
Abstract
Objective:
To use the self-assessment INTERMED questionnaire to determine the relationship between biopsychosocial complexity and healthcare and social costs of patients after orthopaedic trauma.
Design:
Secondary prospective analysis based on the validation study cohort of the self-assessment INTERMED questionnaire.
Setting:
Inpatients orthopaedic rehabilitation with vocational aspects.
Subjects:
In total, 136 patients with chronic pain and impairments were included in this study: mean (SD) age, 42.6 (10.7) years; 116 men, with moderate pain intensity (51/100); suffering from upper (n = 55), lower-limb (n = 51) or spine (n = 30) pain after orthopaedic trauma; with minor or moderate injury severity (severe injury for 25).
Main measures:
Biopsychosocial complexity, assessed with the self-assessment INTERMED questionnaire, and other confounding variables collected prospectively during rehabilitation. Outcome measures (healthcare costs, loss of wage costs and time for fitness-to-work) were collected through insurance files after case settlements. Linear multiple regression models adjusted for age, gender, pain, trauma severity, education and employment contract were performed to measure the influence of biopsychosocial complexity on the three outcome variables.
Results:
High-cost patients were older (+3.6 years) and more anxious (9.0 vs 7.3 points at HADS-A), came later to rehabilitation (+105 days), and showed higher biopsychosocial complexity (+3.2 points). After adjustment, biopsychosocial complexity was significantly associated with healthcare (ß = 0.02; P = 0.003; expß = 1.02) and social costs (ß = 0.03; P = 0.006, expß = 1.03) and duration before fitness-to-work (ß = 0.04; P < 0.001, expß = 1.04).
Conclusion:
Biopsychosocial complexity assessed with the self-assessment INTERMED questionnaire is associated with higher healthcare and social costs.
Introduction
Long-term analyses of outcomes after orthopaedic trauma are scarce, despite being a leading cause of disability 1 and causing a high social burden for some patients.2–4 Poor outcomes are not only related to trauma severity but also to factors unrelated to injury such as age, psychiatric comorbidity, lack of education or working situation,5–7 which call for a biopsychosocial approach. However, there are few studies addressing the influence of biopsychosocial complexity on trauma outcomes. 8 Literature on healthcare costs is mostly derived from a biomedical model of health, which focuses on the diagnosis and severity of illness or injury.3–6 However, this model is disputed, since the severity of trauma or disease is only one of the variables in the equation.9–13
In order to improve the biomedical model’s explanatory power, the biopsychosocial model of care, developed by Engel 40 years ago, 14 takes into account personal and environmental factors that influence the outcome of disease or trauma. 13 Despite growing numbers of publications, its promotion by the World Health Organization in its ‘International Classification of Functioning, Disability and Health’ 15 and its inclusion in clinical guidelines, the biopsychosocial model of care struggles to be implemented by caregivers, 16 and to be accepted by patients and health economics managers. 13 The self-assessment INTERMED questionnaire is one of few screening tools available to detect patients with a high biopsychosocial complexity. 13 It has been shown to be reliable and valid 17 in identifying patients with complex health needs who are at risk for high use of healthcare services. There is, to the best of our knowledge, no research addressing the association of biopsychosocial complexity and healthcare costs after orthopaedic trauma.
The aim of our study was to investigate, by means of the self-assessment INTERMED questionnaire, the influence of biopsychosocial complexity on healthcare costs, daily wage compensations paid and durations before fitness-to-work in a population of patients admitted to rehabilitation after orthopaedic trauma. Our hypothesis was that a high biopsychosocial complexity would be associated with higher costs and a longer time before fitness-to-work.
Methods
This study was a secondary prospective analysis of part of the cohort of patients who participated in the validation study of the self-assessment INTERMED questionnaire. 18 Patients were included between September 2011 and March 2012 at the Clinique Romande de Réadaptation in Sion, Switzerland. Outcomes concerning costs and duration before fitness-to-work were retrieved through insurance data after case settlement in July 2019. The duration since inclusion has made it possible to know the full costs associated with trauma after the cases had been settled. The study was conducted according to the ethical principles expressed by the World Medical Association Declaration of Helsinki. All participants gave their informed consent to the access to and use of their clinical data for the present study. The protocol was approved by the local medical ethics committee of the Canton du Valais for the validation study of the self-assessment INTERMED questionnaire 18 [CCVEM 034/11], with an addendum for the collection of insurance data from the Lausanne University Ethical committee [CER-VD/PB_2019-00044 034/12]. This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Any patient of working age (18–60 years old) referred after orthopaedic trauma for a rehabilitation programme with a vocational aspect was eligible for this secondary analysis. We included patients who were insured by the main insurance supplier for trauma of Switzerland (Suva). Suva insures 2 million workers, representing half of Swiss employees from a third of the country’s companies. We chose 60 years of age as a limit for inclusion in the study, because the compensation system changes after the retirement age of 65 years in Switzerland. Being interested in social costs, which are largely related to the daily allowances paid by the accident insurance, we limited inclusion to patients younger than 60 years old, expecting cases to be settled in our population after five years. Exclusion criteria from the self-assessment INTERMED questionnaire validation study 18 included refusal to participate, language difficulties, being incapable of judgement, or under legal custody. If a patient was treated twice during this period, only data from their first admittance to hospital were taken into account.
The study took place in a rehabilitation centre to which patients are referred if the initial rehabilitation measures that take place close to patients’ residence fail or if patients cannot return to their work. The therapeutic programme was based on a multidisciplinary biopsychosocial approach, addressing physical, psychological and social factors for every patient according to the practice recommendations for chronic pain patients.19,20 The programme involved physical treatments (physiotherapy and occupational therapy with individual and group sessions, including graded exercises and functional training), vocational training, social advice and psychological therapy with a cognitive and behavioural approach. More details on the setting are provided elsewhere.21,22
Patients’ characteristics and socio-demographic data were collected upon admission from medical assessment and questionnaires. Included biological variables were (i) age; (ii) gender; (iii) Abbreviated Injury Scale (AIS) score (minor vs moderate or severe injury) 23 ; and (iv) pain assessed on a Visual Analogue Scale (range, 0–100). 24 Social variables consisted of (i) education (in years), (ii) employment contract at the time of rehabilitation (yes versus no). Psychological variables included (i) anxious and (ii) depressive symptoms assessed with the Hospital Anxiety and Depression Scale (HAD-S) (range, 0–21). 25 Quality of life was evaluated with the Short-Form-36 questionnaire (SF-36). 26
The self-assessment INTERMED questionnaire was used to assess bio-psychosocial complexity. It is a self-reported-questionnaire based on the INTERMED method,8,27–31 with which it is adequately (r = 0.64) correlated. 18 Associations of biopsychosocial complexity with higher health service reliance have been found with the self-assessment INTERMED questionnaire.18,32
Healthcare costs and other insurance data were retrieved after case settlement was declared by the insurance in charge (Suva). Time to fitness-for-work (TFW) was defined as the number of days during which compensation was paid by the insurer in cases of work disability. 33 During this period, compensations were paid in the form of daily allowances until patients regained the capacity to work without risking their own and others’ health and safety. 34 Daily wage compensations were the equivalent to 80% of a person’s usual salary and were paid until the patient either returned to work or was declared permanently disabled, in which case compensation payments switched to a permanent disability pension. Daily wage compensations were considered part of social costs, as opposed to direct healthcare costs, which were defined as any expenditures allocated for diagnostic procedures (e.g. medical consultations, laboratory or radiological examinations), or for treatment (e.g. surgery, medication, hospitalisation or physiotherapy). 35
To minimise measurement bias, clinical and demographic data were collected before starting the therapeutic programme. Questionnaires were administered in the two or three days after admission to the rehabilitation centre. Data was digitally recorded to diminish transcription bias. As aforementioned, data concerning costs and time for case settlement were retrieved through insurance files. In Switzerland, the insurer in charge of a patient after trauma is responsible for all treatment costs and pay for sick leave. The insurer registers all treatment bills and daily wage compensations for every case and is able to determine the exact costs of treatments and daily allowances allocated to every patient.
Descriptive statistics were expressed as mean and standard deviation for continuous variables, whereas median and interquartile range (IQR) were used if the distribution was skewed. To assess the hypothesis of normality, we performed a visual inspection of the distribution of data. Categorical variables were expressed as count and percentage. Comparison of high and low-cost groups of patients were presented based on the median of total costs, which correspond to the sum of healthcare and social costs.
To study the association between biopsychosocial complexity and outcomes, we used continuous scores for the self-assessment INTERMED questionnaire score and outcome variables of costs and time for fitness-to-work. Standard multiple linear regression models were applied to measure the associations between outcomes and the complexity score, while adjusting for potential confounders. Potential confounders were based on literature3–6 and clinical expertise: age, gender, education (in years), trauma severity (minor injury vs moderate vs severe injury based on the AIS score), pain (VAS) and work contract at the time of rehabilitation (yes vs no). Only patients with complete data sets were included in the analysis. The available sample size allowed the estimation of up to nine parameters in regression models to keep a minimum of 15 observations per parameter. 36 As healthcare costs and time for fitness-to-work were not normally distributed, we used a logarithmic transformation in the models. For interpretation, β coefficient was back transformed and presented as expβ, which represents the expected ratio between two patients with equal covariates who would have a difference of one point in the variable of interest. 37
The significance level was set as a probability of less than 0.05. All analyses were performed using Stata 16 (StataCorp, College Station, Texas, USA).
Results
Of the 175 patients who participated in the self-assessment INTERMED questionnaire validation study, 34 were excluded because outcomes from their insurance suppliers could not be retrieved or they were older than 60 years, and five others had missing data (see Figure 1). We could thus include 136 patients in this analysis. High-cost patients were older, more anxious, had arrived to rehabilitation later and had a higher self-assessment INTERMED questionnaire score. The sample characteristics are detailed in Table 1.
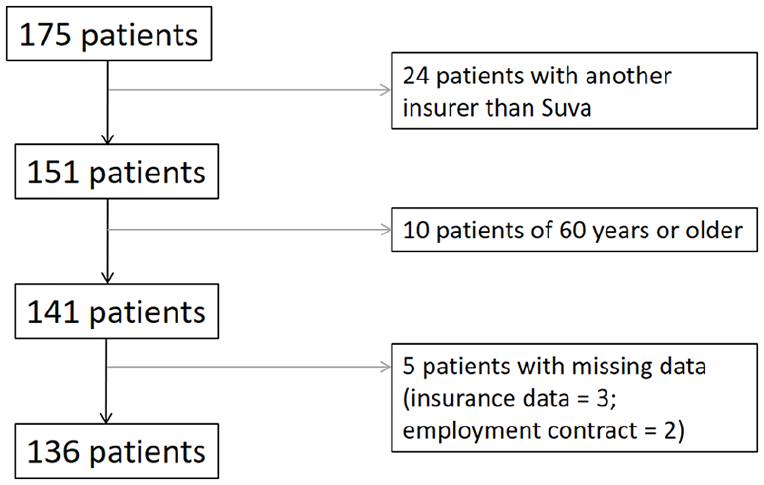
Flowchart.
Summary statistics for the entire cohort and high and low-costs groups defined by the median of the sum of healthcare and social costs.
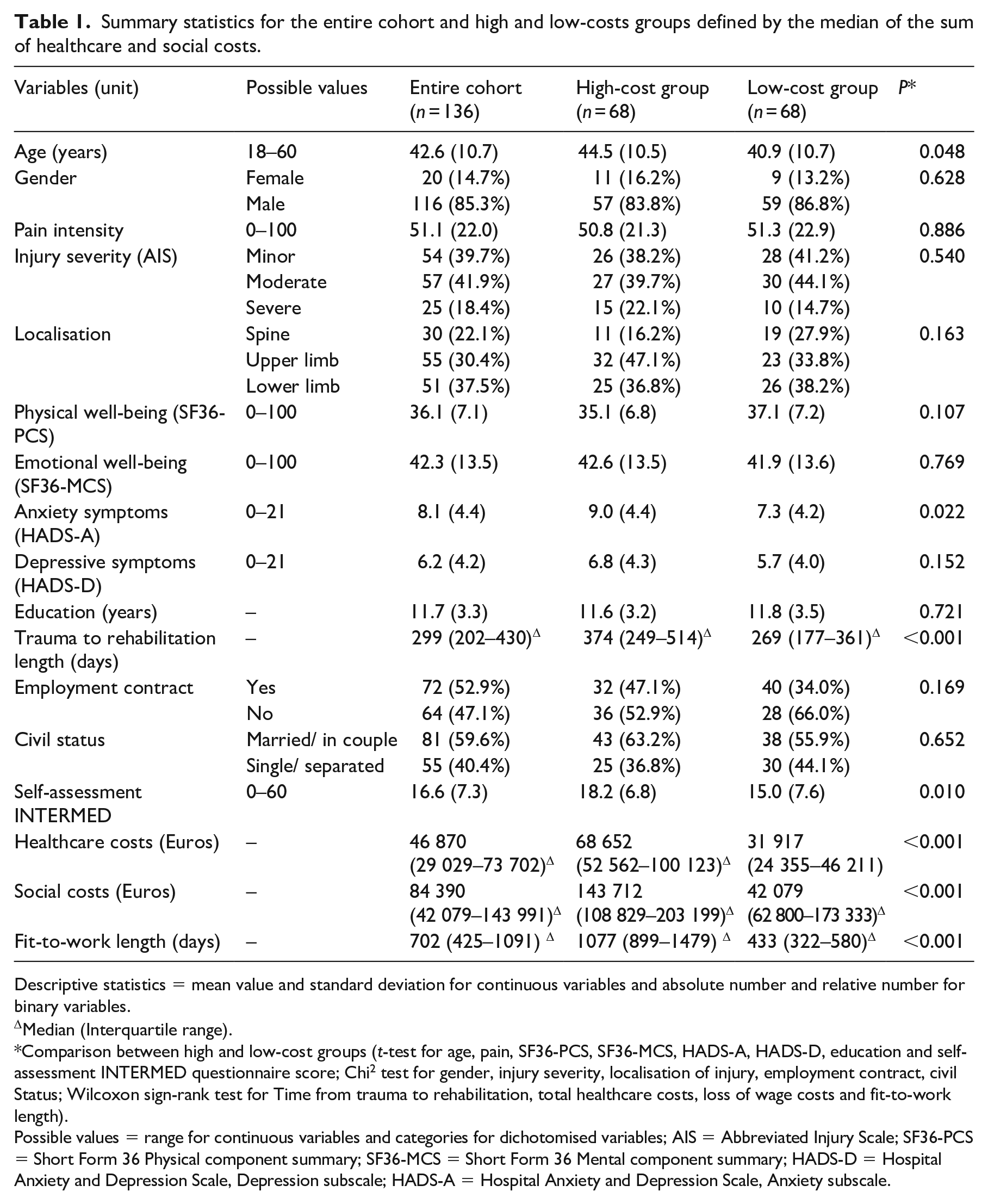
Descriptive statistics = mean value and standard deviation for continuous variables and absolute number and relative number for binary variables.
Median (Interquartile range).
Comparison between high and low-cost groups (t-test for age, pain, SF36-PCS, SF36-MCS, HADS-A, HADS-D, education and self-assessment INTERMED questionnaire score; Chi 2 test for gender, injury severity, localisation of injury, employment contract, civil Status; Wilcoxon sign-rank test for Time from trauma to rehabilitation, total healthcare costs, loss of wage costs and fit-to-work length).
Possible values = range for continuous variables and categories for dichotomised variables; AIS = Abbreviated Injury Scale; SF36-PCS = Short Form 36 Physical component summary; SF36-MCS = Short Form 36 Mental component summary; HADS-D = Hospital Anxiety and Depression Scale, Depression subscale; HADS-A = Hospital Anxiety and Depression Scale, Anxiety subscale.
Results of the standard multiple linear regression model analysis are presented in Table 2. A higher biopsychosocial complexity was found to be associated with the three outcomes after adjustment with confounding variables.
Standard multiple linear regression models for INTERMED-SA and treatment costs.
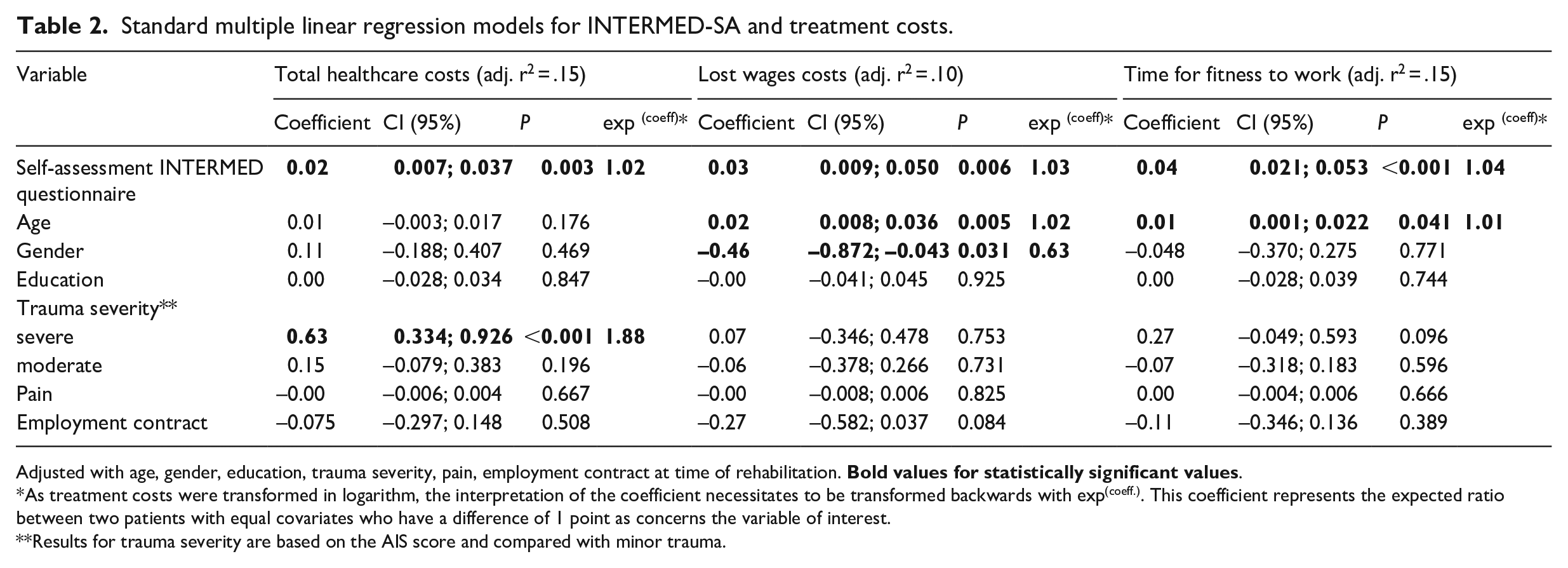
Adjusted with age, gender, education, trauma severity, pain, employment contract at time of rehabilitation.
As treatment costs were transformed in logarithm, the interpretation of the coefficient necessitates to be transformed backwards with exp(coeff.). This coefficient represents the expected ratio between two patients with equal covariates who have a difference of 1 point as concerns the variable of interest.
Results for trauma severity are based on the AIS score and compared with minor trauma.
A higher biopsychosocial complexity was associated with higher healthcare costs. Apart from trauma severity, none of the other variables of the model were associated with treatment costs. The transformed coefficient of 1.02 corresponds to an expected increase of 2% in costs for every one-point difference in the self-assessment INTERMED questionnaire score between two patients with the same confounding variables.
Higher biopsychosocial complexity was associated with higher social costs measured by lost wages. Among other variables included in the model, higher age and male gender were also associated with higher lost wages. The transformed coefficient of 1.03 corresponds to an expected increase of 3% in costs for every one-point difference in the self-assessment INTERMED questionnaire score between two patients with the same confounding variables.
For fitness-to-work time, a higher complexity score was also associated with a longer duration before fitness-to-work. Apart from age, none of the other confounding variables were associated with time for fitness-to-work. The transformed coefficient of 1.04 corresponds to an expected increase of 4% in work incapacity duration for every one-point difference in the self-assessment INTERMED questionnaire score between two patients with the same confounding variables.
Figure 2 illustrates the association between biopsychosocial complexity and the three outcomes for three single patients who would have mean values for each of the confounding variables (age, education, pain) and have had a trauma of minor (red), moderate (green) or severe (orange) severity according to the AIS.
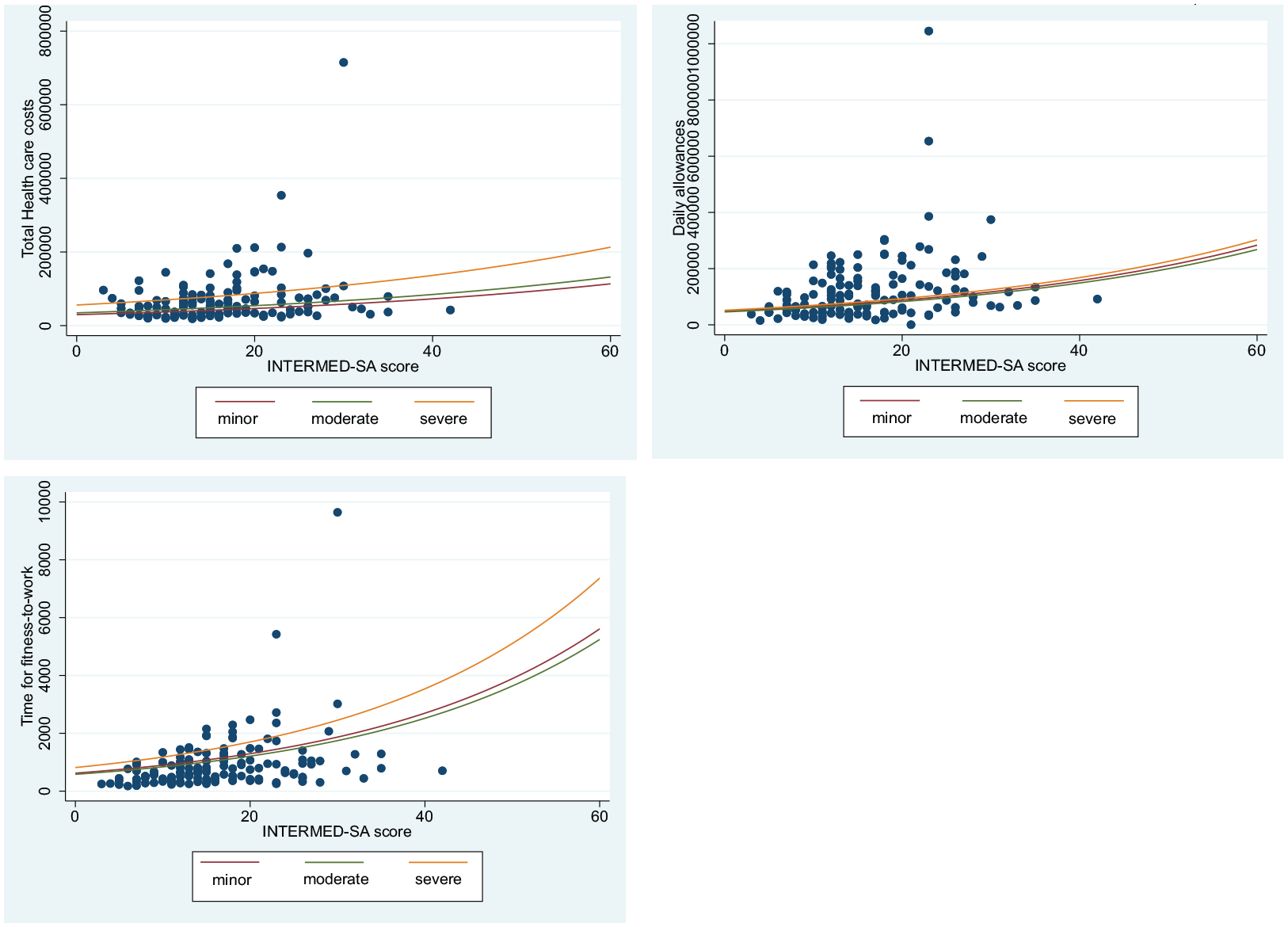
Illustration of the associations between biopsychosocial complexity and the three outcomes for three single patients who would have mean values for each of the confounding variables (age, education, pain) and have had a trauma of minor (red), moderate (green) or severe (orange) severity according to the AIS score.
Discussion
Biopsychosocial complexity measured by the self-assessment INTERMED questionnaire was – after adjustment for numerous confounding variables – significantly associated with a longer work incapacity and higher healthcare and social costs. Considering the median duration for fitness-to-work of 702 days, the expected increase for every self-assessment INTERMED questionnaire point is 26 days (95% CI: 16–41 days). Taking into consideration the median healthcare costs of 46,870 Euros in our population, the expected difference for every point (range of 0–60 points) is 1056 (95% CI: 654–1682) Euros. If we consider the median daily allowances of 84,390 Euros allocated to our population, the expected increase of social costs for every self-assessment INTERMED questionnaire point is 2518 (95% CI: 1256–4289) Euros. By adding healthcare and social costs, the expected increase in cost for every point in our model is 3574 Euros.
The association between biopsychosocial complexity and sick-leave duration is in accordance with two other studies that used the semi-structured interview INTERMED method.8,38 Our results also confirm studies showing that sick-leave duration is related to factors unrelated to injury severity, 6 such as age, the presence of psychiatric comorbidity, lower education and being on sick-leave the month preceding trauma,4,7 which confirms that factors influencing consequences of trauma are beyond the biomedical realm.
Concerning treatment costs, we found only one study in a geriatric patient population, which showed that a higher biopsychosocial complexity assessed with the self-assessment INTERMED questionnaire was associated with higher costs. 32 Other studies using this questionnaire 18 or the original INTERMED semi-structured interview8,27,39,40 consistently found associations between biopsychosocial complexity and a higher consumption of health care services. We could not find any other study addressing biopsychosocial complexity and social costs.
In our model older age and male gender were also associated with higher compensations. These results may primarily be due to the fact that, according to Switzerland’s salary scales, 41 women are 12% less paid and work part-time three times more often than men. 42 With regard to age, elderly workers also receive higher salaries, 41 which might explain these associations.
This study has some limitations. First, its unusual setting with a sample mainly composed of men coming for late rehabilitation after trauma may limit the generalisation of the results. Second, biopsychosocial complexity and the presence of an employment contract were assessed during rehabilitation and not at the time of the trauma. However, even if the variable was collected during rehabilitation, we considered that it was more pertinent to take the working situation at the time of rehabilitation, as some patients had lost their jobs during the interval between trauma and rehabilitation. Finally, the biopsychosocial complexity measured during rehabilitation in our clinic may not represent baseline complexity, as it has been shown that the interval between injury and rehabilitation may play a role in the development of chronicity,43,44 which may influence the complexity of patients. An earlier assessment after trauma was not possible but may indicate an interesting direction for future research in the detection of patients with high complexity.
The strength of this study lies in the robustness of the data it uses with regard to healthcare and social costs and the duration of fitness-to-work provided by the insurance supplier. Our results stress the importance of addressing biopsychosocial complexity for patients after trauma in order not only to provide good care but also to limit costs and work incapacity.
There is a real need to promote the biopsychosocial model of care in clinical practice and health service management. 16 Other studies will be needed to deepen the understanding of personal and environmental factors’ influences on the development of biopsychosocial complexity and to evaluate the benefits of early psychosocial interventions complementing physical treatments. Intervention studies based on INTERMED case complexity have demonstrated to be beneficial for patients and for costs containment. 45 The self-assessment INTERMED questionnaire, which allows an easy screening, also has the potential of being used earlier in the rehabilitation process to identify patients at risk of complex healthcare needs and to subsequently provide them with appropriate and coordinated interdisciplinary care, with the aim of reducing disability and costs.
Clinical messages
A higher biopsychosocial complexity, as measured by the self-assessment INTERMED questionnaire, is associated both with higher medical treatment costs and higher social costs in people who have suffered an orthopaedic injury.
Footnotes
Acknowledgements
We thank the nursing team who collected the questionnaires, Pierre-Dominique Varone who helped to collect data, and Alice Burrus and Hong Phuoc Duong for proofreading the manuscript.
Author contributions
C.B., F.L, and B.L., planned the study, and C.B. and F.L. carried out measurements. C.B. and P.V. analysed the data. C.B. wrote the manuscript with critical feedback and help from P.V., B.L., G.R., F.S. and F.L. All authors discussed the results and contributed to the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.