
Abstract
Background:
As the number of people ageing in prison with complex healthcare needs continues to increase, so does the need for palliative care in the restrictive prison context. Palliative care for people in prison is facilitated by correctional officers, and prison- and hospital-based clinicians. A collective analysis of existing research to identify common experiences of these stakeholders globally has not been completed.
Aim:
To explore the perceptions and experiences of correctional officers and prison- and hospital-based clinicians who facilitate palliative care for people in prison.
Design:
A systematic review and meta-synthesis.
Data sources:
Keywords and subject headings related to palliative care and prisons were used to search seven databases with no time limitations. Peer-reviewed research in English, containing qualitative data from stakeholders facilitating palliative care for people in prison were included, and appraised using the CASP tool.
Results:
Two analytical themes emerged: (i) a prison lens on a palliative approach and (ii) coping complexities. Palliative care is ‘translated’ into the prison setting according to security and environmental constraints. Stakeholders experienced ethical, personal and professional difficulties, because prison-based palliative care did not align with community norms. Ambiguous policy and expectations regarding prioritising care needs and balancing custodial rules led to role stress.
Conclusions:
Providing palliative care for people in prison is complex and impacts stakeholders and people in prison with palliative care needs. Supporting person-centred care through a multi-service approach, stakeholder education and standards will improve the quality and accessibility of care.
What is already known about this topic?
Globally, the need for palliative care for people in prisons is increasing as the number of older people with complex, chronic illnesses continues to rise.
Current research describes challenges of managing advanced, life-limiting illnesses in prison.
The views of people in prison regarding dying and palliative care in prison have been explored in a meta-synthesis.
What this paper adds?
The prison setting creates a ‘lens’ through which palliative care is filtered, to account for security protocols that shape care provision.
Perceptions of patients, prioritisation of healthcare, role stress and the expectations of others impact clinicians’ and officers’ practice.
Implications for practice, theory or policy?
A multidisciplinary, multi-service based palliative approach will create shared responsibility and mutual understanding between stakeholders.
Person-centred, relational education specific to each discipline will increase palliative care knowledge and confidence.
Expanding the use of standardised measures and reporting will improve transparency and drive quality improvement.
Introduction
The management of people in prison with advanced, chronic and terminal illnesses is of growing importance as global prison populations continue to age and increase.1 –4 People in prison with palliative care needs are managed while remaining in custody, or in community settings by allowing early release or parole on compassionate grounds. 5
Though laws allowing for compassionate release are relatively common, eligibility criteria are often highly restrictive and vary between and within countries.5 –8 As a result, patients require palliative care in prison, and there is mounting pressure to improve the accessibility and quality of palliative care provided within a custodial environment. 9
While the United Nations Nelson Mandela Rules 10 state that people in prison have a right to receive healthcare equal to that available in the community, there are many additional barriers to accessing high-quality, person-centred palliative care in prison. 11 The social and environmental context of prisons restricts palliative care provision in pursuit of security, though clinicians are held to the same professional standards as community providers.10,12,13
There is no global standardised approach to prison-based palliative care between countries. Most services rely on a mix of prison- and hospital-based care. 14 Approaches include an in-reach model linked with local palliative care services and some specialist onsite facilities (UK), 15 onsite hospices managed by staff and peer caregivers (US) 16 or an expectation that all palliative patients will be released to die outside of prison (France). 17
Correctional healthcare clinicians provide primary palliative care within prison facilities, either while the patient is housed with the general population or when admitted to an onsite healthcare unit, if present. 18 Hospital-based clinicians facilitate inpatient specialist palliative care, 19 while correctional officers oversee security in all settings. 20
The aim of this systematic review and meta-synthesis is to examine the perceptions and experiences of stakeholders who facilitate palliative care for people in prison and understand their perspectives on palliative care and dying in prison. This review was designed to address the following research questions:
How do prison-based clinicians, hospital-based clinicians and correctional officers characterise their experiences and involvement in facilitating palliative care for people in prison?
What do these stakeholders identify as the barriers and enablers to palliative care provision for people in prison?
Method
Design
Systematic review and meta-synthesis.
Protocol registration and ethical approval
The protocol for this work was registered with PROSPERO (CRD42021290740). Ethical approval was not required.
Methodology
This study used Thomas and Harden’s 21 meta-synthesis approach to explore primary data published in existing qualitative studies to draw new meaning. This approach allows close examination of data through free coding, collation of key ideas in descriptive themes, and generation of new theory or concepts by developing analytical themes. The mix between objective and subjective approaches make this a flexible and useful methodology for data synthesis.
Search strategy
A search strategy comprised keywords and MeSH terms related to palliative or end-of-life care, and prison (Supplementary file 1) was used to search PubMed, MEDLINE, Embase, CINAHL, ProQuest, Web of Science, PsycINFO and CINCH. The ‘prisoner’ population filter designed by CareSearch was also used to search PubMed. The search was conducted in February 2023.
Eligibility criteria
No limitations were placed on the search. Articles were included if published in English in a peer-reviewed journal, described primary research, and contained raw qualitative data of stakeholders’ perceptions and experiences of palliative care provision in prison. As limited research from low- and middle-income countries is available, and resources and experiences of stakeholders are likely to differ considerably from the majority of research conducted in high-income countries, these articles were excluded. Articles describing unexpected deaths, illness that was not advanced, chronic or life-limiting, or detention related to immigration or war were excluded. Stakeholders were defined as prison- or hospital-based healthcare providers, and correctional personnel who provided or facilitated palliative care for people experiencing incarceration. The focus of this review was on professional roles that would be common to most or all prison palliative care models globally. Therefore, articles reporting models of supportive care provided by other people in prison (peer caregiving) were excluded.
Screening
Articles were screened using EndNote 20 and Covidence. Duplicates were removed using the EndNote 20 ‘Remove Duplicates’ tool and by manual screening. Each title and abstract was screened by two authors, IS and either MD, NH or JP. All articles underwent full text screening by two authors (IS and JP or NH) and final inclusions reviewed in discussion with all authors to reach consensus.
Data extraction
Information including author, year, country (lead author), title, qualitative approach, aim and sample size were recorded into an Excel spreadsheet. Quotes from correctional healthcare providers, community-based healthcare providers, correctional officers and other stakeholders managing people in prison with palliative care needs (either in prison or community healthcare settings) were extracted into a separate spreadsheet.
Critical appraisal
Articles were appraised using the Critical Appraisal Skills Programme (CASP) tool for reporting qualitative research (IS). An additional author appraised five of the included articles, and results were discussed until a consensus was reached (Supplementary file 2). Critical appraisal results did not impact the inclusion of articles.
Data synthesis
Thomas and Harden’s 21 approach was used to sequentially and inductively explore ideas evident in raw qualitative data. Data was first categorised (step one, free coding), distilled (step two, descriptive themes) and interpreted to develop new meaning (step three, analytical themes). Step one comprised free coding, assigning representative keywords to each quote that summarise the content. This enables repeated, meaningful engagement with data and gathering of related content. Initial free coding (IS) generated free codes that were provided to MD and NH, who independently coded 25% of quotes. Consensus was reached through discussion.
During step two, free codes were collected and connected inductively to describe interlinked nature of concepts. Codes were collected into branching hierarchies that described supra- and sub-ordinate ideas in a coding tree (Supplementary file 3). The coding tree illustrated common and significant perceptions, barriers and facilitators of palliative care in prison from the perspective of clinicians and correctional officers, which were then developed into explanatory descriptive themes. Descriptive themes were used to illustrate the emerging concepts and identify associated ideas, which were then interpreted to develop analytical themes based on the collective dataset (step three, all authors).
Results
Search results
A total of 2664 records were retrieved during the search conducted in February 2023. After removing 1675 duplicates, 989 records were screened, and 953 records excluded (see Figure 1). Of the 36 remaining for full-text review, 23 articles were excluded as they did not contain qualitative data from clinicians or correctional officers (n = 15), or were related to peer caregiving programs (n = 8). Therefore 13 articles were included in the review (Table 1). Articles originated in the United Kingdom (n = 7), the United States (n = 3) and one each from Australia, France and Switzerland.
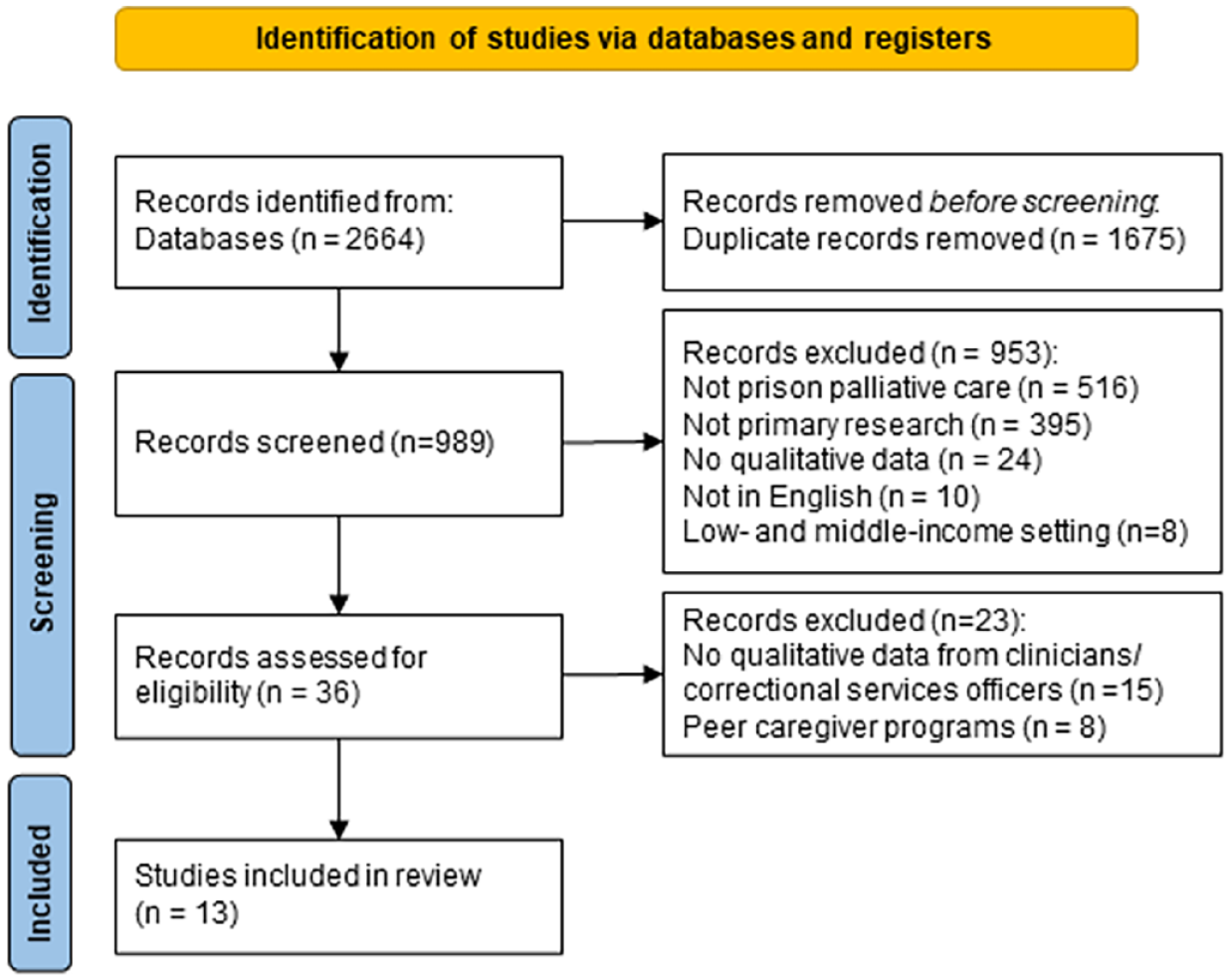
PRISMA flow diagram. 30
Summary of included articles (N = 13).
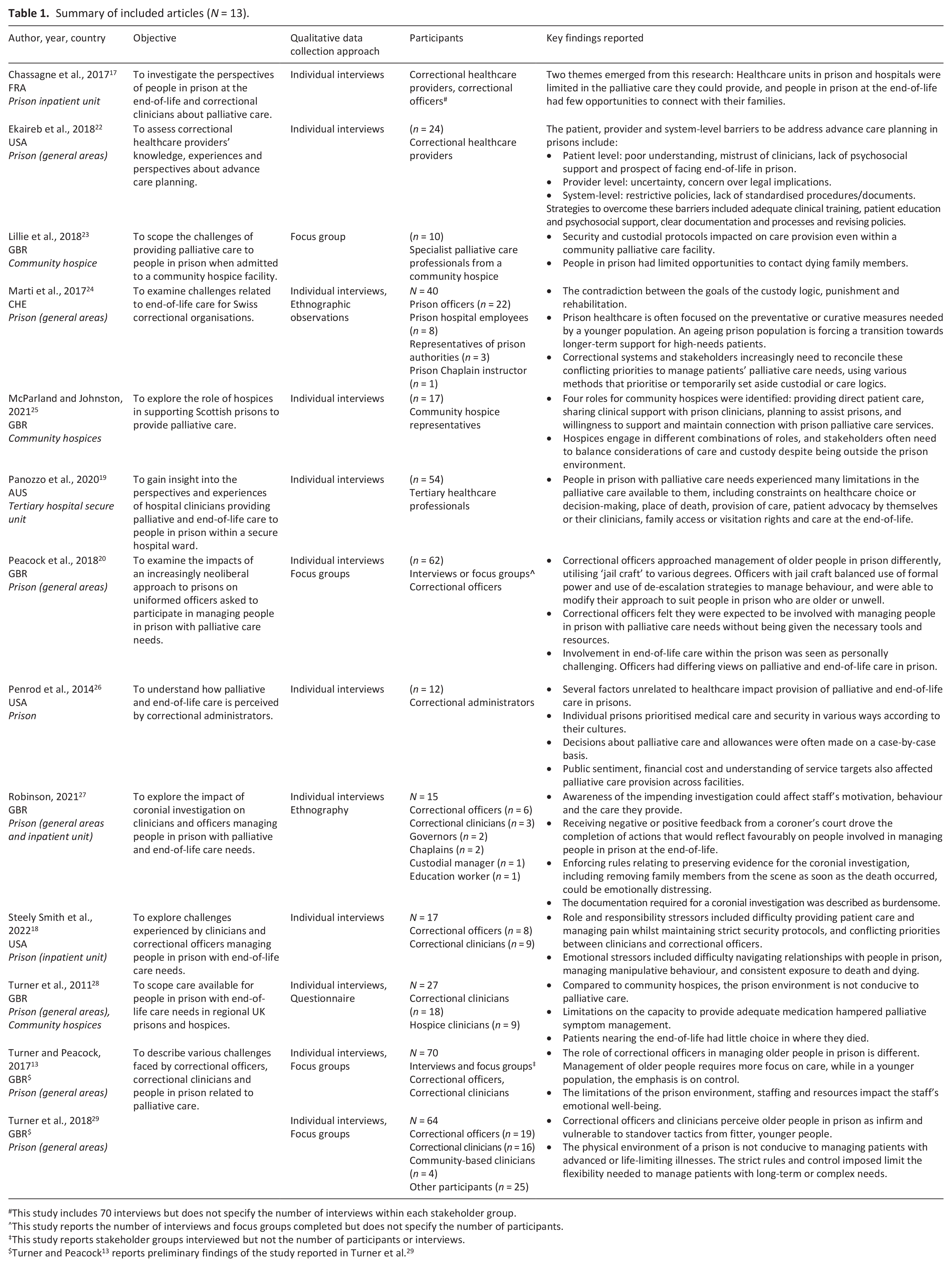
This study includes 70 interviews but does not specify the number of interviews within each stakeholder group.
This study reports the number of interviews and focus groups completed but does not specify the number of participants.
This study reports stakeholder groups interviewed but not the number of participants or interviews.
Critical appraisal
Included articles addressed an average of 7 out of 10 CASP criteria, with individual articles fulfilling between six and nine criteria. All articles provided a clear statement of aims, were compatible with qualitative methodology, used research design appropriate to the aims, collected data in a way that addressed the research question, included a clear statement of findings, and generated valuable research. The recruitment strategies were rarely sufficiently detailed to assess appropriateness (n = 5), as was the relationship between researcher and participants (n = 2) and the degree to which ethical issues had been considered (n = 2). Articles were not excluded on the basis of appraisal.
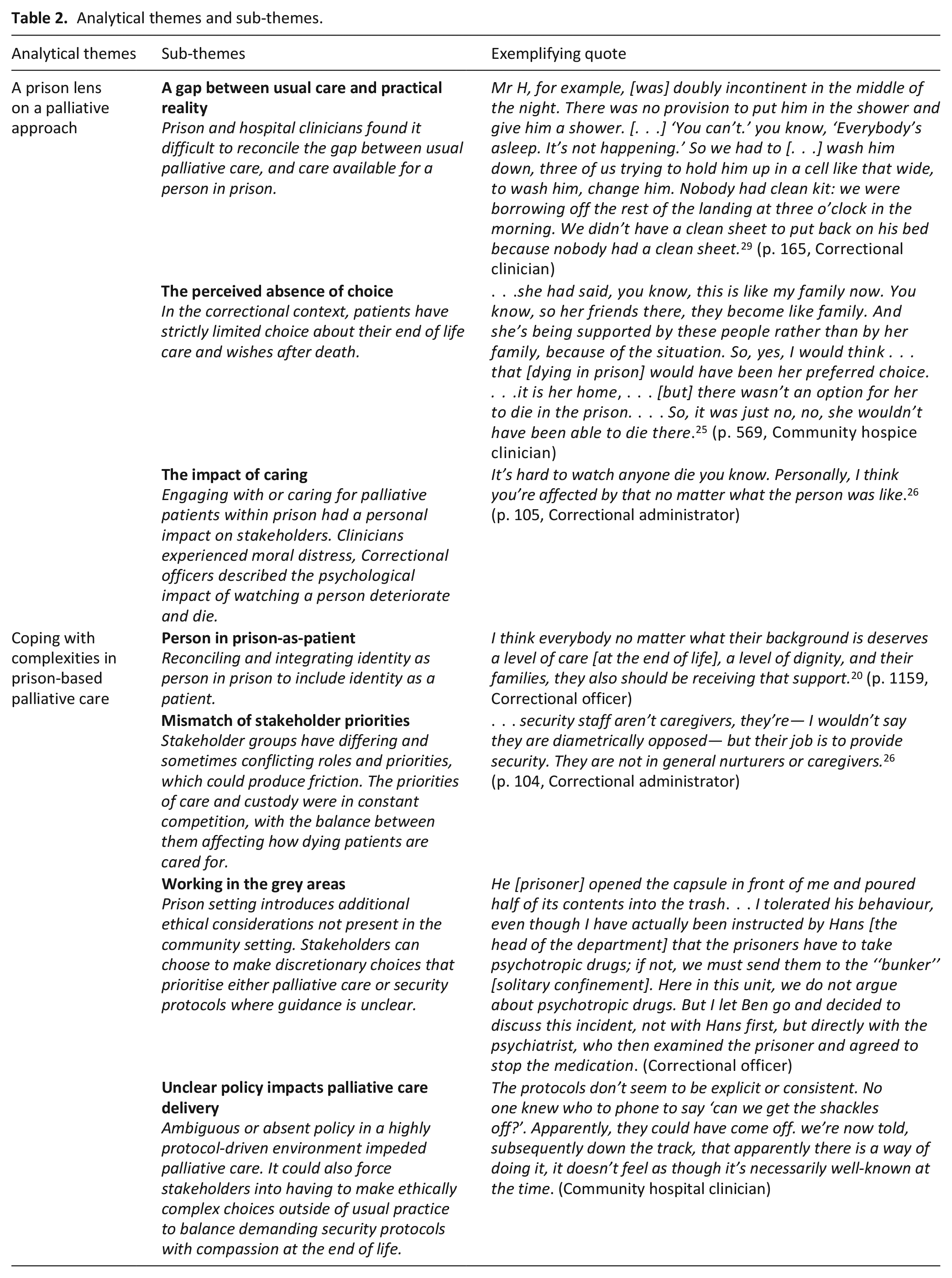
The meta-synthesis generated two analytical themes (Table 2), which described correctional healthcare clinicians’, correctional officers’, and hospital-based clinicians’ perspectives and experiences of facilitating or providing palliative care for people in prison.
Analytical themes and sub-themes.
A prison lens on a palliative approach
Participants’ reflections on palliative care for people in prison encapsulate the pervasive influence of the prison environment and culture on delivery of palliative care. The prison context effectively creates a ‘lens’ through which palliative care is viewed and alters expectations of ‘usual care’ to fit what is possible in a custodial environment.
A gap between usual care and practical reality
Clinicians providing palliative care to people in prison found it difficult to reconcile the difference between palliative care available to people in prison and that available to people in the community. In particular, limitations in clinical autonomy were evident and affected practice. While community-based clinicians operate autonomously and independently, all aspects of healthcare for people in prison are mediated by correctional officers who uphold the various prison rules and regulations.
. . .their rules are their rules, and we have to operate within those rules
18
(p. 232, Correctional nurse, US)
Clinicians working in the custodial environment perceived that security measures could ‘. . .get in the way. . .’
18
(p. 232, Correctional clinician, US) of clinical care, impeding practices that ‘. . .you wouldn’t even blink an eyelid [at,] out in the community. . .’
29
(p. 165, Correctional nurse, UK). When providing healthcare in prison: Everything is harder. You want to do things for the patients. Sometimes even simple things, but you just can’t. There are multiple hoops to jump through for even something as simple as an extra pillow or blanket. There has to be a medical necessity for everything. It’s hard to get used to
18
(p. 233, Correctional clinician, US)
Managing pain within the prison environment was particularly problematic due to practical limitations such as not having a pharmacy onsite, 18 slow implementation of medication changes, 28 needing two nurses to administer pain medication, 29 limited access to pro re nata medication while in a cell, 19 and restrictions on the type17,28 and use17,28 of opioid medications because of concerns about trafficking. Managing pain within the prison ‘. . .is the most important thing here, but it can also be the most challenging’ 18 (p. 231, Correctional clinician, US).
Even when people experiencing incarceration were managed in an external community hospice or hospital, caring for them was ‘. . .much, much harder because the prison is always with you, the prison comes into the hospice. . .’ 23 (p. 370, Community hospice clinician, UK). The constant presence of correctional officers at the patient’s bedside, including during inpatient medical consultations or family visits, was intrusive and ‘. . .does affect how you can have conversations, and the conversations you can have with them [the patient]. . .’ 23 (p. 370, Community hospice clinician, UK). Even therapeutic psychiatric sessions with the person in prison were always conducted in the presence of correctional officers. 19
Clinicians also reflected on whether close supervision and physical restraints in community healthcare facilities were necessary for frail, unwell patients 23 and questioned the negative impact it had on the care they could provide.17,19,23 While community clinicians wanted to provide usual palliative care to patients from prisons, they acknowledged that ‘. . .even if you want to do the best, deliver the best care, it is different’ 23 (p. 370, Community hospice clinician, UK).
For correctional officers, adjusting care for people with palliative care needs to comply with security protocols was perceived to be reasonable and justified: Security plays such a major role. And rightfully so in what we do in corrections. I mean don’t forget, don’t lose sight of what is our mission in terms of being a Department of Corrections. That sometimes can blur the line and what you would normally expect to happen in a community. . . for someone who is dying, and for death, doesn’t necessarily have a place in the prison system that is. . .basically focused on security and public safety. . .
26
(p. 6, Correctional administrator, US)
The perceived absence of choice
Correctional and community clinicians contrasted the restricted choice palliative patients in prison had compared to community patients, expressing frustration when they could not fulfil patient preferences in line with usual palliative care practice.19,22,25,28
In Australia, patients are often transferred from lower security regional facilities to maximum security metropolitan centres with greater access to hospitals for specialist palliative care. However, doing so meant ‘. . .los[ing] their room [cell] and los[ing] their job, so they’re effectively discharged from the [minimum or medium security] prison, even if it’s just an outpatient appointment. That’s a big deal’ 19 (p. 987, Hospital clinician, AUS).
Clinicians’ frustration was particularly amplified regarding preferred place of death because: . . .a major foundational part of palliative care is trying to. . .achieve death in the desired site of death. I think it grates against us. . . because a person who’s incarcerated has lost the privilege of deciding where they are’
19
(p. 987, Correctional clinician, AUS)
Where patients could not be released, clinicians wanted to offer ‘. . .somewhere that was slightly more therapeutic than just a prison cell. . .’ 28 (p. 375, Correctional clinician, UK). Being unable to facilitate a patient’s wishes as they would for a community-based patient and in line with ethical principles of palliative care was difficult to reconcile. 25
Advance care planning was perceived to be particularly fraught due to the legal and social context of prisons, yet only discussed in one study. Some clinicians were committed to facilitating patients’ choices because ‘. . .you have control over so little in your life here. . .’ 22 (p. 2385, Correctional clinician, US), and it was an opportunity to exercise a degree of autonomy. Other clinicians felt that people in prison ‘. . .are different from us. They have a different desire to live than we have’ 22 (p. 2385, Correctional clinician, US), and suggested that many would not want a ‘Do Not Resuscitate’ (DNR) order.
The prison context influenced clinician’s willingness to have conversations about advance care planning, with some expressing concern that these discussions may be perceived as withholding treatment, or that patients may feel coerced into a decision. Clinicians were also wary that a patient’s imprisonment may influence their end-of-life care preferences, and that any advance care planning conversations may be distressing, as they prompt patients to think about dying in prison with limited family or social supports. 22
There was a perception that even where opportunities for advance care planning existed, many patients doubted that their end-of-life wishes would be implemented which could make them reluctant to engage in these conversations. 22
Small instances of choices by patients were described, with some patients choosing to refuse specialist care in order to remain in their usual prison 19 or refusing medication. 24
The impact of caring
All participant groups reflected on the personal and professional impact of managing people in prison with palliative care needs. Both correctional- and community-based clinicians struggled with ‘. . .wanting to do more when you can’t. . .’ 18 (p. 233, Correctional clinician, US), such as giving patients an extra pillow or blanket, 18 equipment such as pressure mattresses, 29 more family visitation, 19 ready access to pain relief13,19 or comfort therapies such as music or flowers. 19
As correctional clinicians could ‘. . .essentially live with them [patients] for 8-10 hours a day. . .’ 18 (p. 234, Correctional clinician, US) for long periods of the patient’s sentence, they observed their deterioration firsthand, which could have an emotional impact.13,18
It’s difficult and especially when you’re used to your patient, attachment is there. . . But my relation[ship] with them is just like a normal patient; I never see them as a prisoner. . . So, when they die, you feel [pause] you feel hurt [pause], but you just have to carry on
13
(p. 63, Correctional clinician, UK)
The impact of being unable to provide usual care extended to after the patient died. As deaths in custody often automatically trigger a formal inquest into how and why the patient died, the area becomes a crime scene and cannot be disturbed. A nurse described that: . . .I find [it] quite strange because when you’re in a hospice or on a ward, we do the last offices and we wash them, wrap them up. Here, when they die, you just leave them. And that’s quite difficult. . ., because it’s a crime scene. . .you have to come out [of the patient’s room]
27
(p. 10, Correctional clinician, UK)
For correctional officers, managing older people and those nearing the end of life in prison was an unexpected aspect of their role. These participants felt ill prepared to deal with the end-of-life needs of people dying in prison. 20 They expressed discomfort with having to undertake extended hospital supervision of a dying patient or attending their funeral, which was ‘. . .pretty grim, really’ 13 (p. 63, Correctional officer, UK), and ‘. . .quite oppressive, especially if you’ve got your own personal circumstances as well’ 20 (p. 1159, Correctional officer, UK). These effects were magnified if participants were also dealing with issues of death and dying in their personal lives.
As a result of their role in maintaining security, correctional officers were also more hesitant to engage with people in prison for fear of being perceived as too empathetic: ‘Certainly you can’t expect that there isn’t some sort of attachment. . .but everyone doesn’t accept that’ 26 (p. 106, Correctional administrator, US).
Correctional clinicians and correctional officers described how their capacity to cope with end-of-life issues and the strategies changed as they became more experienced in their roles. Early in their careers, some felt they empathised too much with people in prison who died, which led to a greater emotional impact after their death. 18
The first time I had an experience with death, I had to call the Chaplain. The look they [dying patients] give you is just something you don’t forget, like you just can’t help them. We had a long talk about life and death, and I even talked to friends to get a better perspective where I could be at peace with it. Before here, I’ve never just watched someone die. . .
18
(p. 233, Correctional officer, US)
Participants noted how their approach to managing these feelings had changed over time, with many describing emotion-focused strategies such as avoidance, compartmentalisation, and distancing themselves from patients as coping methods. Some described that they ‘. . .just shut it off’ 18 (p. 234, Correctional officer, US), ‘. . .go into robot-mode. . .’ 13 (p. 63, Correctional clinician, UK) or that they ‘. . . don’t discuss what I do here at home with my wife. . .’ 18 (p. 234, Correctional officer, US). Only one correctional officer noted that they actively sought to talk to others about their experiences to cope rather than repressing or avoiding their emotions. 18 Even with that social support, ‘. . .it gets overwhelming. Some deaths are harder than others’ 18 (p. 233, Correctional officer, US). Participants were also reluctant to share their experiences at work with their families, ‘. . .unless [it’s] something really good’ 18 (p. 234, Correctional officer, US), which compounded their sense of needing to cope with this alone.
A lack of community understanding also contributed to correctional clinicians
13
and officers
20
adopting more individual rather than social coping strategies, largely because the public could be ‘. . .very judgemental. . .’
13
(p. 63, Correctional clinician, UK) about them providing any care or support to people in prisons: . . .[because they say], ‘Well, you know, how could you do anything to help prisoners? They’re not very nice people’
13
(p. 63, Correctional clinician, UK)
Managing people in prison at the end of life had a profound effect on correctional officers and clinicians, introducing challenging ethical questions and accompanied by fewer opportunities for social support.
Coping with complexities in prison-based palliative care
Person in prison-as-patient
While the harsh reality of a person’s incarceration was omnipresent, details of their crime and sentence are rarely disclosed to treating clinicians to preserve the person’s privacy. For some community-based clinicians, this lack of disclosure amplified their feelings of insecurity when caring for people in prison and impacted their patient-provider relationship
23
: You feel a little bit insecure because you don’t know what he did, even though he looks perhaps pathetic and unable to do anything different, and no crime probably, you just feel different because you have a different relationship with the patient . . . Although we want the best care and the best everything
23
(p. 370, Community hospice clinician, UK)
The nature of a person’s crimes could also impact how clinicians perceived patients from prison and the acceptability of caring for them.23,25,26 In one community hospice, staff were cautious about caring for an incarcerated patient until they knew the patient was not a sex offender, after which ‘. . .they weren’t really bothered anymore’ 25 (p. 569, Community hospice clinician, UK).
In a secure inpatient hospital unit that routinely cares for people in prison, it was noted that clinicians did not want to know a patient’s offence because they did not want this information to impact their management of the patient’s care. 19 However, it was perceived by clinicians that not knowing a patient’s sentence or time left to serve also limited their capacity to have conversations about prognosis, to embark on long-term care planning, and to explore the potential for compassionate release. 19
Despite these concerns, clinicians were committed to providing the best possible care for people in prison with palliative care needs.
They’re people at the end of the day so you [pause] it is amazing how you put aside any thoughts or feelings you have for who they are or what they are, as to care for them for being a person
13
(p. 63, Correctional clinician, UK)
Clinicians felt that the prison context unavoidably changed the patient-provider relationship. Though correctional clinicians focused on improving health and well-being, they reflected that their role in the prison system impacted patient’s trust in their care.
People perceive that providers in a jail-based setting care less about them than community providers. There is a perception quality of care is poorer. I think that creates a lot of mistrust
22
(p. 2384, Correctional clinician, UK)
Though still strongly security focused, correctional officers and administrators also acknowledged that managing older or chronically ill people in prison required some adjustment to their usual approach, which is oriented to managing young men and a greater emphasis on discipline.
You are getting people in their late 60s, 70s—even into the 80s—which is [pause] quite a different level of care. Their needs are different, it’s more around medical, health issues; not really any control problems as you get in the younger population. . . I think some of the staff probably find it difficult – because with the younger population it’s more you front it out and shouting, and the older guys you don’t . . . they don’t need that
20
(p. 59, Prison Governor, UK)
Correctional officers described a range of attitudes towards their role in facilitating palliative care for people in prison. Some correctional officers were less oriented towards beneficence as a motivator of palliative care, and more towards a duty of care and obligation, as ‘. . .it’s part of your job, you know, you’ve got to care whether you want to or not’
20
(p. 1159, Correctional Officer, UK). Others thought that: . . .everybody, no matter what their background is, deserves a level of care, a level of dignity. . . Just because they’re a prisoner, just because they’ve done wrong in life – haven’t we all?
20
(p. 1159, Correctional officer, UK)
Some officers were more tentative in their openness to compassionate measures such as early medical release.
I’m tempted to say that a dying inmate should not be in prison
17
(p. 71, Correctional officer, FRA, emphasis added)
Motivations for care provision could also be impacted by the impending coronial investigation. 27 Coronial inquests closely examine how patients are managed at the end-of-life both by correctional services and correctional healthcare providers as a means of assessing quality, equity and appropriateness of the care provided. As deaths in custody are often subject to mandatory inquests, awareness of the need to justify their choices can motivate delivery of care that the coroner will look upon favourably, rather than being guided entirely by patient need. 27 Doing so mitigates the risk of future criticism in the coronial court, but may result in care that is less patient-centred and needs-focused. 27
Mismatch of stakeholder priorities
The differing roles of those involved in providing palliative care and those responsible for prison security caused tension, especially when their goals or practices conflicted or impeded one another. With their primary focus on care, prison- and community-based clinicians could be frustrated by security protocols that impacted their capacity to provide palliative care.
It makes no sense! This is not palliative care! There should be no locked doors. In palliative care, the patient has the right to come see caregivers when they have a free moment, and vice versa. That’s why we ask for open doors
17
(p. 70, Correctional clinician, FRA)
Some clinicians also believed that correctional officers’ lack of experience in managing terminally ill patients led them to overestimate the risk posed by individuals, and resulted in excessive security precautions.
23
This was acknowledged by a correctional administrator, who noted that: . . .we often have greater fears of security than what’s really likely to happen. But—that’s how the DOC [Department of Corrections] has to think, you know
26
(p. 103, Correctional administrator, US)
Correctional officers and administrators prioritised security considerations when mediating care because ‘. . .ultimately, we are responsible for the safety of the inmates, medical staff, and ourselves’ 18 (p. 232, Correctional officer, US). Being committed to upholding their responsibility to protect staff and maintain order meant some correctional staff distanced themselves from engaging with aspects of healthcare, framing it as outside their role and inappropriate for them to engage in. 26
. . .security staff aren’t caregivers, they’re— I wouldn’t say they are diametrically opposed— but their job is to provide security
26
(p. 104, Correctional administrator, US)
Where clinicians perceived correctional officers as overly cautious as palliative patients are already frail and functionally impaired, correctional officers believed that clinicians were not sensitive enough to the risks17,18: The caregivers, they sometimes have a tendency not to see the danger when they are with the inmate. . .
17
(p. 70, Correctional officer, FRA)
Therefore, correctional officers could ask clinicians to provide care quickly and reduce the amount of time in contact with the patient. 17 Correctional staff felt they needed to find a balance because ‘. . .even though we are compassionate, we have to keep order’ 18 (p. 232, Correctional officer, US).
Working in the grey areas
The prison environment is bound by strict protocols that govern every activity, resulting in a very ‘black and white’ approach that discourages deviation from the norm. When managing people with palliative care needs, correctional officers can choose to temporarily set aside protocol or predefined roles that could impede palliative care in order to appropriately manage patients.
While correctional officers did not see healthcare as a part of their role, they could make a pragmatic decision to engage in care, such as giving a person in prison a twice-daily ointment because the correctional healthcare provider was short-staffed. 24 Even though this was outside the role of correctional officers, ‘. . .it was completely logical that we do it. But, of course, some team members first said: no, this is a medical case . . .’ 24 (p. 38, Correctional officer, CHE).
In situations like this this case, the officer justified working outside their usual role because of the patient’s need, the lack of other solution, and by showing the task was not burdensome: ‘. . .[I] put on the gloves, . . . then I started the treatment and when I was done he said: what? Have you already finished?’ 24 (p. 38, Correctional officer, CHE).
However, others felt that crossing this professional boundary meant correctional officers risked being labelled as someone who would take on this undesirable role again in the future. 20
The Prison Service are renowned for the willing horse syndrome . . . If it’s a touchy-feely thing, ‘Well, such-a-body’ll do that . . .’. And you get that person labelled and I worry that if the [palliative care suite] has been set up . . . that’s what’ll happen
20
(p. 1159, Correctional officer, UK)
Correctional officers and clinicians shared instances of choosing to momentarily set aside protocol for compassionate reasons after a person’s death, such as covering them with a sheet once they had died, or moving a patient who died on a commode to maintain their dignity. 30 These compassionate actions not only deviated from prison protocol, but also legal requirements to preserve evidence for investigations after a death in custody. Correctional officers justified these actions as reasonable and humane steps that were worth the risk of breaking protocol for the sake of the patient’s dignity.
. . .the police said ‘Who’s done this? Who’s done that? Have you touched the body?’ ‘Yeah’ [laughs], yeah it were me. And we’d got the last rites too
27
(p. 12, Correctional officer, UK)
Such instances illustrate the discretionary decision-making used by correctional officers and clinicians to facilitate palliative and end-of-life care in prison.
Unclear policy impacts palliative care delivery
The presence, absence and implementation of policy impacted palliative care provision for people in prison. Though jurisdictional palliative care policy that applied to all facilities was present in some jurisdictions, the unique culture and demographic of each facility, and the interest of senior leaders in palliative care strongly influenced whether palliative care was available in various prisons in practice. 26 While prisons within a jurisdiction may ‘. . .physically have a strong [physical] resemblance. Culturally they don’t’ 26 (p. 102, Correctional administrator, US).
There could be wide variation across prisons, with some more focused on security, while others incorporated a more therapeutic approach which may include palliative care. This variation in approach also meant that implementing standardised, specific protocols for palliative care was impractical. The implementation of extended visitation rights at the end of life across all jurisdictional prisons was unfeasible because each prison operates differently, and such policies ‘may not make sense to the operation of the institution’ 26 (p. 104, Correctional administrator, US).
Jurisdictional policy regarding end-of-life care provision was therefore designed to be ‘. . .permissive. . .’ 26 (p. 103, Correctional administrator, US), with implementation dependent on the institution’s culture, interest of correctional leaders, population needs and demographic. 26 It was therefore difficult to advocate for development of capacity to provide end-of-life care in a highly security-focused environment. Doing so was ‘. . .a struggle. . .getting that paradigm shifted a little bit is. . .a challenge’ 26 (p. 104, Correctional administrator, US).
Managers of correctional officers were also concerned about having sufficient resources to facilitate palliative care given their shrinking budgets,20,26 wondering whether ‘. . .the staff have the time to actually to go in and sit and talk to somebody. . .?’ 26 (p. 105, Correctional administrator, US). Some correctional officers chose to volunteer their time to ensure palliative care could be provided to those who needed it. 26 However, this led to an assumption that future palliative care would also rely on unpaid work, with participants motivated to donate their time ‘. . .because they believe in what they are doing. They believe in hospice care’ 26 (p. 104, Correctional administrator, US).
An absence of policy to translate palliative care practices into prisons impacted patient autonomy, care planning and advocacy. While advance care planning was ostensibly available to people in some prisons, ‘We don’t have an organized system for dealing with [Advance care planning]. . .so it gets neglected’ 22 (p. 2385, Correctional clinician, US).
Unclear guidance about which clinicians should be undertaking advance care planning, which patients were eligible, and how to ensure plans were enacted in prison or in hospital left clinicians reluctant to complete care plans.
‘Our policy does say we take care of patients, but we don’t advocate for them. . .’
22
(p. 2385, Correctional clinician, US)
Concern about legal repercussions of completing and implementing an Advance Directive or Advance Care Plan was strong in one US study. This indicates that stakeholders felt the threat of legal action because of the complex ethical issues, and that in turn informed their decision-making about care. 22
Discussion
Exploring the perceptions and experiences of correctional officers and prison- and hospital-based clinicians provides valuable insights into the challenges and tensions of providing palliative care to people in prisons. People in prison have the right to receive person-centred palliative care, yet clinicians and officers describe difficulties they encounter facilitating this.
In discussing their experiences, these stakeholders reflected on the difference between ‘usual’ palliative care in the prison setting compared to community norms (‘a prison lens on a palliative approach’) and how the correctional environment introduces ethical and practical ambiguities to care provision (‘coping with complexity in prison-based palliative care’).
Privileging different identities
Previous research has discussed the unavoidable tensions between care and custody from a practical or systems viewpoint, focusing on the conflicting goals of healthcare and imprisonment.11,24,31 Drawing from the above analysis, we examine how that can be applied to stakeholders’ perceptions of the identity of the person in prison with palliative care needs, both within prison and in community healthcare settings.
A central concern for those facilitating palliative care for people in prison was how to reconcile and balance the competing identities of a person in prison with palliative care needs as both a ‘person in prison’, who is experiencing incarceration and as a ‘patient’ with healthcare needs (Figure 2). 24
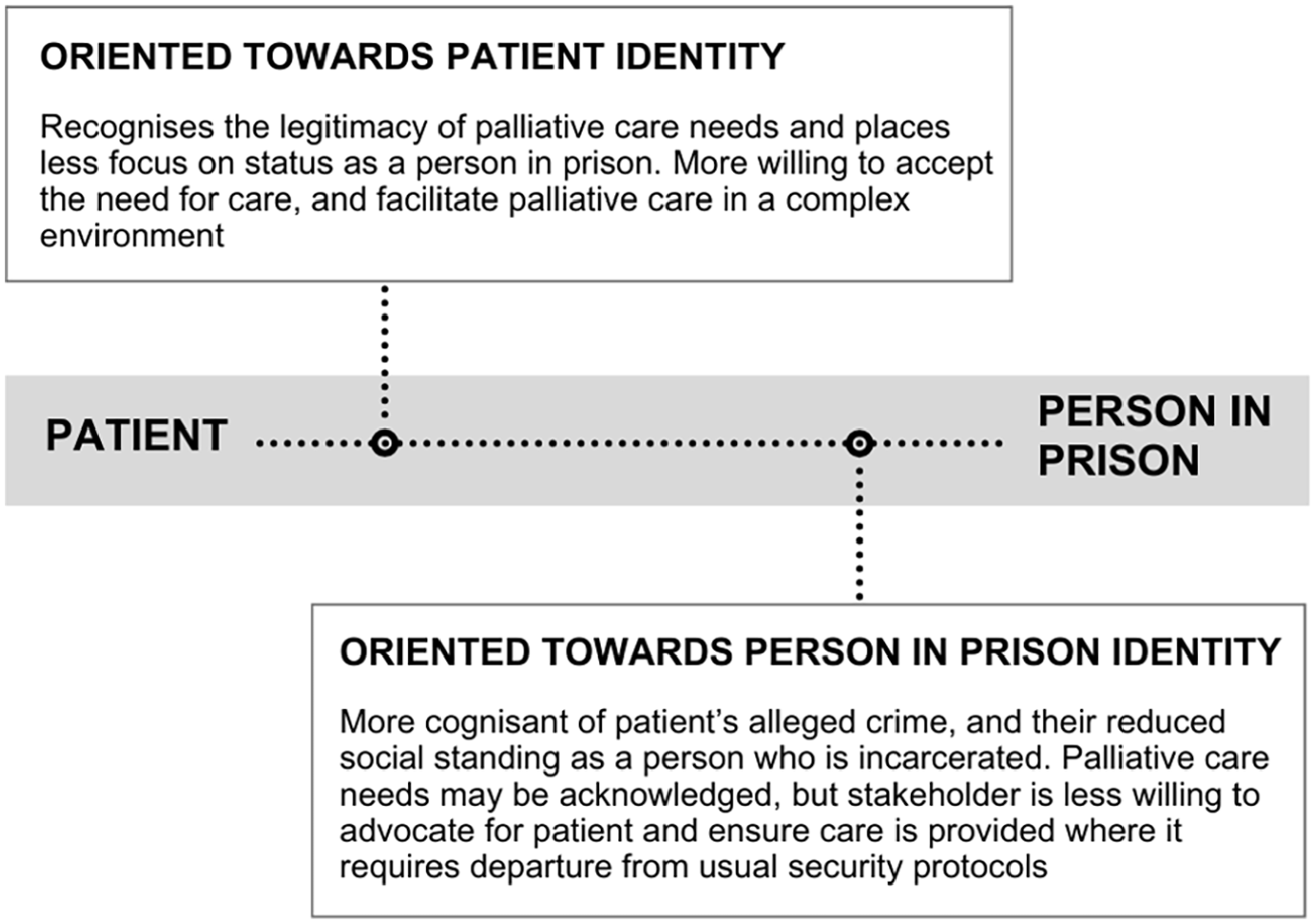
Patient – Person in Prison continuum.
While both ‘patient’ and ‘person-in-prison’ identities are present, privileging one identity over another can shape correctional officers’ and prison- and hospital-based clinicians’ attitudes, inform their decision-making, and influence care for people in prison with palliative care needs.
Assessment of a person in prison’s identity is affected by personal context or attitudes,20,32 professional role,33,34 organisational culture,35,36 approach to managing people in prison, 37 feeling of safety 38 and engagement with healthcare. 36 The critical concern for palliative care patients is that their identity as a person in prison does not affect their access to timely, quality care when needed. 11
Examples of good practice indicate that a collaborative multidisciplinary, multi-service approach fosters a more person-centred palliative approach for people in prison.13,39 –43 This can include correctional healthcare providers, correctional services and community palliative care services. Bringing stakeholder groups together creates a beneficial dialogue between disciplines to promote mutual understanding of roles, responsibilities and environmental limitations, as well as collective problem-solving.
Generating cultural change to effectively recognise and acknowledge palliative care needs requires multiple actions, including formal or informal education for all stakeholders and modelling of person-centred management of palliative patients by palliative care specialists during in-reach visits.
Permitting or prioritising healthcare
Security influences all aspects of prison operations, including provision of palliative care. Prisons are a unique institution in which to provide healthcare, as providers are not entirely autonomous, but allowed to occupy a physical and metaphorical sub-space by another more privileged organisation that provides oversight.44,45 Despite these differences, prison-based healthcare services and providers are still subject to community regulatory bodies and codes of conduct.
Clinicians are permitted to operate in a small physical clinic space within the prison, surrounded by secure areas where clinicians have less power and agency.34,45,46 Even entry into their workplace must be authorised by correctional officers. Similarly in the metaphorical space, healthcare is also shaped by privileged custodial objectives to varying degrees across different facilities, 34 and facilitated by non-clinical correctional officers who tacitly regulate access to care and resources.32,36
A patient’s movement between the general population and the healthcare unit can also reflect change in the balance of the ‘patient’ and ‘person in prison’ identities. Patients continually move between these divergent physical and metaphorical spaces of healthcare areas and general housing areas, between their identity as a patient and a person in prison, and between settings where their individuality can be either set aside, or prioritised.
Providing equivalent healthcare services in prison will always be complicated by the correctional setting, but remains imperative for clinicians to question entrenched practice where improvements could be made. Including correctional officers in training focused on principles and standards of care will assist in an understanding of regulatory requirements, usual practice, and why requests such as leaving doors open at the end of life are made.
Role stress within and between professional groups
The psychological impact of managing people in prison with palliative care needs is evident in the discourse of each stakeholder group. Stress arose from role conflict, the conflict between different goals of their role or divergence between what they expected their role to be and the reality. 47
Despite prisons being a ‘black and white’, protocol-driven context, the difficulties stakeholders described in their daily practice revealed the nuances of operating in this challenging environment reflected in other literature.33,34,44 For correctional clinicians, balancing professional ethical codes of conduct while delivering person-centred care within a context that systematically limits patient autonomy was a source of anxiety.34,48 Correctional officers need to maintain their authoritarian, discipline-oriented role, while simultaneously preserving welfare and health of people in prison. 33
As a result of these conflicting professional objectives, 33 clinicians and particularly correctional officers encountered situations with palliative care patients where they felt they needed to ‘step into the grey’; to temporarily set aside their professional roles to meet patients’ palliative care needs.33,35,44,46
Stepping into the grey meant making pragmatic, discretionary choices that did not entirely align with organisational policy or acting outside their expected professional role, such as correctional officers engaging in healthcare tasks or clinicians integrating custodial considerations into their practice.33,46,49,50 While examples in the literature of stepping into the grey typically support palliative care,20,27 they also involve uncertainty and stress for stakeholders who were concerned about repercussions for moving outside generally accepted practice.
Addressing this source of stakeholder stress requires establishing a sense of shared responsibility for palliative patients through a multidisciplinary approach, as well as an organisational commitment to person-centred care and staff wellbeing to reduce the impact of role stress on stakeholders.
Perceptions and expectations of others
The differing social norms of prison- and hospital-based clinicians, and correctional officers also impacts approach to care. Careful social, physical and emotional distancing 51 between prison employees and people in prison with palliative care needs was apparent, and justified by security rules 52 or framing of a person in prison as ‘other’, and therefore unworthy of care. 28
Stepping outside these cultural expectations, even for patients with palliative care needs, 51 could be perceived as being ‘too caring’ and attract disapproval from other stakeholders. 51 In an environment where in-group solidarity is a core source of emotional and occupational support,53,54 separation from colleagues can have profound consequences for coping. 53
The stress of managing conflicting, varying or ambiguous professional expectations34,46 and moral distress is also evident in the coping mechanisms discussed. Both clinicians and correctional officers discussed using coping mechanisms including distancing language such as referring to a death as a non-specific hypothetical event (‘when it happens’), and shutting down emotional attachments and responses as they became more experienced.13,18,20 Opportunities for social coping are also reduced because of negative public perceptions towards caring for people in prison; and correctional officers and clinicians felt they needed to justify their role in facilitating care to other people.13,20,26
Normalising a person-centred approach, engaging in reflexive practice and increasing opportunities for constructive social coping in the context of a palliative approach to care may better support correctional officers and clinicians and enhance their wellbeing.
Implications and learnings
Informed by this meta-synthesis and literature, several key actions needed to build prison palliative care capacity have emerged.
Firstly, it is essential to expand use of a multidisciplinary, multi-service approach to prison palliative care involving officers, correctional clinicians and in-reach specialist palliative care professionals. This creates a sense of shared responsibility for palliative care, assists mutual understanding of other disciplines’ roles and practice, and supports collaborative problem solving. Further, it promotes day-to-day experiential learning for officers and correctional clinicians, and modelling of good practice by in-reach palliative care specialists. 25 Widening implementation of frameworks that emphasise this, such as the Dying Well in Custody Charter, 55 will support service development. 43
Secondly, investment in discipline-appropriate palliative care education for all stakeholders will improve knowledge and confidence. A person-centred, relational perspective will promote empathy and understanding of the complexities of dying while incarcerated, 56 reorienting stakeholder perspectives towards the patient identity. Group education further provides opportunity for peer leadership, reducing stigma about caring, and constructive social coping activities such as regular debriefing sessions and wellbeing training. Various prison palliative and aged care education approaches are used globally,57 –61 with innovative shared learning strategies such as Project ECHO 62 also building connections between prisons, and communicating instances of good practice.
Lastly, designing systematic, standardised measures and reporting mechanisms aligned with existing prison-based palliative care guidance63 –67 is a key strategy to improving accessibility and quality of healthcare.68,69 Broadening the use of existing standards and assessment tools,63,64,70 and developing new prison-specific indicators where necessary will promote transparency and accountability. 71 This should be informed by existing research about the use of health measurement and indicators in prisons.69,71 –74
What this paper adds
This meta-synthesis complements an existing review describing the perceptions of people in prison about palliative care in prison to provide perspectives from a range of stakeholders. 11 Other reviews have addressed ageing in prison, 75 psychosocial aspects of prison-based palliative care, 76 staff experiences of expected and unexpected deaths in prison, 77 and death and dying in prison.15,78,79
This review builds on this body of literature by focusing on palliative care for patients whose death would be expected, and occur as a result of advanced, life-limiting illness. While some concepts regarding ageing and dying in prison covered in other reviews may be common with those related to palliative care, the impact of managing long-term deterioration, the expectation of death, navigating post-death investigations of an expected death, and considering ethical questions about dying in prison and compassionate release are unique to this population and review.
As Thomas and Harden’s 21 meta-synthesis method allows the synthesis of diverse qualitative research such as varying approaches to prison-based palliative care, it was an appropriate choice for this data. By identifying patterns of concepts across context-specific data, it is possible to link common ideas and draw new meaning. This facilitates analysis driven by both data and theory that is currently absent from published reviews regarding death, dying and care for people in prison approaching the end of life. This step distinguishes the meta-synthesis approach, and this review, from reviews on similar topics using a narrative synthesis approach.
Other research has described aspects of the ‘care versus custody’ tension from the perspectives of prison nurses34,44 or correctional officers,33,37 regarding the clinician’s role in compassionate release, 80 and during direct care delivery.28,29 This work builds on previous research by extending this concept to include how clinicians and officers perceive the identity of people in prison, and appreciate how the tensions between custody and care impact stakeholders.
This study incorporates a theoretical approach to exploring stakeholders’ experiences, including the focus on patient identity, balancing contradictory objectives, the burden of role stress, and the perceptions of others. Practical recommendations are offered to address issues raised by stakeholders.
Limitations
While research from five countries is included in this review, the small number of included papers and variety of disciplines and topics of focus are limitations. Consequently, it is not possible to contrast findings between countries and their various models of care. Future research could address this as the body of literature grows. The meta-synthesis approach is beneficial in drawing analysis directly from primary data from multiple studies. However, as this methodology can only utilise quotes chosen by the original author for publication, contextual information and nuance may be missing.
Conclusion
Quality and accessibility of prison-based palliative care has progressed in recent decades, but it is evident from the reflections of stakeholders and people in prison 11 that there is more to be done. Continued commitment to service improvement, particularly in countries with underdeveloped prison palliative care systems and growing need is an essential first step. Despite different models of prison-based palliative care between countries, there is considerable value in exchanging knowledge and sharing of good practice to drive progress.
Supporting this process at a national level by formalising policies and standards and creating resources to facilitate practice change will further improve palliative care provision beyond the local context. Collectively, these strategies will support the transition of prison-based palliative care globally from aiming to provide a ‘good enough death’ 52 to a ‘good death’. 9
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241262614 – Supplemental material for Perceptions and experiences of clinicians and correctional officers facilitating palliative care for people in prison: A systematic review and meta-synthesis
Supplemental material, sj-docx-1-pmj-10.1177_02692163241262614 for Perceptions and experiences of clinicians and correctional officers facilitating palliative care for people in prison: A systematic review and meta-synthesis by Isabelle Schaefer, Stacey Panozzo, Michelle DiGiacomo, Nicole Heneka and Jane L. Phillips in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163241262614 – Supplemental material for Perceptions and experiences of clinicians and correctional officers facilitating palliative care for people in prison: A systematic review and meta-synthesis
Supplemental material, sj-docx-2-pmj-10.1177_02692163241262614 for Perceptions and experiences of clinicians and correctional officers facilitating palliative care for people in prison: A systematic review and meta-synthesis by Isabelle Schaefer, Stacey Panozzo, Michelle DiGiacomo, Nicole Heneka and Jane L. Phillips in Palliative Medicine
Supplemental Material
sj-png-3-pmj-10.1177_02692163241262614 – Supplemental material for Perceptions and experiences of clinicians and correctional officers facilitating palliative care for people in prison: A systematic review and meta-synthesis
Supplemental material, sj-png-3-pmj-10.1177_02692163241262614 for Perceptions and experiences of clinicians and correctional officers facilitating palliative care for people in prison: A systematic review and meta-synthesis by Isabelle Schaefer, Stacey Panozzo, Michelle DiGiacomo, Nicole Heneka and Jane L. Phillips in Palliative Medicine
Footnotes
Author contributions
JP and IS conceptualised review. IS conducted searches and IS, NH, MD and JP screened papers. All authors contributed to data analysis, conceptualised themes and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Australian Federal Government Department of Health National Palliative Care Projects initiative.
Data management and sharing
The search strategy, coding tree and CASP critical appraisal are available as supplementary documents.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.