
Abstract
Objective:
The aim of the present study was to compare client-centeredness as it was documented by the occupational therapists in the units randomized to the intervention clusters with documentation by occupational therapists in the control clusters.
Design:
Comparison of medical records.
Setting:
The study is conducted in a context of a randomized controlled trial in Sweden, with 16 post-stroke rehabilitation units cluster randomized to intervention or control group.
Subjects:
Occupational therapist documentation in medical records of 279 clients with stroke.
Main measures:
The medical records were reviewed for their level of client-centeredness using a protocol developed from the Stewart et al model. The occupational therapists in the intervention groups participated in a workshop training to enhance their client-centeredness.
Results:
Occupational therapists with training in client-centeredness documented significantly more on goal setting (OR = 4.1; 95% CI, 1.87-8.81), on client participation in goal setting (OR=11.34; 95% CI, 5.97-21.57), on how the goals could be reached (OR=2.8; 95% CI, 1.7-4.62), on client participation in how goals could be reached (OR=4.56; 95% CI, 2.73-7.64), on the follow-up on goals (OR=5.77; 95% CI, 2.78-11-98) and on client participation in follow-up on goals (OR=7.44, 95% CI, 4.33-12.8). This association remained after adjustment for healthcare setting, client socio-demographic variables, and stroke severity.
Conclusion:
Documentation of goal setting and client participation in goal setting can be influenced by training.
Introduction
Stroke is a sudden disease that often impacts multiple parts of both the individual’s and their significant others’ lives; rehabilitation following a stroke therefore involves different health professionals who focus on supporting the client to regain lost abilities and improve life satisfaction. 1 In this rehabilitation, the clients and their significant others should be involved as partners and the whole person, including the lived experience, preferences, values and needs of the client must be considered.2–4 This perspective – often referred to in the literature as patient-centred, person-centred or client-centred5–7 – is thus an important part of the rehabilitation. This paper uses the term client-centred.
It has been suggested that client-centred rehabilitation could improve stroke rehabilitation4,8 and multiple studies have been conducted on client-centred interventions in occupational therapy.9–13 However, several of these studies have not shown any statistically significant differences between the intervention and the control group 9,11–13 and likewise a systematic review of randomized controlled trials of client-centred interventions found no effect on clinical outcomes. 14 As an explanation of why several studies did not demonstrate significant differences in outcome between the intervention and the control group, it has been suggested that the client-centred interventions were too similar to usual interventions – in other words, that a client-centred approach already was applied in the everyday rehabilitation work.10,15
This study was performed in the context of a cluster randomized controlled trial11,12,16 in which no significant difference in outcomes between a client-centred activities of daily living (ADL) intervention and usual ADL interventions was found. The aim of the present study was to compare client-centeredness as it was documented by the occupational therapists in the units randomized to the intervention clusters with documentation by occupational therapists in the control clusters.
Methods
In the cluster randomized controlled trial11,12,16 16 units of stroke rehabilitation in three Swedish county councils participated. The names of the units were written on opaque paper, which were folded and stratified in geriatric inpatient rehabilitation, medical inpatient rehabilitation and home rehabilitation. For each stratum, the papers were randomly drawn to either intervention group (client-centred ADL rehabilitation named “CADL”) or control group (usual ADL rehabilitation).
All occupational therapists from the units randomized to deliver the client-centred ADL intervention were invited to participate in one of five workshops (each consisting of four days distributed over a one-month period and a one-day follow up one month later) led by the third and fourth author. The workshops included lectures by experienced researchers on concepts and theories behind client-centeredness, reading and discussing articles as well as working with cases to inspire the occupational therapists to integrate the research-based knowledge into practice (for a detailed description of the content of the workshop, see Box 1). The therapist’s understanding of the client’s lived experience was used as a point of departure for the client-centred intervention, which entailed that the rehabilitation was to be adjusted to the individual client’s ability, motivation, experiences and needs, and conducted by means of close collaboration between the client and therapist. The overarching goal of the workshops was to give the occupational therapists’ knowledge and tools to enable agency in daily activities and participation in everyday life among persons with stroke. 11 A client’s sense of agency is characterized by a feeling that one can cause one’s own actions and their outcomes. 17 The researchers did a monthly follow-up of all the participating occupational therapists, in both groups, by phone and email (“Stroke news”).
Content of the workshop to enhance client-centeredness in rehabilitation.
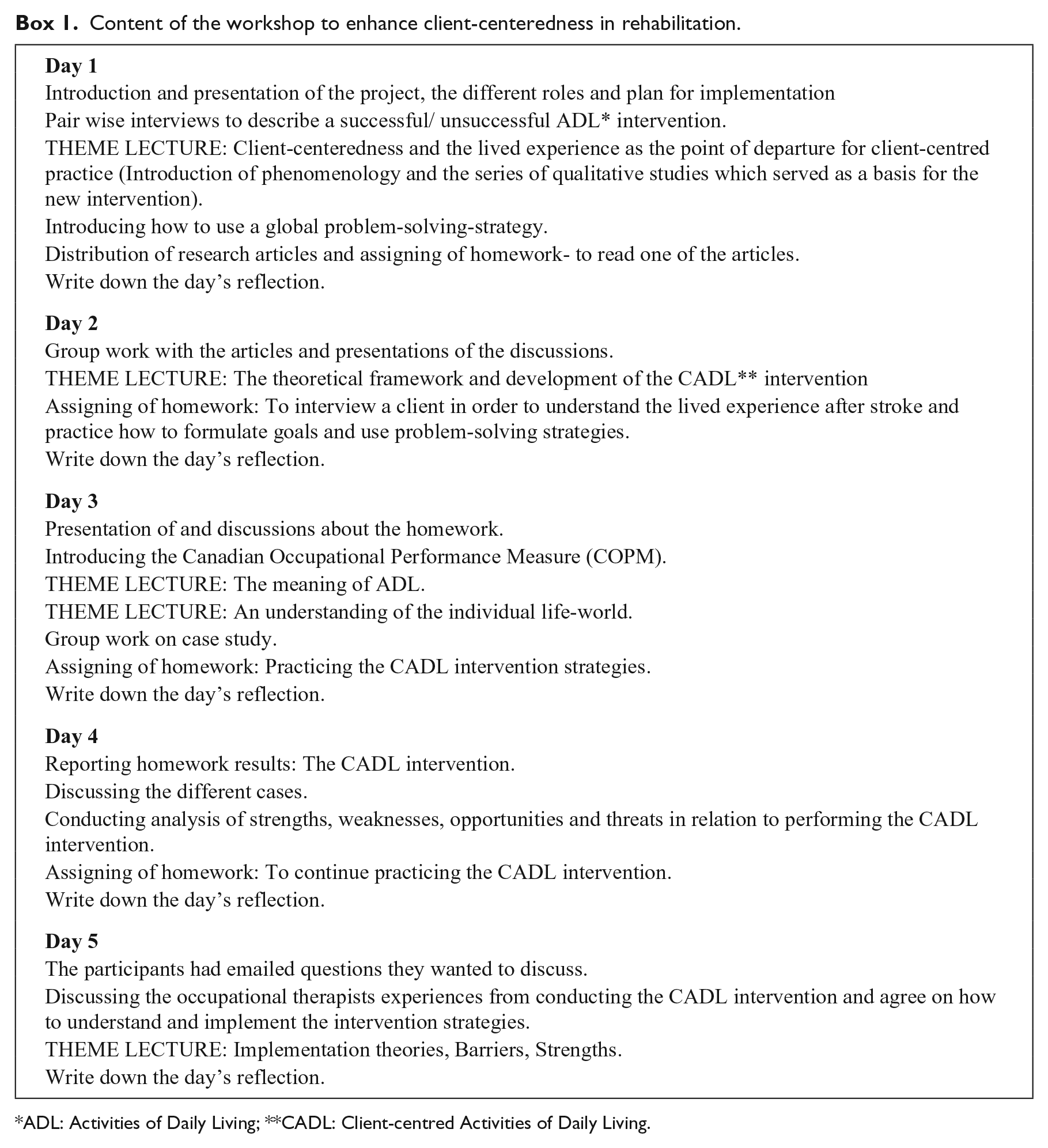
ADL: Activities of Daily Living; **CADL: Client-centred Activities of Daily Living.
The occupational therapists in the both groups were informed about the overall aim of the cluster randomized controlled trial of the client-centred ADL intervention. All occupational therapists were told that the participating clients’ medical records were to be analysed in the context of the study; no instructions were given to the occupational therapists in either group on how they should document in the medical records. Printed copies of the occupational therapist part of the electronic medical records, with the client’s name replaced with the client’s study code, were obtained from the 16 rehabilitation units after the end of each client’s rehabilitation period.
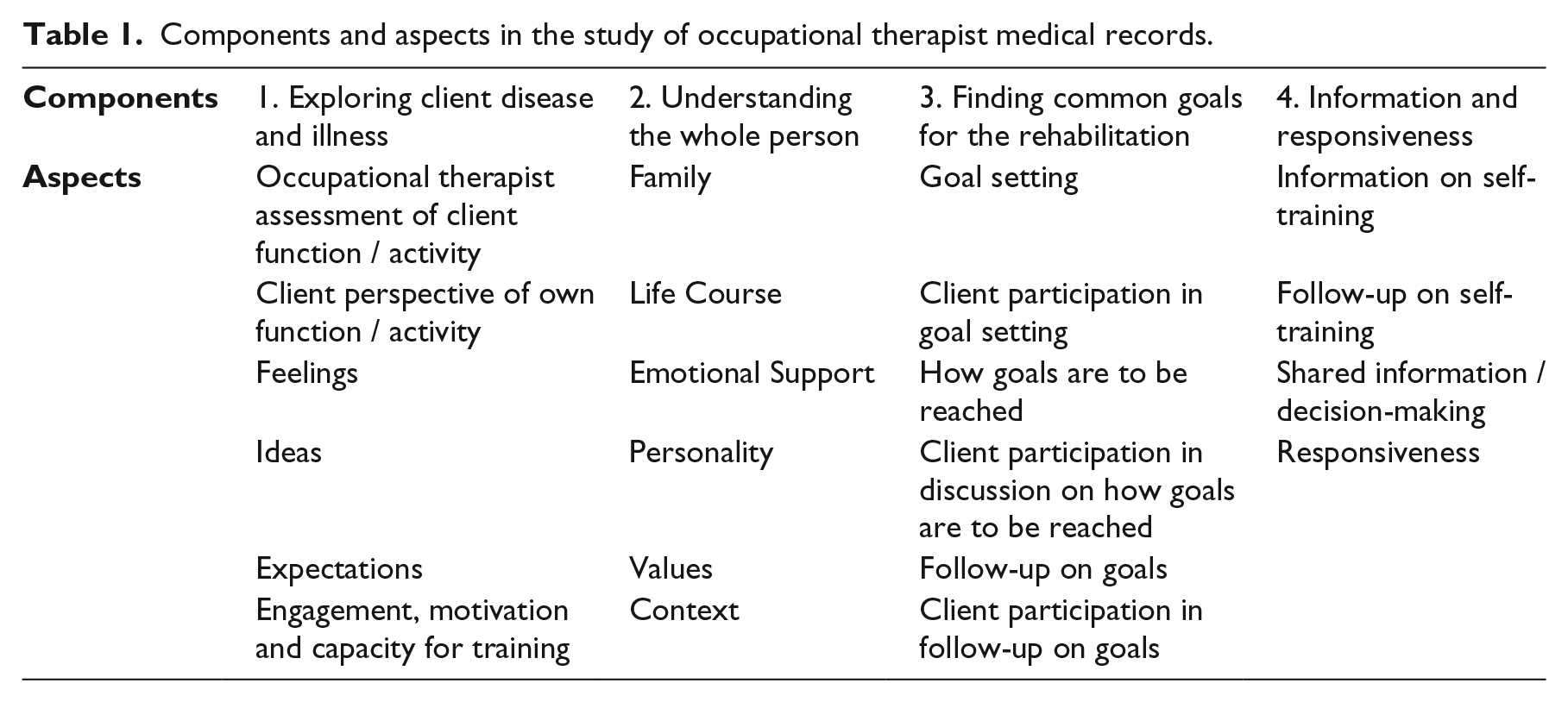
To review the client-centeredness of the medical records, a study protocol was developed based on the Stewart et al model. 18 The Stewart model, originally designed and validated in observed client-physician encounters, is one of the most cited definitions 19 and has previously been used for medical record assessments. 20 The original model consists of three components: 1) exploring both patient disease and illness; 2) understanding the whole person; and 3) finding common ground. All components have defined sub-components, here referred to as aspects, which together form the component. In this study, all components were modified to fit the study context: the occupational therapist medical records of clients with stroke. The two first components were kept the same, while some of their aspects were changed. The last component, Finding common ground was renamed Finding common goals for the rehabilitation, and a fourth component, Information and responsiveness was added in order to obtain further information about the client-occupational therapist interaction. Each aspect was defined and illustrated with examples (see supplementary material appendix). The multi-professional research group worked in an iterative process to reach a common understanding of the study protocol. Initially the first (MF), second (ASB) and the last (LvK) authors read the same medical record separately and identified the presence or absence of the different aspects. Agreements and disagreements in categorization were discussed until consensus was reached. The protocol was then discussed and revised by all authors. The final protocol consisted of four components with a total of 22 aspects (Table 1). During the review process, the reviewers (MF, ASB, LvK) were blinded to intervention/control group.
Components and aspects in the study of occupational therapist medical records.
The medical records were analysed using manifest quantitative content analysis with a deductive approach.21,22 The Stewart model 18 was considered providing sufficient theoretical grounds to allow for a deductive approach. In the review, the medical records were searched for statements that fulfilled the definition criteria of the aspects in the protocol. A binary categorization – yes or no – was applied to indicate presence of the aspect or not. For example, the statement “has previously worked as an assistant nurse, now likes to read and work in the garden”, and the statement “patient is worried that she will get sick again” fulfilled the definition criterions for the Life course aspect and Feelings aspect respectively. An aspect was considered as covered when at least one statement in the medical records agreed with the definition in the definition template (see supplementary material appendix).
Independent variables were drawn from the data collection, described in detail elsewhere,11,12 of the randomized controlled trial: client socio-demographic data (age, education, gender, marital status), client disease related factors (the Frenchay Activity Index, 23 stroke severity); and healthcare setting, (inpatient versus outpatient rehabilitation, and county council). Client-provider interaction has been linked to client characteristics and clinical settings 24,25 and it was hypothesized that these factors could influence the documentation.
All documentation in the medical records that was written by an occupational therapist was analysed. Pearson Chi 2 was used to compare aspects of client-centeredness in the occupational therapist medical records between the intervention and control group. For analysing the association between the aspects of the client-centeredness model and independent variables, we used univariate and stepwise logistic regression to calculate the odds ratio with a 95% confidence interval. In the univariate analysis the following independent variables were included: clients’ age, gender, education, and marital status; Frenchay Activity Index; 23 stroke severity; in/outpatient setting; and county council. In the stepwise logistic regression, independent variables with a significance level set of P<0.05 in the univariate models were included. The significance level was set to P<0.05. Data was analysed using the statistical software SAS.
The inter-rater reliability was investigated during the study. First, pilot assessments of three medical records were reviewed individually and compared collectively by MF, ASB and LvK. Second, after completing approximately half of the medical record reviews, another two records were reviewed individually and compared collectively by the three reviewers. Third, after all reviews had been carried out, the third author (UJ) reviewed randomly selected medical records of the three reviewers.
The study was approved by the Regional Ethic Review Board, Stockholm, Sweden.
Results
The medical records were obtained from a sample of 280 clients included in the cluster randomized controlled trial. The clinical data in this study consisted of the occupational therapists’ medical records of 279 clients living with stroke; one medical record was excluded since no occupational therapy encounter was documented. In total, 133 individual occupational therapists were involved in the rehabilitation: 77 occupational therapists documented in the medical records of the intervention group, whereof 44 therapists had participated in the training workshops. On average, each client had 2.1 occupational therapists involved in their rehabilitation; ranging from 1 to 7 occupational therapists per client. In total, nine clients from the intervention group and one client from the control group had six or more occupational therapists involved in the rehabilitation.
The inter-rater reliability of the present study was high overall; the inter-rater reviews differed in 11.8% of the aspects. The main differences were in two aspects of the component Information and responsiveness (responsiveness and shared decision-making) which had relatively big differences among the reviewers. The remaining 20 aspects had high inter-rater reliability.
The presence of components and their aspects in the groups are presented in Table 2. In summary, occupational therapists in the intervention group overall documented significantly more on all aspects of Finding common goals for rehabilitation. Occupational therapists in the intervention group also documented more, even though not statistically significant, on all aspects of Exploring client disease and illness. For the components Understanding the whole person, and Information and responsiveness, results were mixed. Occupational therapists in control group documented significantly more on the aspects family and emotional support. As depicted in Table 3 the association between Finding common goals for rehabilitation and the intervention having received training to enhance client-centeredness remained in all the logistic regression models.
Number and percentages of aspects covered in intervention and control group medical records.
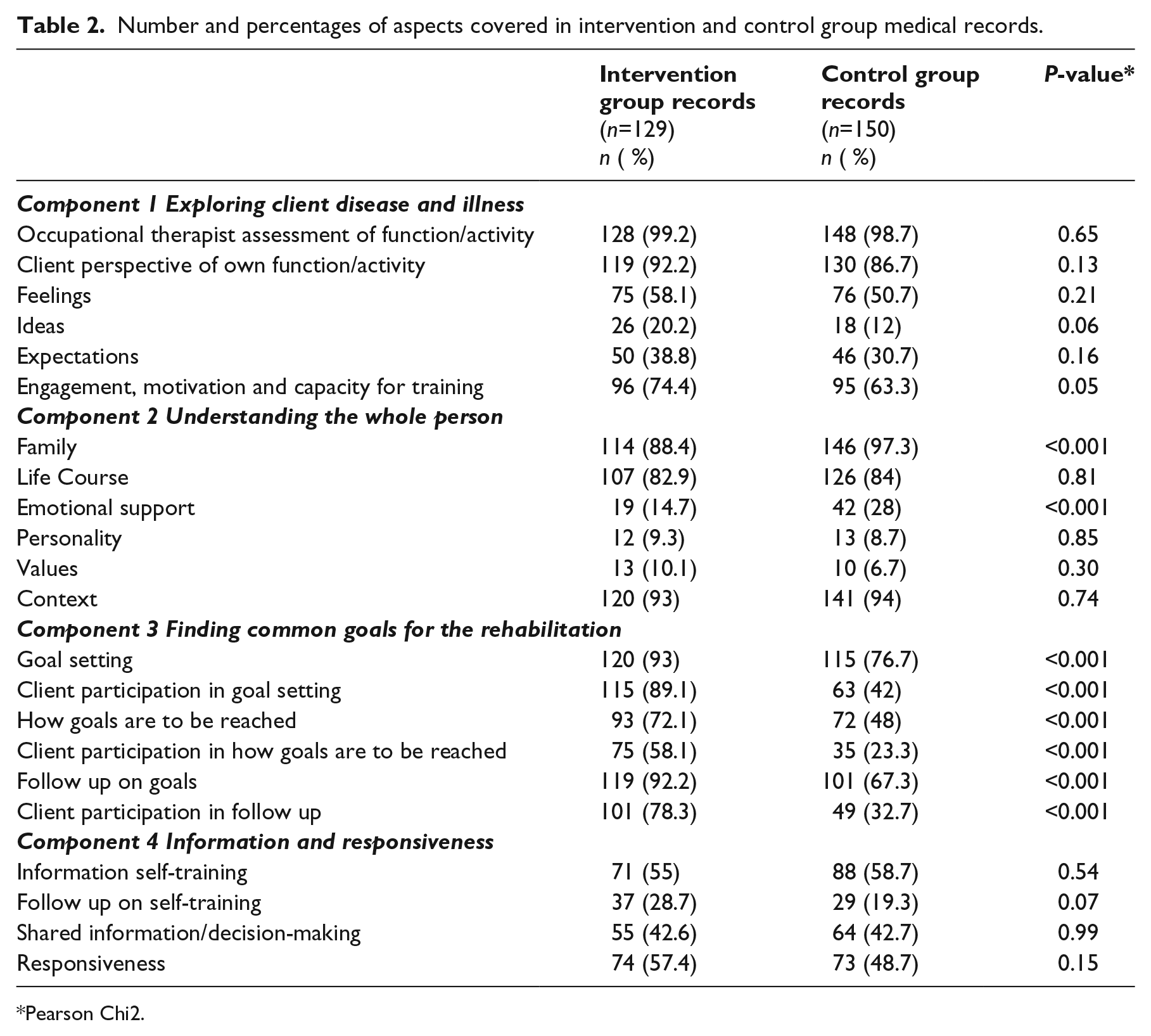
Pearson Chi2.
Crude and adjusted OR for association between aspects of Finding common goals and intervention group; and crude OR for independent variables.
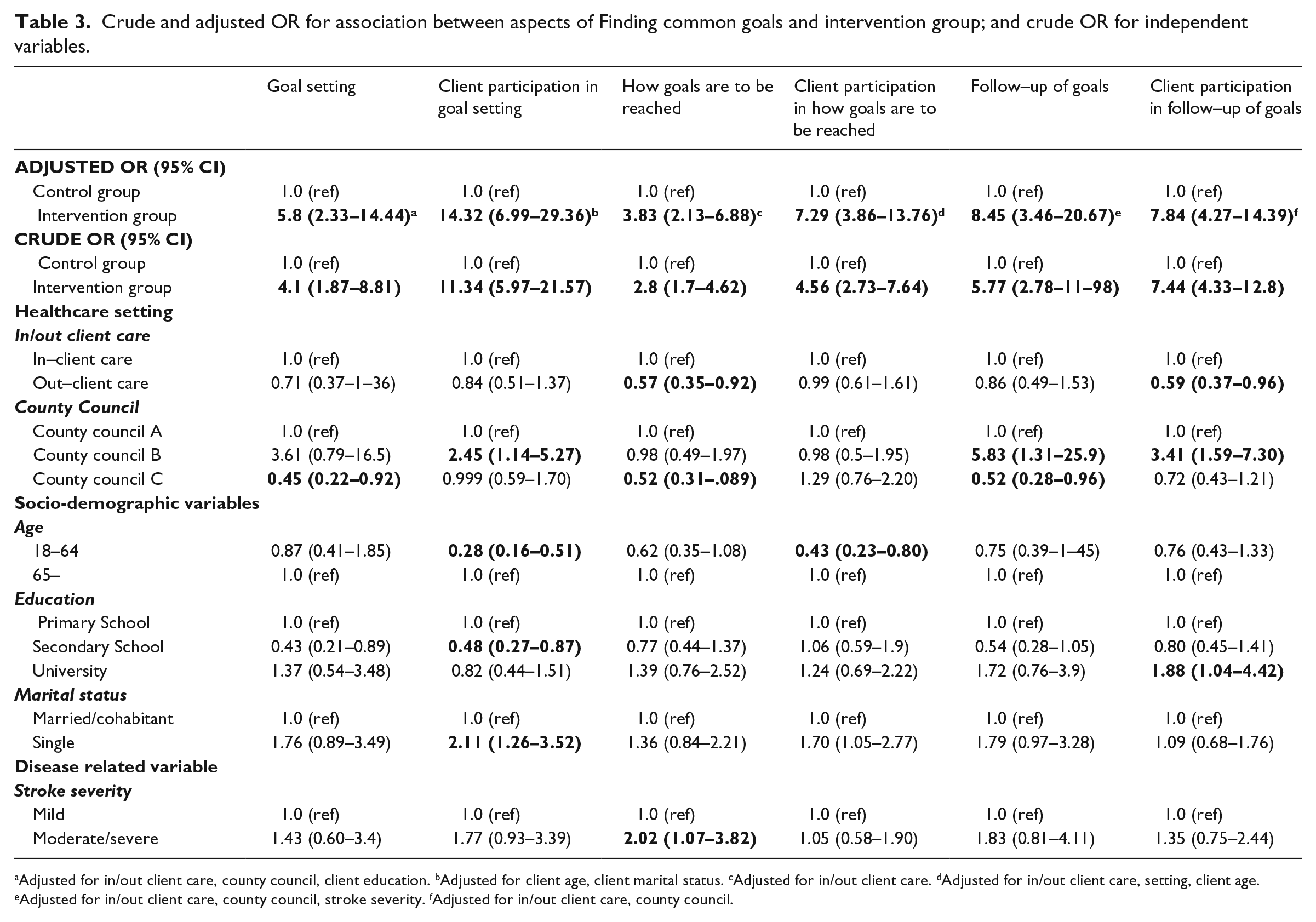
Adjusted for in/out client care, county council, client education. bAdjusted for client age, client marital status. cAdjusted for in/out client care. dAdjusted for in/out client care, setting, client age. eAdjusted for in/out client care, county council, stroke severity. fAdjusted for in/out client care, county council.
Discussion
Occupational therapists in the intervention group documented significantly more on all aspects related to goal setting and on client engagement/motivation for rehabilitation than occupational therapists in the control group. The association between training in client-centeredness and documentation of goal setting and client participation in goal setting remained after adjusting for healthcare setting and client-related factors. However, the occupational therapists in the control group documented significantly more on clients’ families and emotional support.
Goal setting is perceived as one of the cornerstones of improving client outcomes in stroke rehabilitation. 26 , 27 Goal setting is often referred to as the process of negotiation between clients and healthcare professionals when deciding what the rehabilitation should try to achieve.26,28 In this study, finding common goals has a broader application, covering the continuous process from setting the initial goals to deciding how goals are to be achieved and following them up. The client-centeredness training also increased the documentation of client participation in the process of finding common goals, which in other medical record reviews, albeit with small samples, have been found to be poor regarding people with stroke.29,30 Ensuring the process of goal setting was a part of the training aiming to enhance the occupational therapists’ client-centeredness. The findings indicate that the occupational therapists integrated a client-centred approach during the whole process from initial goal setting to follow-up on goals.
Client-centeredness in occupational therapy has been linked to the concepts of sharing power, listening/communicating, partnership, choice and hope. 7 These concepts are related to the aspects that make up the components Finding common goals for rehabilitation and Information and responsiveness in this paper. Interestingly, documentation of the aspects of Information and responsiveness were not more present in the intervention group, and occupational therapists in control group documented significantly more on the clients’ families and emotional support. This result could be caused by the overall focus of the intervention, i.e. that the occupational therapists should enable agency in daily activities and participation in everyday life of the clients with stroke, 11 and thus did not include a specific focus on either family or emotional support. It would therefore seem as if the documentation of the holistic approach of client-centeredness, focusing on the client as a whole person and the relationship between clients and providers,5,31 is not being affected by training. Goal setting and client participation in this process might be more easily documented than subtler issues such as relationships and responsiveness. Indeed, findings from a qualitative study indicate that occupational therapists limit their client-centred documentation to better fit in with the medical context of the rehabilitation. 32 The results could also indicate a negative effect of the training, being that the occupational therapists focused explicitly on finding common goals and hence omitted other important perspectives such as that of family and emotional support.
Documentation of finding common goals and client participation in finding common goals was also partly associated with the healthcare setting and with client related factors. Among the healthcare settings, county councils showed a specific trend, with one county council documenting more than the other two. All county councils had electronic medical record systems, but with different headings for the occupational therapists’ documentation. Previous research 20 has indicated that the choice of headings in medical records could guide healthcare professionals’ documentation. This is in line with studies showing that when healthcare professionals use checklists, they tend to follow the items in the list more than the client’s history.33,34 For the client related factors, socio-demographic variables had the strongest association with client participation in goal setting; older clients and single clients had significantly more documentation than younger clients and married/co-habitant clients. Whereas clients with medium education had significant less documented participation than clients with low or high levels of education. This differs from studies of client-provider interaction in which higher levels of client participation are associated with younger clients and a high level of education.35–37 It has been shown that stroke clients consider their ill health as one reason for not participating in goal setting, 26 which contradicts our findings where clients with severe and moderate stroke had more documentation of participation compared to those with mild stroke. These differences might be a result of the purpose of documentation: to communicate information about the client. 38
A limitation of this study is that no baseline data of the occupational therapists’ documentation habits were collected. Hence, we do not know if the occupational therapists in the intervention and control group differed in their documentation before the occupational therapists in the intervention group received the training aiming to enhance their client-centeredness. Additionally, several other factors – such as aphasia, level of awareness – could besides the presented independent variables have influenced the documentation. The inclusion of patients and occupational therapists from a wide variation of settings (different county councils, hospitals and primary care rehabilitations) were considered to enhance the likelihood of random variance in both groups. Further, of the 77 occupational therapists in the intervention group 44 had participated in the training. This indicates that clients in the intervention group also received rehabilitation from occupational therapists without the training. This might be related to the length of the study period; the study ranged over 23 months and hence involved multiple substitute occupational therapists, without the training, during for example vacations. The statistical significant difference between intervention and control groups indicates that there might be a spill-over effect in the intervention cluster units from occupational therapists with training to their colleagues that did not participate in the training workshops. This was also found in the pilot study of the randomized controlled trial. 39 It is a strength of the study that the researchers preceding blinded to intervention-control group during the reviews. Furthermore we consider it a strength of the study that the first author, who performed the major part of the analysis, is not an occupational therapist and thus not prone to interpret the text based on tacit professional knowledge.
One concern in medical record reviews is whether the documentation can be considered to reflect the interaction between clients and occupational therapists during the rehabilitation process. Studies comparing medical records with client reported data have shown mixed results on concordance. 40 , 41 However, there is no reason to believe that the concordance would differ between the intervention and the control group; both groups were aware that their medical records were going to be analysed, but neither group received instructions on how to document.
Client-centeredness is considered as an essential quality indicator in healthcare 2,42,43 but it has been questioned if the client-centeredness perspective in occupational therapy is more a “rhetoric claim” than a reality. 44 This study shows that training in client-centeredness impacts the documentation of finding common goals and client participation in finding common goals. This indicates that there is room for improvements regarding documentation of goal setting, how to achieve and follow-up on goals, as well as on client participation for occupational therapists in the stroke rehabilitation. The findings of the present study call for future studies with a pre-post design to compare differences in documentation, behaviour and quality of the documentation. Furthermore, studies with an inductive approach to documentation and client-centeredness are warranted.
Clinical messages
Training in client-centeredness enhances the documentation on finding common goals, i.e. on goal setting, how to reach goals and follow-up on goals.
Training in client-centeredness enhances the documentation of clients’ participation in finding common goals for rehabilitation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.