in accessing palliative care and need extra attention and knowledge to ensure that the general standards for good palliative care are met. It is often not so much a question of what needs to be done, but how. Norms 8 (collaboration), 12 (education and training) and 13 (developing and managing services) are, therefore, particularly important for palliative care services.
‘Getting it right’ for people with intellectual disabilities has huge advantages for palliative care services. Those who are able to provide good care for patients with this level of complexity and challenges are likely to be able to provide good care for all their patients. The skills needed to meet the norms in this paper are transferable. For example, the ability to assess symptoms in non-verbal patients with profound intellectual disabilities will benefit all patients who are unable to communicate their symptoms for reasons other than intellectual disabilities. The way in which palliative care is provided for people with intellectual disabilities could thus be a benchmark for palliative care services everywhere.
Recommendations
Cross-fertilisation of expertise
The importance of collaboration (see norm 8) is not limited to local collaboration between disciplines. Expertise in this area is scarce and often isolated. The establishment of the EAPC Taskforce on Intellectual Disabilities has highlighted the benefits of learning from each other, both within and across national boundaries. The Palliative Care for People with Learning Disabilities Network (http://www.pcpld.org), which has a strong UK focus, has spearheaded such cross-fertilisation of expertise in a variety of ways. As different European countries will face different challenges, there will be enormous benefit in ‘comparing notes’ with practitioners in other countries, sharing both difficulties and best practice in a range of settings.
Reaching out
Many intellectual disability services and families are either unaware or suspicious of available palliative care expertise, contributing to the inequalities in access. It is important, therefore, that palliative care services actively build bridges to the population of people with intellectual disabilities within their catchment areas.
Further research
This remains an under-researched area. Most of the available empirical knowledge originates in North West Europe, especially the United Kingdom. Further research, particularly internationally relevant research, is essential in order to understand and address the challenges involved in meeting the needs of people with intellectual disabilities at the end of life. The taskforce has noted the importance of answering the following research questions:
What is the current state of affairs around palliative care provision for people with intellectual disabilities in Europe? In order to address inequalities, it is important to gain insight into the scale of the problem. Studies are needed to investigate (and compare with data for the general population) where people with intellectual disabilities die and who supports them at the end of life.
What are the challenges in achieving the consensus norms set out in paper, across Europe? These challenges are expected to vary, depending on national, cultural, organisational and legal differences. Without a good understanding of the issues involved, it will be impossible to address the current inequalities in palliative care provision.
What are the issues around end-of-life decision making for people with intellectual disabilities across Europe? There are international concerns around the processes of decision making (including patient participation) and the factors influencing end-of-life decision making.
Developing outcome measures for palliative care of people with intellectual disabilities: A common European instrument is needed for measuring the quality of palliative care provision, in order to be able to compare and contrast palliative care for people with intellectual disabilities (1) between settings/regions/countries and (2) in comparison with palliative care for the general population. This White Paper could be a starting point for developing such outcome measures or for adapting existing ones.
Conclusion
We hope that the White Paper has highlighted the importance of having a specific focus on the palliative care needs of people with intellectual disabilities. The consensus norms set a benchmark for changes in policy and practice. To take this work forward and achieve the norms and recommendations, funding will be essential. We would like to encourage national associations, key stakeholders, palliative care services, intellectual disability services and all individual practitioners to examine their own practice and policies and make the changes required in their own countries in order to meet the norms set out here.
Footnotes
Acknowledgements
The authors would like to thank all members of the expert panel for their valuable input and comments; the EAPC Board of Directors for their encouragement and support; Prof Sheila Payne and Prof Chris Hatton for constructive feedback on an early draft of the White Paper; and the Faculty of Health, Social Care and Education at Kingston University & St George’s University of London for providing practical support, including support for the lead author in undertaking this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.