
Abstract
Objective
To identify and prioritize personal risk factors for pressure injuries in wheelchair users.
Design
A Delphi survey was conducted with clinicians specializing in pressure injury prevention and care.
Setting
The study was conducted online using LimeSurvey software.
Participants
In the first round, 90 clinicians participated and completed the survey; in the second round, 68 continued their involvement.
Results
Across all rounds, 39 risk factors were identified by the experts. These factors were weighted according to expert consensus. Immobility, current or past pressure injuries, malnutrition, and sensory perception impairment are ranked among the highest important.
Conclusion
These findings underscore the importance of considering both physiological and behavioral factors when assessing pressure injurie risk. The weighted list of expert-validated factors offers clinicians a practical foundation for more targeted and individualized prevention strategies, ultimately supporting improved care and quality of life for this population.
Introduction
Pressure injuries represent a significant economic burden on health care systems worldwide. In the United States, annual costs are estimated at between US$9 billion and 26.8 billion,1,2 while in Australia, annual costs reach AU$9.11 billion. 3 The UK spends £1.4 billion to £2.1 billion annually on pressure injuries. 1 Treatment costs vary by severity, ranging from £1214 for category 1 to £14,108 for category 4 pressure injuries in the UK. 4 The economic impact of pressure injuries is influenced by patient characteristics, comorbidities, and procedures, generating costs per patient varying from US$4400 to US$24,000 in the US. 5
Among the population of wheelchair users, the occurrence of pressure injuries varies from 17.9% to 58.0%, depending on the specific population studied,6–8 making them a major concern for clinicians who work with them. Since the occurrence of pressure injuries is linked to both external and personal factors, 9 gaining a better understanding of the personal risk factors is essential. It is well known that the presence of multiple personal risk factors can not only add pressure injuries’ effects but also amplify the danger, creating a unique and more significant risk factor for patients. 10
In clinical practice, it is essential for clinicians to evaluate the personal risk of pressure injury occurrences for each wheelchair user to tailor their care accordingly. However, the most common predictive tool, the Braden Scale, 11 does not account for all personal risk factors. It includes sensory perception, moisture, activity level, mobility, and nutritional status. Other important factors, such as advanced age, obesity, initial diagnosis (e.g. cancer or spinal cord injury), medications, and cardiac impairments, are not included. 10 This limitation aligns with the current use of the Braden Scale, as it is primarily applied during hospital stays, under specific health conditions and medical supervision. For wheelchair users, who are at great risk of pressure injuries, 7 the challenge is different. They need to live independently in their communities, without constant medical monitoring. Therefore, they need tools that empower them to self-monitor with a more holistic view of their personal risk factors.
For both clinical and research purposes, it is crucial to accurately assess each patient's risk level, particularly for wheelchair users. In clinical practice, this allows health care providers to individualize care plans, prescribing appropriate adaptive equipment – such as pressure-relieving cushions, back supports, or other assistive devices – based on a patient's specific risk factors. 12 Moreover, it enables clinicians to deliver targeted therapeutic education, helping patients and caregivers understand how to manage these risks in daily life, thereby improving long-term outcomes and preventing complications like pressure injuries. From a research perspective, accurately assessing patient risk profiles is essential to properly classify participants in studies, ensuring that therapeutic interventions are tested on well-defined subgroups of patients. This precision not only improves the relevance of research findings but also helps to identify which populations – such as wheelchair users with specific risk profiles – are most likely to benefit from particular interventions. Consequently, a more accurate assessment supports more evidence-based recommendations for clinical practice and the development of more effective prevention and treatment strategies. 13 Therefore, our long-term goal is to assess the level of risk for wheelchair users of developing pressure injuries. To achieve it, we first aimed to assign weights to personal risk factors for pressure injuries.
Materials and methods
Study design
Since the literature does not provide sufficient guidance on this issue, 10 we chose to consult experts using the Delphi survey method. Full ethical approval for this study was obtained from the Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale Research Ethics Committee (#2024–3017).
The Delphi study was conducted in alignment with international methodological standards. 14 This approach is commonly used to facilitate informed decision-making in health care 14 and aims to reach a consensus among ‘experts’ on a particular topic through multiple rounds of questionnaires.15,16 After each round, the experts’ responses were analysed, and a summary of the findings was shared with them for the next round. 14
Development of the survey
A bilingual (French and English) online survey was created using LimeSurvey (LimeSurvey GmbH, URL: http://www.limesurvey.org). For the first round, the survey included sociodemographic questions, all the risk factors identified in the literature, 10 to be rated on a scale from 1 to 9 (with 1 representing a very low impact and 9 representing a major impact), and a question to identify any unlisted risk factor that a participant might think is important. For subsequent rounds, except for the sociodemographic questions, the remaining questions were based on the results from the previous round (as described in the study analysis section), without open questions.
Participant profiles and dissemination
We initially expected 60 participants, with an anticipated attrition rate of less than one-third in each subsequent round. Participants were eligible if they had experience with wheelchair users and pressure injuries, and if they had a medical or paramedical background (e.g. physicians, occupational therapists, physiotherapists, nurses, and orthotists/prosthetists). The online survey was distributed through the authors’ national and international networks, including established clinical and community partnerships in Canada and France. The authors worked with organizations such as the Association Nationale Française des Ergothérapeutes (French Association of Occupational Therapists), the Société Française des Escarres (French Pressure Injury Society), the Association Positi’F-Mobilité (French Seating and Positioning Association), the Ordre des Ergothérapeutes du Québec (Quebec College of Occupational Therapists), the Ordre des Physiothérapeutes du Québec (Quebec College of Physiotherapists), AGE-WELL Canada's Technology and Aging Network (AGE-WELL), and the Rehabilitation Engineering and Assistive Technology Society of North America (RESNA). The survey was also disseminated via personalized and general email invitations (including the Centre Intégré Universitaire de Santé et de Services Sociaux de la Capitale-Nationale, the European Seating Symposium Network, and the National Pressure Injury Advisory Panel Network), social media platforms, and word of mouth. Only respondents from the first round were invited to participate in the subsequent rounds.
Analysis
For data analysis, the arithmetic mean, standard deviation, median, first quartile (q1), third quartile (q3), and interquartile range (q1–q3) were calculated based on the 1–9 weight score the experts assigned to each factor. A consensus was considered to have been achieved when the interquartile range was less than or equal to 2. 17 Risk factors that did not reach consensus were not included in the next round. When consensus was reached, if a risk factor's median was less than or equal to 3, it was deemed unimportant and excluded from the next round. After the first round, all additional risk factors the participants identified were classified and reformulated by the research team before being added to the survey. Risk factors were continuously evaluated by respondents in subsequent rounds until they met the interquartile range threshold of 2 for consensus.
Weight calculation methods for the scoring propositions
Since we plan to develop a scoring system in the future – based on the sum of each factor multiplied by its weight – we explored two approaches for the calculation of the final weight, given the exploratory nature of this work. The first is a simple method that uses the mean weight assigned to each factor. To refine the weighting scale and better reflect the relative importance of each selected factor, we transformed the initial weight range from 3 to 9 (weight range obtained from the experts’ rating of the selected factors) to a new scale ranging from 1 to 10. After adjusting the scale, we calculated the mean weight for each selected factor, providing a clearer assessment of its importance, according to the experts.
18
The second method was designed to account for variations in consensus levels and differences in the number of respondents, which we felt should be reflected in the weight calculation. To account for both the variability of responses and the number of respondents, we modified the first method by adding an adjustment step. In this step, we subtracted each factor's initial standard deviation (calculated from the raw data), divided by the number of respondents, from its mean weight. This correction minimized the impact of variability in responses and further refined the final weight for each factor.
Results
Participants
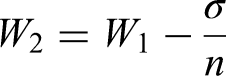
The first round of recruitment took place between 26 August 2024 and 3 October 2024. A total of 90 clinicians participated: 20 men and 70 women (Table 1). A diverse group of professionals took part: occupational therapists, physical therapists, physicians, nurses, and prosthetists. The participants had a mean age of 41.7 ± 10.2 years and a mean of 17.3 ± 10.0 years of professional experience, including 15.0 ± 10.0 years working with wheelchair users. All of them came from North America or Europe, with the highest numbers from Canada and France. Regarding their frequency of involvement in pressure injury management, three-quarters of them (76%) reported being involved very often or often. Thus, overall, this was a group with plenty of experience in the area.
Participants’ sociodemographic data.
The second round of recruitment occurred between 7 October 2024 and 29 October 2024, with 68 clinicians participating (Table 1): 17 men and 51 women, from the same professions and the same geographic areas as in the first round. This group's age was 41.3 ± 10.7 years, and they had a mean of 16.8 ± 10.2 years of professional experience, including 15.0 ± 10.0 years with wheelchair users; 78% of them reported being involved with pressure injury management very often or often. This group's experience level was therefore equivalent to the first group's.
Weight identification
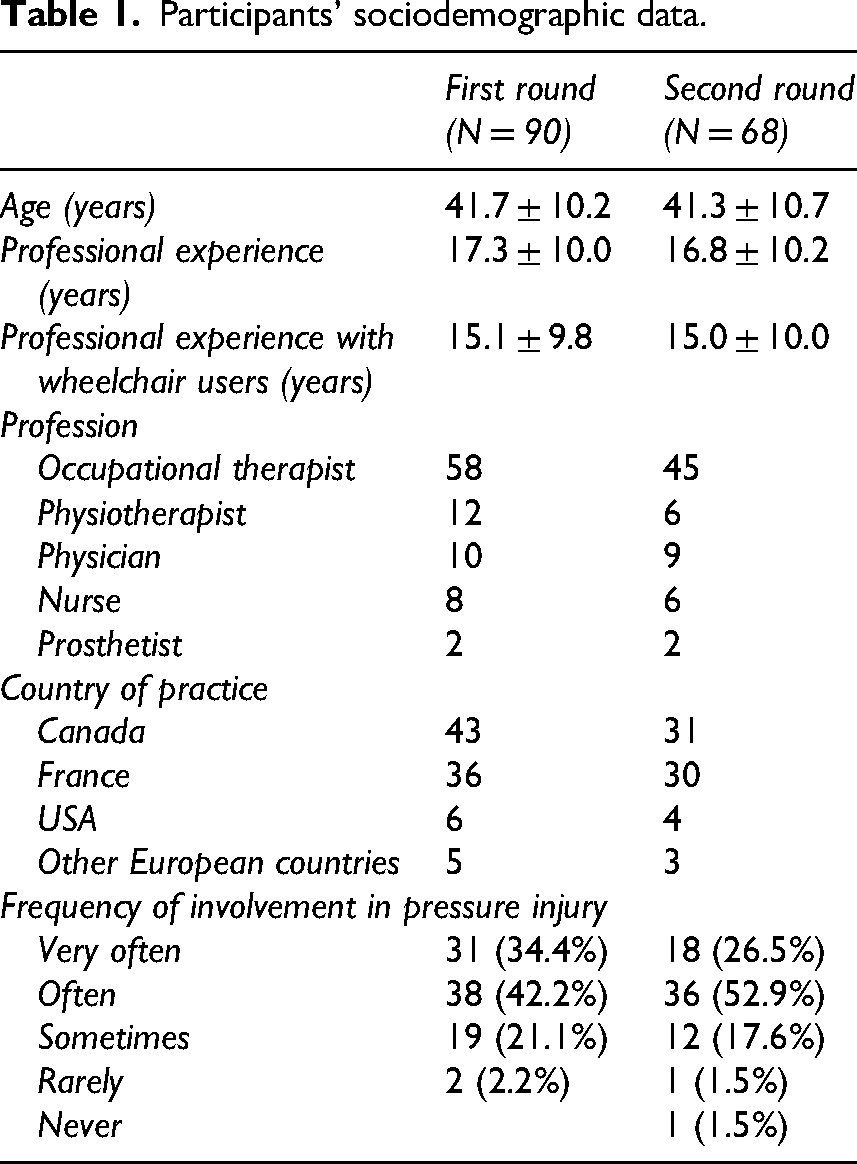
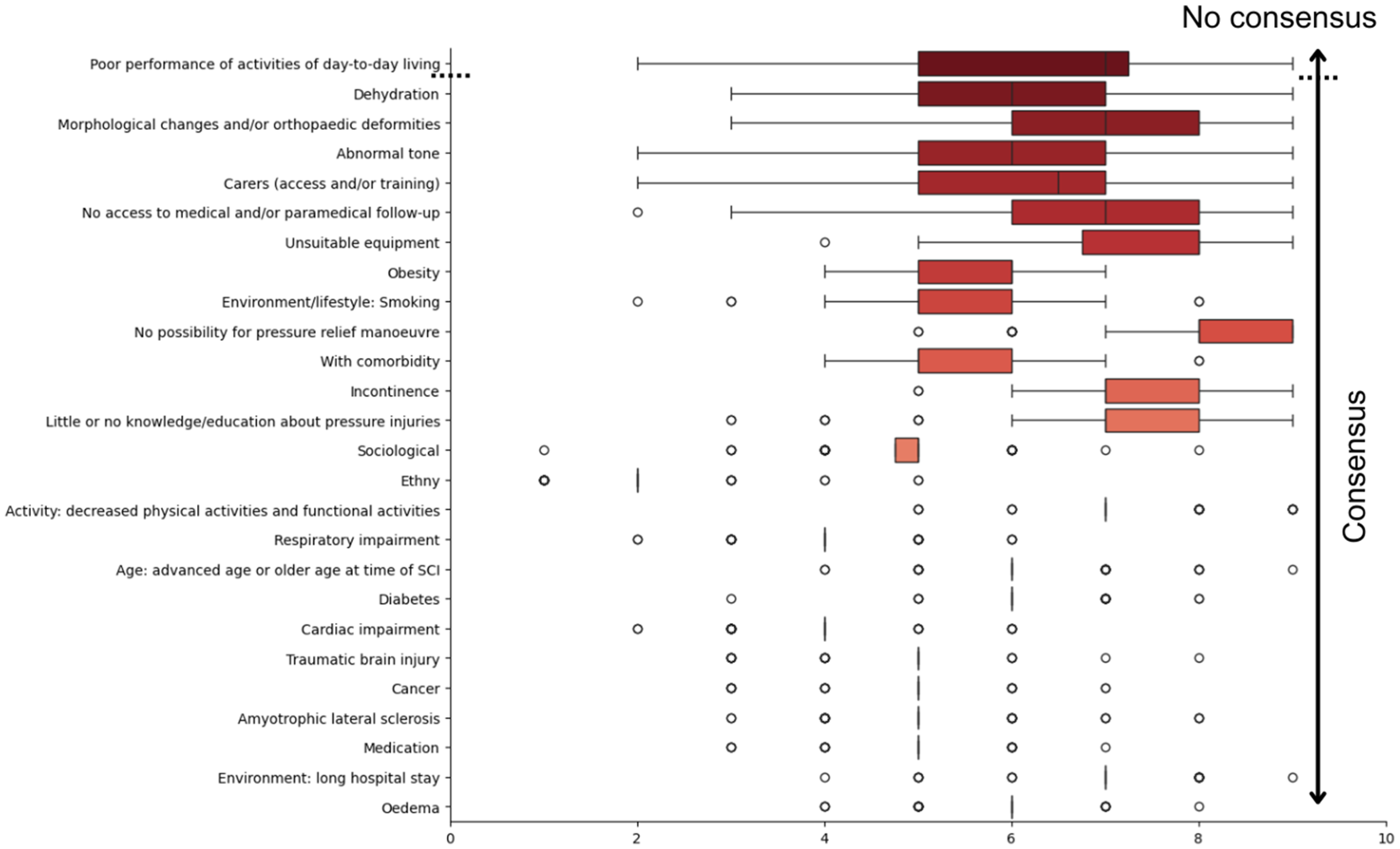
In the first round, we assessed the importance of 32 factors from the literature. Consensus was reached for 15 factors: quality of the skin; sensory perception impairment; vascular impairment; altered behaviour, vigilance and cognition; spinal cord injury: time since the injury; spinal cord injury: level; spinal cord injury: completeness; spinal cord injury: autonomic dysreflexia; hyperthermia and/or infection; specific type of nutrition; spinal cord injury status; immobility; current or previous pressure injury; and malnutrition. One factor, gender, did not meet the predefined importance threshold of 3 (Figure 1). Additionally, nine new factors were proposed: no access to medical and/or paramedical follow-up; little or no knowledge/education about pressure injuries; carers (access and/or training); unsuitable equipment; abnormal tone; morphological changes and/or orthopaedic deformities; dehydration; no possibility of pressure relief manoeuvres; and poor performance of activities of daily living.
Box plot of each factor's weight classified by the interquartile range q1–q3, with the median; from the first round of the Delphi process.
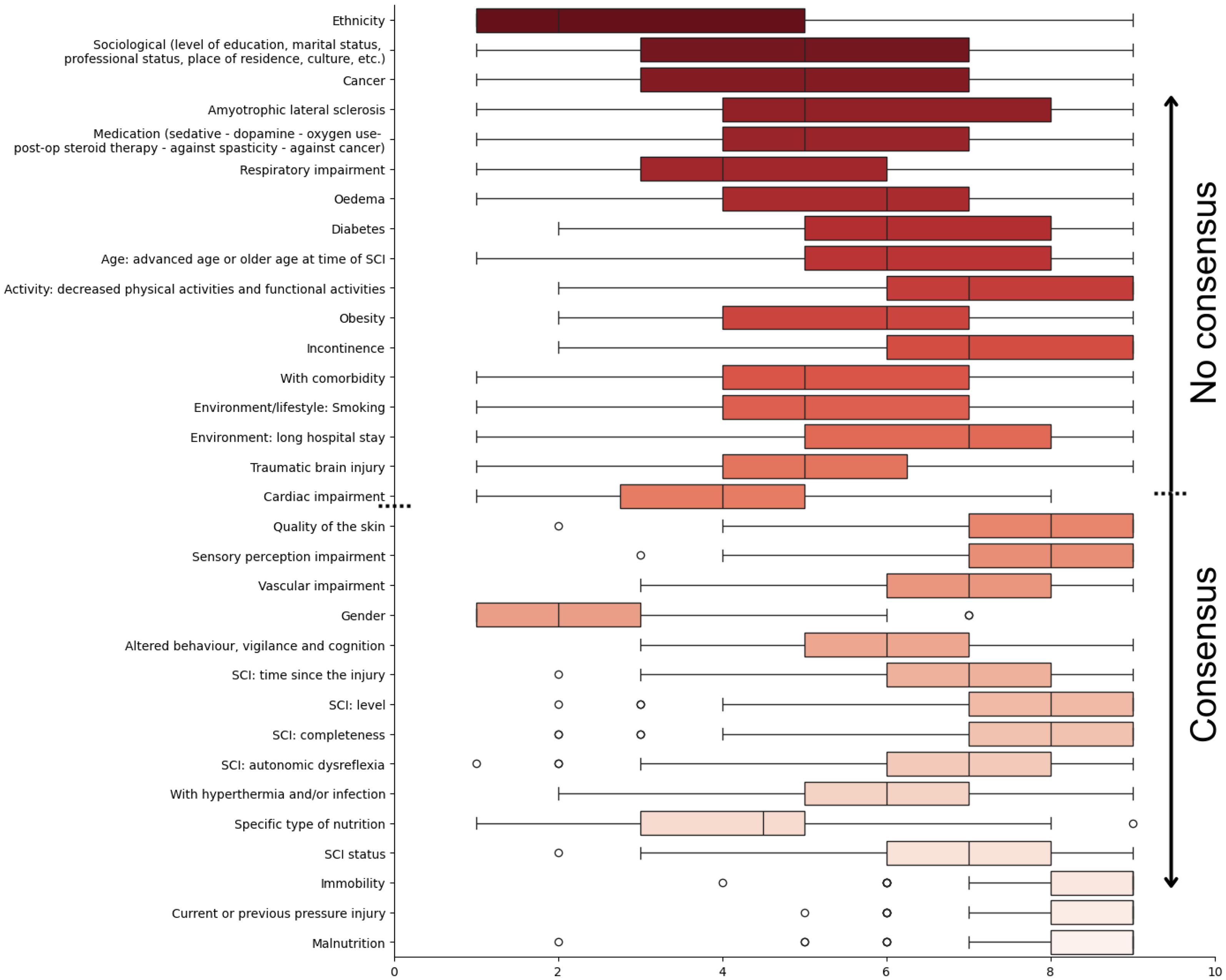
In the second round, 26 factors were reviewed: 17 from the literature and 9 additional ones from the first round. Of these, all but one (ethnicity) reached the importance threshold. Of the 26 factors proposed during this round, only one, poor performance in activities of daily living, failed to reach consensus. Because this factor overlapped with ‘activity: decreased physical activity and functional activity’, it was removed from further analysis (Figure 2). As all remaining factors – except one with a low mean weight – reached the expected consensus threshold, a third round was not conducted.
Box plot of each factor's weight classified by the interquartile range q1–q3, with the median, from the second round of the Delphi process.
Across both rounds, a total of 39 factors achieved consensus. Given that some factors are specific to individuals with spinal cord injury, two lists were created: factors applicable to all wheelchair users (34 factors) and factors specific to wheelchair users with spinal cord injury (33 factors). The weight of each factor was normalized to a 1-to-10 scale while preserving the original standard deviation (Figures 3 and 4). The five most critical factors common to both lists, with normalized mean weights between 8 and 9, were immobility (9.01 ± 0.98), current or past pressure injury (8.81 ± 0.94), malnutrition (8.50 ± 1.21), no possibility of pressure relief manoeuvre (8.26 ± 1.09) and sensory perception impairment (7.98 ± 1.30).
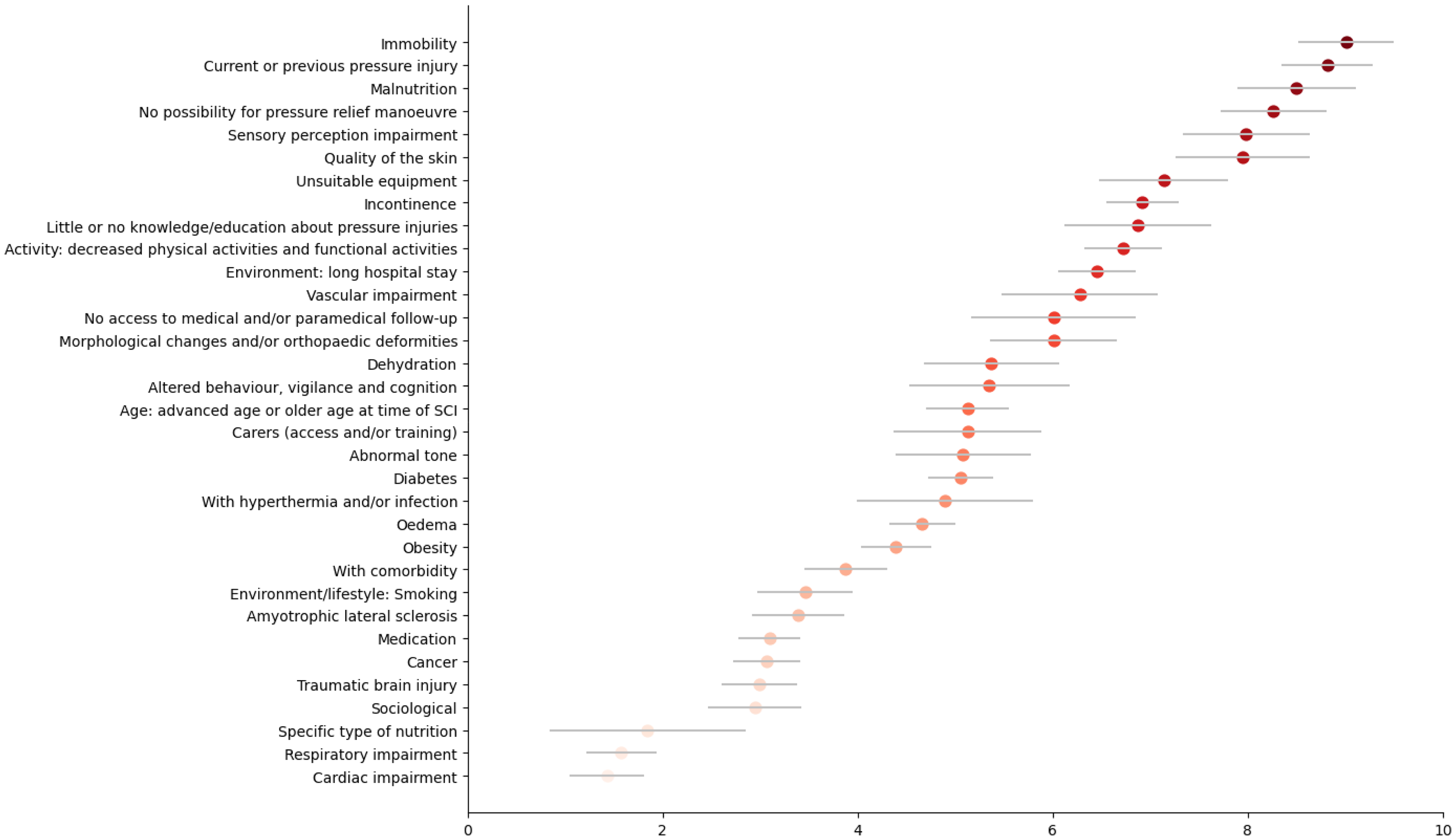
Point plot (normalized mean with original standard deviation) of the weight of each factor assigned by the experts, for wheelchair users without spinal cord injury.
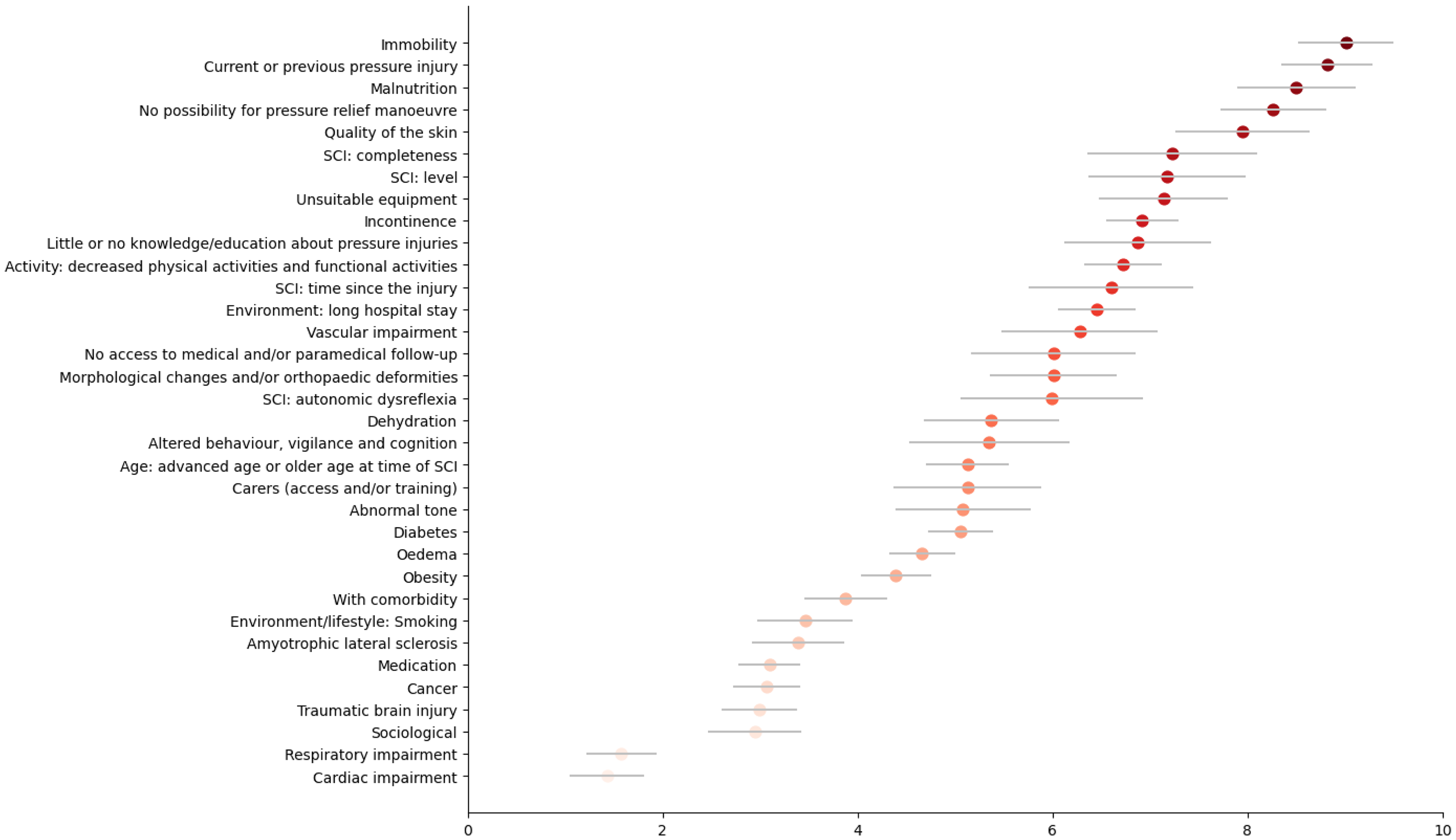
Point plot (normalized mean with original standard deviation) of the weight of each factor assigned by the experts, for wheelchair users with spinal cord injury.
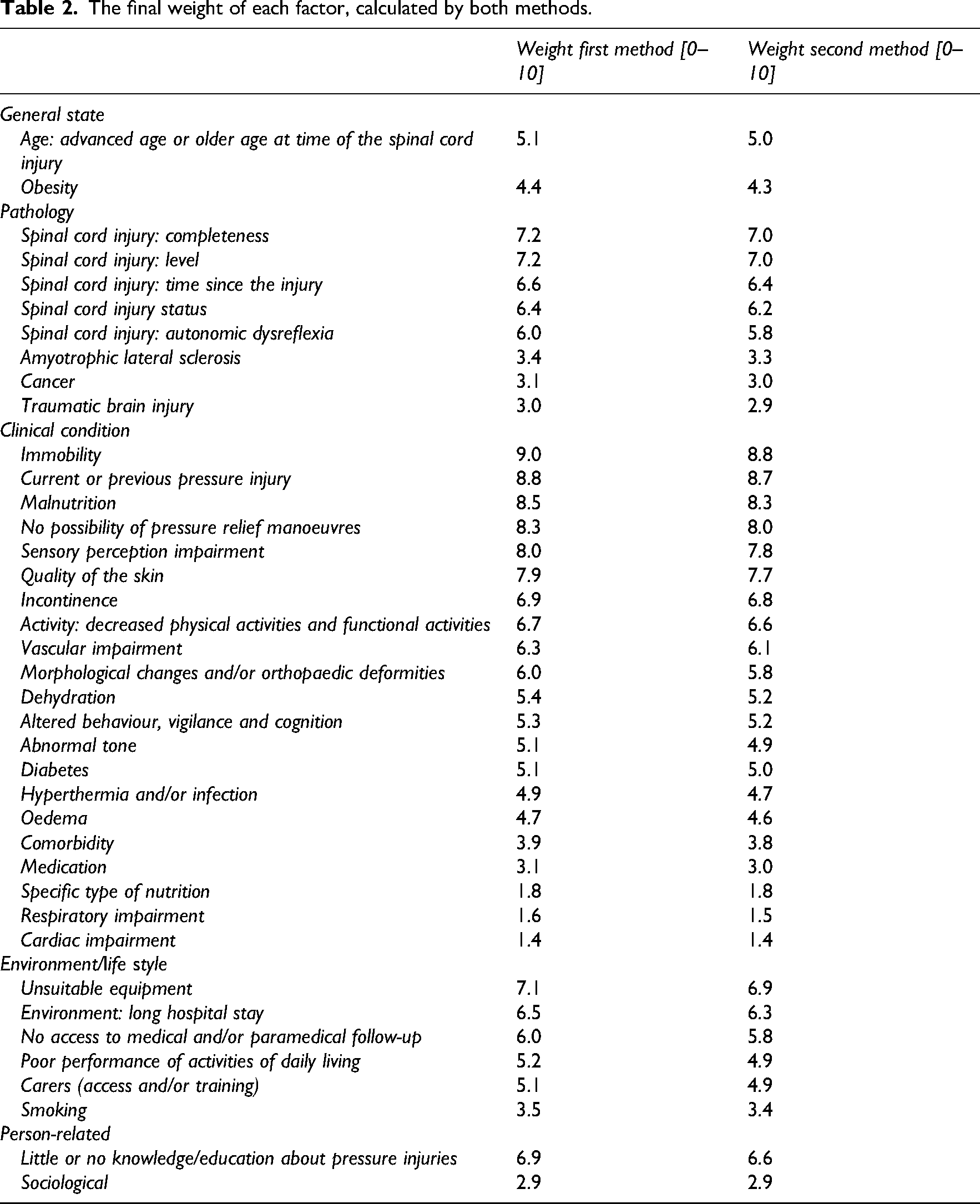
Based on the analysis of the weighting factors, the average weight across the 39 factors was 5.49 ± 1.99 using the first method and 5.34 ± 1.94 using the second method (Table 2).
The final weight of each factor, calculated by both methods.
Discussion
This study presents a clinically grounded and expert-informed framework for assessing pressure injury risk in wheelchair users, identifying 39 relevant factors and establishing their relative importance through a structured Delphi process. The findings reflect the multifactorial nature of pressure injury development and benefit from the input of a diverse panel of experienced clinicians. By assigning weights to each factor, the study goes beyond simple identification to offer a prioritized risk profile, enhancing its applicability in clinical decision-making. While geographic and professional representation was somewhat limited, the rapid consensus and inclusion of underreported factors strengthen the clinical relevance of the results.
To better understand the foundation of these findings, it is important to consider the demographic and professional profiles of the participating experts. The sample included a diverse and experienced group of clinicians involved in pressure injury management for wheelchair users. The high proportion of occupational therapists and physiotherapists reflects the central role these professionals play in this area for the population of wheelchair users. Participants’ mean professional experience of 17 years, including 15 years working with wheelchair users, underscores their great expertise and lends credibility to the findings. Similar to previous studies highlighting the importance of experienced care teams in preventing pressure injuries,6,7 this study emphasizes the critical role of clinician expertise.
The geographic distribution – mainly from Canada, France, and the United States – provides a cross-cultural perspective, though the relatively smaller representation from other regions may limit generalizability to a global context. Experts were specifically selected for their experience with wheelchair users, a population with distinct clinical needs. While not all participants were in regular contact with pressure injuries, their expertise in wheelchair user care was considered sufficient to contribute meaningfully to the Delphi process. Moreover, the frequency of involvement in pressure injury management among many participants reinforces the relevance of the insights gathered. Importantly, because the expert panel was well-balanced in terms of both professional expertise and geographic representation, the fact that consensus was reached within two Delphi rounds should not be considered a limitation.
The study successfully identified 39 factors associated with pressure injury risk in wheelchair users, with consensus achieved across the two rounds. The factors encompass a comprehensive range of physiological, behavioural, and contextual elements, reflecting the multifactorial nature of pressure injury development, consistent with prior findings that the physiopathology of pressure injury is complex and relies on various factors.1,9 The inclusion of new factors proposed by participants, such as ‘no access to medical and/or paramedical follow-up’ and ‘little or no knowledge/education about pressure injuries’, highlights the value of expert-driven Delphi processes in capturing clinically relevant nuances that may be underrepresented in existing literature.14,16
The division of factors into two lists – one applicable to all wheelchair users and another specific to those with spinal cord injury – ensures that the unique needs of the spinal cord injury subpopulation are addressed. For instance, factors such as ‘spinal cord injury: level’ and ‘spinal cord injury: completeness’ are critical considerations for patients with spinal cord injury but less relevant for other wheelchair users. This distinction aligns with current clinical guidelines emphasizing personalized care approaches. 13
The normalized weighting of factors provided a clear ranking, with ‘immobility’, ‘current or past pressure injury’, ‘malnutrition’, ‘no possibility of pressure relief manoeuvres’, and ‘sensory perception impairment’ emerging as the most critical. These results are consistent with the literature, which identifies these factors as significant contributors to pressure injury risk. 10 For instance, immobility and sensory perception impairment are well-documented primary risk factors due to their direct impact on pressure redistribution and tissue health. 9 Interestingly, factors related to behavioural and contextual aspects, such as ‘no access to medical and/or paramedical follow-up’ and ‘little or no knowledge/education about pressure injuries’, also achieved consensus. This underscores the importance of addressing systemic and educational barriers alongside physiological risk factors in comprehensive pressure injury prevention strategies. 19
The Delphi method proved effective in facilitating consensus among a diverse group of clinicians. The iterative process allowed factors to be refined and ensured that the final list reflected both evidence-based practices and expert opinion. Similar to previous research utilizing the Delphi method,20,21 this study demonstrates its utility in health care quality improvement initiatives. However, some limitations should be acknowledged. The geographic concentration of participants in North America and Europe may have introduced cultural or systemic biases, as health care practices and resource availability differ globally. Additionally, the relatively lower representation of certain professions, such as nurses, who are usually very involved in working with wheelchair users, may have limited the diversity of perspectives.
The findings of this study have significant implications for clinical practice. The ranked factors provide a structured framework for clinicians to systematically assess pressure injury risk in wheelchair users. The dual lists of factors enable tailored risk assessment for spinal cord injury and non-spinal cord injury populations, enhancing the precision of preventive interventions. These findings align with recommendations in existing clinical guidelines for pressure injury prevention and treatment. 22 Moreover, the identification of systemic and educational barriers emphasizes the need for multidisciplinary approaches that extend beyond clinical settings to include caregiver training, patient education, and health care policy improvements. 22
As previously stated, our long-term goal is to develop a scoring system based on this study's findings. Since both weight calculation methods gave similar results, in future work we will choose the simpler method (first method), consisting of normalizing the mean weight attributed by experts. The next step will be to test this score in clinical practice and compare it with expert clinicians’ subjective assessments and the gold standard, the Braden Scale. 11
Clinical messages
Pressure injury risk is influenced by a combination of physiological, behavioral, and environmental factors.
Effective prevention requires a comprehensive approach that extends beyond clinical interventions to include patient education and systemic support.
Applying these findings in practice can help reduce pressure injury risks and improve the quality of life for wheelchair users.
Footnotes
Ethical considerations
Full ethical approval for this study was obtained from the Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale Research Ethics Committee (#2024–3017).
Consent to participate
Consent information and forms were obtained online with the survey, as described in the ethical form validated by the Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale.
Consent for publication
Not applicable.
Authors’ contributions
Clémence Paquin: designing the study, data collection, and data analysis and writing. François Routhier: designing the study, and writing and funding. Marie-Ève Lamontagne: designing the study and writing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the Ministère de l’économie, de l’innovation et de l’énergie du Québec and by the Réseau d’évaluation et de l’innovation en santé durable du Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale du Québec. Moreover, Clémence Paquin received a postdoctoral Mitacs Accelerate Fellowship and François Routhier is an FRQS Senior Research Scholar.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data are available from the corresponding author on reasonable request.