
Abstract
Introduction
Venous leg ulcers (VLUs) account for up to 80% of chronic lower limb ulcers. The management of these ulcers is complex and can involve multiple interventions, ranging from compression, to pharmacotherapy, surgical and endovenous procedures. Despite these, VLUs are associated with prolonged healing times and high recurrence rates. They therefore pose a significant burden to both patients and the healthcare system, costing the National Health Service over £3 billion annually. Previous studies have largely compared interventions with standard of care rather than against each other. Due to a lack of head-to-head comparisons, this network meta-analysis is necessary to establish which adjunctive intervention, when combined with compression therapy, is most effective in healing VLUs.
Methods
This network meta-analysis was completed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the PRISMA for Network Meta-Analyses (PRISMA-NMA) extension. A comprehensive search algorithm identified all relevant human studies published in English across MEDLINE, EMBASE, ClinicalTrials.gov and PubMed databases. This study included only randomised controlled trials reporting on complete venous leg ulcer healing rates at 24 weeks on patients over the age of 18 years. Two independent authors screened and reviewed all articles for inclusion and performed data extraction.
Results
The search resulted in 2,237 papers. Of these, 15 randomised controlled trials met the inclusion criteria, enrolling a total of 2,571 patients. Four studies evaluated pentoxifylline, three looked at ablation, three studied sclerotherapy, two evaluated surgery, one studied aspirin, one focused on flavonoids and one on ultrasound therapy. All studies employed these interventions as an adjunct to compression. Both pentoxifylline (OR 3.1, CI 1.46 – 6.57, p < .05) and endovenous ablation (OR 2.86, CI 1.19 – 6.88, p < .05) were shown to significantly improve ulcer healing at 24 weeks when compared to compression monotherapy. No other interventions demonstrated a statistically significant improvement in ulcer healing. Heterogeneity was moderate across the studies (I2 = 66.4%) and there was moderate inconsistency in the network (Q score = 20.82, p < .05).
Conclusions
The results demonstrate the potential for pentoxifylline and endovenous ablation to have a significant beneficial impact on ulcer healing. However, the results should be interpreted with a degree of caution given the moderate heterogeneity and inconsistency. Further large-scale randomised controlled trials evaluating interventions in head-to-head comparisons are needed in the future.
Introduction
Venous leg ulcers (VLU) account up to 80% of chronic lower limb ulcers. 1 Within the UK, VLU prevalence is estimated at 1% of the population, with prevalence increasing with age and expected to rise due to an ageing population with multiple comorbidities.1,2 Prolonged healing times and high recurrence rates are commonly associated with VLUs.2,3 This poses a significant burden to patients by affecting their overall quality of life, as well as having a considerable psychological impact. It also places a substantial burden on health care systems, costing the National Health Service over £3.2 billion annually. 4
There are numerous treatments available that aim to treat VLUs, with the established gold standard internationally being compression therapy.5–7 National and international guidelines6,7 also recommend superficial venous reflux treatment, including both conventional surgery such as high ligation and stripping, and endovenous options (e.g. thermal ablation, sclerotherapy). 9 Endovenous treatment is now the preferred modality for both patients and clinicians based on level 1 evidence supporting its efficacy. However, it should be noted that there exists heterogeneity in this evidence base, attributable to diverse populations, varied inclusion criteria, and different analytical approaches.
Real world data suggests that most patients with VLUs are managed in the community, with various barriers in place preventing timely review and treatment in secondary care. 10 This often either precludes or delays surgical or endovenous interventions for this patient population, leading to poor healing rates reported in the literature of up to 30% after 6 months. 11 Given that chronic non-healing ulcers can cost up to 4.5-times than healing ulcers to manage (£13,455 vs £2,981), 12 there is also a pressing financial need to consider the relative effectiveness of all possible treatments to aid VLU healing. There is increasing discussion regarding the use of pharmacological therapies, which can be delivered in the community in conjunction with compression. Therapeutics that have been investigated include, but are not limited to, pentoxifylline, sulodexide, flavonoids and, more recently, aspirin. The European Society for Vascular Surgery, for example, gives a Class IIa Level A recommendation that states “medical treatment with venoactive drugs should be considered to reduce venous symptoms and oedema, based on the available evidence for each individual drug”. 13 However, it is important to note that these therapies have a weaker evidence base due to lower quality randomised controlled trials (RCTs).
There is clearly a wide range of treatments available for VLU management and equally evidently, there remains no clear guidance on each intervention’s relative effectiveness. The current body of evidence is varied in quality and while some interventions work for most individuals, they do not work for others. The underlying reason for this variation is unknown. Typically, previous studies have largely compared interventions with the standard of care rather than against each other. Due to the lack of robust head-to-head comparisons between these interventions, this network meta-analysis is needed to understand which adjunctive intervention, when used with compression, has the most potential for improving venous ulcer healing.
Methods
A network meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the PRISMA for Network Meta-Analyses (PRISMA-NMA) extension. The review was prospectively registered on PROSPERO (CRD420251047725). A search algorithm, using MeSH headings, was created to systematically search PubMed, ClinicalTrials.gov, MEDLINE and EMBASE databases for all relevant human studies published in English.
Inclusion and exclusion criteria
This study included any article which reported on complete ulcer healing rates at 24 weeks on patients over 18 years of age with a venous leg ulcer. Only randomised controlled trials published in the English language were included. Any article reporting on mixed or arterial ulcers were excluded. Reviews, case reports, editorial letters and opinion pieces were also excluded.
Data extraction and critical appraisal
The search results were uploaded into the reference management software programme, Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia, 2022). Following the removal of duplicates, two independent reviewers (S.D., M.S.) screened the title and abstracts of publications. Full text review was completed and articles that met the inclusion criteria were extracted. The references of the included studies were carefully reviewed for additional articles that met inclusion criteria. Any discrepancies were discussed and resolved with a third reviewer (M.T.).
The following data was extracted from each article: patient demographics, the number of patients with a VLU, ulcer duration and size, the rate of complete ulcer healing, time taken for the ulcer to heal, recurrence rate of the ulcer and time to recurrence. Ulcer healing was defined as complete re-epithelisation of the skin with no scab present. The primary outcome for the network meta-analysis was complete ulcer healing at 24 weeks.
Statistical analysis
Statistical analysis was performed using R (R Core Team, GNU GPL v2 License). A frequentist network meta-analysis was conducted using a random-effects model. Network plots were created with the thickness of each arm representing the number of studies included in that arm. Model consistency was calculated using the Q score and the I2 test was used to assess statistical heterogeneity of effect size between the trials. Meta-regression was performed where possible.
Quality and risk of bias assessment
The studies were assessed for risk of bias using the Cochrane risk of bias tool for randomised controlled trials. This was completed by two independent reviewers (S.D., M.S.). Any discrepancies were discussed and resolved with a third reviewer (M.T.).
Results
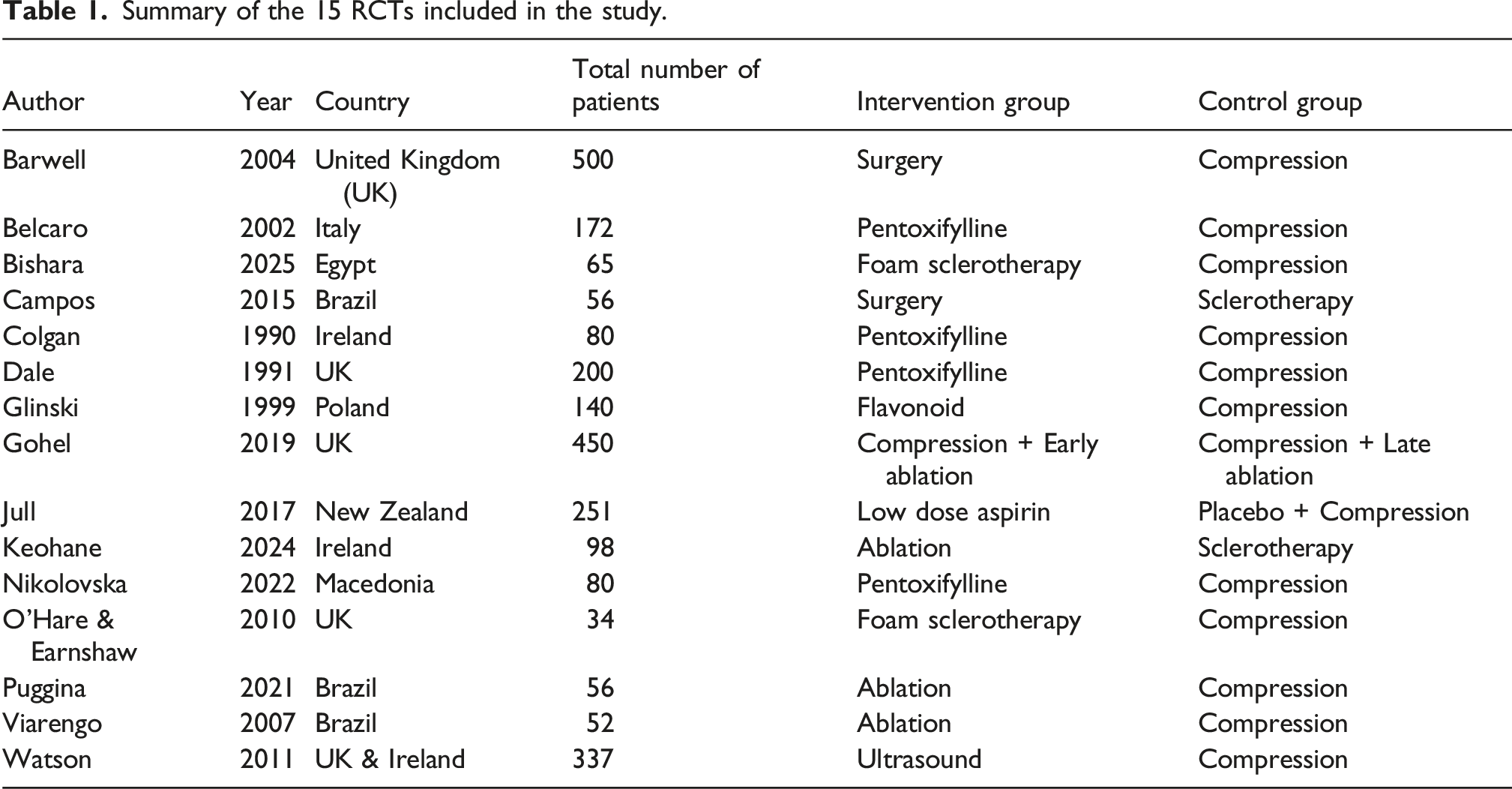
There were a total of 2,238 studies identified from the search (Figure 1). Fifteen studies met the inclusion criteria and were included for analysis (Table 1). PRISMA diagram. Summary of the 15 RCTs included in the study.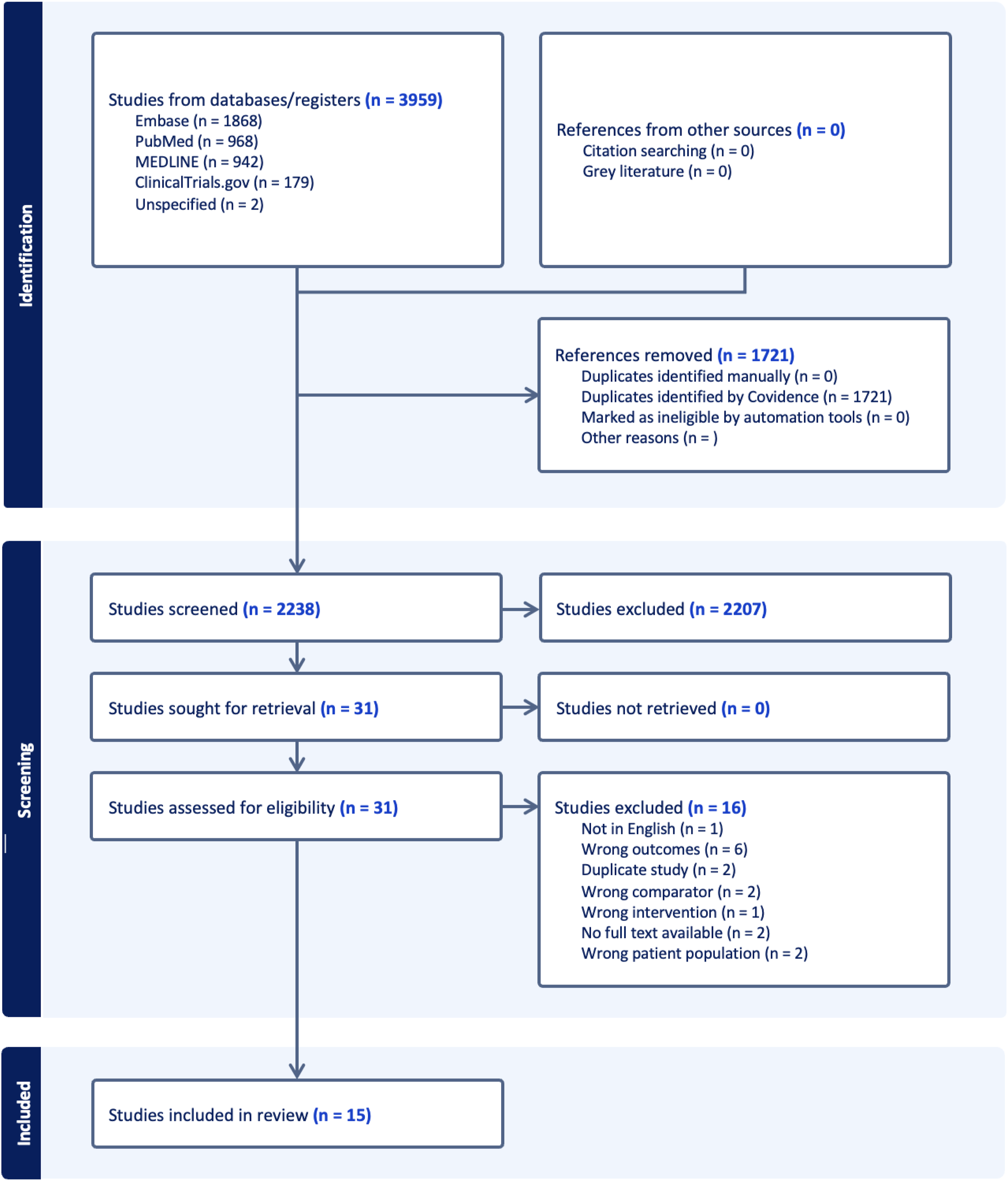
Risk of bias
Risk of bias assessment was conducted. No study was considered to have an overall high risk of bias. Most of the studies were at low risk of bias, with only five studies considered to have some concerns (Figure 2), suggesting that the findings from this set of studies is likely to be relatively robust. However, when considering the individual domains, most studies had concerns when it came to deviations from intended interventions and the measurement of the outcome. These potential protocol deviations and biased outcome assessment must be considered when interpreting the results below. Risk of bias table.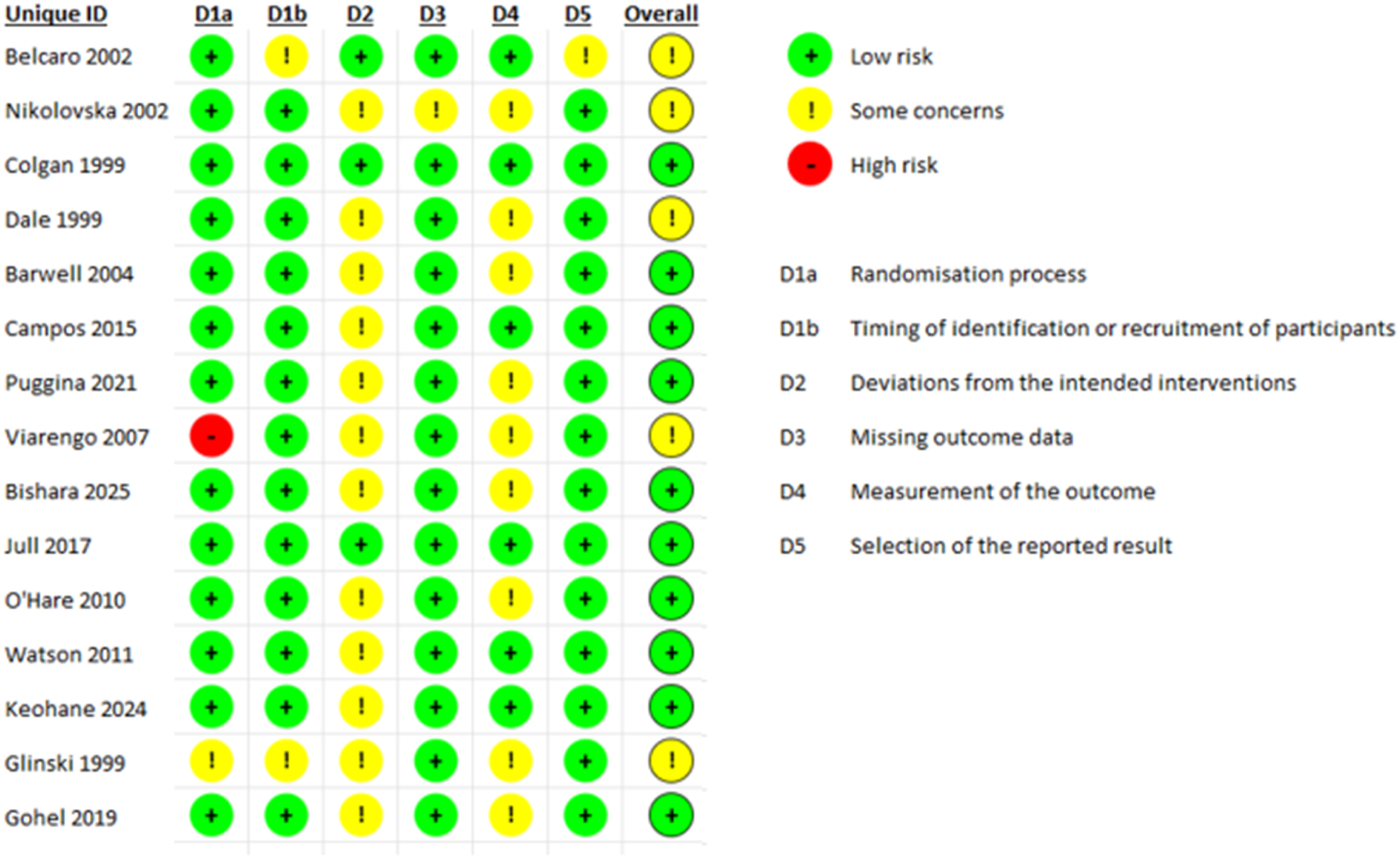
Study characteristics
All studies were RCTs, enrolling a total of 2,571 patients. These studies were conducted between 1990 and 2025 in the UK (n = 5), Europe (n = 5), Egypt (n = 1), Brazil (n = 3) and New Zealand (n = 1). Four studies evaluated pentoxifylline, two evaluated surgery, one studied aspirin, seven studies looked at endovenous interventions (both ablation and sclerotherapy), one focused on flavonoids and one on ultrasound therapy. All studies ensured that patients received compression therapy in addition to any further interventions. All pharmacological RCTs used oral medication. Heterogeneity was high across the studies (I2 = 62%) and there was moderate inconsistency between designs (Q score = 21.08, p < .05).
Ulcer healing outcomes
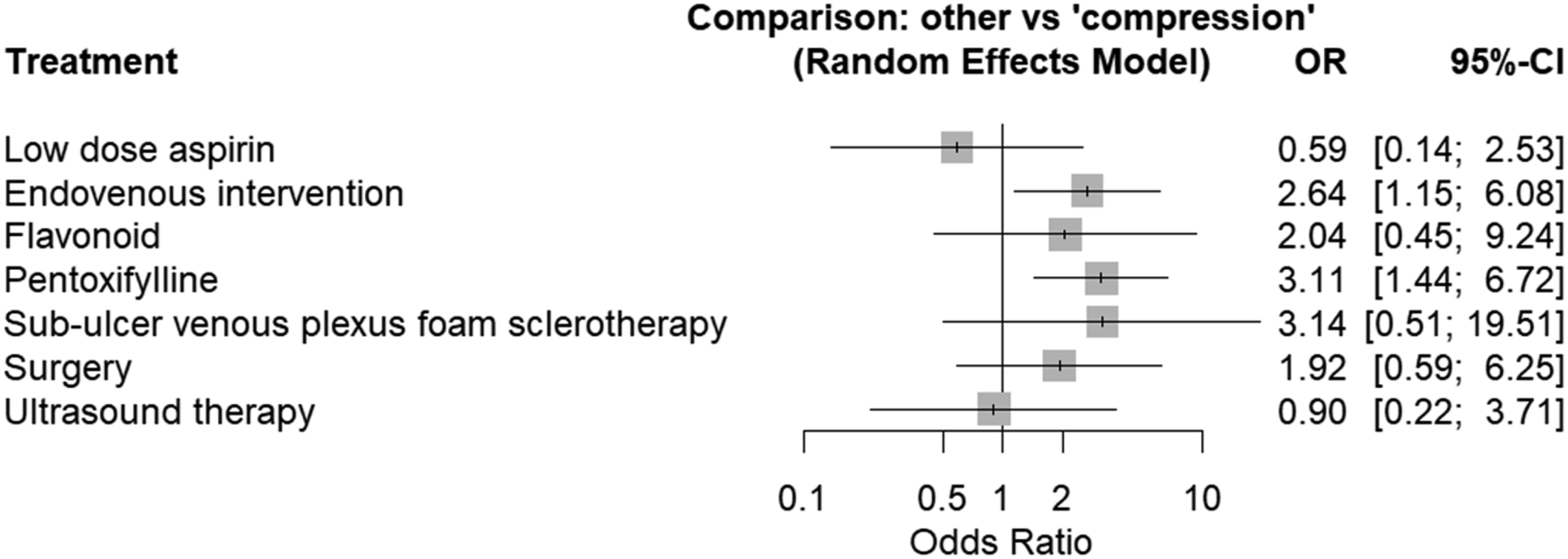
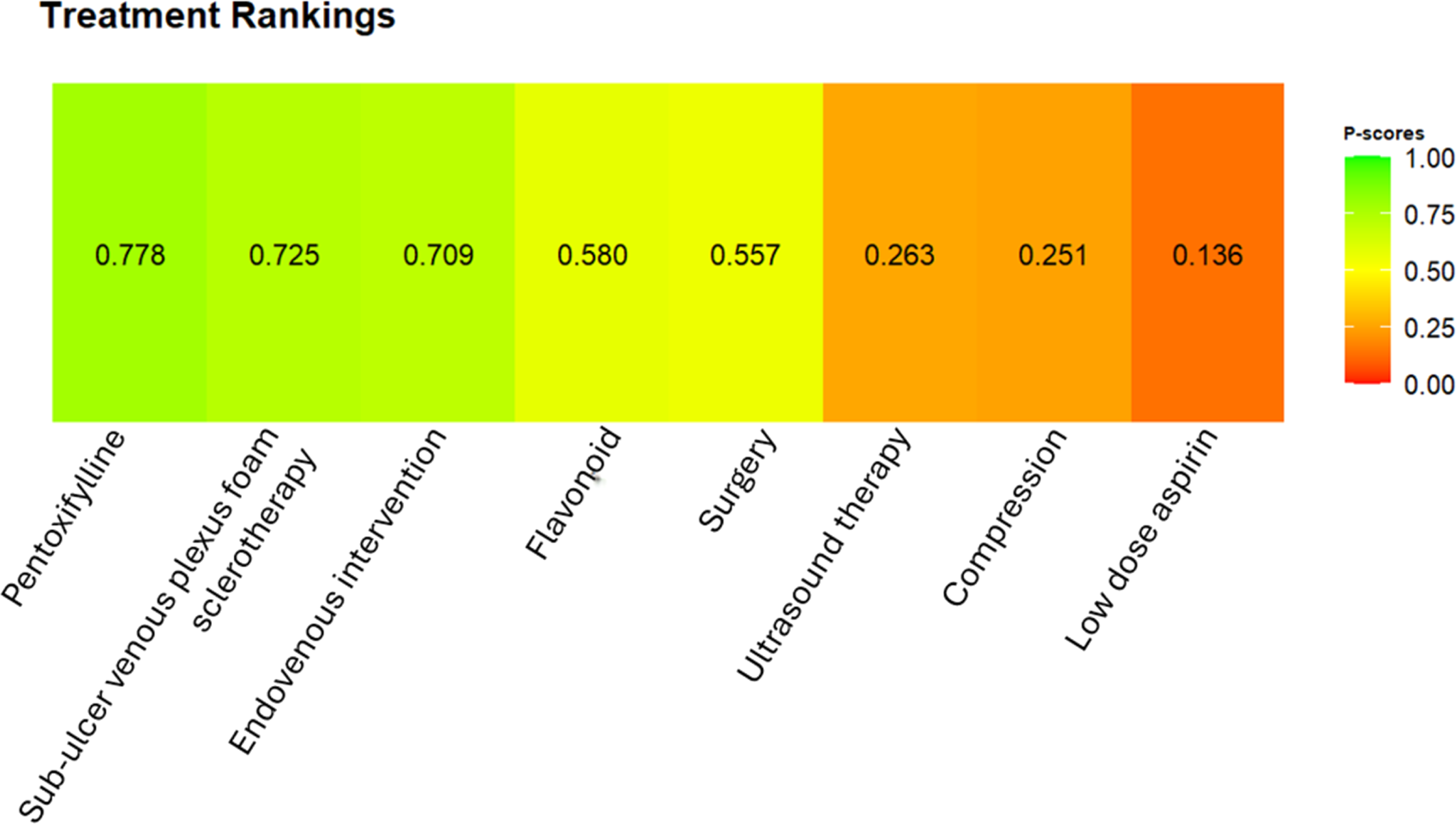
The healing network included only 15 studies which reported on complete ulcer healing at 24 weeks (Figure 3). The only statistically significant interventions that improved ulcer healing were pentoxifylline (OR 3.11, CI 1.44 – 6.72, p < .05) and endovenous interventions (OR 2.64, CI 1.15 – 6.08, p < .05) (Figure 4). No other interventions significantly improved ulcer healing rates at 24 weeks. Indirect pairwise comparisons were conducted as an exploration of which adjunctive therapies were promising (Figure 5). This suggested that pentoxifylline may be considered more effective than ablation (Figure 6), although these results are not statistically significant. Network plot for complete venous leg ulcer healing at 24 weeks. Forest plot of complete venous leg ulcer healing at 24 weeks. League table of indirect pairwise comparisons. Treatment ranking plot of each intervention.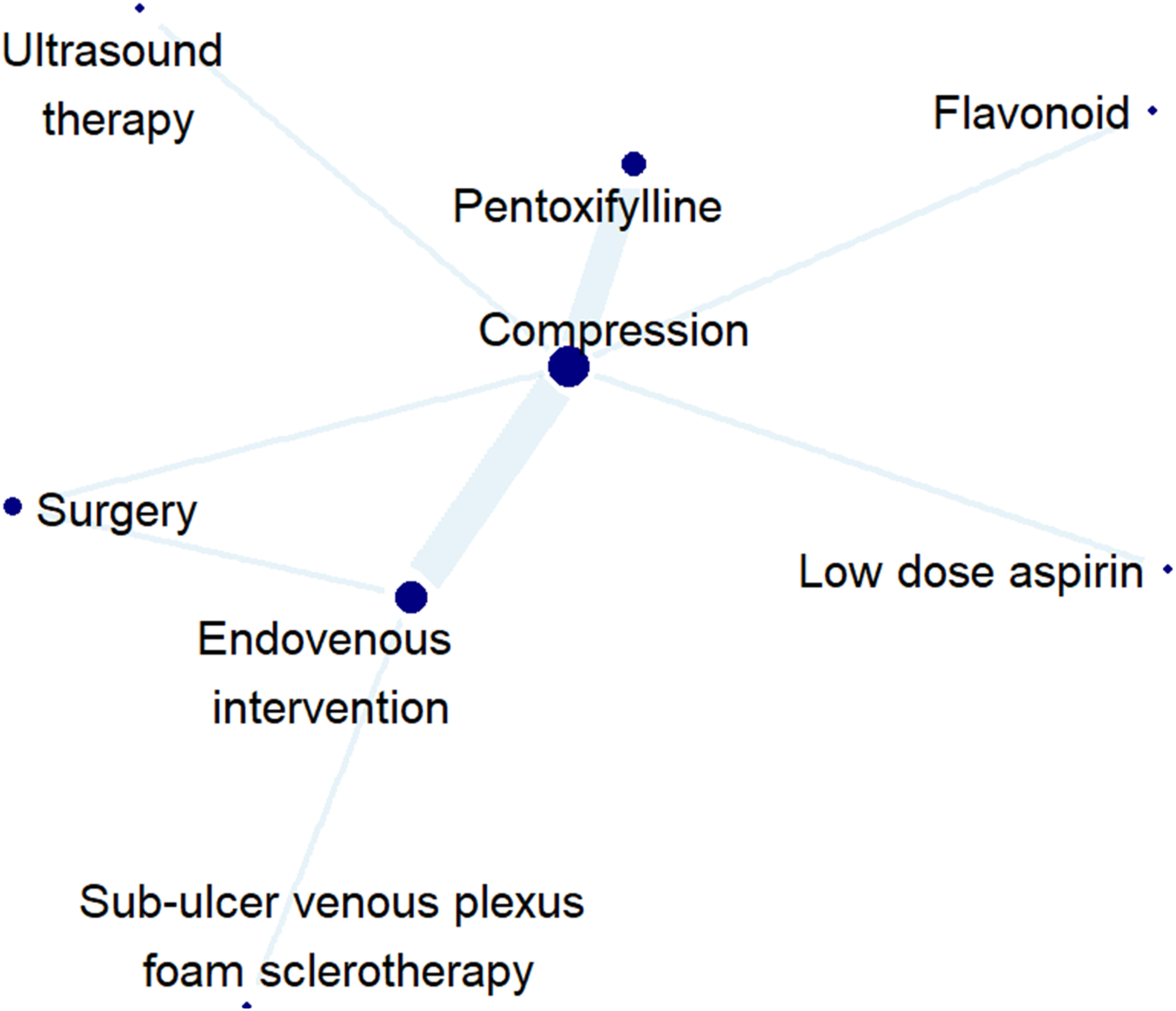

Discussion
The management of VLUs is complex and can involve multiple interventions. This is the first network meta-analysis comparing compression, pharmacological treatments, surgical and endovenous interventions in the management of VLUs. The findings are exploratory and highlight promising adjunctive therapies which should be prioritised in future trials. In particular, our findings suggest that pentoxifylline and endovenous intervention in combination with compression improve VLU healing compared to compression alone. The latter is in keeping with results from previous reviews. However, with ample evidence in the literature that show the majority of VLU care occurs in the community and in primary practice, 14 these patients often do not have access to these endovenous interventions. It is therefore imperative that the relative effectiveness of interventions that are deliverable in the community, such as pharmacotherapy, are studied in greater detail.
A recent meta-analysis found that patients who took pentoxifylline alongside compression were more likely to heal their VLUs (OR 2.56, 95% CI 1.97 - 3.32, p < .001). 3 The potential effectiveness of pentoxifylline is reflected in international guidelines. The European Society for Vascular Surgery (ESVS) and the American Venous Forum both recommended the use of pentoxifylline in the management of venous leg ulcers.7,15 Currently in the UK, NICE recommend its use as an off-license recommendation. 6 However, it is important to note that there is a large variability in the quality of the pentoxifylline RCTs – many have small sample sizes and were conducted decades ago, during which time techniques for treating venous ulcers has progressed significantly. There is a clear need for further large-scale trials that investigate the true impact of pentoxifylline on VLUs.
There has been an increase in the popularity of endovenous interventions used to treat chronic venous insufficiency over the last 25 years, 9 with strong evidence for its use in VLU management. A 2023 Cochrane review demonstrated that endovenous ablation improved time to complete ulcer healing when used in conjunction with compression. 9 Given the high-quality support for endovenous interventions, national and international guidelines recommend endovenous interventions to treat venous leg ulcers.6,7 It should however be noted that this analysis grouped all endovenous treatment as a class of interventions for the direct and indirect comparisons, grouping thermal ablation, non-thermal ablation and foam sclerotherapy. The results from this paper reflect the potential class-level benefit of endovenous interventions as a whole. It is difficult to establish whether one particular endovenous technique is superior to the other given the limited data collected from trials. This could be explored in an individual patient data meta-analysis in future network meta-analyses.
This network meta-analysis conducted indirect pairwise comparisons between all interventions. Although, a ranking was given to all interventions based on these indirect comparisons (Figure 4), this should be interpreted with caution, especially given the moderate heterogeneity and inconsistency across the studies. Overall, the evidence did not demonstrate a clear advantage of either endovenous ablation or pentoxifylline over the other. It is plausible that there may be a potential additive benefit of using pentoxifylline in combination with ablation. However, due to the lack of head-to-head comparative studies, it is difficult to draw any firm conclusions. Therefore, it is imperative that future RCTs focus on directly determining the effectiveness of pentoxifylline as an adjunct to compression and endovenous ablation.
This can be further applied to the other interventions in this study. For example, surgical interventions often play a supplementary role in the management of chronic venous disease, with compression being regarded as standard of care. 7 Previous RCTs have shown that this can increase healing and reduce ulcer recurrence rates. 8 Another consideration is that not all patients will be able to tolerate surgery, and some patients will not consent to when offered, which can limit its uptake rate.9,16 It would be interesting to investigate the relative effectiveness of open surgical intervention against endovenous interventions directly. A network meta-analysis has suggested that there is some evidence of endovenous interventions being superior to older surgical techniques such as high-tie ligation and stripping, 5 although further direct comparisons are needed.
This analysis has made apparent that there is a lack of robust large-scale RCTs investigating each intervention against one another in the management of VLUs. This study showed no statistically significant association between ulcer healing and sulodexide, aspirin or flavonoids. Previously, studies have compared pharmacotherapy adjuncts against compression monotherapy. Patients receiving sulodexide have demonstrated a moderate increase in the rate of VLU healing, although the RCTs demonstrating this were noted to be of low quality. 17 Studies have also investigated the impact of flavonoids on venous ulcer healing, with some evidence suggesting that it may improve healing rates. 18 More recently, the anti-inflammatory properties of aspirin have allowed for newer studies to assess their impact on VLU healing, although many of these are yet to show any conclusive evidence of their usefulness as a pharmacological adjunct. 19 Future work with larger randomised trials would be beneficial to investigate the effectiveness of these pharmacotherapies as adjuncts to compression in treating VLUs.
The practical implications of these findings suggest promising pharmacotherapies in the management of VLUs. More robust trials in the future could provide a stronger evidence base and therefore change current guidelines to encourage their use in conjunction with other therapies. A large advantage of pharmacotherapies is that they can be delivered in the community. This could be particularly beneficial for patients who have difficulty accessing secondary care endovenous interventions. It also would give patients more choice with respect to the treatment strategy they would prefer, allowing for more shared decision making.
Our results showed moderate heterogeneity, which suggests that our findings should be interpreted with caution. There are many reasons for this including diverse patient populations, varying sample sizes and variation in care amongst those who received treatment primarily in the community compared to specialist-managed populations. Further contributors to heterogeneity include the differences in superficial venous reflux patterns amongst patients as well as ulcer characteristics at baseline (such as ulcer duration and size). More complex patterns of reflux or longer ulcer duration may lead to poorer healing with compression monotherapy only. These factors could explain why some patients do not respond to adjunctive therapies while others do. Unfortunately, few papers consistently reported on these factors, making it difficult to analyse which variables specifically contributed most to heterogeneity. We aimed to mitigate this by using a random-effects model when conducting our analysis. This allowed for the consideration of variations both within each study and between studies to be accounted for. This increases the reliability and generalisability of the findings. In future trials, there would be an added benefit from studies explicitly reporting these variables to determine how they might affect healing outcomes.
Study limitations
There were a few limitations to our study. The main limitation is that there was sparse data for some interventions, leading to some weak links in the network. This resulted in fewer direct comparisons, leading to wider confidence intervals. There were further studies on some interventions but the lack of reporting on the primary outcome led to their exclusion. There is also moderate heterogeneity and inconsistency between the studies. This network meta-analysis focuses on complete venous ulcer healing; however, this is only one factor in the management of venous ulcers. Other relevant parameters that should be considered include time to ulcer healing, recurrence rate of ulcers as well as the impact on the quality of life of patients. These factors should also be considered and evaluated in future clinical trials.
Conclusion
To conclude, this network meta-analysis has demonstrated the potential benefits of pentoxifylline and ablation in improving venous ulcer healing. However, there were few direct comparisons between the individual interventions, limiting the reliability of the results. The results suggest that both pentoxifylline and ablation have the potential to enhance VLU healing. Future trials should investigate whether there is a possible potential additive benefit of using these two interventions together. To do this, future studies need to focus on comparing studies against one another, rather than against compression monotherapy alone, and in different combinations to truly assess which intervention is best for treating VLUs. This will allow for better informed guidelines and recommendations, allowing clinicians to deliver targeted care for patients with venous ulcers.
Supplemental material
Supplemental material - Comparing interventions used to treat venous leg ulcers – A network meta-analysis
Supplemental material for Comparing interventions used to treat venous leg ulcers – A network meta-analysis by Shruti Das, Marwah Salih, Matthew Tan, Sarah Onida, Alun Huw Davies in Phlebology.
Footnotes
Author Contributions
SO and AHD conceptualised the study. SD, MS, and MT developed the protocol, performed the literature search, screening, and data extraction. SD and MS wrote the initial draft of the paper, which was reviewed and edited by MT All authors reviewed the final draft of the paper prior to submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
HD.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.