
Abstract
Objective
To validate a previously described 5-item short-form Nottingham Extended Activities of Daily Living and assess the properties of incorporating contemporary tasks to create a novel Contemporary Extended Activities of Daily Living scale.
Design
Validation study.
Setting
Conducted through an online questionnaire.
Participants
Adults over 60 years of age, living with a chronic condition or receiving care, caregivers, and healthcare providers.
Main measures
We assessed internal consistency of each scale using Cronbach's alpha. Additionally, criterion validity and convergent validity of the short-form and contemporary scales were assessed using Spearman's correlation analyses with the original 22-item Nottingham scale, and with quality of life measured by the European Quality of Life 5-dimension scale.
Results
Across 712 participants (n = 256, 36% with a chronic condition), both the short-form Nottingham Extended Activities of Daily Living scale (α = 0.84, 95% CI: 0.82–0.86) and a novel Contemporary Extended Activities of Daily Living scale (α = 0.88, 95% CI: 0.87–0.89) had good internal consistency. The short-form scale had excellent concurrent validity (rs = 0.82, p < .00). Each contemporary item was correlated with the original Nottingham scale, and the full Contemporary scale had good concurrent validity (rs = 0.78, p < .001). Both scales had moderate construct validity in relation to quality of life (short-form Nottingham scale rs = 0.68, p < .001, contemporary scale rs = 0.56, p ≤ .001).
Conclusions
Our initial evaluation of a Contemporary Extended Activities of Daily Living scale shows that construct validity is not compromised by the inclusion of contemporary tasks. Future research is needed to account for the diversity of activity patterns to improve the perceived relevance of scales assessing functional outcomes.
Keywords
Clinical messages
Extended activities of daily living scales can help quantify function, but commonly used scales are not suited to current practice.
A short form of the Nottingham extended activities of daily living scale, which has shown promise in stroke, also worked well in an older adult population.
Contemporary tasks, such as mobile phone use or internet shopping, can be added to activities of daily living scales without compromising validity.
To retain both cultural validity and clinical utility, tasks included in activities of daily living assessments should be reviewed and updated as needed.
Introduction
The ability to function well is fundamental for healthy ageing. 1 Functional decline in older adults may be precipitated, or accelerated, by disease, injury, or chronic condition. 2 Assessment of function in daily life, using validated scales, is vital, as the resulting score may inform the level of support needed post-discharge or serve as an endpoint in randomized controlled trials.3–5
An approach to quantifying function is assessing the ability to perform activities of daily living (ADL). ‘Basic’ ADLs capture fundamental personal needs (e.g. toileting), whereas ‘extended’ ADLs include more complex tasks (e.g. shopping). 6 Extended ADLs are more sensitive to change as they place higher demands on cognitive and physical ability, 7 and their decline may be considered an early indicator of underlying pathology, such as dementia.8,9
The Nottingham Extended Activities of Daily Living 10 and the Lawton Extended Activities of Daily Living 11 are the most common measures of extended ADLs used in research. 12 The 22-item Nottingham scale was designed to assess functional outcome after stroke or other conditions. 13 The Nottingham self-report scale offers the advantage of capturing self-perception of performance. However, recognising that self-report may lead to bias through incorrect interpretation or cognitive impairment, the scale can also be scored by a clinician. 14 The 8-item Lawton scale is typically assessed by a healthcare professional. 15 While both tools remain popular, key concerns relate to item redundancy and contemporary relevance.16–18
Item redundancy in extended ADL scales can be driven by the number and content of items. Current scales take 10–15 minutes to administer by a healthcare professional, 19 presenting a potential burden. 20 Shorter scales may improve completion rates 21 while minimising fatigue.22,23 Attempts to shorten extended ADL scales have described a 5-item short-form Nottingham Extended Activities of Daily Living scale, which retained good internal consistency and validity. 17 Although validated in a stroke population, 24 its properties should be described for other populations to maximise benefits. Given the associations between extended ADLs and quality of life,25,26 this construct can be used to validate any new iterations of the scale. 13
Furthermore, the issue of the relevance of component items needs to be addressed. Both the Nottingham and Lawton scales are decades old, and their face validity is questioned. A recent study 16 reported that up to 80% of older adults do not engage in activities described by common extended ADL scales. Rather, many activities have shifted to the online space (e.g. banking and socializing), a change not reflected in the traditional assessments. 16
We aimed to evaluate psychometric properties (construct and concurrent validity, reliability) of the short-form Nottingham Extended Activities of Daily Living scale in a mixed sample of adults. Furthermore, we aimed to initially validate a novel Contemporary Extended Activities of Daily Living scale, evaluating its construct validity and reliability.
Methods
The study was approved by the University of Glasgow Medical, Veterinary and Life Sciences Ethics Committee (application number 200210164). Participants provided informed consent prior to participation. Eligible participants were English-speaking adults, older than 50 years (who self-identified as living with a chronic condition or not), caregivers, or healthcare providers. There were no exclusion criteria. Participants were recruited on a voluntary basis via the Join Dementia Research network. The study was advertised on the platform between January and April 2024. The advertisement included the participant information sheet and a link to an online questionnaire, which volunteers could respond to with no time limitation. Recruitment was staggered over time and geography to manage demand. We did not calculate a target sample size a-priori due to a lack of precedent for our target comparisons.
We used the 22-item Nottingham Extended Activities of Daily Living scale, where scores range from 0 to 66, with higher scores representing greater independence. The short-form Nottingham Extended Activities of Daily Living scale we used consisted of 5 items from the original scale 17 : walking over uneven ground, crossing roads, taking hot drinks from one room to another, washing up, and making oneself a hot snack; with a maximum score of 15. For both the short form and 22-item scale, responses were captured in four levels scored from 0 to 3. 13 The maximum score on the short form scale was 15.
To explore the utility of adding contemporary tasks to an extended ADL scale, we assessed the 5-item short-form Nottingham Extended Activities of Daily Living scale with an additional five items. 16 These were the tasks most frequently reported by older adults but not captured by the original Nottingham and Lawton scales (referred to as ‘Contemporary Extended Activities of Daily Living scale’). Additional tasks were using online banking, paying by card, using a mobile phone, shopping online, using the internet and using social media. The contemporary items were operationalised following the format of the original Nottingham scale questions (e.g. ‘Do you use online banking?’). The scoring followed the same 4-level format described above, with scores ranging from 0 to 30.
The Lawton Extended Activities of Daily Living scale was presented in a format that enabled self-administration, with all questions presented regardless of gender. Participants were instructed to select the option that best applied to them for each extended ADL task (e.g. shopping). The options intended to be administered by health professionals were converted to ‘I’ statements. For example, when referring to shopping, ‘Takes care of all the shopping needs independently’ was rephrased as ‘I take care of all shopping needs independently’. We assigned scores of 0 (cannot perform) and 1 (can perform) to each response, with the maximum score of 8 reflecting full independence in extended ADLs.
Finally, we measured a related construct, quality of life, as this has been previously used to evaluate construct validity of the original 22-item Nottingham scale. 13 We administered the European Quality of Life 5-dimension 3-level health-related quality of life scale, 27 scored across three severity levels, with higher scores indicating lower quality of life. The scores are typically expressed as a five-digit code describing the health state in each dimension (e.g. 11111 represents the highest quality of life). We chose this scale over other quality of life measures for its reduced number of items and simple response scale. The 8-item short-form Stroke Impact Scale 28 was used as a measure of a related construct, the perceived impact of stroke on function, where relevant to participants. The scale is scored on a 5-point Likert scale and chosen over the original Stroke Impact Scale 29 for its brevity. Total mean scores are converted into a 0–100 range with higher scores representing a more favourable outcome.
Participants answered a series of online questionnaires, taking ∼10–15 minutes to complete. Hosted on the Qualtrics platform, 30 the questionnaire included the following scales in this order (Figure 1): the short-form Nottingham Extended Activities of Daily Living scale 17 ; the Nottingham Extended Activities of Daily Living scale 10 ; five additional contemporary extended ADLs questions 16 ; the Lawton Extended Activities of Daily Living scale 11 ; the European Quality of Life 5-dimension 3-level health related quality of life scale 27 ; and the optional short-form Stroke Impact Scale. 28 At the end, participants were asked for demographic details: gender, age group, and a self-identified status (living with a chronic condition, caregiver, and healthcare provider). Age was collected in categorised groups to minimise potentially identifiable data. All participants were instructed to respond based on their own experiences (i.e. not acting as a proxy).
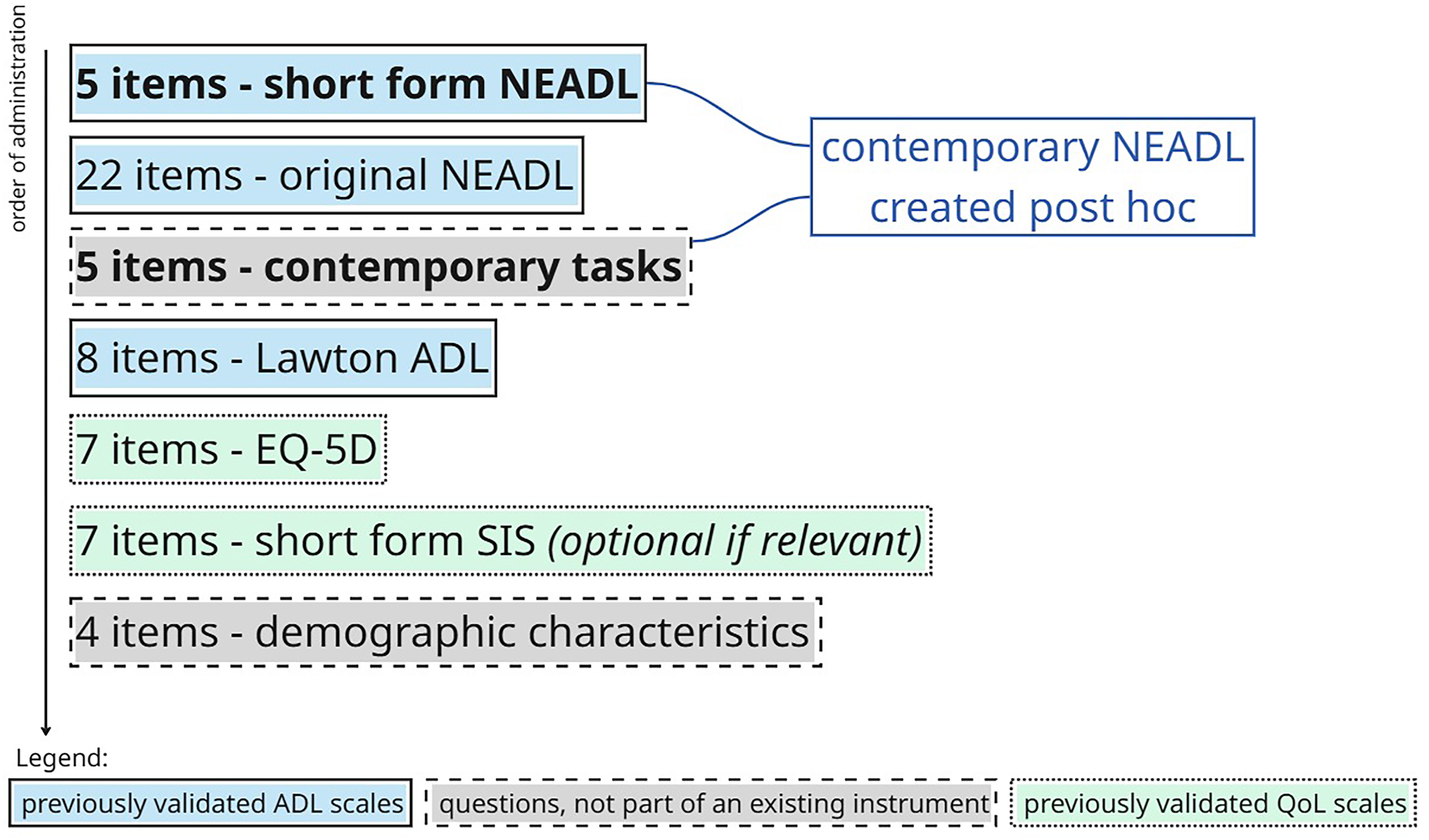
Illustration of questionnaire contents in order of administration. ADL: Activities of Daily Living; QoL: quality of life; NEADL: 22-item Nottingham extended Activities of Daily Living; EQ-5D: EuroQol-5 dimensions; SIS: Stroke Impact Scale.
The study was conducted in accordance with the Declaration of Helsinki 31 and followed the reporting checklist for studies on measurement properties of patient-reported outcome measures (COSMIN). 32
We inspected the distribution of responses across all scales using density plots to identify potential outliers. In case of outliers, we conducted a sensitivity analysis, removing these values. We calculated the proportion of participants reaching the maximum score, with >15% being the threshold for the ceiling effect. Similarly, floor effect was reported if >15% of participants scored the lowest value on the scale. Descriptive statistics (mean, standard deviation) were used to summarise responses across scales. All missing rows were excluded from the individual analyses. All analyses were conducted in RStudio 33 using R. 34
To assess the reliability of each scale and the strength of associations between individual items, we calculated internal consistency using Cronbach's alpha with 95% confidence intervals (95% CI) based on standard error for both the short-form Nottingham Extended Activities of Daily Living and the Contemporary Extended Activities of Daily Living scales. A value of [0.7, 0.95] is accepted as evidence of good internal consistency, 35 while higher values may indicate item redundancy. 12
We assessed two types of validity. Criterion validity represents the extent to which a new scale agrees with a ‘gold-standard’ scale measuring the same construct. We evaluated concurrent criterion validity of the short-form Nottingham Extended Activities of Daily Living, Contemporary Extended Activities of Daily Living, and each single contemporary item with the 22-item Nottingham and Lawton extended ADL scales using Spearman's correlation coefficient. 36
Similarly, we assessed convergent construct validity reflecting the extent to which the short-form Nottingham Extended Activities of Daily Living and Contemporary Extended Activities of Daily Living scales capture the intended construct of functional independence in extended ADLs. We used Spearman's correlation with the related (but distinct) construct of quality of life, as measured by the European Quality of Life 5-dimension. We had intended to utilise short-form Stroke Impact Scale for construct validity, but we excluded it from analysis due to high missingness (93.5%) observed in our random sample. The demographics questions that followed had expected rates of completion (in order of administration: sex 13.9%, age group 20.4%, and self-identified status 1.8% missingness), which suggests stroke scale missingness was not due to participant fatigue, but rather selective response.
We set the significance threshold at p < .05 with correlation coefficients >0.7 representing good validity. 37 We ran the analyses across all participants, followed by a subgroup analysis of healthy individuals and those living with a chronic condition. All correlation coefficients were corrected for attenuation by unknown reliability. 38
Results
The sample included 712 participants. Self-identified demographic characteristics are shown in Table 1.
Descriptive characteristics of the participants.
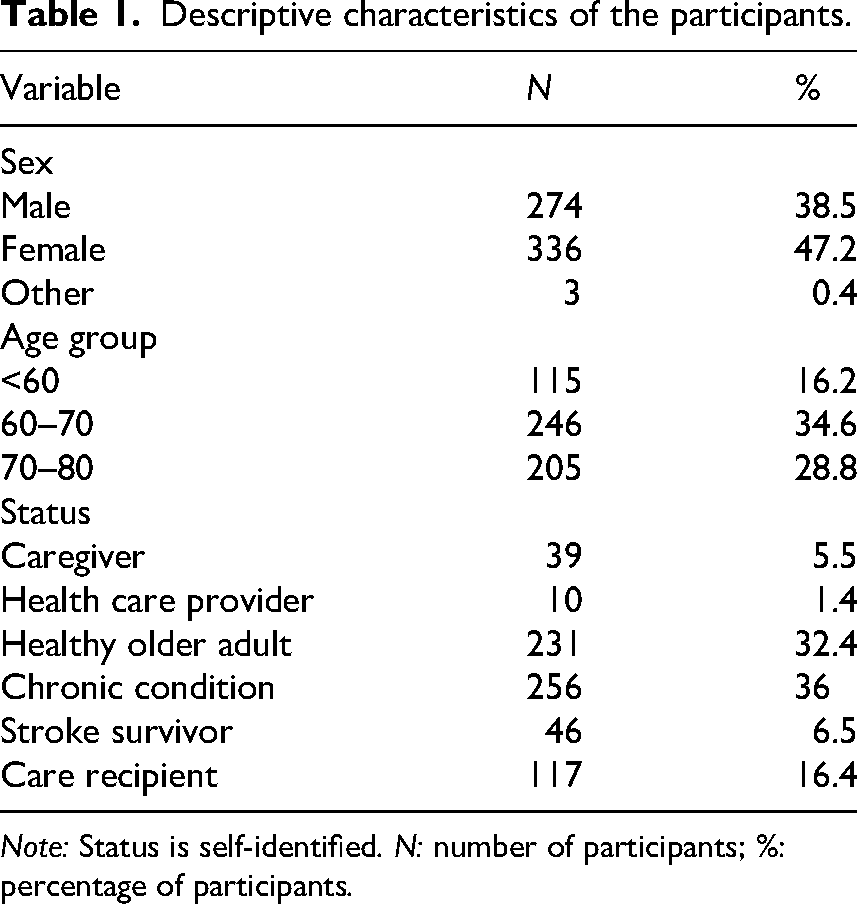
Note: Status is self-identified. N: number of participants; %: percentage of participants.
The mean scores from each scale are shown in Table 2. We did not detect any extreme outliers or impossible values. There were no floor effects, but ceiling effects were observed in all extended ADL scales: Nottingham Extended Activities of Daily Living (38%), short-form Nottingham Extended Activities of Daily Living (72%), Contemporary Extended Activities of Daily Living (60%), and Lawton Extended Activities of Daily Living (77%).
Mean scores across responses to each scale.
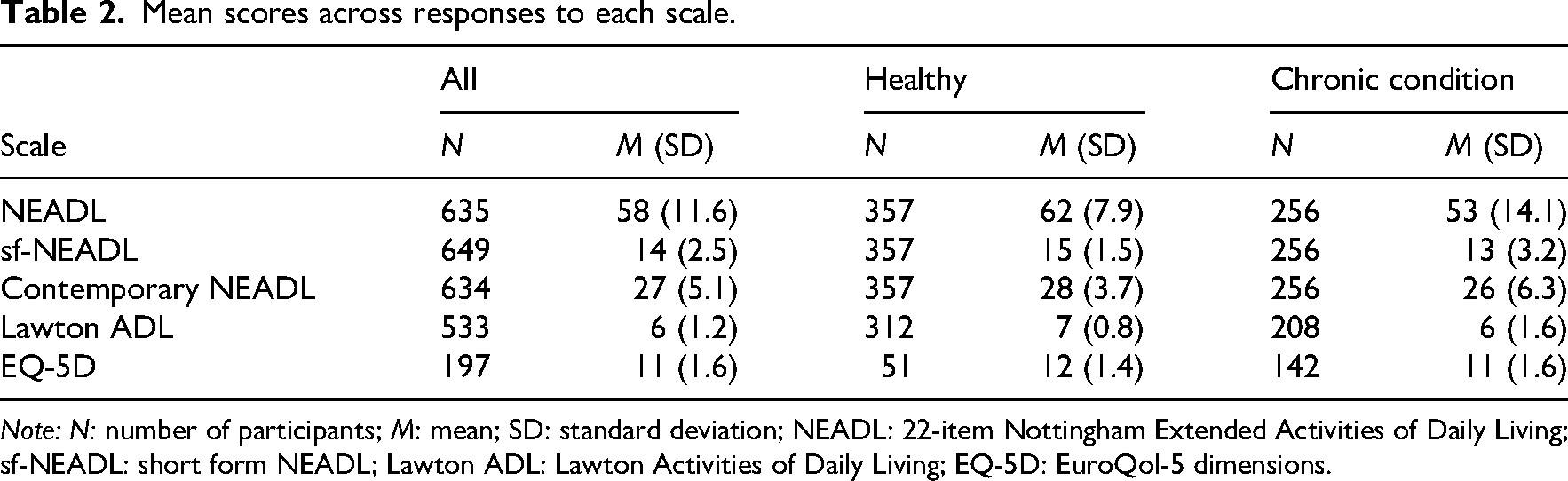
Note: N: number of participants; M: mean; SD: standard deviation; NEADL: 22-item Nottingham Extended Activities of Daily Living; sf-NEADL: short form NEADL; Lawton ADL: Lawton Activities of Daily Living; EQ-5D: EuroQol-5 dimensions.
The short-form Nottingham scale had a good internal consistency (α = 0.84, 95% CI: 0.82–0.86), as did the Contemporary Extended Activities of Daily Living scale (α = 0.88, 95% CI: 0.87–0.89). To compare, the 22-item Nottingham scale had high internal consistency (α = 0.93, 95% CI: 0.92–0.94).
When controlled for attenuation by unknown reliability, the short-form Nottingham scale had excellent concurrent criterion validity, as demonstrated by strong associations with the 22-item Nottingham scale (rs = 0.82, p < .001) and Lawton scale (rs = 0.81, p < .001). As shown in Table 3, each of the contemporary items, as well as the total Contemporary Extended Activities of Daily Living score, were significantly correlated with the 22-item Nottingham scale (rs = 0.78, p < .001).
Concurrent validity of the contemporary Nottingham Activities of Daily Living (NEADL) scale.
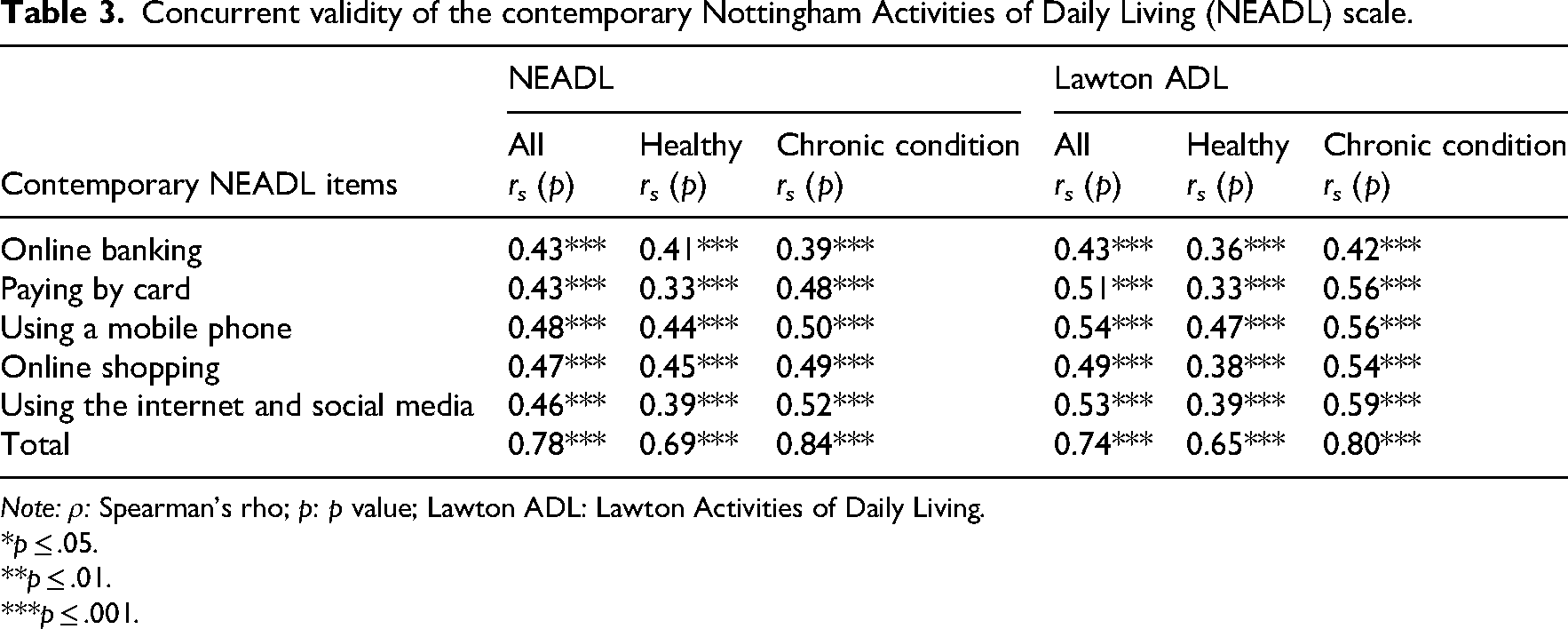
Note: ρ: Spearman's rho; p: p value; Lawton ADL: Lawton Activities of Daily Living.
*p ≤ .05.
**p ≤ .01.
***p ≤ .001.
After controlling for attenuation, there was a moderate association between the short-form Nottingham scale and quality of life. Table 4 shows the correlation coefficients demonstrating good construct validity of the original 22-item Nottingham, short-form Nottingham, and the Contemporary Extended Activities of Daily Living scales.
Construct validity of the Activities of Daily Living scales.
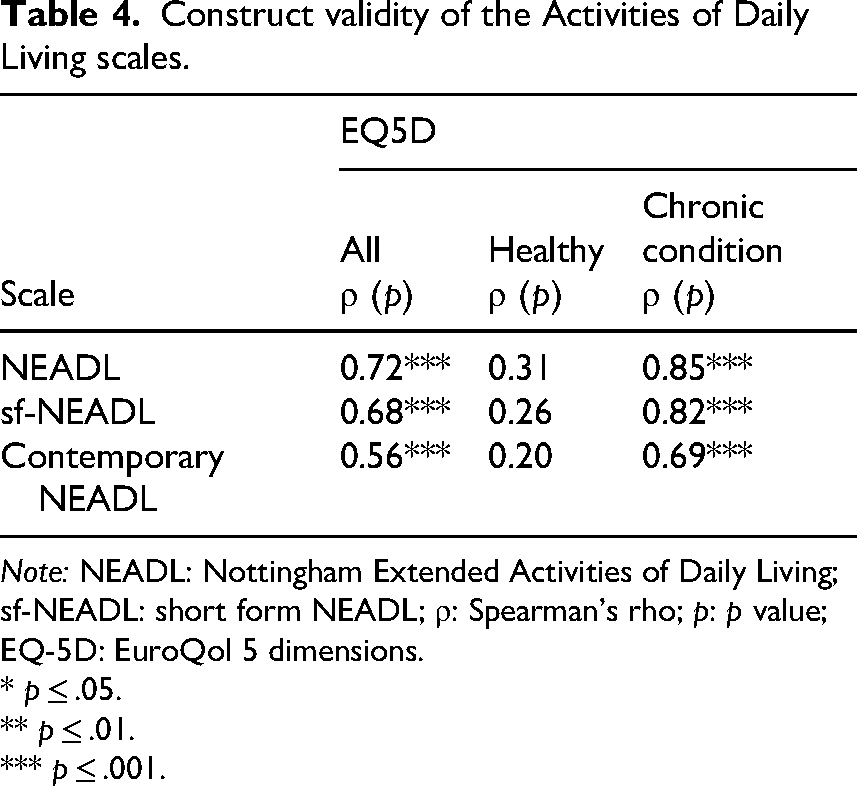
Note: NEADL: Nottingham Extended Activities of Daily Living; sf-NEADL: short form NEADL; ρ: Spearman's rho; p: p value; EQ-5D: EuroQol 5 dimensions.
* p ≤ .05.
** p ≤ .01.
*** p ≤ .001.
Discussion
We assessed the short-form Nottingham Extended Activities of Daily Living and a new Contemporary Extended Activities of Daily Living scale in a large, diverse sample. Although neither scale consistently showed improved psychometric properties compared to the original extended ADL scales, our findings demonstrate that both shorter and more relevant scales can be created without compromising psychometric properties.
Our results agree with the original validation study of the short-form Nottingham scale, but we were able to confirm the scale's external validity in a cohort not exclusively comprised of stroke survivors. 17 This finding supports the use of the short-form Nottingham scale in diverse populations. The lower reliability (internal consistency) seen with the novel extended ADL scales is noted, and is likely to indicate little to no item redundancy previously observed with the original items. 12
We found good criterion validity of the novel contemporary extended ADL scale, albeit with slight variations across individual contemporary items. The items most highly correlated with the Nottingham scale described the use of mobile phone, internet, and social media; while the least valid item was online banking. Notably, Minnis et al. 16 identified online banking and paying by card as the two most common tasks performed by older adult respondents, and in this regard, we note the ceiling effects demonstrated for both novel scales.
While adding contemporary items did not improve the validity of the short-form Nottingham scale, the new scale addresses participant preferences and increases relevance. Perceived relevance of items may be associated with higher willingness to use the scale, and we anticipate that the Contemporary Extended ADL scale will improve completion rates. 39 Thus, although further testing will be required for clinical use, we have demonstrated that functional outcome measures can be improved based on engagement with interest holders.
Construct validity of the contemporary scale and the 5-item short-form Nottingham scale were lower than that of the full Nottingham scale. This does not necessarily imply a problem with the novel scales because, although related, quality of life and functional independence in daily tasks are distinct constructs and therefore a perfect association is not expected. 40 Previous studies have found that quality of life is only moderately correlated with activities of daily living, 13 as opposed to other related constructs, such as the Barthel Index measuring performance in basic ADLs. 41
Across all extended ADL scales, our measures of validity were weaker in healthy participants than in those living with a chronic condition. This is likely due to the ceiling effect present in the healthy group and is not unexpected, as ADL scales were initially developed for people living with disability. 42 Further studies may wish to improve the scale's granularity by adding floor or weighted items. 43
Several limitations should be acknowledged. First, the Contemporary Extended Activities of Daily Living was not administered as a separate scale. Instead, the five contemporary items were combined with the short-form Nottingham scale, which may have hindered independent comparison. This approach was chosen to prevent task fatigue, but future studies should be designed to allow for head-to-head comparisons of novel scales. The wording of the contemporary task questions was not piloted or refined through cognitive debriefing, and there may be scope to improve the question stems. There was a high drop in the number of participants completing the quality of life and short-form Stroke Impact Scale, which were at the end of our battery of assessments. This highlights the importance of keeping scales short while maintaining reasonable psychometric properties. Finally, the Lawton scale was not designed to be administered on the self-report format used in this study.
Despite the limitations, we have evaluated various measurement properties of a shorter and more relevant extended ADL scale. Our sample size was large and included a mixed population living with various long-term conditions, demonstrating the scale's suitability for a wider range of adult users.
In future, validation of the contemporary scale may provide grounds for a shorter and more relevant assessment of functional outcome for older adults. Especially vital for longitudinal follow-up of community-dwelling adults and care home residents, we anticipate that the perceived relevance of a measure will improve the accuracy of response and reinforce engagement. 39 Given the diversity in daily activities and needs, one strictly defined set of tasks is unlikely to achieve consistent perceived relevance. Customisability of extended ADL items to person and circumstance is essential to avoid biases related to individual differences (e.g. disability, gender, and literacy) or temporal changes in activity, which can cause unquantifiable measurement error in research studies and clinical data records.
Future research should account for the availability of care, technology, and gender-related assumptions to create an equitable and accurate measurement of independence in extended ADLs rather than the performance of what is societally determined to be the daily life of an independent person. External validity analyses could clarify clinical utility for specific conditions, while structural validity analyses could elucidate dimensions of updated tests. Improving perceived relevance, while keeping the measurement scale as short as possible, is an integral first step to ensuring the scale's validity and feasibility.
We evaluated the psychometric properties of the short-form Nottingham Extended Activities of Daily Living scale and a novel Contemporary Extended Activities of Daily Living scale. While the new measure did not improve the properties of the original Nottingham scale, it addressed participant preferences and provided the grounds for a shorter and more relevant measure of functional outcome. Future studies are needed to confirm the scale's validity and reliability across differing populations and modes of administration, as well as its suitability for long-term assessment. Assessment of independence in daily tasks is of primary importance to older adults and those living with chronic conditions, therefore the scales used to quantify it should dynamically adapt to the circumstances and needs of the end users.
Footnotes
Acknowledgements
We would like to kindly thank Join Dementia Research for their support and role in recruiting volunteers for this study.
Ethical approval
The present study was approved by the University of Glasgow Medical, Veterinary and Life Sciences Ethics Committee (application number 200210164).
Consent to participate
Participants provided informed consent prior to participation.
Author contribution
All authors contributed according to ICMJE guidelines. KM: conceptualisation; data curation; investigation; methodology; project administration; writing–original draft; and writing–review and editing. LT: data curation; formal analysis; methodology; writing–original draft, and writing–review and editing. TJQ: conceptualisation; supervision; and writing–review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work for this study was funded by the European Union as a part of the Horizon Europe research initiative RES-Q + (grant number 101057603). Views and opinions expressed are, however, those of the authors only and do not necessarily reflect those of the European Union or the Health and Digital Executive Agency. Neither the European Union nor the granting authority can be held responsible for them.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
In response to the risk of triangulation of identity of participants in less densely populated areas, the dataset collected for this study is deposited in a closed record (![]() ). The analysis was pre-registered (doi: 10.17605/OSF.IO/RWTHN), and the code used has been made openly available (doi: 10.17605/OSF.IO/FYW5G).
). The analysis was pre-registered (doi: 10.17605/OSF.IO/RWTHN), and the code used has been made openly available (doi: 10.17605/OSF.IO/FYW5G).