
Abstract
Objective
Post-stroke aphasia (language impairment) has a devastating impact on quality of life and people with aphasia experience long-term unmet needs. A shared understanding of the experiences underpinning these unmet needs is required to identify priorities for improvement. Establishing priorities for meaningful service improvement requires involvement of service users and providers. Therefore, this research aimed to: (1) collaboratively identify priorities for aphasia service improvement according to people with aphasia, significant others, speech pathologists, and (2) co-design a plan for service development and improvement.
Design
Prioritisation phase of an experience-based co-design project. Online surveys were used to prioritise ideas (n = 773). Three multi-stakeholder consensus groups were held to shortlist top priorities. Design principles were applied during three consecutive co-design workshops, to develop a concept design targeting the top priority.
Participants, setting
People with aphasia (n = 41), significant others (n = 35) and speech pathologists (n = 75) across 26 health and hospital sites in remote, regional, and metropolitan Queensland, Australia.
Results
Consensus was established on seven priorities: (1) chart alert system for aphasia, (2) training for healthcare providers in ways to support communication, (3) care that is tailored to the individual, (4) consistent care, (5) equitable access to care, (6) intensive communication therapy options, and (7) mental health service options. A concept design (implementation strategy) was created for the top priority.
Conclusions
Multi-stakeholder consensus was gained on seven priorities. Development, implementation, and evaluation of the co-designed concept plan for the top priority may decrease miscommunication in hospital settings and enhance experiences of people with aphasia communicating with healthcare providers.
Introduction
Aphasia (language/communication impairment) has debilitating effects on quality of life,1,2 and is a devastating consequence of stroke for 30–40% of survivors. 3 Outcomes for people with aphasia remain unacceptably poor with many experiencing long-term unmet needs.4–6 Compounding this, people with aphasia are often subject to inequitable service access due to geographic location (e.g. reduced service availability and access in remote communities) 7 or inadequate communication support,8,9 are excluded from healthcare decision-making, 9 and are at increased risk of preventable adverse events in hospital. 10 Understanding experiences of care and where gaps in service delivery exist is crucial for designing services able to meet needs. 11 Service users (patients, family, friends, caregivers) have unique lived experiences of receiving care, enabling them to highlight strengths and weaknesses. Healthcare providers bring expert insights into service model or system constraints and barriers, and both perspectives are needed to identify new ways to meet needs, 11 enhance care experiences, and the quality of care provided.12,13
Experience-based co-design is a collaborative participatory approach, where touchpoints (emotionally charged themes related to the journey of care experiences) are transformed into actionable change by applying design principles. 12 Design thinking refers to the creative approaches taken to both define a problem and develop a solution that is fit for purpose within the context of a specified social reality. 14 The application of design principles, synthesises experience data into possible interventions for specific service contexts. 15 One way to effectively translate a synthesis of healthcare experiences into practical principles for designing change within a healthcare setting, is through using the heuristic ‘if we want to achieve (Y) in (S) context then (X) might help’.12,15 Experience-based co-design typically encapsulates a six-stage quality improvement process, 12 however, in the current study, these steps have been modified to support the inclusion of people with aphasia in the design of new services to meet their needs. 16
Multiple and varied unmet needs have been identified by people with aphasia, their significant others and speech pathologists across geographic remoteness areas and service contexts.5,6 However, shared understanding and prioritisation is required to focus future improvement initiatives. Research reported in this study builds on our knowledge of people with aphasia, significant others, and speech pathologists experiences and unmet needs (gained in previous research stages).5,6 This study sought to collaboratively identify the key priorities for improvement and to co-design a plan for change. Specifically, this research aimed to: (1) collaboratively identify priorities for aphasia service improvement according to people with aphasia, significant others, and speech pathologists, and (2) co-design a concept design for service improvement.
Methods
Patient and Public Involvement
This research was co-produced with a consumer advisory committee comprising people with aphasia (n = 3; authors KM, KD, and BA), significant others (n = 2; author JD), and a cultural capability officer (author GB). 1 This committee: (1) confirmed research questions, advised on recruitment processes, and co-presented research updates/recruitment information at community aphasia groups; (2) co-designed study materials and processes (e.g. online surveys and personas (personas represented a synthesis of experiences, ideas, and characteristics, translated into an archetypal person with aphasia, to represent a single priority focus area)); and (3) reviewed findings and contributed to publications (e.g. plain English summary, video abstracts).
Study Design
A modified experience-based co-design 12 approach was used, as part of a larger program of research, to co-produce aphasia services. 16 An overview of data collection procedures and alignment with experience-based co-design stages, is provided in Figure 1. Detailed information about study design and sampling criteria are described in the published protocol. 16 Earlier stages have been reported elsewhere (experience gathering data from research stages 2–3).5,6 Ethical approvals were granted by the Royal Brisbane and Women's Hospital (approval number: HREC/2020/QRBW/61368) and The University of Queensland (approval number: 2020000965) Human Research Ethics Committees. The COREQ guidelines for qualitative research studies 17 and the GRIPP-2 18 guidelines for reporting patient and public involvement have guided reporting. Consent was obtained using standard procedures.
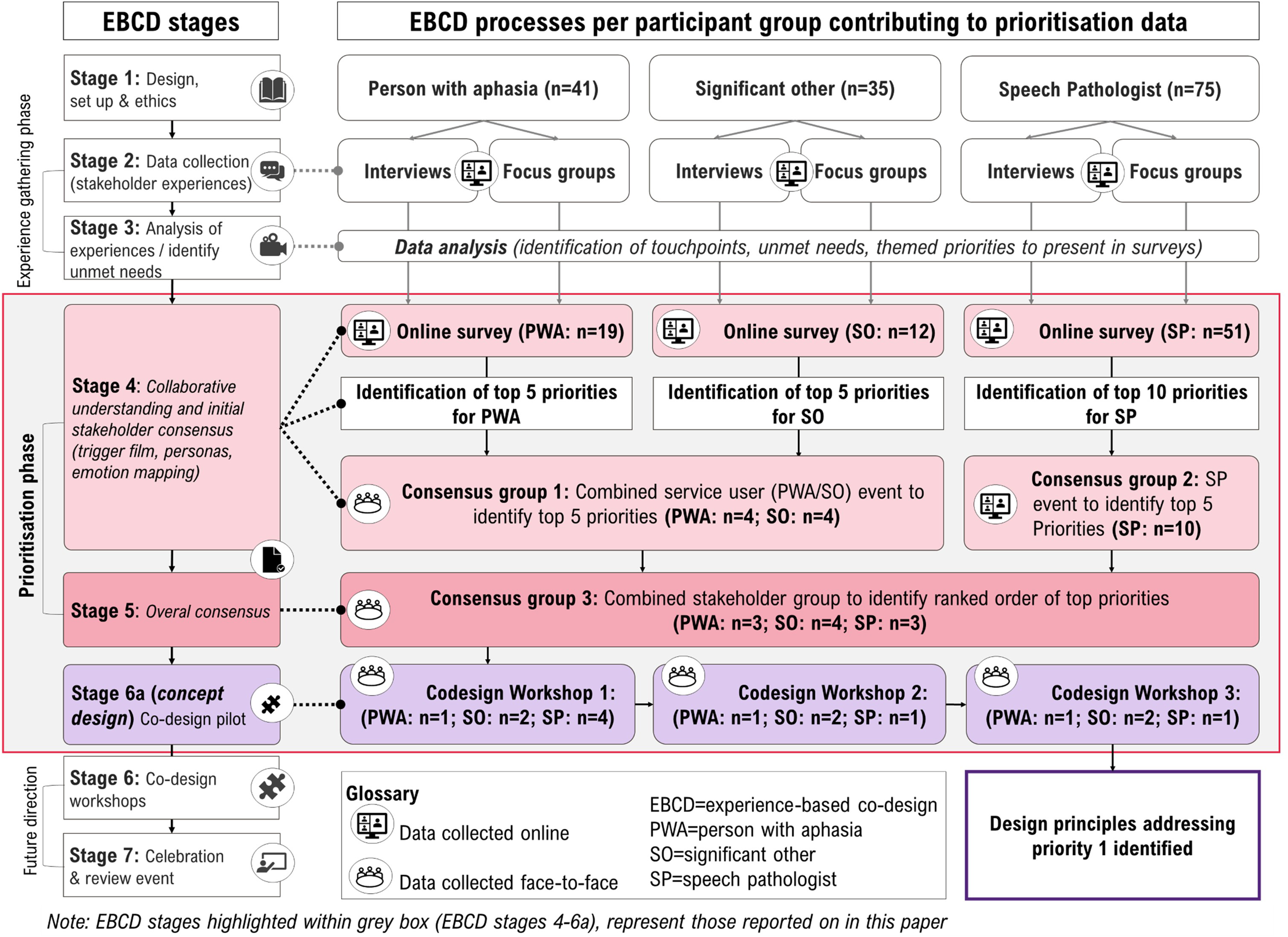
Experience-based co-design stages and corresponding data collection activities with details of processes used and numbers of participants involved.
This article reports the prioritisation phase of a larger experience-based co-design 12 project, and focuses on the participatory design (e.g. stakeholders working as equal partners to identify priorities) and design thinking elements (e.g. application of design principles to determine suitable actions). 12 Experience-based co-design is underpinned by qualitative enquiry and participatory methods to understand experiences, determine priorities, and co-design solutions. 12 An overview of the prioritisation refinement process is provided in Figure 2. Initial priority lists were derived from the earlier experience gathering phase (research stages 2–3).5,6
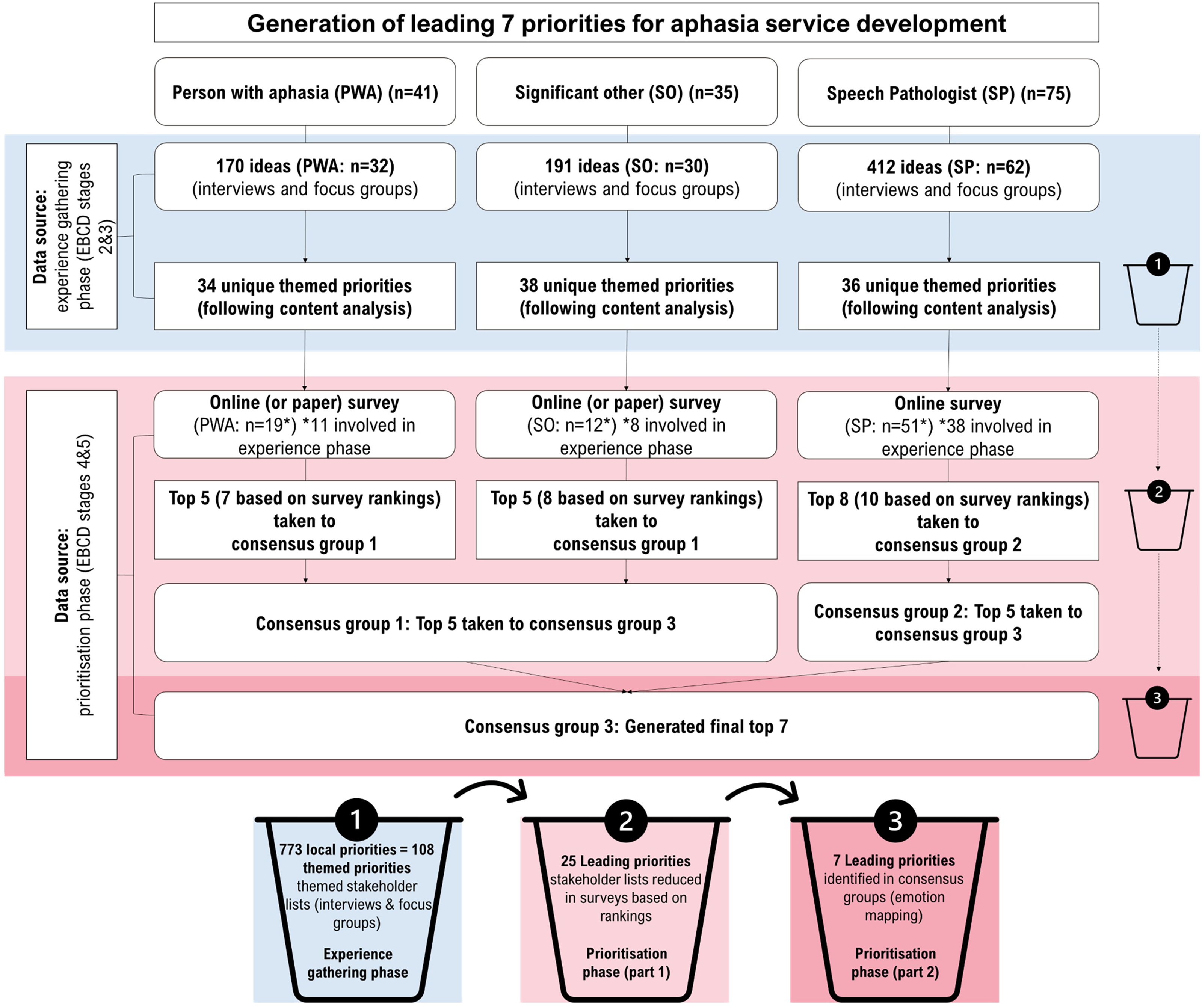
Overview of prioritisation phase refinement processes and data source origins.
Participants
Participants were people with aphasia (≥ 6 weeks post-stroke), significant others (family, close friend, carer, main contact, i.e. someone who knew the person with aphasia well), and speech pathologists (experience working with people with aphasia in Queensland, Australia). Eligible participants were adults (age ≥ 18 years). Eligible people with aphasia (assessed at point of participation as per Aphasia Severity Rating Scale) 19 who were able to participate in research processes. Exclusion criteria: (1) not proficient in English (group involvement only); (2) aphasia due to non-stroke aetiology; (3) presence of neurodegenerative or neuropsychological disorder.
Participants contributing to previous research stages were invited to be involved. Additional recruitment was conducted through 21 participating hospital and healthcare sites, online advertisements, and aphasia community groups. Purposive sampling was used (for consensus groups and co-design workshops) to ensure diversity in participant characteristics according to: (1) geographic remoteness (remote, regional or metropolitan, determined by postcode); (2) aphasia severity (people with aphasia/significant others), caseload (speech pathologists); (3) time post-onset (people with aphasia/significant others), health service setting (speech pathologists); and (4) age (people with aphasia/significant others), years of experience (speech pathologists).
Modifications to support inclusion of people with aphasia
A speech pathologist supported inclusion of people with aphasia and resources were developed using communication accessible formatting. 20 Supportive communication strategies were used throughout (e.g. facilitating processing time, verifying content). 21 Additionally, prioritisation surveys and resources for consensus groups (personas, touchpoint film) 12 were co-designed and piloted with the consumer advisory committee to ensure processes and methods were acceptable. In this research, touchpoint films were a digital representation of key touchpoints identified, used to elicit emotional connections with experiences of care (https://youtu.be/RUpUdITuF1s). Adjustments made to the touchpoint film to promote engagement included: (1) limiting the video length (14 min); (2) modification of voice recordings to maintain a consistent pace across speakers; (3) removal of repetitions or circumlocutions to increase clarity; and (4) visual content formatted using guidelines for supporting accessibility. 20
Data collection (prioritisation phase)
Three methods of data collection were used: (1) stakeholder surveys, (2) consensus groups, and (3) co-design workshops. Participants provided feedback on experiences of involvement (to be reported elsewhere). Data collection occurred during the COVID-19 pandemic (2021–2022). All groups/co-design workshops were audio and video recorded.
Procedures
Results
A summary of participant characteristics is provided in Table 1. Participants involved in experience gathering phase (stage 2) contributed to data presented (see Figure 2). All geographic remoteness areas were represented by speech pathologists (consensus group 2). Only metropolitan areas were represented across all other consensus groups and co-design workshops. People with aphasia (severe n = 1, moderate n = 1, mild n = 2) and significant others (severe n = 3, mild n = 1) represented a diverse sample of aphasia severities in consensus groups, and co-design workshops (people with aphasia: moderate n = 1; significant others: severe n = 2).
Overview of participant characteristics.
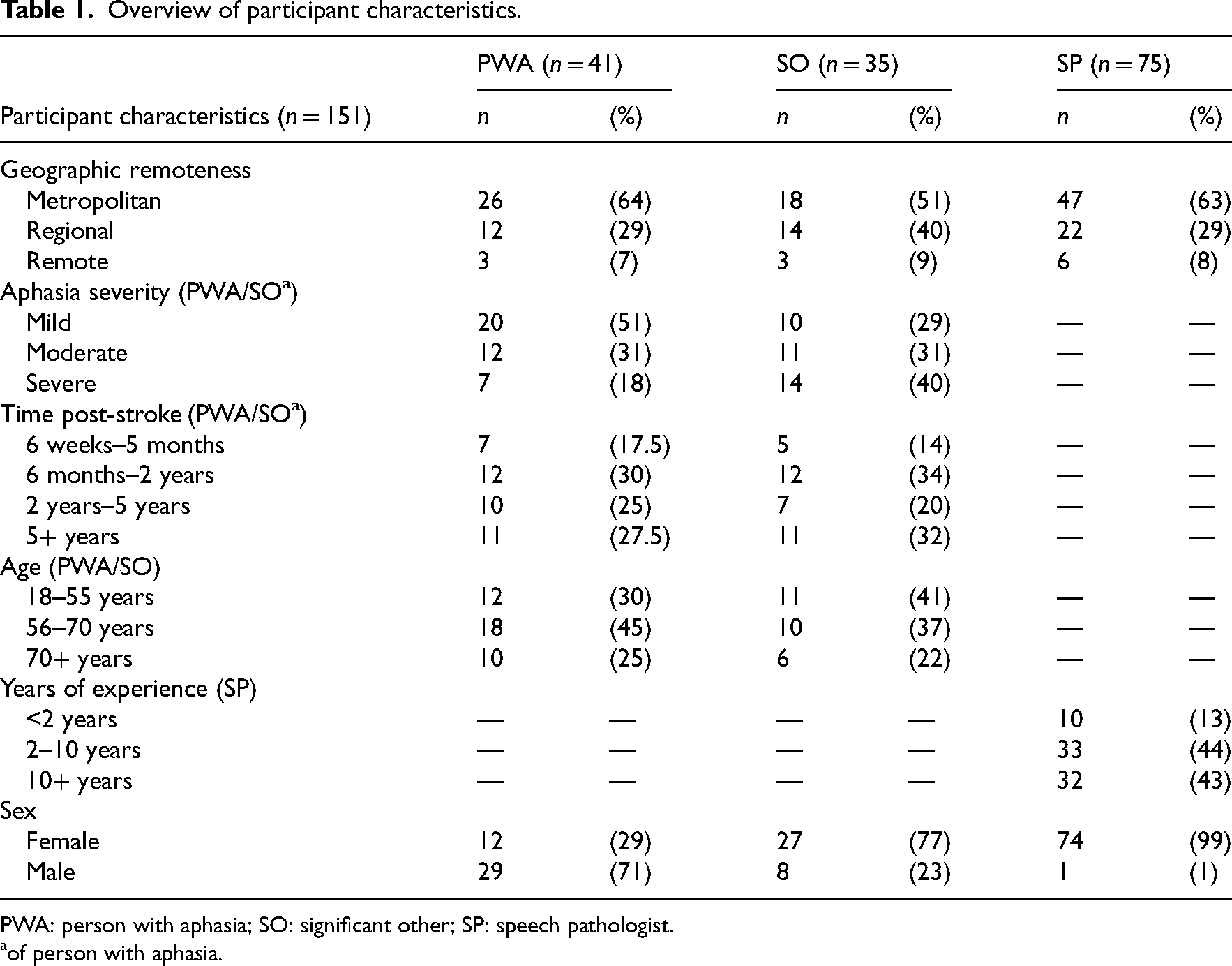
PWA: person with aphasia; SO: significant other; SP: speech pathologist.
of person with aphasia.
Final priorities in ranked order with details of those combined during consensus meetings.
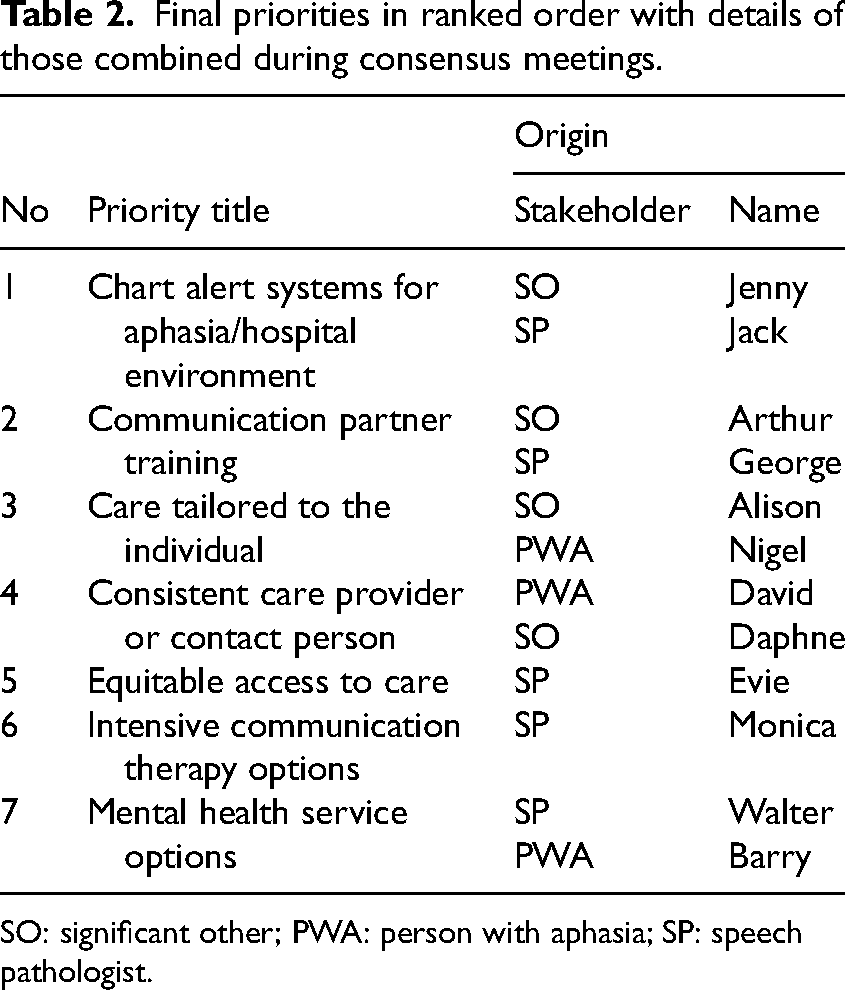
SO: significant other; PWA: person with aphasia; SP: speech pathologist.
Poor awareness of the impact of aphasia and knowledge of how to support their communication among healthcare providers. Hospital signage and wayfinding not suited to a person with aphasia. Reports/medical instructions provided to patients not being communicatively accessible (e.g. medication dose/timing, risk factors). Hospital menus and systems for ordering meals not suitably formatted or accessible. Lack of supported communication opportunities for people with aphasia to express needs.
Participants felt hospitals should have a chart alert system for aphasia to ensure staff were aware that a patient has aphasia (and access to recommended communication strategies) before meeting with them. All involved agreed the top priority was suitable for co-design.
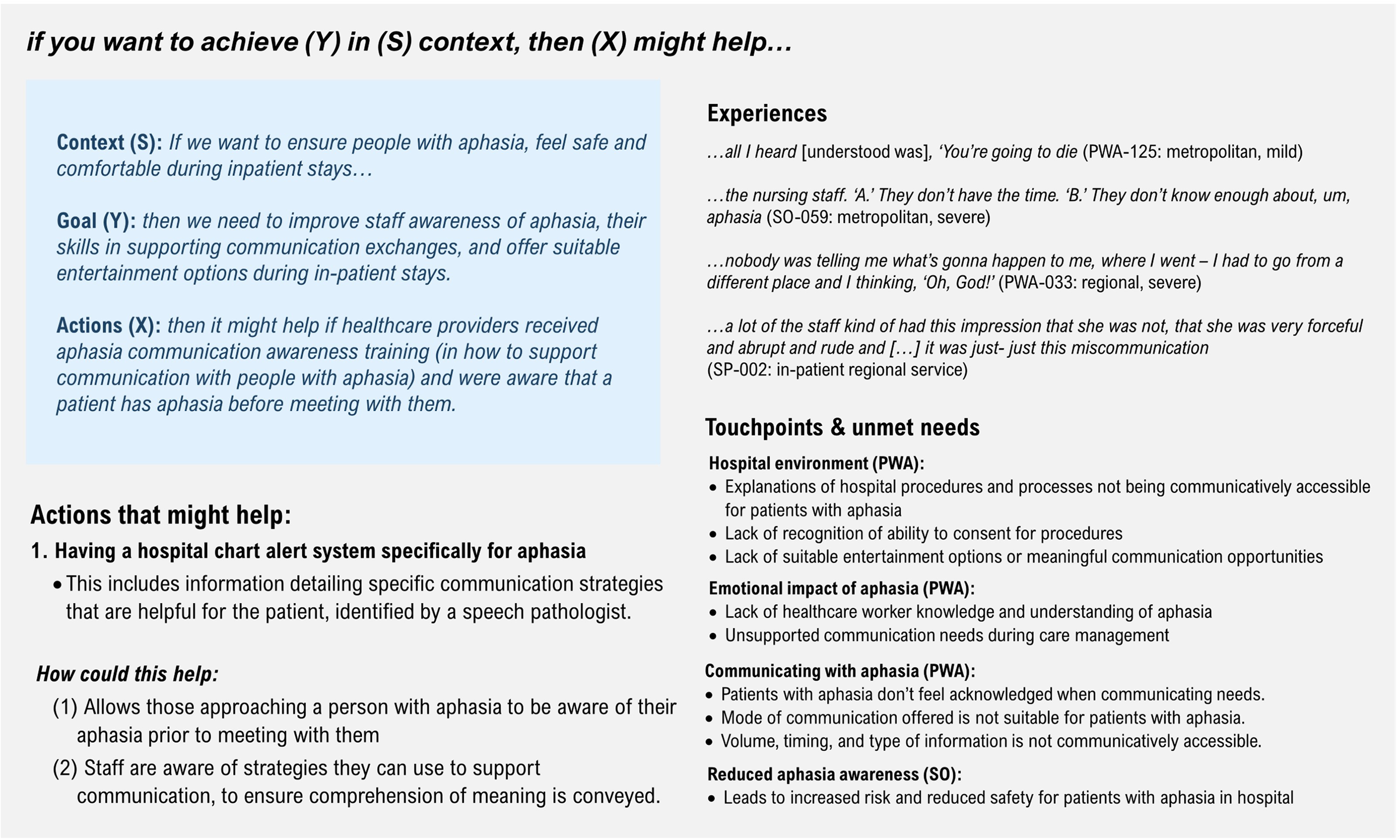
Concept design showing design principle with supporting experience quotes and touchpoints.
Design principles, in this context, seek to first identify key patterns across healthcare experiences, and transform these (agreed upon) patterns into actionable interventions that might improve both outcomes and experiences.
12
Future co-design should ensure interventions designed to meet needs are suitably scaled for service contexts, prior to implementation and evaluation. The following steps (modified, based on Bate and Robert
12
) are suggested as a way to move from the limitations inherent in current service models towards a future model of aphasia service care, designed to meet needs and improve experiences:
Confirm an understanding of the aphasia service pathway within service context of interest. Identify key stakeholders needed to inform change (e.g. lived-experience experts, clinical staff, healthcare designers, researchers). Co-design concept designs that translate experiences of care (aligned with priorities) into actionable change with stakeholders, tailored to service contexts. Determine scope (e.g. identify co-design categories)
24
needed to support and resource project planning. Co-design implementation and evaluation with stakeholders. Host celebration and reporting event.
Discussion
Establishing priorities for meaningful and sustainable service improvement requires a joint understanding of the experiences of care. The research aimed to collaboratively identify leading priorities for aphasia service development, and to develop a concept design targeting one of these priority areas. Those involved represented a broad cross-section of service users and providers with diversity in geographic remoteness, age, cultural ethnicity, time post-onset, aphasia severity, and service contexts in Australia. From the 773 ideas put forward, consensus was reached across stakeholders on seven top priorities for co-designing change, indicating these are key priorities for a diverse range of people who both receive or provide aphasia care.
Areas for aphasia service development considered equitable and improved access to suitable or personalised aphasia therapy and treatment options, or access to mental health service options tailored for people with aphasia. All stakeholders identified the need for education and information about care management to be delivered by healthcare providers trained in how to support communication, and for improved co-ordination of care for people with aphasia. The development of communicatively accessible and engaging hospital environments was also universally prioritised. In the current study, self-management of care did not make the final top seven, however, it did feature in those prioritised, across stakeholders. This suggests that while other areas might rank higher, it remains an area of importance. 25 Overall, these priorities reflect stakeholders’ desire to address the unmet needs identified in previous stages of this research.5,6
Across stakeholder groups, we found that a lack of communication support in both hospital and community-based settings was associated with reduced emotional wellbeing.5,6 This study extends upon previous findings, 26 showing that the emotional turmoil associated with the onset (and ongoing burden) of aphasia, coupled with a lack of communication support (e.g. experienced with limited access to mental health services), was not only recognised as an unmet need, but also prioritised for development by all stakeholders (across the care continuum). Importantly, people with aphasia ranked the need to design accessible mental health services higher than: self-management approaches, preparing for home, appropriately formatted education materials, scheduling assistance, or even ways to offer protection against online scams. Given many mental health services involve talk-based therapies, 27 and people with aphasia are almost twice as likely to experience depression or emotional changes post-onset (compared to stroke survivors without aphasia), 28 clinicians should ensure time is spent supporting patients with aphasia to find (and access) suitable and available mental health service resources.
While all stakeholders felt care should be tailored to the individual, each group had a unique take on concepts that should be considered when designing care. For example, all groups reported on the importance of identifying an individual's communication profile, their interests, goals, and personal values.29,30 However, speech pathologists felt tailoring of care should also include tailoring of care delivery options (e.g. hospital, patient home, community context) or the use of alternative approaches for optimal gains (e.g. trialling virtual reality to work on functional or social goals). People with aphasia felt tailoring of care should encompass connecting them with aphasia research opportunities (e.g. clinical trials), offering (accessible) knowledge about new findings in stroke or aphasia research, and providing information on any beneficial health outcomes associated with alternative treatments (e.g. massage, acupuncture, dance, choir).
The top priority, agreed by all stakeholders, was the development of a chart alert system to support centralised access to appropriate communication strategies and resources for healthcare providers. This is comparable with previous research 31 which suggests centralised access to communication aids are needed to support nurses to form communicatively accessible hospital environments. Prior research 32 observing that healthcare providers employ few strategies to support conversation, lack confidence managing communication, and disempower patients with aphasia in their communication interactions (compared to those without aphasia), correspond with our findings. Previous research has additionally shown that patients with post-stroke aphasia experience more complications during stroke admissions compared with stroke survivors without aphasia.9,33 Research reporting healthcare providers avoidance of communication attempts and their challenges communicating with patients with aphasia,8,34 suggest they have fewer conversations about their health than patients without aphasia. The reduced awareness of how to effectively support communication reported in this research5,6 (by all stakeholders), and experiences of people with aphasia not understanding what is happening to them, may indeed reduce their safety while in hospital.
Electronic medical record alerts provide clinicians with real-time, up to date information or reminders that have been shown to improve the safety and quality of care. 35 One way to support clinical decision making and improve the accessibility and delivery of healthcare, might be in the development of such a system for aphasia. Implementation of a chart alert system within an electronic medical record would alert care providers to the presence of aphasia and could direct them to information on suitable communication support strategies. Having an awareness of aphasia, and effective communication strategies (or resources) may improve clinician's confidence with supporting communication and the effectiveness of their interactions. Improved communication interactions may reduce miscommunication or decreased comprehension of what healthcare providers say by those with aphasia, offer opportunities for people with aphasia to express needs, and improve their experiences of care.
Study strengths include the co-development of project design, resources, and processes with our consumer advisory committee. The comprehensive and rigorous consensus processes used to identify top priority improvement areas, with stakeholders representing diversity in aphasia severity, age, time post-stroke, and service context. While the limited diversity in geographic remoteness (consensus and co-design) is acknowledged, the final seven top priorities contain ideas and priorities put forward by stakeholders from regional and remote areas. This suggests that the priorities of stakeholders from these areas have nevertheless been captured. A final limitation is the collection of experience stories (which informed touchpoints) during the COVID-19 pandemic, which may be less representative of care usually provided. However, given the strain COVID-19 pandemic measures exerted on healthcare services, capturing experiences under potentially ‘extreme’ conditions may have highlighted areas for change that might otherwise have gone unnoticed. Future research will complete the co-design, implementation and evaluation cycles incorporated (stages 6–7) in the overarching study design.
This research highlights the increased risk patients with aphasia face in hospitals and the top priority emphasises the relative importance of improving the safety of hospital environments for these populations. Development, implementation, and evaluation of this co-designed concept plan may decrease miscommunication with healthcare providers and enhance experiences of care for people with aphasia during hospital stays. Our findings confirm the importance of increasing healthcare providers awareness of the impact of aphasia, and their capacity to meaningfully engage people with aphasia in conversations about their health. Future research should co-design concept designs to target each of the top priority improvement areas collaboratively identified.
Clinical messages
Aphasia reduces patient safety and the ability to communicate preferences and needs in hospital.
Upskilling healthcare providers in supported communication techniques may reduce patient distress and risk of adverse events and increase compliance with medical recommendations.
Ensuring hospital environments are communicatively accessible and engaging is important to people with aphasia.
Supplemental Material
sj-pdf-1-cre-10.1177_02692155241310579 - Supplemental material for Priorities for post-stroke aphasia service development: Prioritisation phase of an experience-based co-design study
Supplemental material, sj-pdf-1-cre-10.1177_02692155241310579 for Priorities for post-stroke aphasia service development: Prioritisation phase of an experience-based co-design study by Lisa Anemaat, Victoria J Palmer and David A Copland, Geoffrey Binge, Kent Druery, Julia Druery, Kathryn Mainstone, Bruce Aisthorpe, Sarah J Wallace in Clinical Rehabilitation
Supplemental Material
sj-pdf-2-cre-10.1177_02692155241310579 - Supplemental material for Priorities for post-stroke aphasia service development: Prioritisation phase of an experience-based co-design study
Supplemental material, sj-pdf-2-cre-10.1177_02692155241310579 for Priorities for post-stroke aphasia service development: Prioritisation phase of an experience-based co-design study by Lisa Anemaat, Victoria J Palmer and David A Copland, Geoffrey Binge, Kent Druery, Julia Druery, Kathryn Mainstone, Bruce Aisthorpe, Sarah J Wallace in Clinical Rehabilitation
Supplemental Material
sj-pdf-3-cre-10.1177_02692155241310579 - Supplemental material for Priorities for post-stroke aphasia service development: Prioritisation phase of an experience-based co-design study
Supplemental material, sj-pdf-3-cre-10.1177_02692155241310579 for Priorities for post-stroke aphasia service development: Prioritisation phase of an experience-based co-design study by Lisa Anemaat, Victoria J Palmer and David A Copland, Geoffrey Binge, Kent Druery, Julia Druery, Kathryn Mainstone, Bruce Aisthorpe, Sarah J Wallace in Clinical Rehabilitation
Supplemental Material
sj-pdf-4-cre-10.1177_02692155241310579 - Supplemental material for Priorities for post-stroke aphasia service development: Prioritisation phase of an experience-based co-design study
Supplemental material, sj-pdf-4-cre-10.1177_02692155241310579 for Priorities for post-stroke aphasia service development: Prioritisation phase of an experience-based co-design study by Lisa Anemaat, Victoria J Palmer and David A Copland, Geoffrey Binge, Kent Druery, Julia Druery, Kathryn Mainstone, Bruce Aisthorpe, Sarah J Wallace in Clinical Rehabilitation
Footnotes
Acknowledgements
We would like to acknowledge each of people living with aphasia, their significant others, and the speech pathologists who generously contributed their time to this research. We would also like to thank members of the consumer advisory committee for their valuable input, Mr Geoffrey Binge for his expert guidance on respectfully engaging Aboriginal and/or Torres Strait Islander Peoples, speech pathology management staff from participating sites, and Margot Sexton, Emma Caird, Bridget Burton, Kimberly Garden, Aoife Reardon, and Jessica Campbell from the Queensland Aphasia Research Centre.
Author Contributions
LA was responsible for the initial draft of this manuscript, research design, all data collection, analysis, and interpretation as part of her doctoral studies. SW, DC, and VP provided regular supervision throughout, contributed to research design, data analysis, interpretation and critical review and editing to revisions of the manuscript. Members of the consumer advisory group: KM (person with aphasia), KD (person with aphasia), JD (family member of a person with aphasia), BA (person with aphasia), GB (cultural capability officer for the Royal Brisbane and Women's Hospital, and a proud Kamilaroi man from North West New South Wales, Australia), PM (family member of a person with aphasia) provided input on methods, research design, co-designed resources used (with LA and SW), recruitment processes, analysis, and dissemination. All authors have read and approved the final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by The University of Queensland Aphasia Rehabilitation Research Fund (2018–2023) and a New Researcher grant awarded by Speech Pathology Australia (2020). SJW is supported by a National Health and Medical Research Council (NHMRC) Emerging Leadership Investigator Grant (Grant No. APP1175821) and LA is supported by The University of Queensland—Research Training Program Scholarship (QARC).
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.