
Abstract
Objective:
To identify the barriers and facilitators to goal-setting during rehabilitation for stroke and other acquired brain injuries.
Data sources:
AMED, Proquest, CINAHL and MEDLINE.
Review methods:
Two reviewers independently screened, extracted data and assessed study quality using the Mixed Methods Appraisal Tool and undertook thematic content analysis for papers examining the barriers and facilitators to goal-setting during stroke/neurological rehabilitation (any design). Last searches were completed in May 2016.
Results:
Nine qualitative papers were selected, involving 202 participants in total: 88 patients, 89 health care professionals and 25 relatives of participating patients. Main barriers were: Differences in staff and patients perspectives of goal-setting; patient-related barriers; staff-related barriers, and organisational level barriers. Main facilitators were: individually tailored goal-setting processes, strategies to promote communication and understanding, and strategies to avoid disappointment and unrealistic goals. In addition, patients’ and staff’s knowledge, experience, skill, and engagement with goal-setting could be either a barrier (if these aspects were absent) or a facilitator (if they were present).
Conclusion:
The main barriers and facilitators to goal-setting during stroke rehabilitation have been identified. They suggest that current methods of goal-setting during inpatient/early stage stroke or neurological rehabilitation are not fit for purpose.
Introduction
Goal setting is a key part of stroke rehabilitation and is recommended in National Clinical Guidelines.1–5 It is said to enhance patient confidence and motivation, engagement in, and satisfaction with rehabilitation, whilst improving task performance, team communication and team work and, possibly improving recovery, goal achievement and self-care.6,7 This evidence has been summarised in two systematic reviews.6,7 Rosewilliam et al. 6 reviewed the effects of patient-centred goal-setting during stroke rehabilitation up to 2010, while Sugavanam et al. 7 assessed the effects and experience of using goal-setting in stroke rehabilitation up to 2011. Both found that low methodological quality and heterogeneity of the selected studies meant that no firm conclusions regarding the effects of goal-setting could be drawn. Furthermore, both noted that adoption of patient-centred goal-setting was limited and faced multiple challenges, not least discrepancies between patients’ and staff’s perceptions and experience.
This is supported by work on staff’s perspectives of goal-setting.8–12 Patient-centeredness is a central tenet of goal-setting. That is, patients should be actively involved in the process with clinicians who understand and respect their needs. 13 However, the use of patient-centred goal setting appears to be a challenge. Both patients and clinicians often report difficulty with this approach, particularly during in-patient rehabilitation.6,9,11,12,14–17 Limited patient participation, professional skill and conflicting priorities are considered contributory factors to the difficulty using patient-centred goal-setting. 11 Several different methods of goal setting during stroke rehabilitation have been proposed2,6,7,17–21 but no method of choice has emerged.6,7,22,23
Thus as an initial stage to developing a goal-setting model which addresses the barriers to uptake during in-patient stroke rehabilitation, we undertook a mixed methods systematic review of contemporaneous evidence to specifically identify the barriers and facilitators to goal-setting during stroke rehabilitation using the ENTREQ guidelines for meta-synthesis. 24
Method
Electronic databases (AMED, Proquest, CINAHL and MEDLINE) were searched from their earliest date to May 2016 using the following keywords: goal or goal set* or GAS or goal attainment AND Stroke or cerebrovascular accident or TBI or ABI or head injury or brain injury, rehab*, or *therapy AND
Barrier* or facilitat*.
In addition we searched the reference lists of papers selected for the full text review for any further articles that met the selection criteria. All searches were limited to studies in a full peer reviewed publication, written in English and involving human adults. The search strategy is shown in Supplementary Appendix 1.
Two reviewers (SP and ST) independently screened the titles, abstracts and then full texts of articles identified by the search against the selection criteria. These were:
Any types of research design excluding systematic reviews (although the reference list of any systematic reviews were screened for additional papers that could be selected).
Regarding the barriers and facilitators to goal setting.
Involved adult patients with stroke or other acquired brain injuries under-going rehabilitation and/ or their families, carers or the health care professionals treating them.
Studies involving participants with conditions other than stroke or acquired brain injury were included if at least 50% of patients had stroke or acquired brain injury.
The following data were extracted from the selected studies and tabulated: the method (research approach, data collection process and analysis); participants and main themes identified (Supplementary Table 1). The methodological quality of the selected studies was independently assessed by two of the authors (SP and SK) using the Mixed Methods Appraisal Tool 25 Consensus was achieved through discussion with a 3rd person (ST) to act as arbitrator if necessary. The Mixed Methods Appraisal Tool is designed to structure the appraisal of complex systematic reviews involving studies that use a range of methodologies. It enables the methodological quality of mixed methods, qualitative and quantitative studies to be described and evaluated using different evaluation criteria for each. The criteria assessed reflect the factors which impact on the risk of bias, completeness and transparency. They are detailed in Supplementary Table 2(a) and 2(b).
Finally, thematic content analysis was used to draw out key themes from the findings of the selected studies. 26 The results were read several times by three of the authors (ST, SP and JP) to familiarise themselves with the content. Then main findings relating to barriers and facilitators to goal-setting were identified and open coded using Excel spreadsheets. The codes were analysed and grouped into themes, and refined to develop sub-themes or categories. Then the papers were read again and further data supporting or contradicting the themes and categories were added, and the data were iteratively summarised and clustered by all authors until consensus was reached.
Results
The searches initially identified 1034 papers. After removing of duplicate and screening of titles and abstracts this was reduced to 25 papers, which were assessed for eligibility. Sixteen papers were subsequently rejected after evaluation of the full text, leaving nine selected papers.10–12,14,16–19,27 The PRISMA diagram for the search is shown in Figure 1, details of the rejected papers are shown in Supplementary Appendix 2.
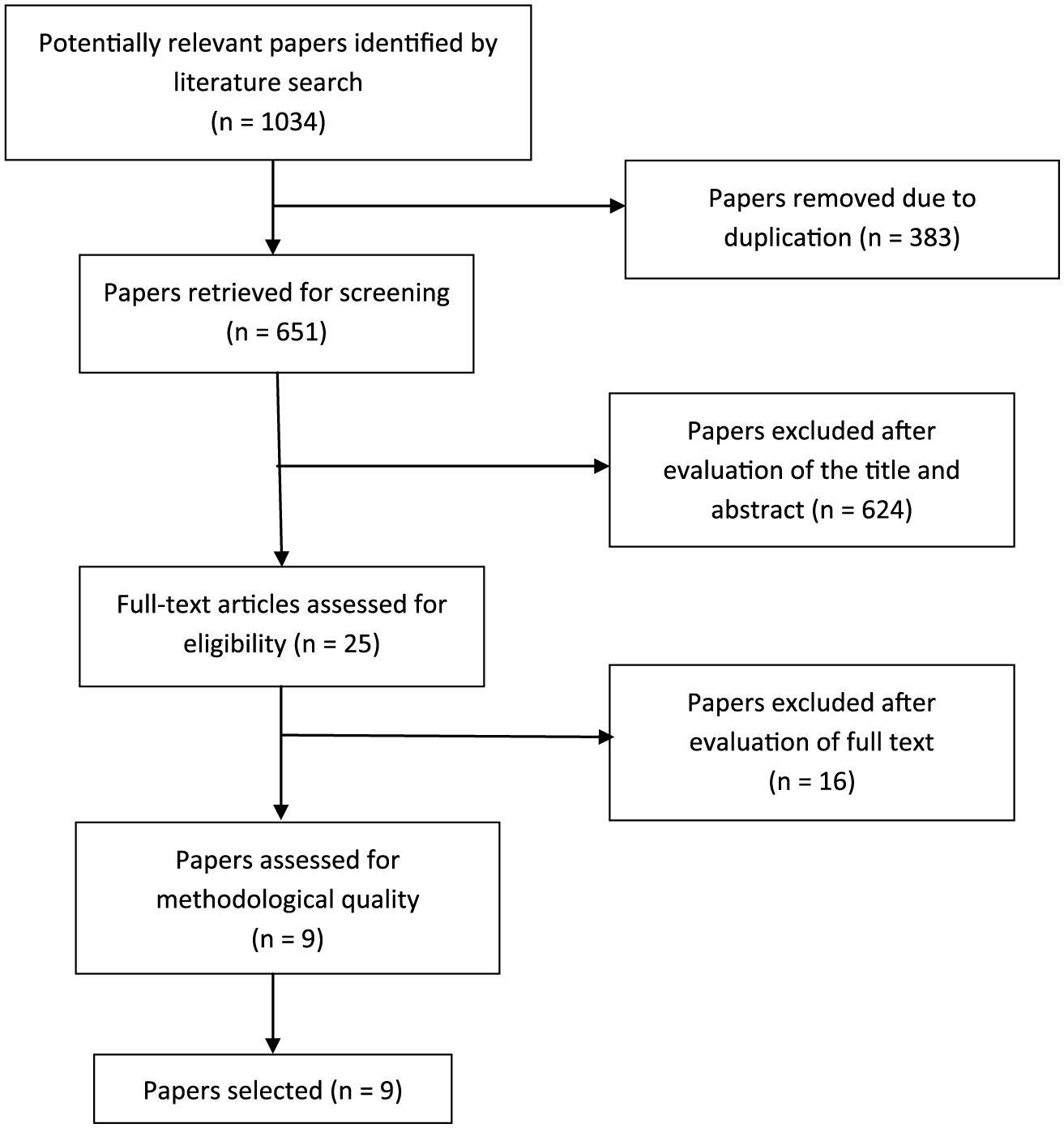
Showing the results of the search strategy.
All the selected papers used a qualitative design; three used face-to-face interviews to collect the data,9,14,27 one used telephone interviews 16 one used email interviews, 17 two used focus groups,12,18 and two used mixed methods (interviews, observations and document analysis).11,19 All studies used thematic content analysis as the means of data analysis.
The selected papers involved 202 participants in total: 88 patients, 89 health care professionals and 25 relatives of participating patients. Three studies involved patients alone;16,18,27 two involved staff alone;12,17 one involved staff and patients 19 and two involved staff, patients and relatives.11,14 Full details are found in Supplementary Table 1. All but one selected paper 12 involved in-patient rehabilitation on specialist stroke or rehabilitation units, although two studies14,27 interviewed patients after their discharge. The stroke survivor participants were typical of the in-patient stroke rehabilitation population; approximately equal numbers of men and women, mostly in the sub-acute stages of stroke. Their ages ranging from early adulthood to extreme age and most mean ages were in the early 60’s. Staff participants covered the full range of the multidisciplinary team (18 physiotherapists; 18 occupational therapists; 12 speech therapists; 24 nurses; 8 doctors; 4 psychologists; 2 social workers; 1 dietician and 1 cultural advisor). The family participants involved 17 spouse/partners, five adult children and three parents.
All the selected papers were of good quality (Supplementary Table 2(a) and 2(b)), answering ‘Yes’ to most quality criteria, and were included in the synthesis stage.
Four themes emerged as barriers to goal-setting: Differences in staff and patients perspectives of goal setting; patient-related barriers, staff related barriers, and organisational or service level barriers. Three themes emerged as facilitators to goal setting: an individually tailored goal-setting process; strategies to promote communication and understanding; and avoiding disappointment and unrealistic goals. In addition, staff’s and patients’ knowledge, experience and enthusiasm for goal-setting emerged as either a barrier (if these characteristics were absent) or a facilitator (if they were present) to goal-setting.
Barriers to goal-setting
Differences in patients’ and staff’s perspective of goal setting
Most authors11,14,16,17,19,27 noted a mismatch between staff’s and patients’ perspective which hampered goal-setting. They noted that goals set by patients tended to be broad and involve their hopes and aspirations, such as “to improve” 27 or to be “back to normal”.14,16 Their focus was on the long-term, regaining physical function and independence and returning to former activities and roles.11,14,17,18,27 In contrast, staff member’s goals tended to be short-term, specific, focus on impairments and were conservative in ambition and driven by financial and organisational pressures.10,11,14,16,17,19,27
The staff goals tended to take priority over the patients’ and family’s.11,14 While Levack et al. 11 felt this caused tension between staff and patients/families, others reported that patients were satisfied with, and expected this priority. They assumed staff “were experts” who “knew their job” and would guide them through the recovery process while the patients felt they were novices in recovery process and expected to be led by the staff.14,16,27
This perspective has led some to question whether patient-led goal setting is realistic or desirable during early stage stroke rehabilitation. 11 Brown et al. 27 explained how after discharge and in the later stages of rehabilitation, patients were more able to identify and negotiate personally significant goals and wanted to work on things that “made me, me”. It is at this point that ‘traditional’ patient-focussed goal-setting may be most appropriate.
Patient related barriers to goal-setting
In several studies, staff identified factors relating to the severity of the patient’s stroke such as communication difficulties, cognitive impairments, fatigue and mood disorders as barriers to their involvement with goal-setting.14,17,19,27 Those with passive personality traits, considered to lack insight, be “in denial” or over-whelmed by the impact of their stroke were also felt to find goal-setting difficult, 14,17 while co-morbidities and a fluctuating medical condition was also identified as barriers. 19
A further barrier, reported by both staff and patients was patients’ and family’s lack of knowledge of their condition, and thus their understanding of their problems, rehabilitation process and potential for recovery.12,14,16–19,27 They reported that patients often felt stroke recovery was unpredictable and could not be planned for especially in the early stages of rehabilitation.18,27 Van de Wyer et al. 12 described how both staff and patients felt that in the early stages of rehabilitation, patients did not know what recovery was possible and thus did not “know what they want” and thus found goal-setting challenging.
Patient preferences were a further barrier; goal-setting was not for everyone. Several authors found that some patients did not appreciate a need for goal-setting. They reported that some patients felt the staff’s goals during in-patient rehabilitation, which focussed on impairments and the basic activities of daily living were “common sense”.14,16,27 They viewed daily activities, such as walking or washing and dressing as “normal everyday things”, that everyone would want/need to do. Thus, they were a necessity rather than a goal to be chosen.16,27 Furthermore, the patients believed that staff had an plan for their recovery that patients needed to work through and they did not question this as it “went without saying”.16,27 Others felt a formal goal-setting process was unnecessary; feedback from staff would suffice 27 or that they would recover whether goals were set or not, 18 while some preferred to keep their hopes and plans private or were concerned that felt their views might limit the scope of rehabilitation. 27
Patients’ previous experiences of setting goals were also a factor. These experiences were often associated with their workplace where goals were used as performance measures. This therefore had negative connotations for goal-setting during rehabilitation and made patients less interested in be involved in the process. 18
Staff related barriers to goal-setting
Several barriers identified by staff mirrored those of the patients. Staff too were uncertain about how much recovery was possible, especially in the early stages of rehabilitation 18 and how to involve patients soon after their stroke when they “did not know what they wanted” and found goal identification difficult. 12 Many staff also considered that patients’ expectations of recovery (their desire to “get better”) were unrealistic and thus a barrier to effective goal-setting. Coupled to this, they had concerns about their ability to manage these expectations and were concerned to avoid disappointment, or disagreement with patients if recovery was less than hoped,11,12,14,19 which would hamper goal-setting. A further barrier was concern about their ability to manage team discussions while the patient is present. 12
Organisational or service level barriers to goal-setting
The most frequent organisational barrier to goal-setting during rehabilitation was lack of time, especially when there was an emphasis on involving patients in the process.11,12,17,19 Other barriers related to the need to co-ordinate staff, which was hampered by inflexible working practices and shift patterns;12,17 duplication and difficulty transferring information between multiple record systems; 19 integrating goal-setting with other rehabilitation processes:17,19 staff turn-over which required on-going training and support for less experienced and skilled staff, 19 and the pressure of competing priorities, particularly to provide ‘hands-on therapy’.12,19
Facilitators to goal-setting
Individually tailoring the goal-setting process to patients’ preferences
Laver et al. 16 and Brown et al. 27 described how goal-setting was facilitated by tailoring the process to individual patients’ needs and preferences. They identified how some patients wanted high level, long-term ambitious goals which they found motivating, but others found this overwhelming as they feared they may be disappointed. They preferred smaller, shorter term steps to build confidence. 27 Further, some patients wanted to start using goal-setting as soon as possible after their stroke but others initially felt over-whelmed and needed some time to get used to their new situation. 16 Many patients did not want too many goals and felt each goal should be prioritised. 27
The locus of goals also needed to be individualised to facilitate a goal-setting process that suited each individual patient. Some patients had a ‘patient-led’ locus and were keen that personally significant goals (“things that make me, me”) should be included. 27 However, as noted in the section above, others, particularly in the early stages of stroke rehabilitation often preferred a more therapist-led locus. The selected studies that did not use explicitly patient-led goal-setting, indicated that the goals set did, indeed, tend to be therapist-led11,16,17,19,27 while Levack et al. 11 identified strategies that staff used to ensure ‘their goals’ were prioritised (detailed in Supplementary Table 1).
Strategies to promote communication and understanding of goal-setting
Patients reported that goal-setting was facilitated by open, early and frequent communication with patients and their families10,19,27 about the goal-setting process. The process was further enhanced by a positive, encouraging and reassuring attitude from the staff. 27 Goal-setting was felt to be further enhanced by explicit strategies to educate patients and families about goal-setting and enhance participation.10,17,27 None of the studies considered that further education of staff about goal-setting might facilitate the process.
The provision of material to support patients to identify goals were found helpful.10,12,17,27 These included examples of suitable goals; using stock/pre-prepared phrases and questions; work-sheets; a patient-held folder with relevant information, pictures and copies of the goals; using action plans as ‘stepping stones’ to achieving goals; and formal patient-held records facilitated the goal-setting process.10,12,17,27 Participants felt these tools helped to clarify expectations; guided patient-led therapy; enabled progress to be monitored and facilitated family involvement.10,12,17,27 For patients with communication or cognitive limitations, using ‘aphasia friendly’ materials, communication aids, images, and input from speech therapists facilitated goal setting,17,19 although patients with these impairments were often excluded from studies of goal-setting and the goal-setting process.
Input from a experienced and skilled key-worker to help patients negotiate the process was considered faciitatory. 12
Finally, Levak et al. 10 specifically looked at the impact of family involvement in goal-setting process. They reported that early involvement of family could facilitate goal-setting, but contrary to the general ethos to promote family involvement in rehabilitation, this was not always helpful. It could interfere with patient–clinician goal negotiation and relationships. Family members were sometimes seen as disruptive with their own agendas and not always acting in the patients’ interests. In some cases, staff reported that goal-setting was facilitated by excluding family members from the process. 10
Avoiding disappointment and “unrealistic goals”
It was thought that patients’ unrealistic goals could be avoided through counselling and focussing on short-term goals. 14 Disappointment could be avoided by talking to patients and families about barriers to achieving goals and making plans to overcome them; regular reappraisal, feedback and re-negotiation when necessary; reframing failure in a positive way; and focussing on goals that had been achieved while avoiding goals that were not. 19
Resources
Van de Weyer looked at organisational factors impacting on goal-setting. 12 They noted sufficient resources were needed for effective goal-setting, as were sufficient time and expertise within the team. An effective chair for goal-setting meetings and a functional multi-disciplinary team was needed and this was facilitated by electronic records and other ‘alternative’ communication methods.
Discussion
This systematic review aimed to summarise the barriers and facilitators to goal-setting during stroke rehabilitation with a view to improving future practice. The findings identify that the main barriers to goal-setting are: a mismatch between patients’ and staff’s expectations, perspective of goals and recovery; patients’ lack of knowledge about goal-setting, rehabilitation processes and their potential for recovery; their lack of skill in goal-setting; patients’ stroke-related impairments; and organisational pressures.
We found that goal-setting can be facilitated by early, effective communication between staff and patients; tailoring the goal-setting process to individuals’ preferences; providing support material; education for patients and families to build goal-setting skills and confidence; and appropriate resourcing. The involvement of families in goal-setting can be either a facilitator especially if involved early on in the process or a barrier (if families have their own priorities and do not act in the patients’ best interests). Importantly, we identified that, contrary to the received wisdom that a patient-centred approach is an essential and desirable element of effective goal-setting, we found, in the early stages of rehabilitation patients often expect a therapist-led approach.
The two previous systematic reviews of the effects of goal-setting6,7 also identified differing perspectives between patients and staff and the need for education. Like the current review, they noted that a patient-centred approach to goal-setting was not always welcomed by patients or staff, particularly during the early stages of rehabilitation which typically occurs while an in-patient. However, the current review is the first to specifically detail the barriers and facilitators with a view to developing a new model for practice
The emphasis on patient-centred goal-setting found in the selected papers is a reflection of the biopsychosocial model of care that aims to maximise activities and participation and is considered a fundamental element of effective rehabilitation28–30 although evidence to support (or refute) its efficacy is weak. 6 However, it may be that, for some patients at least, in-patient rehabilitation is a transition phase from a medical to biopsychosocial model. In-patient rehabilitation typically occurs during the acute and sub-acute phases of recovery, when relatively rapid recovery can occur, so a short-term focus may appropriate. It is also a time when impairments may be improving and patients are just beginning to regain activities, so, again, goals regarding impairments and basic activities of daily living may be most appropriate. Furthermore, an emphasis on participation during in-patient rehabilitation may be inappropriate as the patient has not yet had opportunity to explore his/her capabilities and priorities in their own environment.
The results of the current review suggest that a more flexible approach is needed. There are points, particularly early in the rehabilitation process when a clinician-led, impairment-based medical model may suit some patients better and thus may be more effective. The results of this review and others6,7 highlight that the main problem with goal-setting is that both patients and clinicians struggle to identify and negotiate goals.18,31-34 This difficulty may be because patient-centred goal-setting is not ‘fit-for-purpose’ for all stages of rehabilitation and for all patients. The clear message from the current review is that the process of goal-setting needs to be tailored to individual patients’ needs and preferences, which may change with time. Although some patients were critical of their experience of goal-setting in the early stages of rehabilitation, others noted that once they had returned home and had some experience of ‘their life after stroke’, they became more able to identify priorities and willing/able to compromise their hopes and ambitions.14,27 It may be at this point that a patient-centred approach is most acceptable and effective.
Patient-centred goal-setting does have potential to facilitate the choice of rehabilitation activities outside formal therapy sessions however. By focusing on the patients’ preferences and needs, their important and preferred activities can be identified, which should in turn promote compliance and satisfaction.
The challenge for stroke rehabilitation researchers and clinicians is to develop a more sophisticated and nuanced model of goal setting which can accommodate the necessary degree of flexibility to suit more patients, more of the time. This needs to encompass diversity in the degree and type of engagement, not merely goal identification, negotiation and selection. Several ways of doing this have been suggested such as using goal-action planning 19 ; goal ‘banks’;22,27,35,36 standardised measures and specific goal setting tools such as Canadian Occupational Performance Measure or Goal Attainment, 22 but no gold standard has been established. 2 Additionally, further investigation is needed to establish how selected goals can best be integrated with other aspects rehabilitation, such as treatment planning and decision-making.
The need for education for patients to understand the rehabilitation process, recovery potential and goal-setting skills runs through all the studies selected for this review. Involving the patient early and actively in the goal-setting process; providing support materials and ‘aphasia’ friendly information, and active communication (such as empathetic listening and negotiation skills) are recommended to facilitate goal-setting. Further research is needed, possibly using techniques such as experience based co-design37,38 to ensure any new developments are fit-for-purpose. Interestingly, although staff identified the difficulties they had with goal setting, particularly goal identification and negotiation and managing patients’ expectations, they did not identify a need for their own training to address and overcome the barriers. The development of new goal-setting methods needs to include training elements to ensure staff can obtain the relevant skills and confidence.
Although the results of this review give a clear direction to how improvements in goal-setting during stroke rehabilitation can be implemented, the work has several limitations which should be taken in to account. Like all reviews, it is only as good as the papers selected. We did not have the resources available to include papers which were not written in English, nor to contact researchers for unpublished work. Subsequently we may have missed some papers with relevant information which could produce some publication and reporting bias. However our search strategies were robust, the papers we identified were of good quality, their participants were representative of our population of interest and their findings consistent so we feel that any missed papers are unlikely to change the main conclusions of this review. The other issue is to reflect on the potential influence of the authors, particularly during the analysis. Three of us (SP, ST, JP) are experienced stroke physiotherapists turned academics. ST is leading a programme of work examining the function of multi-disciplinary teams during stroke rehabilitation with a view to improving practice and ultimately outcomes. Her focus is the pragmatics of service delivery, rather than developing underlying theories of how teams practice. SP is a research physiotherapist who is studying goal-setting during stroke rehabilitation for a Master programme. JP has a more theoretical and qualitative interest and has previously worked extensively on goal-setting in elder rehabilitation. SK is an academic nurse with expertise in qualitative methods and meta-synthesis.
Clinical messages
The main barriers to goal-setting during stroke rehabilitation are:
A mismatch between patients’ and staff’s perspective.
Staff lack of confidence to manage patient expectations.
Patients’ stroke related impairments.
Insufficient time and ineffective organisational systems.
The main facilitators are:
Early, frequent, active communication with patient and family.
Individually tailoring the goal-setting process.
Effective, confident and encouraging staff.
Education of patients and families.
Provision of supporting, educational materials.
Adequate resources.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.