
Abstract
Objectives
The primary objective was to gain insight into the lived experiences of using day-to-day strategies to manage post-stroke fatigue.
Design
Qualitative, descriptive study.
Setting
Community telephone interviews.
Participants
A purposive sample of 20 stroke survivors with current, or previous, post-stroke fatigue, and 8 caregivers, who provided informal care or support, were recruited.
Main Measures
Semi-structured telephone interviews were undertaken. Data were analysed using a framework approach.
Results
Most participants had found their own ways of coping and their personal strategies included acceptance of having fatigue; ‘pacing’ (spreading activities out and interspersing with rest periods); keeping a diary in order to plan activities and to identify ‘trigger’ activities which induced fatigue; talking to (and educating) others about having fatigue; using relaxation; and accessing professional advice and support. The burden placed on caregivers was considerable and they often had to oversee the post-stroke fatigue management strategies used.
Conclusions
Post-stroke fatigue is managed in different ways and there was not one particular strategy that seemed effective for everyone. Most people in our study had had to devise their own ways of coping practically. Given the scale of this problem, which profoundly impacts the lives of both stroke survivors and caregivers, the management of post-stroke fatigue merits more attention and evaluation. However, this must be directly informed by those with lived experience.
Introduction
Despite advances in many areas of stroke rehabilitation, relatively little progress has been made in the management of post-stroke fatigue. Post-stroke fatigue affects almost half of those who survive a stroke1,2 and is best described as overwhelming exhaustion or tiredness, not related to exertion, which does not typically improve with rest. 3
Yet, despite its prevalence, there is little rigorous research about the factors that might improve post-stroke fatigue or research about the personal strategies used by people with lived experience of post-stroke fatigue. Several comprehensive reviews1,4 and Cochrane systematic reviews5,6 have been unable to draw clear conclusions about management because of issues around the definition of post-stroke fatigue, small sample sizes and weak trial design. Consequently, current clinical practice guidelines rely on low levels of evidence, notably expert consensus which is often generated predominantly by healthcare professionals rather than from those living with the condition (e.g. from the Royal College of Physicians, London 7 from Canadian guidelines 8 ). Post-stroke fatigue, therefore, continues to be an ongoing international research priority 9 and it is listed fourth in the top 10 UK priorities for stroke rehabilitation and long-term care research. 10
This qualitative study was part of a larger study by the Nottingham Fatigue Stroke Study (NotFAST2) which sought to examine the management of post-stroke fatigue pragmatically from a range of perspectives. 11 The objective of this specific phase of NotFAST2 was to explore the management of post-stroke fatigue by those living day to day with it, namely stroke survivors with post-stroke fatigue and those providing support or informal care for them. Previous recommendations have evolved based on clinical consensus, but have not been informed by those with lived experiences. We wanted to explore their personal narratives of managing post-stroke fatigue and collective experiences and strategies to inform the design of future management programmes.
Methods
Ethical approval for the study was granted by the University of Nottingham Faculty of Medicine Research Ethics Committee (Reference 480-2001) on 10 March 2020. Stroke survivor interviews occurred between May 2020 and April 2021. Caregiver interviews occurred between April 2021 and July 2021. We followed the Consolidated criteria for reporting qualitative research (COREQ) 12 .
We wanted to explore the practical lived experience of those managing post-stroke fatigue. We were interested in the real-life context of fatigue beyond the clinical aspects. We, therefore, wished to recruit people with current post-stroke fatigue, or who had had post-stroke fatigue previously, and people who currently or previously provided informal support or care for someone with post-stroke fatigue (we refer to these individuals hereafter as ‘care-givers’). We included caregivers because previous research has demonstrated the impact of post-stroke fatigue on their own lives. 1
Our primary recruitment strategy was using social media, and particularly Twitter, to ask people to contact the team if they were interested in participating or to signpost others to the study. The UK Stroke Association, Different Strokes and UK Stroke Assembly also promoted the study via blogs and through their own networks, to encourage their members to contact us. We also circulated posters advertising the study through these networks and directly to stroke clubs who requested this.
Our inclusion criteria were that participants were over 18 years, able to give informed consent, UK-based, English-speaking and able to participate in an interview. Stroke survivors had to have, or have experienced, self-identified fatigue at any point following a diagnosis of stroke. Caregivers had to provide, or have provided, informal practical and/or emotional care or support to someone with post-stroke fatigue.
To capture an even spread of participants, in terms of demographics and clinical characteristics, we undertook purposeful sampling. 13 Our sampling frame considered age, gender, ethnicity, geographical location, employment situation and time since stroke. We also actively included participants with aphasia and provided extra time, breaks and illustrated literature and support to facilitate this participation. The overall aim was to recruit approximately 20 people with post-stroke fatigue and 10 caregivers, which would provide sufficient data to address our aims 14 and offer conceptual depth 15 for a framework analysis.
Interested parties were sent a participant information sheet and consent form electronically. Consent was taken either verbally (and recorded as a part of the interview), or participants completed the consent form and returned it electronically before the interview. All were given the opportunity to ask questions either via email or telephone prior to participating.
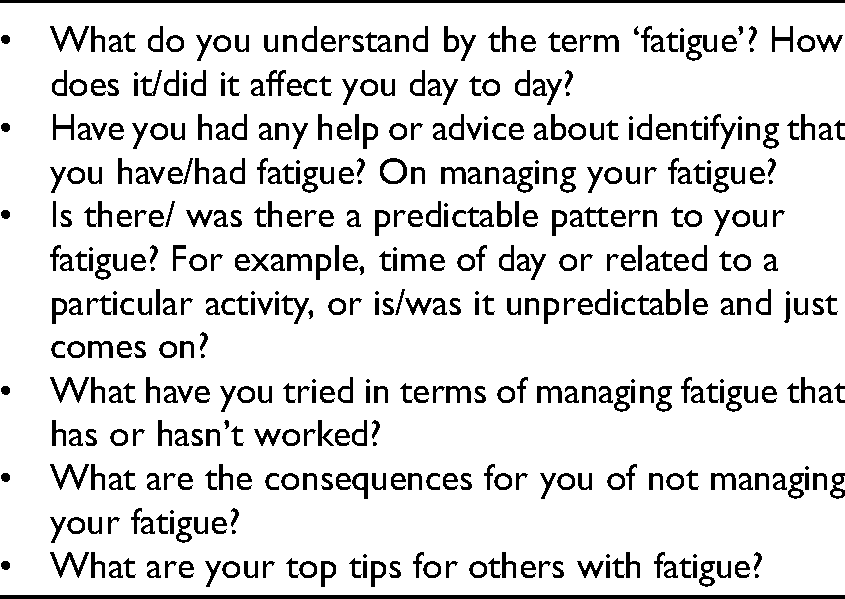
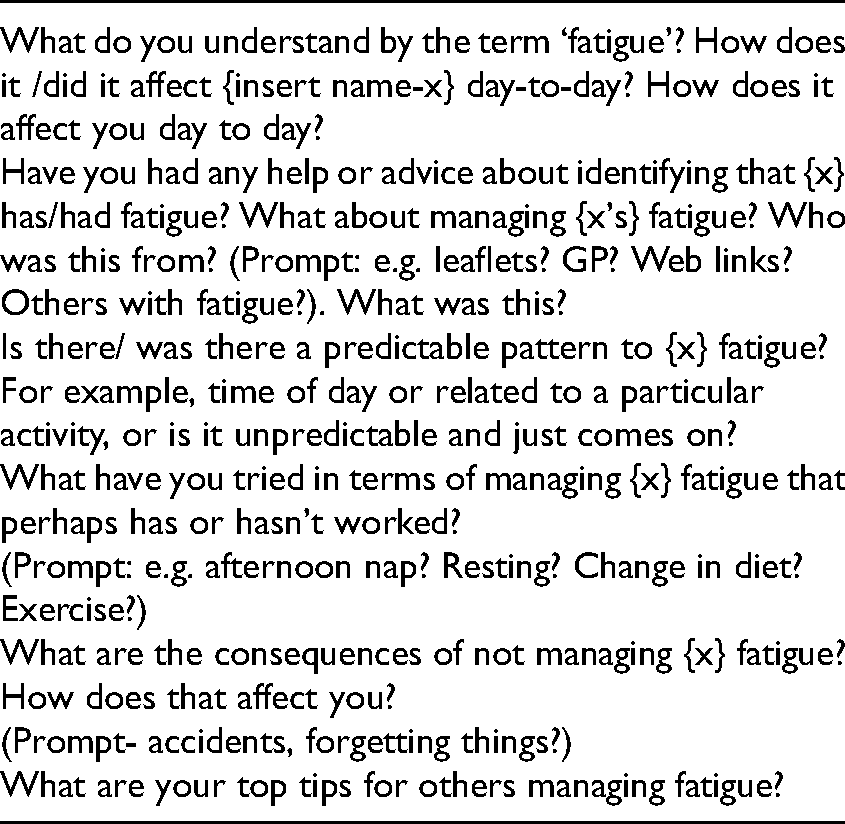
A semi-structured interview guide was developed to explore the lived experiences of post-stroke fatigue and personal strategies for managing. See Table 1 for the interview guides for stroke survivors and Table 2 for caregivers. The guides were based on a recent scoping review, 4 previous research on the experiences of having post-stroke fatigue 16 and input from the research study team and Patient and Public Involvement and Engagement (PPIE) members, all of whom had post-stroke fatigue. The questions were framed in such a way as to gain insights into day-to-day coping and how knowledge and solutions were gained by individuals. All interviews were conducted via telephone, due to the COVID-19 pandemic and the social distancing restrictions in place at the time of the study, video calls were offered as an additional option but participants opted to use the telephone. Interviews were held at a time of the participants’ choosing.
Topics covered in the stroke survivor interviews.
Topics covered in the caregiver interviews.
The interview guide was pilot tested with five stroke survivors who gave informed consent to participate in this aspect of the study. The initial interview guide reflected an exploration of day-to-day experiences and personal strategies, but an additional question was added following feedback from participants regarding whether they believed they could also predict the onset of their fatigue. Including this additional question reflected the ongoing, iterative nature of the qualitative process. 17 Data collected in the pilot interviews were included in the final analysis because rich data were obtained that was relevant to the study.
The caregiver interview guide was developed to mirror the stroke survivor interview guide. Again, following discussions with the participants in the pilot study, a question was added to explore how caring for someone with post-stroke fatigue had impacted on the caregiver specifically, and in their daily lives.
Interviews were conducted by JA, FN and AW who were experienced qualitative researchers with knowledge of both stroke and of fatigue, and with backgrounds in health research, occupational therapy and psychology. The interviewers told the participants that they had a specific interest in post-stroke fatigue. They had no relationship with participants prior to study commencement.
Interviews were conducted via telephone and were digitally audio-recorded. Interviewers did not make any field notes but aimed to make the interviews more of a conversation. Participants were advised that transcripts would be anonymised, treated confidentially and that they were free to withdraw at any point during the interview.
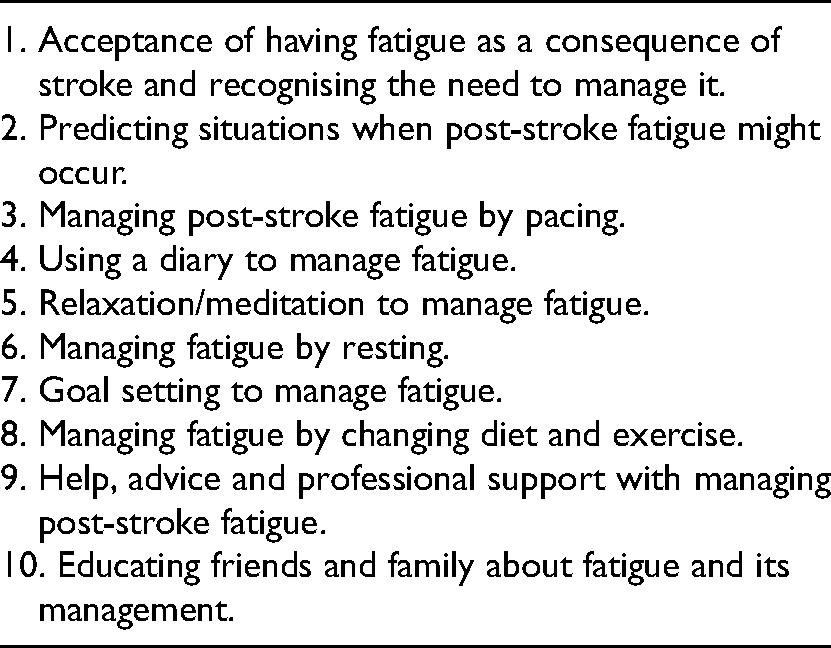
An external specialist transcription company transcribed the interviews verbatim. Transcripts were anonymised and checked for accuracy against the original recordings by the research team with any inconsistencies resolved. Data were systematically analysed using framework analysis 18 and we followed the seven stages of the Framework methodology in the analysis process. This included (i) transcription, (ii) familiarisation with the interview, (iii) coding, (iv) developing a working analytical framework, with the coding scheme (for final themes generated, see Table 4) (v) applying the analytical framework to the data, (vi) charting data and (vii) data interpretation. Nvivo software was used to manage the data.
Themes developed from the framework analysis.
In the first instance, three members of the research team (JA, FN, AW) familiarised themselves with the stroke survivor dataset by thoroughly reading and re-reading each transcript. Initial impressions were noted and shared. The same three researchers then independently coded passages of text of the same three transcripts and met to discuss the codes they had assigned to each passage of text. The researchers agreed on why each passage was interpreted as meaningful, how it might answer the research questions and what it illuminated about the experience and perspective of living with and managing post-stroke fatigue. A PPIE member then independently coded three further transcripts and discussed and agreed, with the research team, additional codes that were then incorporated into the initial analytical framework. This process was then repeated for the caregiver dataset. A coding scheme was then agreed and applied across the entire dataset and this formed the initial analytical framework. We did not return any transcripts to participants for checking or correction.
As this refinement process continued, some overlapping/related codes were grouped into an overarching category. This process continued until no new codes were generated and a final analytical framework was agreed. The two researchers then systematically worked through each transcript and indexed sections of text to an appropriate code from the framework. When the data had been coded, data summaries were written and discussed with the steering group to ensure agreement on interpretation of data. The steering group included PPIE, clinicians and experts in stroke research. Themes were then agreed upon by reviewing these data summaries against the original framework.
Results
Thirty-seven participants expressed an interest in participating in the study and were sent participant information sheets via electronic mail. We approached 22 stroke survivors and 9 caregivers who met our sampling frame criteria, and, of these, 20 stroke survivors and 8 caregivers were interviewed by telephone. Two stroke survivors and one caregiver were not interviewed as they did not respond to the interview invitations. We did not persist in trying to reach these interested parties, nor in approaching other participants, because we found that the same themes and issues were being discussed, suggesting saturation was achieved. Similarly and in addition, the decision was taken to cease recruiting caregivers as the research team felt that the same themes and issues were being identified. Volunteers who had offered help with this study, who were not interviewed, were offered the option of participating in a later phase of the NotFAST2 study.
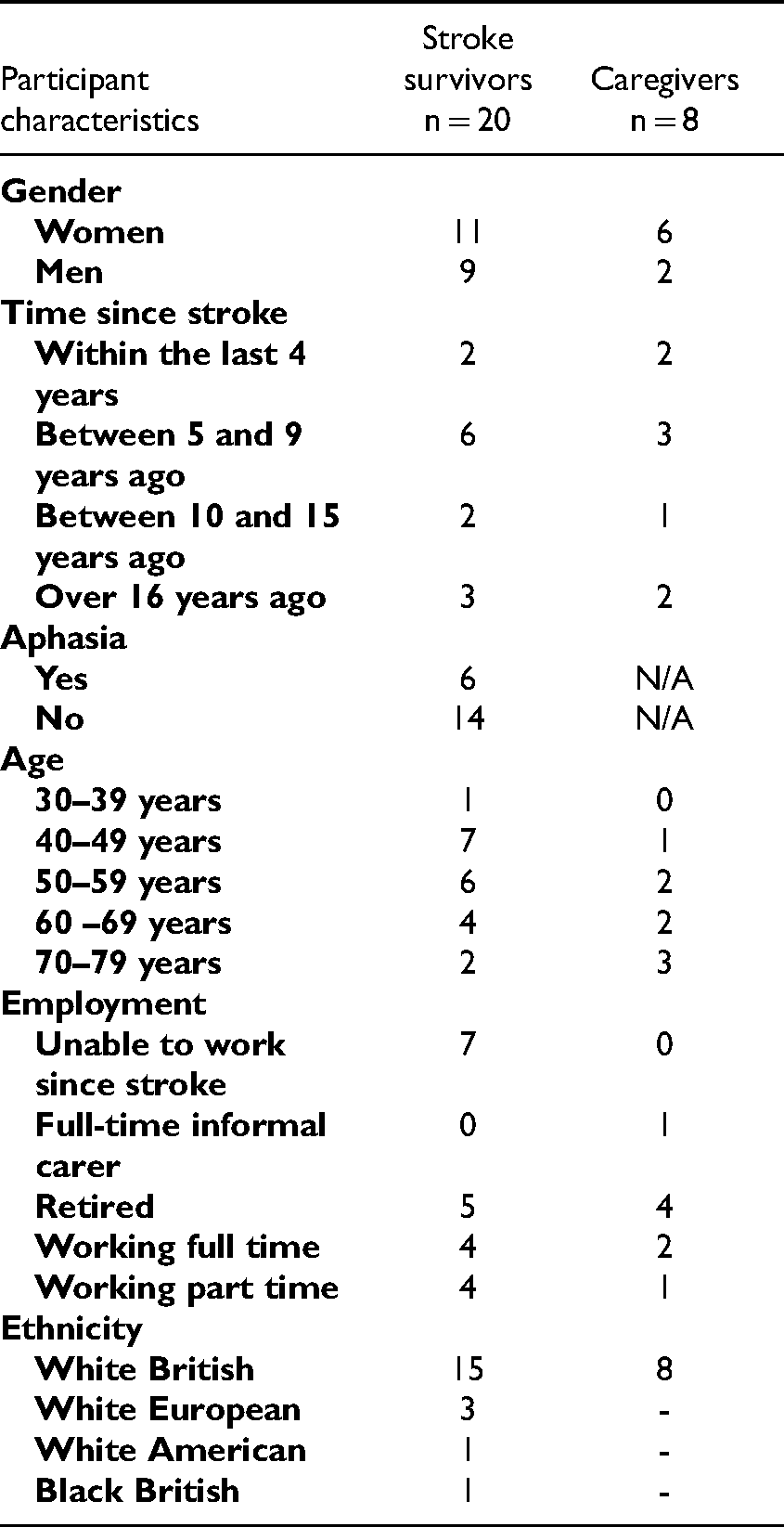
All of the caregivers were the partners of stroke survivors. All stroke survivor participants had current, ongoing fatigue at the time of interview. For each interview, only the researcher and participant were present on the call. The interviews lasted between 20 min and 48 min. The participant characteristics are given in Table 3.
Participant characteristics.
The 10 themes generated are listed in Table 4.
Acceptance of having fatigue as a consequence of stroke and recognising the need to manage it
Participants felt that accepting they had to learn to live with post-stroke fatigue was important: they felt not accepting this made the situation worse. However, for most, achieving acceptance had taken time. “I realised you know, you do have to accept where you’re at, it's no good trying to fight it. That would probably make it worse”. Stroke-survivor 03
Acceptance of the impact of fatigue on their lives and the changes required was also noted by caregivers. The process was described by many as being a long one. “Get used to your life being changed. It is ludicrous but it [post-stroke fatigue] has changed our life enormously…. you just have to accept that it is the way it is. It takes years. It does take years to acclimatise to what you’ve been left with”. Care-giver 01
There was an implication that if survivors tried to ‘fight’ or ‘push through’ having fatigue, they were less likely to cope with the situation.
Predicting situations when post-stroke fatigue might occur
There was variation among participants regarding their descriptions of their ability to predict when they might experience fatigue, and consequently their ability to manage their fatigue. Some participants were able to clearly describe what activities they believed were more likely to trigger their fatigue and they had learnt to find ways to avoid or cope with this. Some participants recognised preliminary fatigue symptoms occurring and managed their behaviour in response, for example, by resting. Others were not able to predict when their fatigue might occur, so found managing their fatigue more difficult. “I’ve never been able to say well for you that's going to trigger it or that's going to trigger it or that's going to trigger it ….and therefore avoid those activities and focus on those”. Stroke-survivor 01
By contrast, caregivers reported that they could often identify when a trigger point might occur and then sought to avoid the situation. When a fatigue triggering situation could not be avoided, this was reported to put an extra burden on them as a caregiver. “Sometimes if he hasn't realised that he's about to overdo it, it's really important for me to recognise it”. Care-giver 01
“…. if he doesn't manage it (the PSF), the consequences are far longer, so it puts more of a burden on me”. Care-giver 04
Managing post-stroke fatigue by ‘pacing’
“Pacing helps, pacing really helps. I probably don't use it the way I would advise people to use it, but it's been really good to be mindful and go oh if we’re going out or meeting up with friends or if we’re doing something that evening, we know it's going to probably be a bit of a busy one, then try not to do too much during the day” Stroke-survivor 06
Although some reported the value of pacing, a number of caregivers observed that the person they were giving care to still tried to do too much: “(name) can't pace himself. So, he goes at something wholeheartedly as fast as he possibly…. you know, wholeheartedly doing something and then finds he just fades”. Care-giver 01
And described the consequences of this: “He just stops if he's tired…. he's… um… tried to push through it, but he just hits a brick wall if you like, which then affects for a few days, rather than just letting it pass” Care-giver 01
Thus, on balance, there was a recognition that activities need to be modified in terms of timing and in terms of level of participation.
Using a diary to manage fatigue
Keeping a fatigue diary was described as a useful management strategy for coping with post-stroke fatigue. It was thought to be useful to help plan daily and weekly activities in advance and, in particular, it was thought to be valuable in identifying triggers. “I found the diary to be good. It does challenge you to think about what you do every day and then you can see when you have good days when you have bad days and what tends to be triggering the cognitive fatigue” Stroke-survivor 01
Caregivers reported using the diary to keep a record of ‘key events’ to enable them to look back, review activities and this enabled the identification of fatigue inducing activities. “It gets to the end of the week and she can say ‘I’m feeling so tired’, and then you can look in the dairy and say well that's because, although you didn't do anything yesterday, in the previous days you’ve been on the go all the time”. Care-giver 05
The diary was viewed as an important fatigue management strategy that facilitated an understanding of activity levels in order to modify these as necessary.
Relaxation/meditation to manage fatigue
Some participants described how engaging in meditative activities was a beneficial fatigue management strategy that they would recommend. Most had identified this strategy themselves rather than this being suggested by health professionals. “What works for me and I would say a lot of that, mindfulness, meditation, deep breathing”. Stroke-survivor 03
“I’ve taken up Tai Chi. So that's been important because that's like breathing and relaxation, it's not a vicious exercise. So those sorts of things have been really helpful”. Stroke-survivor 012
While some used programmes, accessed via a website or an app (an app is software used on a smartphone or mobile device) others spent quiet time recharging their batteries in order to manage their fatigue.
Managing fatigue by resting
Both stroke survivors and caregivers described resting as a helpful way of managing fatigue. For stroke survivors, this usually meant lying down and doing nothing, and very specifically meant not having the TV or radio on, or having any distractions or stimulation. For caregivers, this was about having some space and taking time out of the situation. “After I’ve finished talking to you, I’m going to have a lie down. It's not a case of I can sit down and watch the TV. That's not relaxing. I physically have to lie down and do nothing. I don't even have the radio on. It's really, because if your brain's still working it's still using something, so I actually have to physically do nothing.”. Stroke-survivor 013
“…carers have still got to take 5 min for themselves because otherwise you become overwhelmed yourself”. Care-giver 04
Most participants also described needing sleep to manage their post-stroke fatigue with some experiencing the feeling that they would ‘crash’ if they did not. “It means I slow down and I want to have a sleep. And I just can't carry on function…. You’re exhausted. It's not that you’re a bit tired it's that you can't do it… It means I have to stop and it affects the, for example, my speech. That goes. Also, I joke mainly, I can't walk and talk, I can't do both”. Stroke-survivor 05
However, while this was a useful fatigue management strategy for some, others felt that having more sleep had actually little impact on their fatigue levels, and was not an effective fatigue management strategy for them.
Goal setting to manage fatigue
Some stroke survivors described how setting small personal goals was an important fatigue management strategy. This was described in terms of gradually expanding what they could do. Descriptions included the need to challenge themselves and also to balance this with learning to know their limits. “I think goals are really important. So, my dog really helped me out when I first came out of hospital, because I mainly walked her pretty much most days. And being able to walk her, and then I was expanding it”. Stroke-survivor 06
“I would say respect it, but also try to fight it a little bit at a time. I used to be someone who, I used to set a goal and then I’d achieve it, and then I used to set a goal that was way beyond that and I’ve learnt to do it in steps, in little stages”. Stroke-survivor 011
Managing fatigue by changing diet and exercise
A number of stroke survivors described how changes to their diet had improved the way they felt, but were unsure if this had directly helped with managing their post-stroke fatigue. Some had changed their diet in an attempt to lose weight in order to improve their general health. Others perceived their diet as healthy already and they had made no changes.
With regard to exercise, there were mixed views on this as a fatigue management strategy. Some participants described building up to doing exercise gradually after their stroke, but many were nervous of doing any exercise and felt that ‘pushing too hard’ could be detrimental to their post-stroke fatigue management. “So yeah, I need to lose weight anyway, so I’ve changed my diet. I don't know if it's helped with the fatigue, I do just generally feel better for that. …so, I’ve just been eating healthier and everything”. Stroke-survivor 06
“So, I used to do an exercise, like for example sit to stand and the first year I did 10 and I was knackered. But then I did 12, I did 15. And in the beginning, I would do 10 and I would think oh I’m going to do 25. Which didn't work obviously and then you get fatigue and it sets you back……. I learnt to take it slowly but improve, still improve from 10 to 12, to 15, to 17, to 20 instead of straight to 25”. Stroke-survivor 011
Seeking help, advice and professional support
There were variations in the levels of help, advice and professional support received to support the management of fatigue. Some stroke survivors and caregivers were able to find support groups and found talking to peers very useful in learning how to manage fatigue. Others had no one to talk to, particularly in relation to managing the emotional impact of post-stroke fatigue. Many stroke survivors said they had not heard of post-stroke fatigue until they had experienced it; they did not know initially this was a symptom of stroke. Importantly, post-stroke fatigue and its management had not been discussed at any point by healthcare professionals. When there were conversations, the participants had initiated these.
All the stroke survivor participants felt that having information that post-stroke fatigue is common, how it may affect them, and suggestions for management would have been helpful. The caregivers who had some awareness of potential services available sought these out. They felt that it was unlikely that they would have had received support if they had not advocated on the stroke survivor's behalf. “I would say if I had known about stroke fatigue
“I felt like it was very much me finding out information, it wasn't that people were coming to me with information. And yes, we did get good support, but I wonder would we have had it if not been sought”. Care-giver 08
Many said having professional support was beneficial with learning about fatigue as a common consequence of stroke and for suggestions about management strategies, but felt that more professional contact was needed. “…you don't get all the questions out when you see one person, and then you’ve got nobody else to ask after that”. Stroke-survivor 012
“We managed to link in independently with the occupational therapy team, who were an incredible resource to us. And what they did was they helped us to do almost like a time management plan for going back to work, and that was so helpful. Because you’re in a situation where you don't know, this was new to us, we hadn't expected it to happen, we didn't know what to expect.” Care-giver 08
Educating friends and family about fatigue and its management
Talking to friends and family about the experience of fatigue and how they manage it was described as important in terms of educating friends and family about post-stroke fatigue. Several participants thought this was their single most useful fatigue management strategy. They felt that talking about the stroke and post-stroke fatigue helped them, and also educated their friends and family about post-stroke fatigue who found it difficult to understand. “…just talking about it really helps people. And I think maybe it doesn't get always talked about. And then I think what's really important is family and friends knowing about it as well”. Stroke-survivor 06
Caregivers described the importance of support provided by family members in assisting them to cope with their partner's fatigue. “(name)'s dad did come to let me go back to work sometimes. My mum and dad did an awful lot as well to let me, more my mum and dad really, because they were more…. and I would be able to go back and try and get back to some kind of normality for work. And I’m just grateful that (name) progressed as quickly as he did, otherwise I would have had to think about what I did for my career for future”. Care-giver 03
“I just get on and do… I felt quite isolated … I had to try and get family members to come and look after him, so that I could, because at some point, I had to go back to work and I couldn't leave him. Care-giver 02
Most of the caregivers described how their lives were negatively impacted and limited by their care responsibilities. They reported feelings of loneliness and isolation due to the impact that post-stroke fatigue had on the person they were caring for, and the resultant limitations on their own social life. Some managed the situation by doing some activities by themselves and some adopted the same routines as the stroke survivor. “It actually did change the person he was…. We’d had a very social life up to that point. He didn't want to go anywhere and still doesn't even after all these years … it puts a damper on everything. I tend now to do things by myself”. Care-giver 01.
“Lonely. If you like, because you’re just there. He needs to go to sleep and we like each other's company. We talk a lot, we share ideas a lot, we’ll walk and talk, we watch telly together, we do everything together really. So yeah, if he didn't manage his fatigue and has to go for a sleep, it can be quite lonely”. Care-giver 02
“ You can't do anything, you can't plan anything, and it puts a block on socialisation. But then I become tied into those time schedules, I go to bed at the time, it makes it very difficult to do things”. Care-giver 05
“ It effects my mental health; I want to lose my temper about it or something that is a consequence of it”. Care-giver 05
Discussion
A range of post-stroke fatigue management strategies was used by the stroke survivors and their caregivers. Managing post-stroke fatigue was described in different ways, and there was not one particular fatigue management strategy that seemed effective for everyone. It was notable that people had to identify their own methods of coping and that fatigue had profound impacts on the lives of both stroke survivors and their caregivers. The burden on caregivers was considerable: all had an explicit role in overseeing the implementation of the potential strategies used.
Ultimately, although the strategies which emerged from our interviews mirror broadly what clinicians recommend to their patients 19 and use to manage post-stroke fatigue 20 there is little robust evidence to support the strategies recommended 7 and in use. Although our study focused specifically on post-stroke fatigue, other qualitative studies have been published on fatigue arising from a wide range of other conditions such as rheumatoid arthritis, 21 chronic obstructive pulmonary disease 22 and cancer. 23 There are common threads in all these studies: people having to devise personal management strategies to cope with their fatigue; a lack of clear engagement with healthcare professionals about it; and that, to date, clinicians have not been explicitly informed by those with lived experiences. Although there are clinical guidelines for all of these conditions, people ultimately seem to have to devise their own management plan. There have also been trials to evaluate management strategies for fatigue in other conditions, for example, in multiple sclerosis 24 but, just as in stroke, trials have generally been underpowered and generated produced relatively low-grade evidence.
Our study recruited participants from across the United Kingdom. The use of qualitative methods permitted in-depth exploration of both stroke survivor and career management of post-stroke fatigue. However, although our aim was to recruit a diverse sample of stroke survivors and caregivers, COVID-19 limited opportunities to talk to those with severe communication or cognitive problems by preventing in-person face-to-face interviews. In addition, COVID-19 resulted in a reliance on recruiting people remotely, and we were unable to visit stroke groups to promote participation. Our emphasis on using social media may explain the fact that more of our participants were under 50 years of age. 25 This has implications for our findings, as participants of different age groups may have differing aspirations and expectations for returning to vocational and recreational activities. We also allowed participants to self-define their fatigue and some of the participants were several years after their stroke. Although it is possible that people experience different fatigue at different points in their recovery, our focus was on its management – regardless of aetiology or time since stroke. However, some of the participants were several years after their stroke and therefore their fatigue may also have been due to new additional factors.
Ultimately, our findings show that stroke survivors and caregivers are resourceful. They also illustrate their ability to devise different strategies, some of which seemed to be more helpful than others. This suggests that individuals may need a programme that is tailored to them as individuals rather than using the same management approach for everyone. The participants in our study used strategies that clinicians would recommend; 20 however, there were variations in the levels of help, advice and professional support they received. Post-stroke fatigue symptoms and management were not discussed although our participants felt that this would have been useful and would have welcomed it.
Post-stroke fatigue is not a trivial enterprise and it has profound effects on both survivors and their caregivers. Given the magnitude of this problem, and recognition that this is a priority area for further investigation,9,10 we need research to determine whether certain strategies are more, or less, helpful than others for specific groups of stroke survivors and their carers. However, it is vital that this is directly informed and guided by those with lived experience. The new initiative to name fatigue as a Stroke Recovery and Roundtable (SRRR) international priority area should energise and stimulate more research into this issue.
Clinical messages
Those living with post-stroke fatigue use a wide range of self-management strategies.
Many people have to develop their own management strategies, without receiving professional support.
There does not seem to be any single strategy that is useful for everyone.
Footnotes
Acknowledgements
The authors greatly appreciate the time given by those who took part in the interviews. We would also like to acknowledge the contribution of the NotFAST2 steering group members and particularly one of the PPIE members, who had post-stroke fatigue, who independently coded three transcripts and discussed and agreed additional codes that were incorporated into the initial analytical framework.
Author’s contribution
All authors contributed to the study design, interpretation of data and commented on the final manuscript. JA, FN and AW conducted interviews. JA, FN, FJ and RdN led on analysis. JA, FN and AD drafted the manuscript. All authors agreed the final version of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Stroke Association (grant number SA PG 19\100060).