
Abstract
Objective:
To investigate the effect of a new therapeutic approach, using an oscillating rod to strength the pelvic floor and deep abdominal musculature and to speed up recovery of continence after radical prostatectomy.
Design:
Prospective randomized controlled clinical trial.
Setting:
Inpatient uro-oncology rehabilitation clinic.
Subjects:
Ninety-three (intervention group (IG)) and ninety-one patients (control group (CG)) with urinary incontinence after prostatectomy were examined.
Intervention:
All patients were randomly allocated to either standard pelvic floor muscle exercises and oscillating rod therapy (IG) or standard pelvic floor muscle exercises and relaxation therapy (CG).
Main outcome measures:
Urinary incontinence (1- and 24-hour pad test) was assessed, and health-related quality of life (HRQL; Functional Assessment of Cancer Therapy-Prostate (FACT-P) questionnaire) was measured for all patients before and after three weeks of treatment.
Results:
One hundred and eighty-four patients (mean (SD) age: 64.1 (6.94) years) completed the study. The IG showed a significant reduction in urinary incontinence (1-hour pad test: P = 0.008, 24-hour pad test: P = 0.012) and a significant improvement of HRQL (P = 0.017) compared with CG. Continence was significantly improved in both groups (1-hour pad test: 22.6–8.5 g (IG) vs. 23.0–18.1 g (CG)/24-hour pad test: 242.9–126.7 g (IG) vs. 237.6–180.9 g (CG)).
Conclusion:
The study demonstrated that a combination of conventional continence exercises and the new oscillation rod training increased abdominal and pelvic floor musculature and speeded up recovery of continence after radical prostatectomy.
Introduction
Urinary incontinence is a common, in most cases a temporary, functional problem after radical prostatectomy and other treatments for carcinoma of the prostate. Postprostatectomy incontinence has a major impact on health-related quality of life (HRQL) and patient satisfaction. 1 The aim of rehabilitation should be to quickly overcome incontinence and reintegration into occupation and participation in social life. 2
There are several therapies that help treat urinary incontinence, including some that focus on pelvic floor muscles. Pelvic floor muscle exercises, biofeedback, electrical stimulation and external magnetic innervation are different therapeutic options used for the conservative treatment of postprostatectomy incontinence. 3
In addition to the pelvic floor muscles, the deep abdominal and back muscles play a decisive role in the treatment of urinary incontinence. With training of the deep abdominal muscles which stabilize the trunk musculature, the pelvic floor is trained at the same time and thereby urinary incontinence is improved.4,5 This type of training is more effective than specific pelvic floor strength training for treating incontinence.4,5 Currently, there are only a small sample of randomized controlled trials which address the combination of pelvic floor muscle training and deep abdominal muscle activation after radical prostatectomy, for example, Pedriali et al. 6 and Gomes et al. 7 demonstrated positive effects concerning continence using Pilates exercises in combination with continence training. Interestingly, the approaches used in these studies were based on voluntary activation of deep abdominal muscles. Both voluntary and involuntary muscle activation is a necessary prerequisite for participation in normal life. Therefore, the involuntary activation should also take into account therapeutic approaches concerning postprostatectomy incontinence. Anders et al. 8 demonstrated specific involuntary activations characteristic of the trunk muscles (rectus abdominis muscle, obliquus abdominis muscle, multifidi muscles and erector spinae muscle) using an oscillation rod in healthy subjects. In the latter study, the trunk muscles were activated by a forward and backward movement of the trainings device. 8 Hodges 9 even demonstrated a feedforward function. This means that the transversus abdominis muscle is also activated by voluntary arm movements. Consequently, the continence system (pelvic floor muscles) is activated by the coactivation of the local musculature of the trunk (multifidi muscle and transversus abdominis muscle).4,5
Due to physiological considerations and experiences from trunk muscle activation through an oscillating rod therapy, we investigated the effects of a sensorimotor training with an oscillation rod compared with pelvic floor muscle training. In comparison to recent studies, we hypoth-esized that a combination of a specific involuntary trunk muscle activation and the voluntary activation of pelvic floor muscles would reduce the recovery time after radical prostatectomy and improve the urinary incontinence and HRQL. Based on the known success of supervised and controlled daily continence training, we investigated an additional sensorimotor treatment option in order to help increase the speed of recovery of urinary continence.10,11
Therefore, the aim of this study was to assess the effects of sensorimotor training with an oscillation rod compared with standard pelvic floor muscle training on reduction of incontinence level, recovery time and the HRQL.
Methods
This was a prospective, randomized controlled trial. The Vogtland-Rehabilitation Hospital Bad Elster jointly conducted this study between September 2016 and December 2017. The study design was approved by the ethics committee of Chemnitz University of Technology (# V-146-TM-HS-Incontinence-29062016). The study was also registered in the German Clinical Trials Register (ID: DRKS00011028). All the patients gave their written informed consent.
Two hundred patients were consecutively recruited from a urological rehabilitation hospital in Bad Elster with urinary incontinence after radical prostatectomy.
The patients were examined by a physician for inclusion criteria, exclusion criteria and psychological problems. The inclusion criteria were radical prostatectomy for prostate cancer, postprostatectomy urinary incontinence (>1 g and <200 g urine loss/1-hour pad test), normal operative and postoperative course and time interval to surgery less than four weeks. The exclusion criteria included continence after prostatectomy, reduced physical capacity due to relevant comorbidities, no patient consent, incomplete data and pelvic floor exercises prior to surgery. Sixteen patients were excluded from the study because they met one or more of the exclusion criteria.
After initial medical examination, patients received comprehensive information about the study, they provided written consent and were randomized in a parallel design to the intervention (n = 93) or control group (CG; n = 91) and were evaluated before and after three weeks of rehabilitation.
All patients completed a standard treatment program, and this consisted of continence exercises, general endurance and moderate strength training for three weeks.
The standard continence training for both groups included pelvic floor muscle training conducted by a specialized physiotherapist with a three-year education and a further education with a focus on continence training. The training protocol was standardized based on the work of Dorey et al. 12 and the exercises were performed daily for 30 minutes over three weeks. In the first lesson, the physiotherapist gave verbal information about the pelvic floor anatomy and its function using anatomy models and illustrations. The patients then learned the correct muscle contraction and how to contract without adjacent muscles (e.g. abdominal or gluteal muscles). Exercises were carried out in different positions (lying, sitting and standing) and in everyday life situations.
The intervention group (IG) performed daily supervised continence training and additional coordination training for the pelvic floor muscle using an oscillating rod. The training device was a Bioswing Improve 150 (Haider Bioswing GmbH, Dechantseeser Str. 4, 95704 Pullenreuth, Germany). It was demonstrated in an introduction lesson followed by daily training sessions for 30 minutes. Supplemental Figure S1 provides detailed information about the training device, the three exercises and how it works.
The CG performed daily relaxation therapy in addition to supervised continence training. In the former, the patients listened to relaxation music in a lying position for 30 minutes.
The data of the patients with respect to age (years), height (cm), weight (kg), body mass index (BMI; kg/m²), abdominal girth (cm), waist/hip ratio (cm), catheter days, surgical technique and tumor classification were collected during the anamnesis at the initial and the final medical examination.
The functional results of the treatment process were evaluated using the 1- and 24-hour pad test (urinary incontinence symptoms). The 1-hour pad test was performed based on the recommended protocol of the International Continence Society. Patients were asked to empty their bladder before the test. The pads were weighed and inserted before the test. After inserting a pad, the patients had to drink 500 mL of fluid within 15 minutes. Then they performed standardized exercises, and after 1 hour, the pads were reweighed to calculate urine loss. 13
The 24-hour pad test was carried out as follows. The patient was briefed on the test procedures, received the pads and was asked to keep a micturition protocol. The pads were weighed and one pad was inserted before the test. The pads were worn over one day and night. The fluid volume and number of used pads were noted in the micturition protocol. The pads were changed by the patient, collected and weighed after 24 hours. 14 Data of 1- and 24-hour pad test were independently documented by a physiotherapist and a sports scientist and were recorded at the beginning and at the end of the three-week study period.
In order to evaluate the effects of incontinence on the HRQL, the Functional Assessment of Cancer Therapy-Prostate (FACT-P) self-administered FACT-P questionnaire was used. 15 The focal points were urinary incontinence, erectile dysfunction, pain and HRQL. The individual items were added to a total score. 16 Data of the HRQL questionnaire were documented by a physiotherapist and a sports scientist at the beginning and at the end of the three-week study period. The questionnaire was handed out after the initial and final medical examination and completed by the patient.
Our sample size was analyzed using a sample size calculator. 17 There was a two-sided alpha value of 0.05, effect size (d) of 0.5, a power of 0.9 and a sample size of 86 per group. To allow for drop-outs, the sample size was set at 200.
The randomization to the intervention and CG was carried out using a computer-generated list of random numbers. The allocation sequence was generated by the study leader. Patients were randomly assigned following simple randomization procedures (even number—IG; odd number—CG). The numbers were placed in numbered, opaque and sealed envelopes and opened after the patient’s initial medical examination. The person collecting the data knew whether the patients were in either the intervention or CG. In this study, blinding was not performed, because the treatment was disclosed to all involved (physician, patient and physiotherapist). Patients were informed about the investigation, because the study was performed as part of an inpatient rehabilitation program.
All data were entered into a spreadsheet (Microsoft Excel 2016). For data analysis, the statistical software package SPSS Statistics Version 17 was used. All results were represented as mean and standard deviation. The analysis was carried out using parametric tests on the basis of the central limit theorem. For the comparison of baseline demographics (age, size, weight, BMI, abdominal girth, waist/hip ratio and catheter days), an independent t-test was used. The frequencies in percent and actual number for surgical technique und tumor classification were determined with descriptive statistics.
To evaluate urine loss (1/24-hour pad test) and HRQL (FACT-P) within the groups before and after three weeks of treatment, the dependent t-test was used. The independent t-test was applied to identify changes of the 1- and 24-hour pad test and FACT-P between intervention and CG. The severity of incontinence was determined in accordance with Hahn and Fall. 18 The significance level of 0.05 was chosen.
The effect size for dependent and independent groups was determined in accordance with Morris and DeShon 19 and interpreted using Cohen’s d. 20 Cohen 20 reported the following intervals for d: 0.2–0.4 small effect, 0.5–0.7 intermediate effect and >0.8 large effect.
Results
One hundred and eighty-four patients (mean (SD): age 64.1 (6.94) years) met all study inclusion criteria and completed the study successfully. Their data were appropriate for statistical analysis (Figure 1).
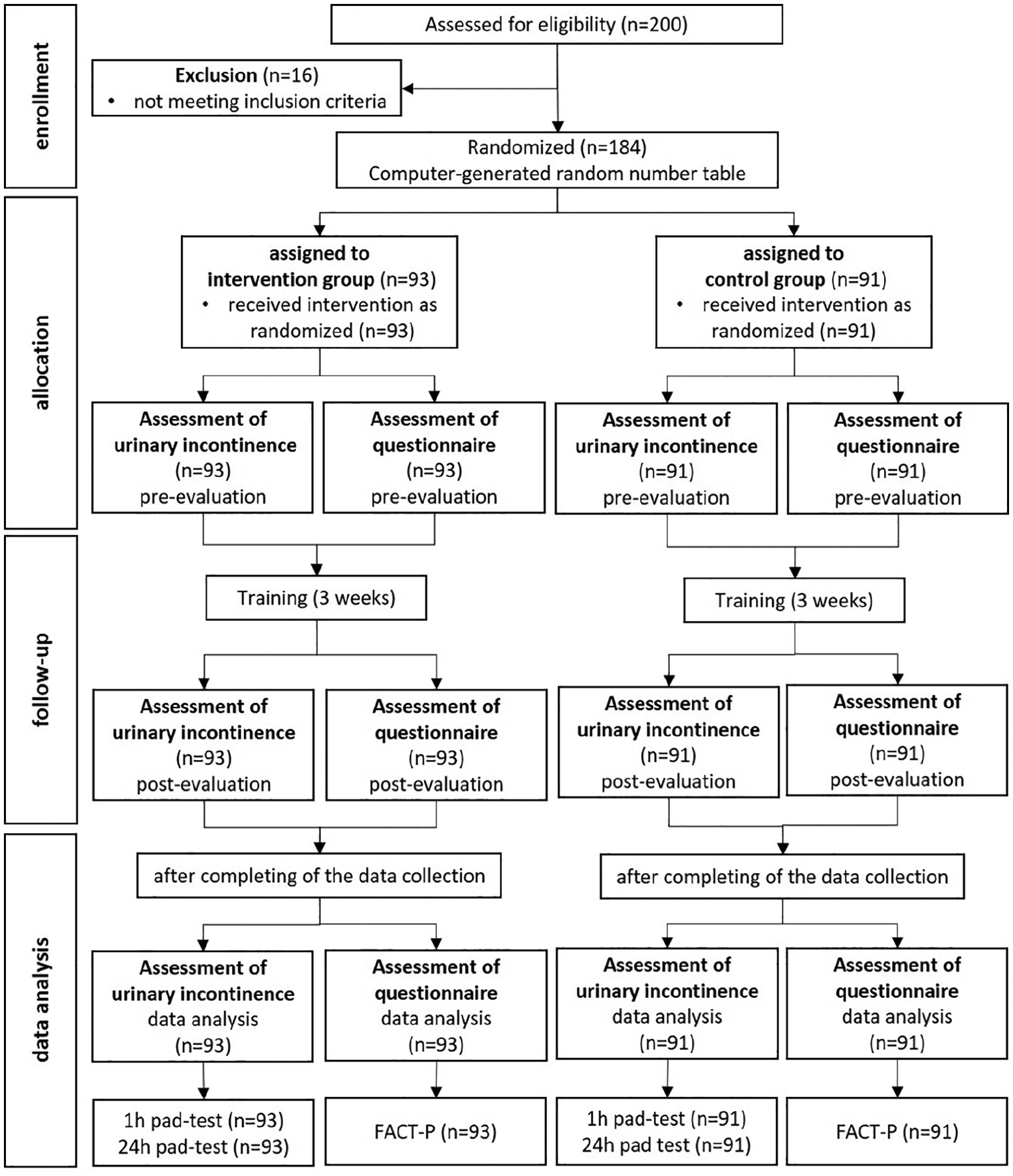
Design of the study (CONSORT flow diagram).
The baseline demographic and clinical characteristics of the patients are presented in Table 1. The analysis between the two groups indicated no significant differences in the demographic characteristics (Table 1). The comparison of the groups revealed no significant differences at baseline of clinical characteristics for surgical technique and tumor classification (P > 0.05; Table 1).
Baseline values of demographic and clinical characteristics (mean (SD)).
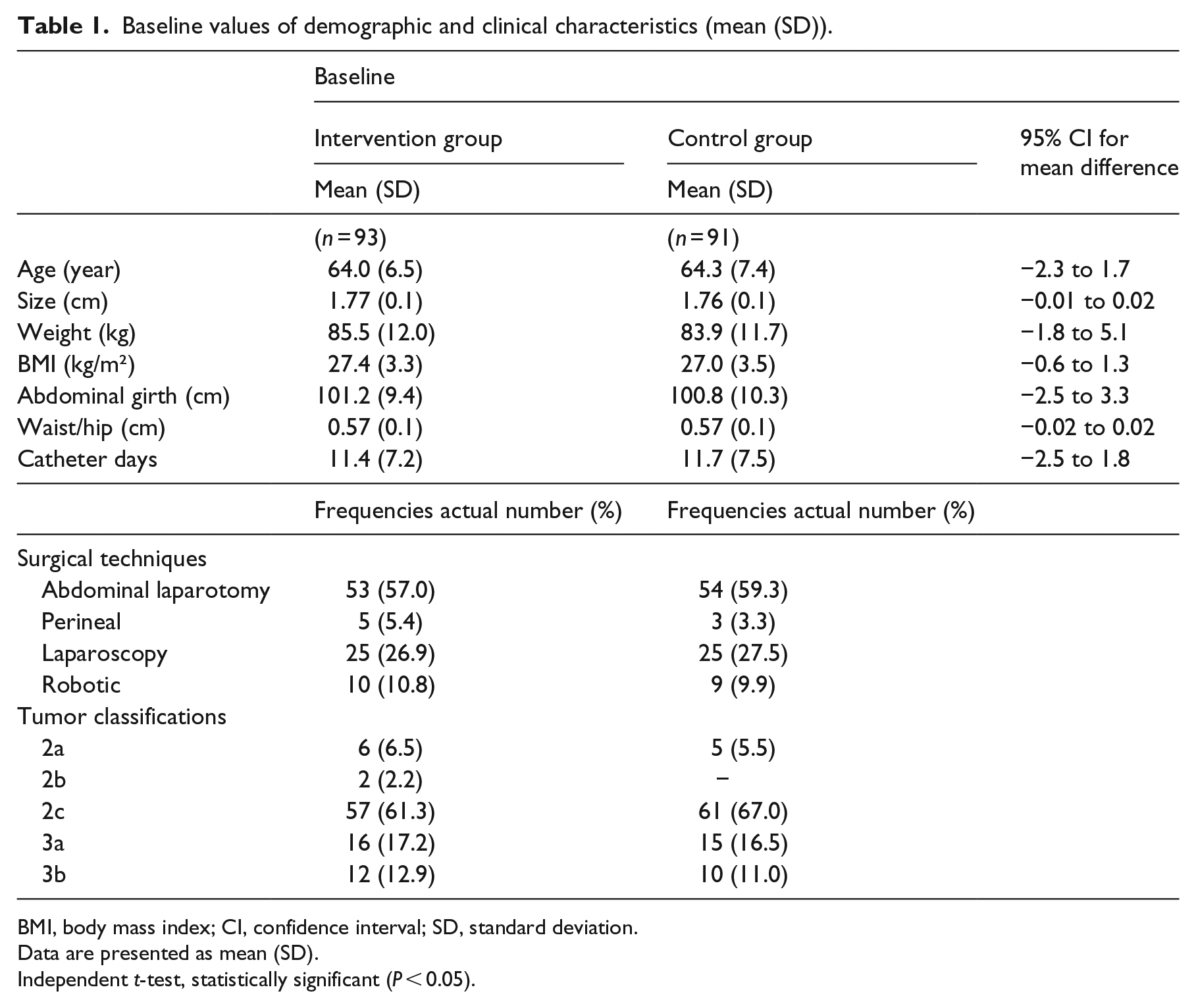
BMI, body mass index; CI, confidence interval; SD, standard deviation.
Data are presented as mean (SD).
Independent t-test, statistically significant (P < 0.05).
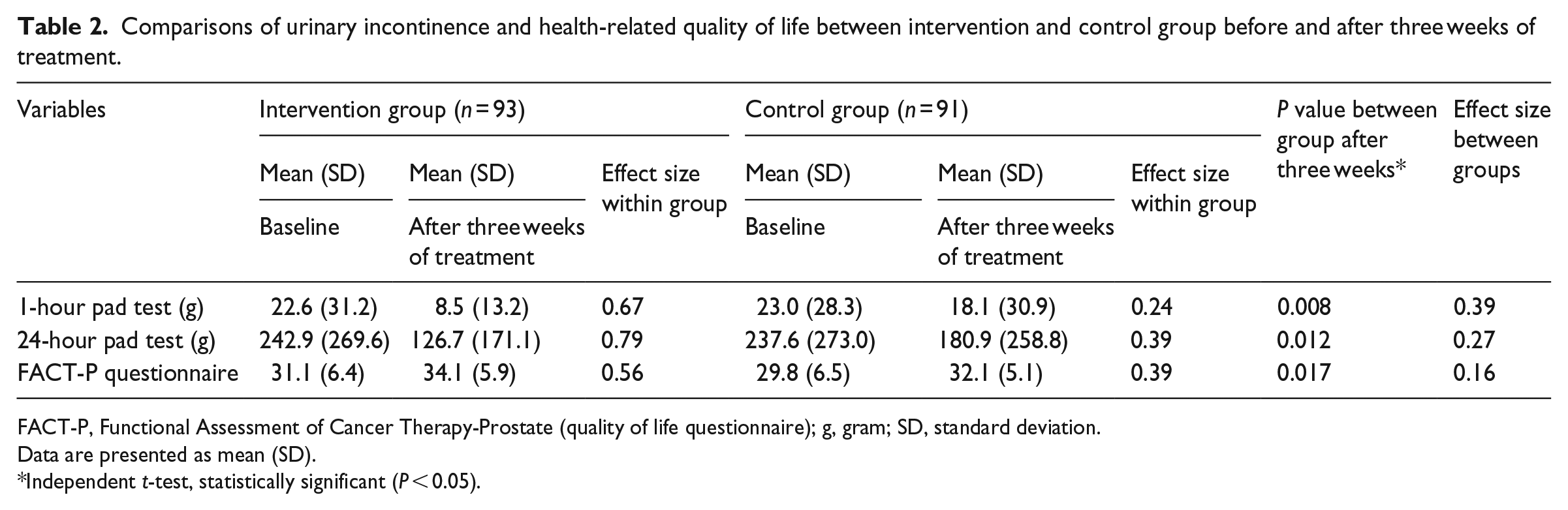
The comparisons of urinary incontinence (1- and 24-hour pad test) and HRQL (FACT-P questionnaire) before and after three weeks of treatment between the groups is shown in Table 2. There was no significant difference between intervention and CG at the baseline of the study for the 1- and 24-hour pad test and HRQL (P > 0.05).
Comparisons of urinary incontinence and health-related quality of life between intervention and control group before and after three weeks of treatment.
FACT-P, Functional Assessment of Cancer Therapy-Prostate (quality of life questionnaire); g, gram; SD, standard deviation.
Data are presented as mean (SD).
Independent t-test, statistically significant (P < 0.05).
Significant improvements of urinary incontinence were found measured with the 1- and 24-hour pad test in both study groups. However, the reduction in urine loss in the IG was significantly higher compared with in the CG (1- and 24-hour pad test P < 0.01 between groups; Table 2).
The effect size of the IG after three weeks of treatment showed an intermediate effect for 1-hour pad test and a large effect for 24-hour pad test. The CG demonstrated only a small effect for 1- and 24-hour pad test (Table 2). The effect size between groups is shown in Table 2.
The subgroup analysis of the 1-hour pad test can be seen in Table 3. There was a statistically significant improvement of urinary incontinence in the IG at all incontinence severity levels (P = 0.0001 within group). In comparison, the CG demonstrated only a significant improvement in urinary incontinence in patients with mild urine loss (P = 0.016 within group). The effect size of the IG after three weeks of treatment showed at all incontinence severity levels a large effect and for the CG a small effect. Reduction of urine loss measured with the 1-hour pad test was significantly higher in the IG than in the CG after three weeks of treatment at all incontinence severity levels (mild, P = 0.051; moderate, P = 0.094; large, P = 0.003; between groups). The effect size between groups is shown in Table 3.
Subgroup analysis of the 1-hour pad test between intervention and control group before and after three weeks of treatment.
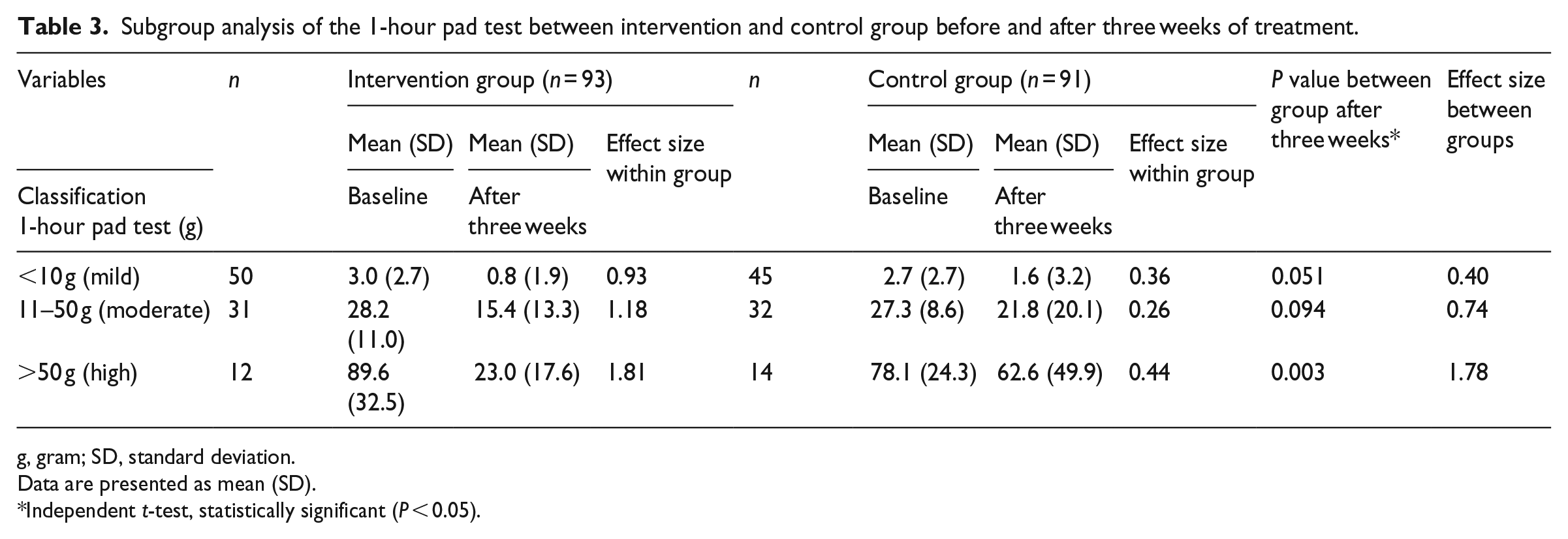
g, gram; SD, standard deviation.
Data are presented as mean (SD).
Independent t-test, statistically significant (P < 0.05).
The results show that early continence recovery will result in an improvement of HRQL and increased patient satisfaction. There were significant improvements in HRQL in the intervention (P < 0.001) and the CG (P = 0.001; Table 2). The effect size of the IG after three weeks of treatment showed an intermediate effect and for the CG a small effect (Table 2). Improvement for HRQL measured with FACT-P questionnaire was significantly higher in the IG compared with CG after three weeks of treatment (P = 0.017; between groups). The effect size between the groups is shown in Table 2.
The subgroup analysis of the 1-hour pad test and HRQL is presented in Table 4. Early continence recovery did not result in a higher improvement of HRQL for the IG in comparison to CG (Table 4).
Subgroup analysis of 1-hour pad test compared with health-related quality of life for intervention and control group before and after three weeks of treatment.
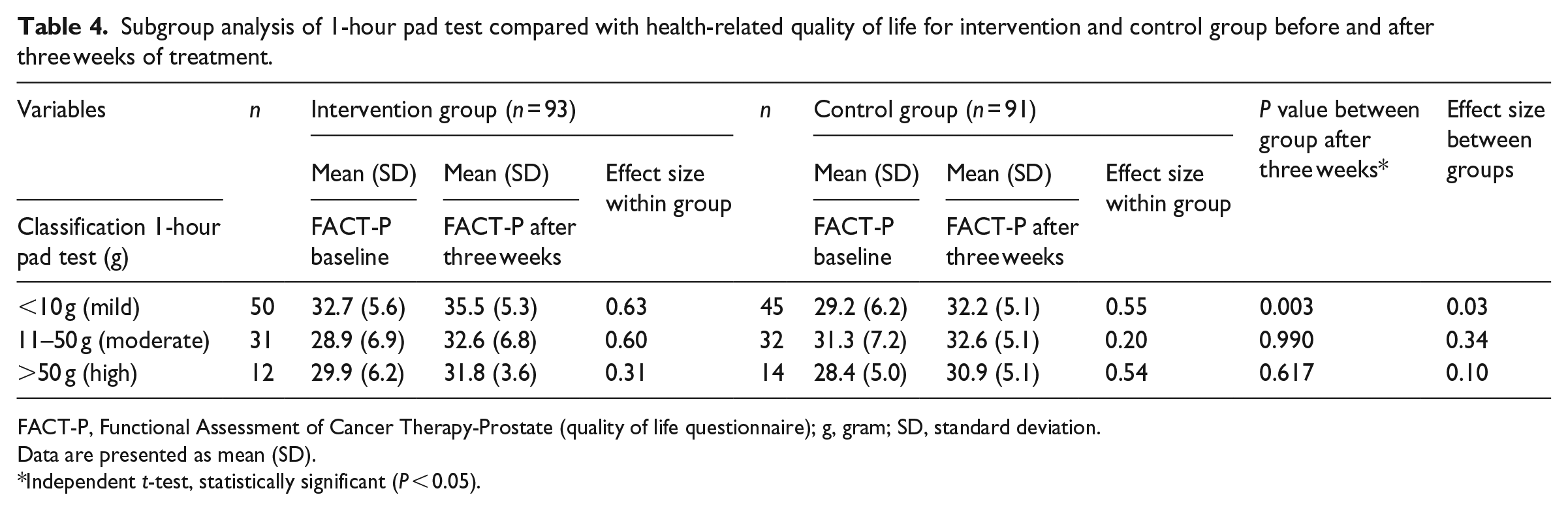
FACT-P, Functional Assessment of Cancer Therapy-Prostate (quality of life questionnaire); g, gram; SD, standard deviation.
Data are presented as mean (SD).
Independent t-test, statistically significant (P < 0.05).
Discussion
This study was designed to assess the effects of sensorimotor training with an oscillation rod compared with standard pelvic floor muscle training on reduction of incontinence level, recovery time and the HRQL. The results showed that a combination of continence exercises and oscillating rod therapy is a more effective therapeutic approach compared with standard continence training alone for overcoming stress urinary incontinence after radical prostatectomy.
Patients with severe stress urinary incontinence above 50 g measured with the 1-hour pad test can benefit most from the new treatment approach. Consequently, the HRQL and patient satisfaction are enhanced versus the CG. This point once again illustrates the importance and added value of the oscillation rod in combination with standard continence training for everyday clinical practice.
The first hypothesis of our study investigated that a combination of standard continence exercises and specialized coordination training is a more effective therapeutic approach for overcoming stress urinary incontinence than standard continence training alone. This study showed that urinary incontinence improved significantly for both intervention and CG. Both groups could benefit from the different therapies. These results can be confirmed by studies examining the effects of conservative therapy on urinary incontinence following radical prostatectomy. 3 The majority of the studies compared pelvic floor training supplemented by biofeedback or electrotherapy. 3 Comparisons with our study are difficult because of the different study periods and urinary incontinence values after surgery.
Another problem is that various risk factors can influence urinary incontinence following a radical prostatectomy. These include patients’ age, bladder dysfunction and lack of surgical expertise. 21 In this study, there was no significant difference between the intervention and CG (baseline) in terms of age, size, weight, abdominal girth, BMI, waist/hip ratio, catheter days, tumor classification and surgical technique. This means that these risk factors did not affect the results of the study. In agreement with the study of Cambio and Evans, 22 body weight had no influence on postprostatectomy incontinence.
The question is, what effect has the oscillation rod in combination with continence exercises compared with a CG that performed continence training alone. The results showed that the IG achieved significantly better urinary incontinence values (1- and 24-hour pad test) compared with CG after three weeks of rehabilitation. The additional effect of sensorimotor training with the oscillation rod measured by the effect size is only small. We have been unable to find any other studies using a specific intervention to compare the effect sizes with other therapies.
Previous studies using an additional passive approach alone like electrical and magnetic stimulation were not that successful. 3 Electrical stimulation of the pelvic floor muscles using different kinds of abdominal, perineal, penile and rectal electrodes is not that specific and focused on pelvic floor physiology. Electrical impulses aid sensory perception and thereby support the conventional continence training approach. The latter treatment is useful in patients with significant problems in body and pelvic floor perception and consequently greater urine loss only. The same can probably be said about magnetic stimulation. These conclusions are supported by the results of previous studies.23–26
In our study, urinary incontinence was evaluated by 1- and 24-hour pad test. A few studies used these tests to evaluate urinary incontinence.27,28 In addition to the pad tests, there are other objective measurement parameters, such as frequency of micturitions (over 24 hours), number of pad (pad changes per 24 hours) and frequency of urinary incontinence from self-report or diary (incontinent episodes per 24 hours). The advantage of the 1-hour pad test over other procedures is that it runs under standardized conditions and is used to determine the urinary incontinence under stress. 13 The 24-hour pad test is carried out under everyday conditions and gave information about the fatigue of the urethral sphincter and the severity of urinary incontinence.29–31 The disadvantage is that the 24-hour pad test is highly dependent on the number of visits to the toilet, the volume consumed and daily stress. Both tests should be used together to determine urinary incontinence.
The second hypothesis examined that patients with severe stress urinary incontinence will benefit most from the new treatment approach. The results of the subgroup analysis illustrate the advantage of the additional use of the oscillation rod in comparison to continence training alone. In patients with low urinary incontinence levels (<10 g–1-hour pad test), the oscillation rod has only a small benefit. However, patients benefit with urine losses of more than 50 g in the 1-hour pad test most strongly from the oscillation rod. This fact clarifies effect sizes of more than 1. There are currently no publications that have evaluated the minimal clinical difference and the effect size for the 1- and 24-hour pad test. The results and effect sizes clearly demonstrate the clinical value of the oscillation rod in combination with standard continence training. In comparison with the intervention and CG, only a small additional effect for the oscillation rod can be demonstrated for the total sample for the 1- and 24-hour pad test. This circumstance is due to the very large standard deviation of the two tests. The issue is that the amount of urine lost by patients varies from a few grams to over a liter over 24 hours (24-hour pad test). The variation of the continence rates after radical prostatectomy is confirmed by earlier authors.32,33
The third hypothesis tested that early continence recovery will result in an improvement of quality of life and increased patient satisfaction. The results showed that the IG achieved significantly better HRQL values than the CG after three weeks of rehabilitation. This means that early continence recovery will result in an improvement of HRQL. However, the oscillation rod has no direct influence on the HRQL. This fact clarifies the effect sizes of 0.16. We found no publications that have evaluated HRQL with FACT-P questionnaire. Therefore, it is difficult to compare the quality of life with other studies. Most studies used as measurement parameters International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF), King’s Health Questionnaire (KHQ), Short Form 36 (SF-36), European Organisation for Research and Treatment of Cancer-Quality of Life of Cancer Patients (EORTC QLQ C30) und Incontinence Impact Questionnaire-7 (IIQ-7). The results of HRQL are very different in the various studies. For example, Seleme et al. (2008) examined men receiving pelvic floor muscle training plus electro stimulation plus biofeedback and reported better quality of life using the Incontinence Quality of Life Score than those receiving pelvic floor muscle training alone. In contrast, Glazener et al. (2011) found no significant difference. 3
The key in treating timely urinary incontinence in patients without surgical complications, based on this study, is a combination of coordination training (oscillating rod) of the pelvic floor muscles and the continence system with conventional pelvic floor muscle training. It has been shown that this therapeutic approach is more effective than conventional continence training alone. There are different effects of treatment modalities on the pelvic floor muscles (see Supplemental Figure S1 D). 3 For optimal training of the continent system, it is important to train strength, endurance and coordination of this muscle. The question is why was continence training combined with oscillation rod therapy? The aim of pelvic floor muscle training is to improve strength, endurance and perception of the pelvic floor and to learn voluntary activation of the muscles. In addition to continence training, the oscillation rod is used to train inter- and intra-muscular coordination and involuntary activation of the continence system.
The basis for the anatomical mechanism of the oscillation rod is the global and local trunk musculature. These serve the segmental stabilization of the spine. 34 In addition to transversus abdominis muscle and multifidus muscle, the pelvic floor muscles are among the local trunk muscles (Supplemental Figure S1 C). A pure strength training is not effective because the transversus abdominis muscle optimally fulfills its stabilizing function with 25% of its maximum force. The aim should be a coordinative and sensorimotor training with focus on improving intra- and inter-muscular coordination and neuromuscular activation of local muscles. 35 These muscles form a functional unit and work together synergistically. Consequently, the continence system is activated by a coactivation of the local musculature of the trunk (multifidi muscle and transversus abdominis muscle) and the pelvic floor muscles.4,5 Various studies support the explanation of the anatomical mechanism. Anders et al. 8 demonstrated specific involuntary activations characteristic of the trunk muscles (rectus abdominis muscle, obliquus abdominis muscle, multifidi muscles and erector spinae muscle) using an oscillation rod in healthy subjects. These superficial abdominal (rectus abdominis muscle, obliquus abdominis muscle) and deep back muscles (multifidi muscles, erector spinae muscle) were activated by a forward and backward movement of training device. 8 Hodges 9 could even demonstrate a feedforward function. This suggests that the transversus abdominis muscle is also activated by voluntary arm movements. 9
The value of coordination and trunk muscles training is also supported by Pedriali et al. 6 and Gomes et al. 7 who used a Pilates exercise program for continence recovery and demonstrated that the Pilates approach is more effective than conventional physiotherapeutic training.
It has to be mentioned that rest and relaxing the pelvic floor is as important as the training itself, and it is therefore part of every successful physiotherapeutic/exercise therapeutic continence treatment scheme. The patient suffering from postprostatectomy urinary incontinence needs supervised training and a constant monitoring of the pelvic floor muscle exercises.
The strengths of this study are that the oscillation rod treatment can be applied by an experienced instructor in small treatment groups and urinary incontinence can be treated more effectively and faster using this new therapy. Comparable studies usually have longer study periods, to achieve the same effect.28,36,37
The main limitation of our study was the lack of long-term follow-up. The study was focused on early continence rates. It was conducted as part of a three-week inpatient follow-up rehabilitation after radical prostatectomy. Three weeks training is insufficient to draw strong conclusions of the effectiveness of the rod for urinary incontinence. This study has provided preliminary evidence for the effectiveness of the rod. The aim for further studies should be to investigate the long-term effect of the coordinative training using an oscillation rod in combination with continence training.
In conclusion, based on the results of this study, we recommend the combination of conventional continence training and sensorimotor training with an oscillation rod that has an effect on reduction of incontinence level, improved recovery time and the HRQL after radical prostatectomy.
Clinical messages
Within three weeks, a combination of continence training and sensorimotor training with an oscillation rod is more effective than conventional continence training alone and it has a beneficial effect on measured quality of life.
Benefits are greater in those patients with more severe incontinence.
Supplemental Material
Supplemental_Material – Supplemental material for Does trunk muscle training with an oscillating rod improve urinary incontinence after radical prostatectomy? A prospective randomized controlled trial
Supplemental material, Supplemental_Material for Does trunk muscle training with an oscillating rod improve urinary incontinence after radical prostatectomy? A prospective randomized controlled trial by Marc Heydenreich, Christian Puta, Holger HW Gabriel, Andre Dietze, Peter Wright and Dirk-Henrik Zermann in Clinical Rehabilitation
Footnotes
Author contributions
M.H. performed data collection, management and analysis, protocol development and manuscript writing and edition; C.P. contributed to data collection and analysis; H.H.W.G. helped in manuscript editing; A.D. helped in manuscript editing; P.W. helped in manuscript writing and ethics and D.-H.Z. contributed to protocol development and manuscript writing and edition.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data access and responsibility
The principal investigator, M.H., had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Ethical approval
The study design was approved by the University’s ethics committee (Chemnitz University of Technology: # V-146-TM-HS-Incontinence-29062016).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The funding source (Haider Bioswing GmbH, Dechantseeser Str. 4, 95704 Pullenreuth, Germany) had no role in the design of this study and had no role during its execution, analyses, interpretation of the data or decision to submit results.
Informed consent
Informed consent was obtained from all patients included in the study.
Trial registration data
Identifying number: DRKS00011028—German Clinical Trials Register.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.