
Abstract
Objective:
To compare the long-term effectiveness of an integrated rehabilitation programme with an existing rehabilitation programme, in terms of back-specific disability, in patients with chronic low back pain.
Design:
A single-centre, pragmatic, two-arm parallel, randomised controlled trial.
Setting:
A rheumatology rehabilitation centre in Denmark.
Subjects:
A total of 165 adults (aged ⩾ 18 years) with chronic low back pain.
Interventions:
An integrated programme (a pre-admission day, two weeks at home, two weeks inpatient followed by home-based activities, plus two 2-day inpatient booster sessions, and six-month follow-up visit) was compared with an existing programme (four-week inpatient, and six-month follow-up visit).
Main measure:
The primary outcome was disability measured using the Oswestry Disability Index after one year. Secondary outcomes included pain intensity (Numerical Rating Scale), pain self-efficacy (Pain Self-Efficacy Questionnaire), health-related quality of life (EuroQol-5 Domain 5-level (EQ-5D)), and depression (Major Depression Inventory). Analysis was by intention-to-treat, using linear mixed models.
Results:
303 patients were assessed for eligibility of whom 165 patients (mean age 50 years (SD 13) with a mean Oswestry Disability Index score of 42 (SD 11)) were randomly allocated (1:1 ratio) to the integrated programme (n = 82) or the existing programme (n = 83). The mean difference (integrated programme minus existing programme) in disability was –0.53 (95% CI –4.08 to 3.02); p = 0.770). No statistically significant differences were found in the secondary outcomes.
Conclusion:
The integrated programme was not more effective in reducing long-term disability in patients with chronic low back pain than the existing programme.
Keywords
Introduction
Multidisciplinary rehabilitation is recommended as second-line treatment in the management of chronic low back pain.1–3 It is based on the widely accepted biopsychosocial approach1,4,5 and comprises a multifaceted intervention targeting the wide range of modifiable factors known to contribute to chronic low back pain. 6 The team providing rehabilitation can reinforce integration of knowledge, skills and behaviours by taking the patient’s environment into account5,7 and ensuring regular interaction with the patient via scheduled booster sessions. 8 Thus, combining the biopsychosocial approach5,7 with the Chronic Care Model 8 seems reasonable from a theoretical point of view. 9 However, the optimal dose, content and delivery of multidisciplinary rehabilitation programmes remain unknown. 4
Therefore, as described in a previous paper, we designed an integrated multidisciplinary rehabilitation programme comprising inpatient stays alternating with home-based activities and booster sessions. 9 The intention was to support integration of knowledge, skills and behaviours gained from a multidisciplinary inpatient rehabilitation programme into the daily life of patients with chronic low back pain. 9 In another previous paper, we reported results from the six-month follow up from a randomised controlled trial comparing an integrated rehabilitation programme with an existing rehabilitation programme. 10
Long-term (one year) follow-up data on the effect of such a rehabilitation programme are needed given that time is thought to be related to successful integration of knowledge, skills, and behaviours. 11 Consequently, the aim of this paper was to compare the effectiveness of the integrated programme with an existing programme in terms of back-specific disability in patients with chronic low back pain at one-year follow up.
Methods
The Central Denmark Region Committees on Biomedical and Research Ethics approved the trial (journal number: 1-10-72-117-16), and the trial was registered at ClinicalTrials.gov (identifier NCT02884466).
Participant recruitment started in February 2016 and ended in August 2018. The first rehabilitation programmes commenced in September 2016 and patients in the last rehabilitation programme reached the one-year follow up in November 2019.
This was a single-centre, pragmatic, two-arm parallel, randomised controlled trial comparing two rehabilitation programmes for patients with chronic low back pain.9,10 The clinical activities comprising the rehabilitation programmes have been described 9 and adhere to the Template for Intervention Description and Replication (TIDieR) checklist. 12 The participants, randomisation procedures, outcomes, and sample size have been described in detail in the six-month follow-up paper 10 and adhere to Consolidated Standards of Reporting Trials (CONSORT) 2010 Statement. 13
The key difference between the two rehabilitation programmes being compared was the way in which they were delivered (Figure 1).
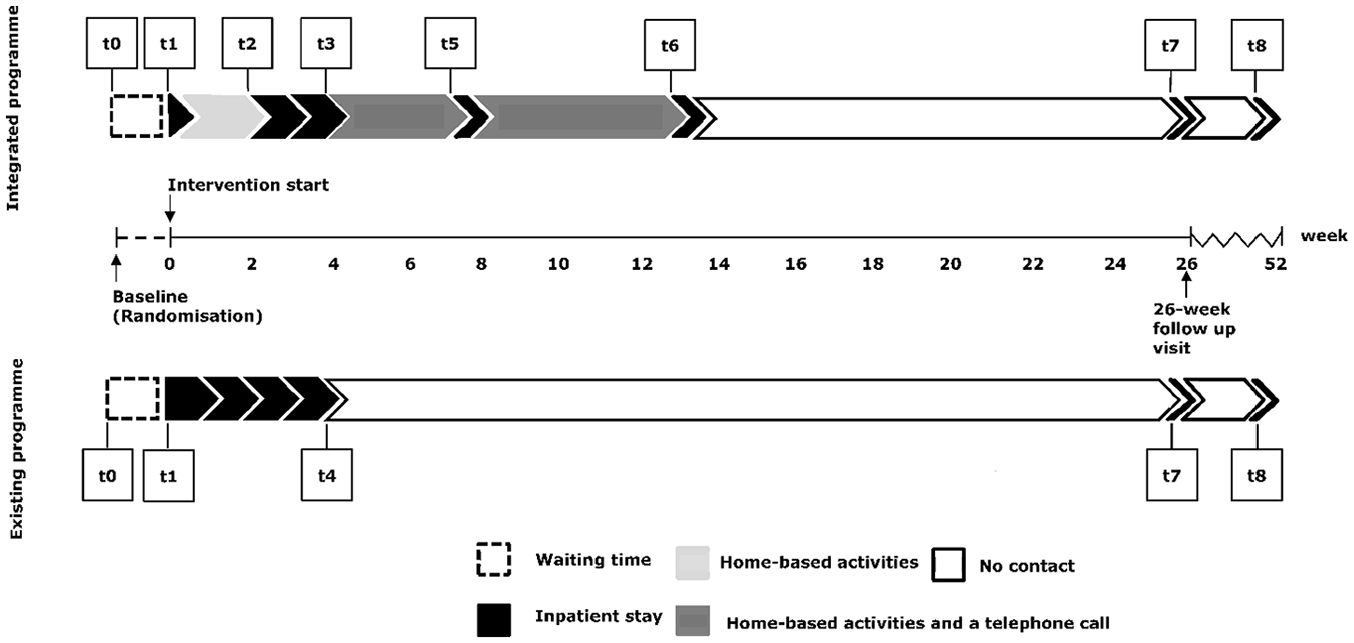
The integrated programme and the existing programme with related measurement time points. t0 = baseline, t1 = before the pre-assessment day (integrated programme) and before the four-week inpatient stay (existing programme), t2 = before the two-week inpatient stay (integrated programme), t3 = the end of the two-week inpatient stay (integrated programme), t4 = the end of the four-week inpatient stay (existing programme), t5 = before the initial booster session (integrated programme, t6 = before the second booster session (integrated programme), t7 = before the six-month follow-up visit (integrated programme + existing programme), and t8 = at the one-year follow up (integrated programme + existing programme).
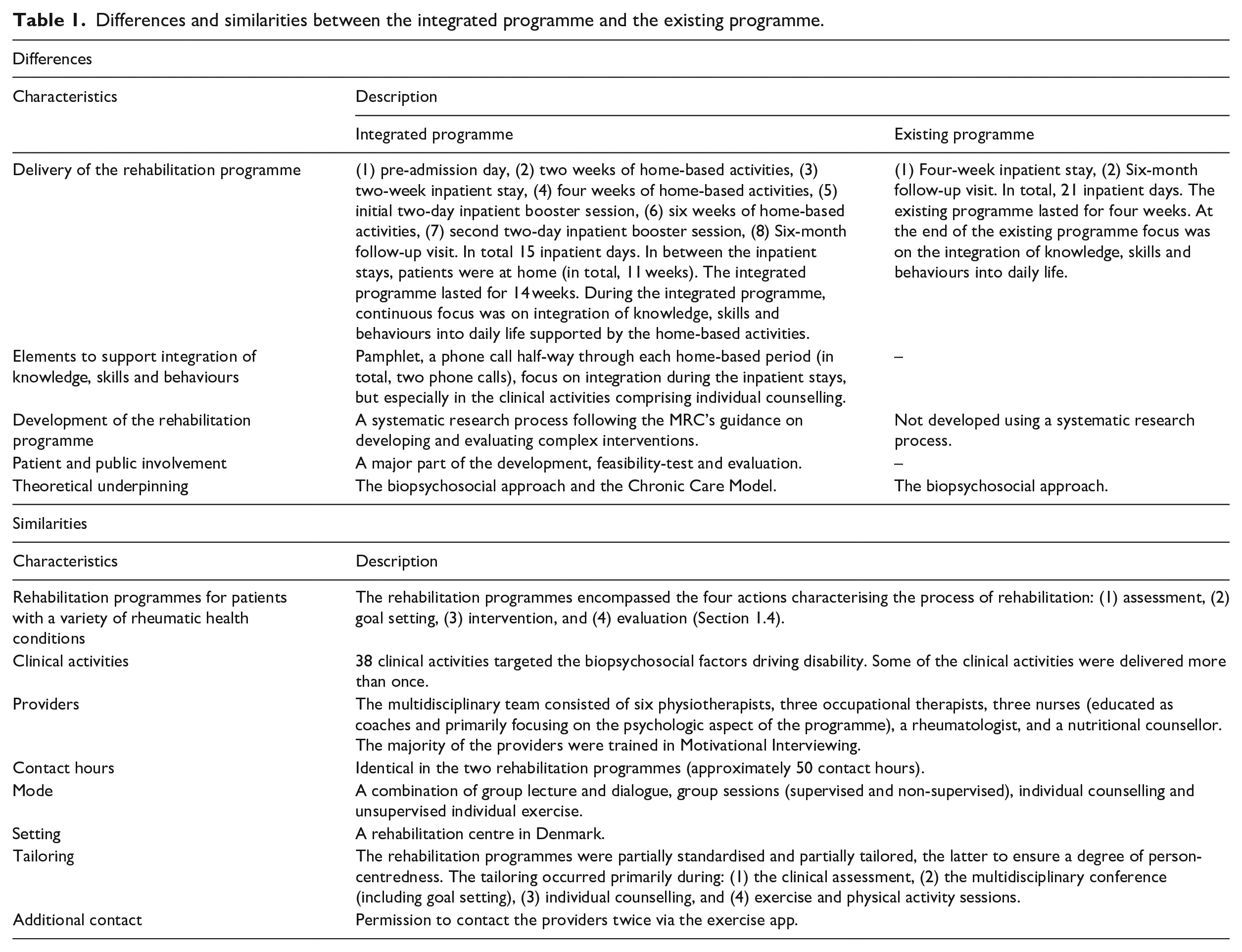
The differences and similarities between the two rehabilitation programmes are illustrated in Table 1.
Differences and similarities between the integrated programme and the existing programme.
Baseline characteristics were collected before randomisation (t0). Outcome measures were collected several times. Measurement time points in both groups were identical at baseline (t0), before intervention start (t1), before the six-month follow-up visit (t7), and one year after the start of the rehabilitation programme (t8) (Figure 1).
The choice of outcome domains and outcome measures was based on patient and public involvement 10 in combination with international recommendations.14,15 The primary outcome was back-specific disability, assessed by the Oswestry Disability Index version 2.1a. 16 Secondary outcome measures were back pain intensity assessed by a Numerical Rating Scale, 14 pain self-efficacy measured by the Pain Self-Efficacy Questionnaire, 17 health-related quality of life measured by the EQ-5D 5L© 18 and depression measured by the Major Depression Inventory. 19
Descriptive statistics were presented with means and standard deviations (SD) or numbers and percentages, depending on the type of variable. The primary analysis was performed as an intention-to-treat analysis including the four identical measurement time points (t0, t1, t7 and t8). Intervention effects on the primary and secondary outcomes were estimated by the difference in change between the two groups (integrated programme minus existing programme) from baseline to one year using a linear mixed model with a random intercept. The analysis included time (as a categorical variable), group, and the interaction between group and time as the only explanatory variables. Furthermore, the linear mixed model was used to test if the outcomes over time in the two rehabilitation programmes were similar (i.e. test of no interaction between group and time). The underlying assumptions behind a linear mixed model were checked by inspection of plots of random intercepts and residuals. For all outcomes except the EQ-5D 5L and the Major Depression Inventory, the assumptions were fulfilled, and hence we used the non-parametric bootstrap method with 1000 repetitions to compute p-values and 95% confidence interval’s (CI) for these two measures. Three secondary analyses were conducted to examine the robustness of the primary analysis: (1) adding waiting time to intervention start as a covariate (as waiting time differed between the two rehabilitation programmes by chance 10 ), (2) replacing missing values by the average of non-missing scores at the particular time point, and (3) replacing missing values by the worst possible score (=100) in the integrated programme and the best possible score (=0) in the existing programme. Additionally, graphs including means at all nine measurement time points (t0-t8) were presented in order to illustrate changes over time for patients allocated to each rehabilitation programme.
Statistical significance was defined as p ⩽ 0.05. A statistical analysis plan was developed and finalised prior to data analysis (Supplementary file 1 (supplementary data, online only)), and STATA 16 was used for all statistical analyses.
Results
In total, 165 patients were randomly allocated to the integrated programme (n = 82) or to the existing programme (n = 83) (Figure 2). There were no systematic differences in either baseline or outcome variables between patients lost to follow up and those who completed the one-year follow up (data not shown).
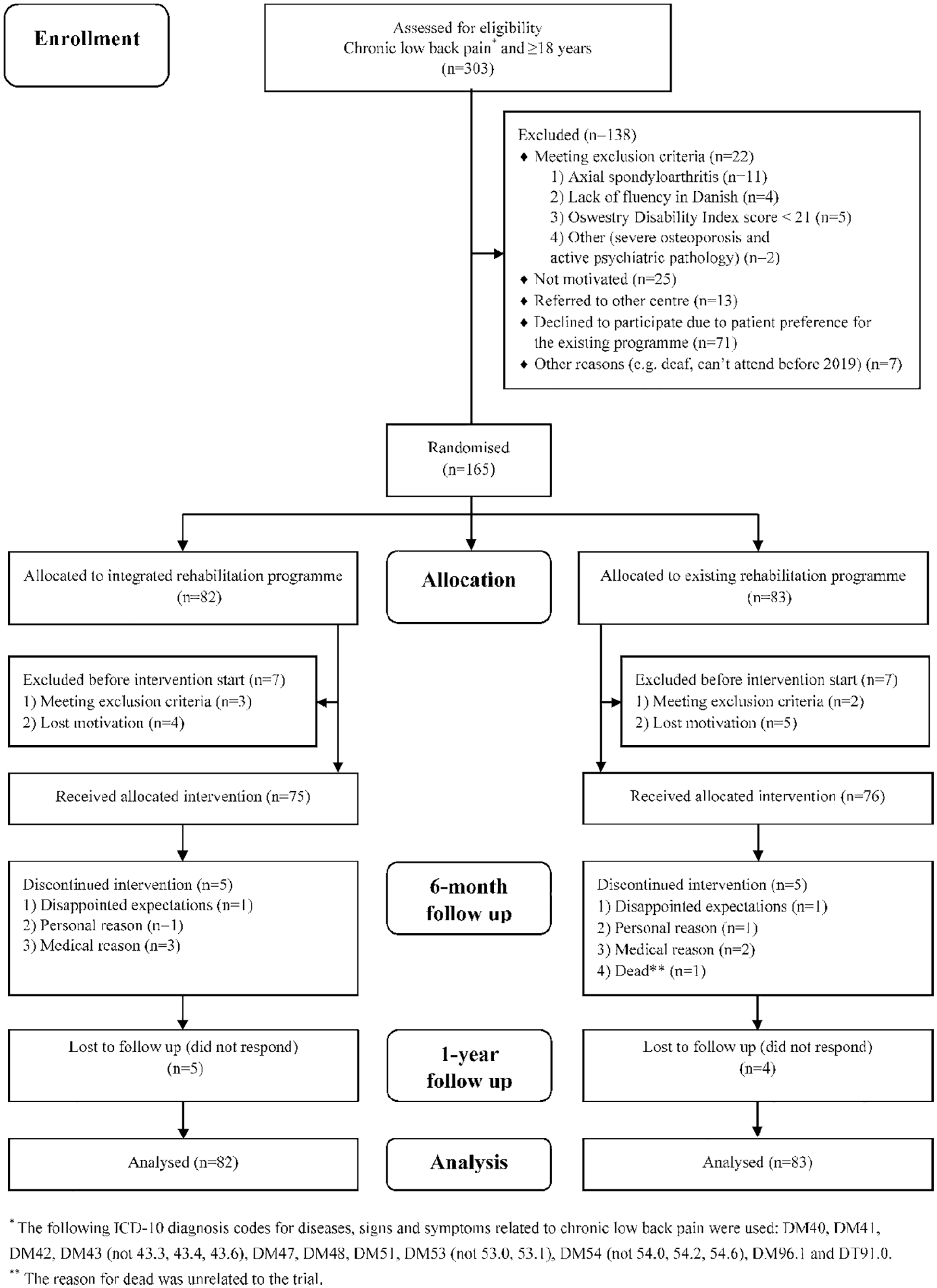
Flow-chart of participants through the trial.
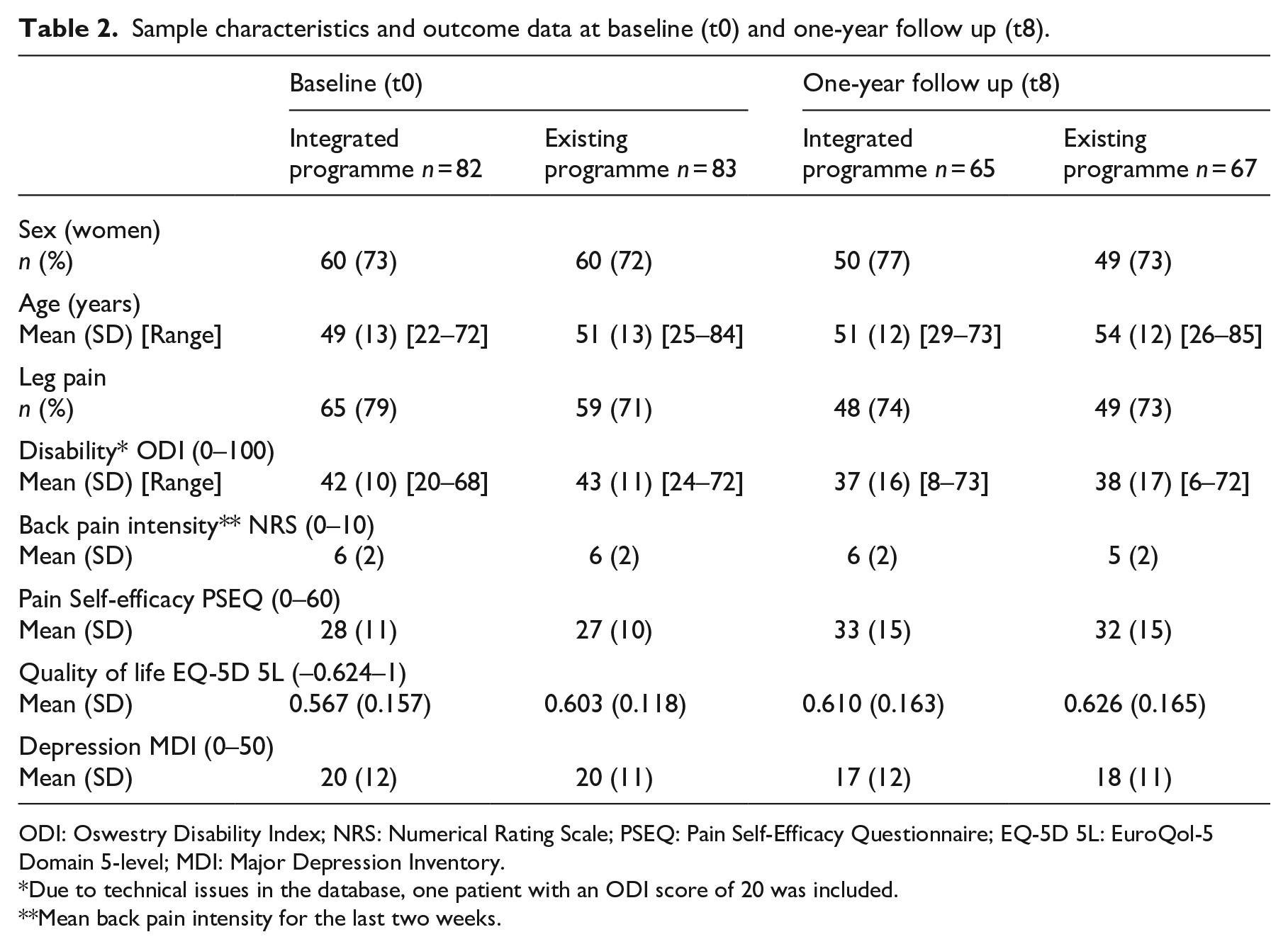
Sample characteristics and outcome data at baseline (t0) and one-year follow up (t8) are displayed in Table 2; these were comparable between programmes at baseline (t0). For further details on sample characteristics at baseline (t0), see the six-month follow-up paper. 10 There were no adverse events or deaths related to either of the rehabilitation programmes.
Sample characteristics and outcome data at baseline (t0) and one-year follow up (t8).
ODI: Oswestry Disability Index; NRS: Numerical Rating Scale; PSEQ: Pain Self-Efficacy Questionnaire; EQ-5D 5L: EuroQol-5 Domain 5-level; MDI: Major Depression Inventory.
Due to technical issues in the database, one patient with an ODI score of 20 was included.
Mean back pain intensity for the last two weeks.
The mean difference of –0.53 (95% CI; –4.08; 3.02) in the change in back-specific disability between rehabilitation programmes was neither statistically nor clinically significant (Table 3).
Summary of one-year follow up outcome data on between-group and within-group differences on primary and secondary outcomes.
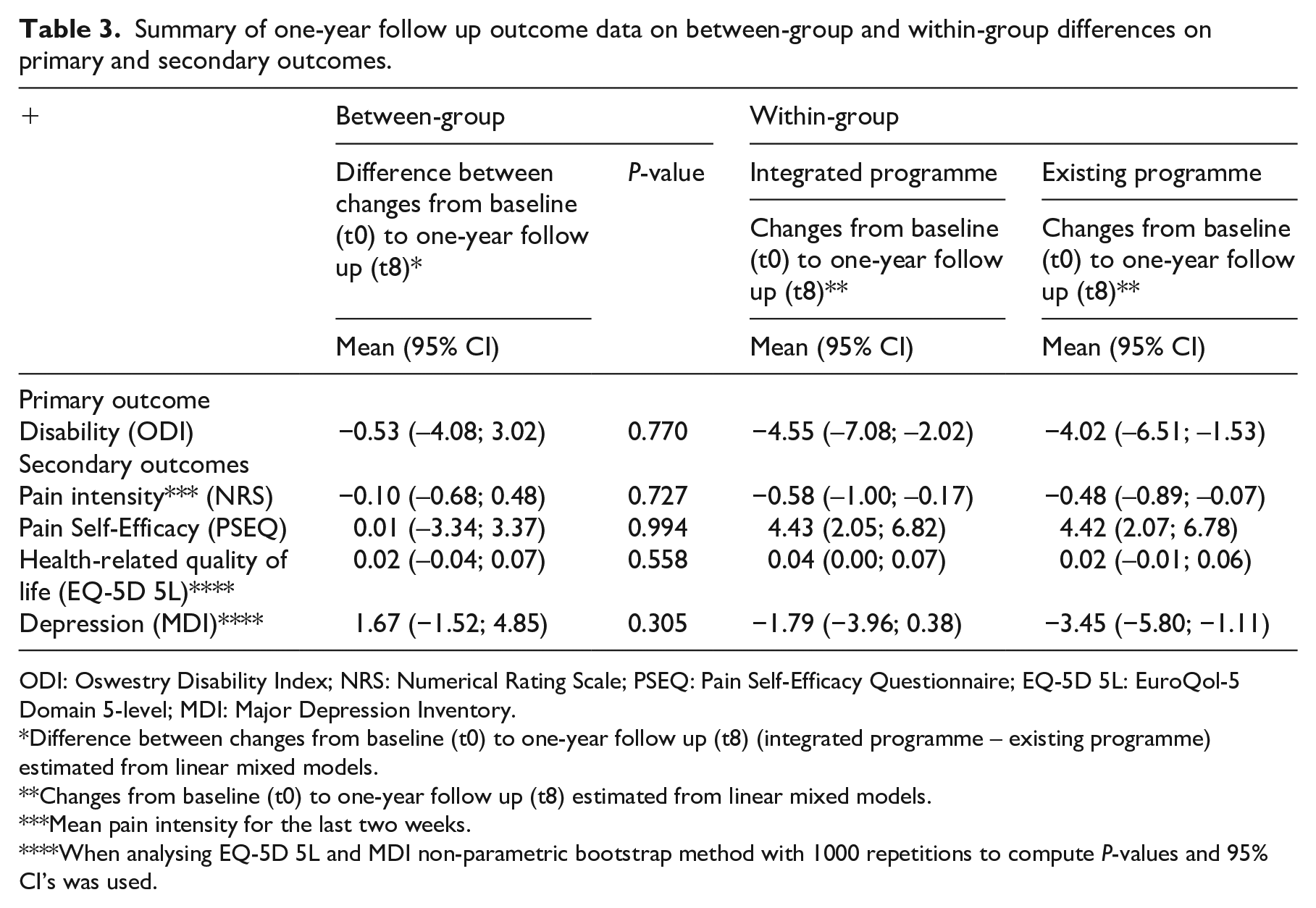
ODI: Oswestry Disability Index; NRS: Numerical Rating Scale; PSEQ: Pain Self-Efficacy Questionnaire; EQ-5D 5L: EuroQol-5 Domain 5-level; MDI: Major Depression Inventory.
Difference between changes from baseline (t0) to one-year follow up (t8) (integrated programme – existing programme) estimated from linear mixed models.
Changes from baseline (t0) to one-year follow up (t8) estimated from linear mixed models.
Mean pain intensity for the last two weeks.
When analysing EQ-5D 5L and MDI non-parametric bootstrap method with 1000 repetitions to compute P-values and 95% CI’s was used.
No evidence of a difference in development in the Oswestry Disability Index score over time was found (χ2(3) = 0.12, p-value = 0.989) (Figure S1). Further, there were no statistically significant differences between rehabilitation programmes for any of the secondary outcomes at the one-year follow up (Table 3). Figures illustrating the secondary outcomes are provided in Supplementary file 2 (supplementary data, online only).
In the integrated programme, the average decrease in Oswestry Disability Index scores was from 42 (95% CI: 39; 44) at baseline to 37 (95% CI: 33; 41) at the one-year follow up (Table 2). In the existing programme the average decrease in Oswestry Disability Index scores was from 43 (95% CI: 40; 45) at baseline to 38 (95% CI: 34; 43) at the one-year follow up (Table 2).
Neither the secondary analysis adjusted for waiting time, nor the secondary analyses replacing missing values by the average of non-missing scores at the particular time point changed the primary result. Replacing missing values by the worst possible score (=100) for the integrated programme and by the best possible score (=0) for the existing programme changed the results (mean difference: 19.79 (95% CI: 13.80; 25.77), p = 0.000).
The outcome trajectories including all measurement time points from t0-t8 illustrate that mean changes over time were similar in patients in both rehabilitation programmes (Figure S2).
Discussion
At one-year follow up, the integrated programme comprising inpatient stays alternating with home-based activities and booster sessions did not improve back-specific disability or any other outcomes in patients with chronic low back pain when compared with an existing four-week inpatient programme. The results are in line with those from the six-month follow up. 10 However, as they are contrary to our hypothesis, they warrant scrutiny, not only because of design choices for the integrated programme, but also of the evidence base upon which the integrated programme was built.
In terms of design choices, the integrated programme was designed to support the integration of knowledge, skills, and behaviours, acquired during an inpatient stay, into the daily life of the patient. The justification for the integrated programme was based on a thorough development process and feasibility testing following the Medical Research Council’s guidance on complex interventions. 20
In the development stage, firstly, we drew on recent clinical guidelines2,3 and other evidence 4 confirming that multidisciplinary rehabilitation is recommended as a second-line treatment for patients with chronic low back pain. Secondly, we identified the biopsychosocial approach5,7 and the Chronic Care Model 8 as recognised theories to justify the way in which the integrated programme was delivered. Finally, when modelling processes and outcomes, we aimed for a high degree of patient and public involvement. Scrutinising the development stage, in general, it still seems as a reasonable foundation upon which to build the integrated programme. However, the particular theories5,7,8 underpinning the integrated programme, and the primary outcome measure chosen 16 could be questioned. In terms of the biopsychosocial approach,5,7 a Cochrane review 4 found evidence favouring multidisciplinary rehabilitation when aligned with the biopsychosocial model. Furthermore, the biopsychosocial approach has been widely accepted as appropriate in patients with chronic low back pain since the 1980s, 21 and it still is. 6
The potential for better outcomes was based on adding booster sessions underpinned by the Chronic Care Model. 8 When it comes to adding booster sessions to interventions delivered to patients with musculoskeletal conditions, the evidence is equivocal, and thus, questionable.22–26 The choice of the Oswestry Disability Index as the primary outcome measure also warrants elaboration. The lack of any difference may be explained by the fact that since the integrated programme aimed at integrating knowledge, skills and behaviours into the patients’ daily lives, it may have been better for the primary outcome measure to measure these domains. There was, however, no validated outcome measures to capture this. Furthermore, we wished to evaluate an outcome which is broadly acknowledged in this population. Thus, achieving improvements in disability and other outcomes, were seen as proxies of successful integration of knowledge, skills and behaviours. Given the broad biopsychosocial coverage of the different outcomes used in the trial, and the consistent finding of no between-group differences, it is therefore unlikely that the result of the trial would have been different had we selected a different primary outcome.
The feasibility stage resulted in fine-tuning of the administrative procedures, and following that, we believed that the integrated programme had the potential to be successfully implemented and evaluated. However, a nested process evaluation revealed unexpected challenges and, with the value of hindsight, running a pilot randomised controlled trial would have been beneficial. The process evaluation revealed challenges implementing important elements of the integrated programme (pamphlet and phone calls) which were developed to support the intended integration of knowledge, skills, and behaviours into the patient’s daily life. Further, it revealed administrative challenges, including postponements and low adherence to the six-month follow-up visit. With these findings, it became obvious that the logistics of implementing the integrated programme in daily clinical practice was a challenge. This could potentially have caused bias in favour of the existing programme.
In terms of the evidence base, six trials comparing two or more rehabilitation programmes in patients with chronic low back pain using disability as the primary outcome were identified.22,27–31 These trials had some substantial differences. Firstly, the populations included had different levels of disability at baseline. Secondly, four different measurements (the Oswestry Disability Index,27,28 the Roland Morris Disability Questionnaire,30,31 the Quebec Back Pain Disability Scale, 29 and the Pain Disability Index 22 ) were used. Thirdly, some compared different dose and content,28–30 and some compared identical rehabilitation programmes but added a further component to one of the rehabilitation programmes for example, involvement of spouses, 31 more specifically tailored interventions, 27 or subsequent booster sessions. 22 Lastly, two trials had short-term follow up (three months or less),27,28 others medium-term follow up (three to less than 12 months),29,30 and yet others incorporated long-term follow up (12 months or more).22,27,30,31 These differences limit direct comparison with the current trial. However, regardless of the differences, the results of the six trials were similar to the current trial, namely no significant differences in disability when comparing two or more rehabilitation programmes.
In general, evidence indicates that rehabilitation as a process is beneficial, 32 and it supports the effect of rehabilitation in the field of chronic low back pain.1–4 However, when adding our results to the current evidence base, it seems difficult to demonstrate if and how much dose, content and delivery of a specific multidisciplinary rehabilitation programmes matters. 32 It could be discussed whether the reasons for the repeated null effect in the trials could be due to trial features or quality. Rather, it should be considered whether it is owing to the comprehensive nature of the rehabilitation programmes being compared, or whether the complex interplay between person-specific biopsychosocial factors driving disability in patients with chronic low back pain makes it difficult to improve disability with programmes that more or less are one-size-fits-all. 32
The trial had several strengths including randomisation and allocation concealment, the two-arm parallel design, blinding of the researcher performing the statistical analysis, high adherence and follow-up rates, as well as equal lost to follow-up rates in the two rehabilitation programmes. Further strengths are the thorough development and feasibility tests of the integrated programme including patient and public involvement and a nested process evaluation, 10 the use of the TIDieR checklist to justify and describe the integrated programme, 9 and the preparation of a statistical analysis plan (Supplementary file 1 (supplementary data, online only)).
One limitation of the trial is the lack of measured adherence to home-based activities. Hence, whether patients from the integrated programme actually did integrate acquired knowledge, skills and behaviours into their daily lives was not directly evaluated. Another limitation was the risk of contamination, since the trial was delivered by non-blinded providers to non-blinded patients in the same rehabilitation centre, at the same time, and whether providers and patients in the existing programme were inspired by the integrated programme and patients took the opportunity to integrate knowledge, skills and behaviours into their daily lives is unknown.
Providers and decision-makers ought to know, and patients need to be reassured, that evidence supports the effectiveness of multidisciplinary rehabilitation.1–4,32 Currently, there is no evidence to guide the decision about the most optimal way to deliver a multidisciplinary rehabilitation programme for patients with chronic low back pain. In light of the plethora of research in this field, new intervention studies are probably not the best solution to address this challenge. Maybe we need to gain a wider perspective and look into new actions required by the political, public health, and health care systems. 33
Clinical messages
Changing the delivery of an inpatient rehabilitation programme does not lead to improved long-term back-specific disability for patients with chronic low back pain.
Chronic low back pain is driven by biopsychosocial factors, and it seems challenging to target each individual patient primarily with a one-size-fits-all approach.
Supplemental Material
Figure_S1 – Supplemental material for The effect of an integrated multidisciplinary rehabilitation programme for patients with chronic low back pain: Long-term follow up of a randomised controlled trial
Supplemental material, Figure_S1 for The effect of an integrated multidisciplinary rehabilitation programme for patients with chronic low back pain: Long-term follow up of a randomised controlled trial by Anne Mette Schmidt, Trine Bay Laurberg, Line Thorndal Moll, Berit Schiøttz-Christensen and Thomas Maribo in Clinical Rehabilitation
Supplemental Material
Supplementary_file_1 – Supplemental material for The effect of an integrated multidisciplinary rehabilitation programme for patients with chronic low back pain: Long-term follow up of a randomised controlled trial
Supplemental material, Supplementary_file_1 for The effect of an integrated multidisciplinary rehabilitation programme for patients with chronic low back pain: Long-term follow up of a randomised controlled trial by Anne Mette Schmidt, Trine Bay Laurberg, Line Thorndal Moll, Berit Schiøttz-Christensen and Thomas Maribo in Clinical Rehabilitation
Supplemental Material
Supplementary_file_2 – Supplemental material for The effect of an integrated multidisciplinary rehabilitation programme for patients with chronic low back pain: Long-term follow up of a randomised controlled trial
Supplemental material, Supplementary_file_2 for The effect of an integrated multidisciplinary rehabilitation programme for patients with chronic low back pain: Long-term follow up of a randomised controlled trial by Anne Mette Schmidt, Trine Bay Laurberg, Line Thorndal Moll, Berit Schiøttz-Christensen and Thomas Maribo in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors are grateful to patients, providers, administrative and management staff at Sano who made the trial possible. Thanks are also extended to statistician Jens Søndergaard Jensen for his supervision, and Professor Nadine E Foster is thanked for review of this paper.
Author contributions
All authors have contributed substantially to (1) conception and design, or analysis and interpretation of data; (2) drafting or revising the article critically for important intellectual content; and (3) final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The trial was funded by Sano, Aarhus University, the Danish Rheumatism Association, and Familien Hede Nielsens Fond. None of the funders had any influence on the trial.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.