
Abstract
Background
Venous malformations (VMs) are the most common vascular malformations, which can be classified as focal, multifocal, or diffuse types. But the risk of focal venous malformations with muscle involvement is not well defined.
Methods
This is a single-center, retrospective review of patients treated for focal VMs between February 2021 and February 2022.
Results
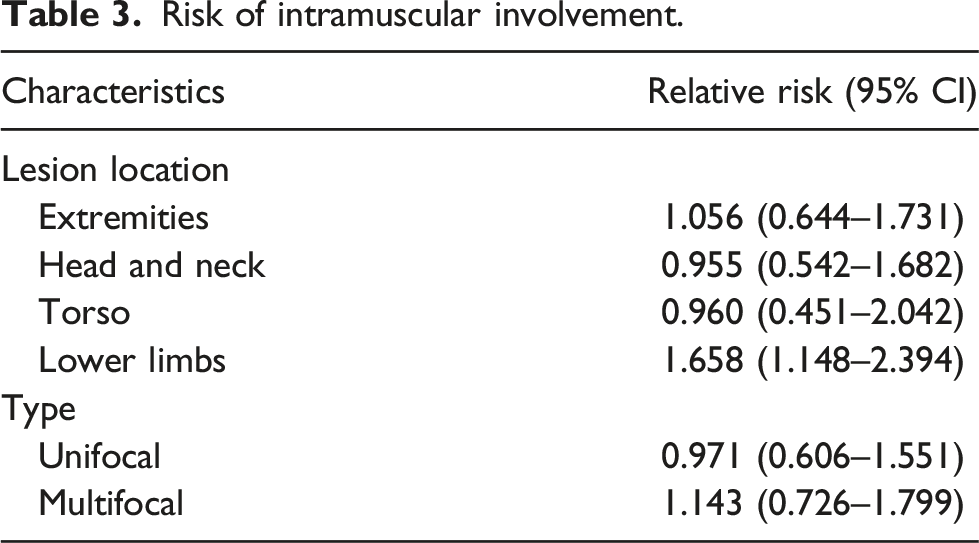
We assessed 26 patients focal VMs with 47 lesions; 18 (69%) were unifocal, 3 (12%) were dual-focal, and 5 (19%) were multifocal type VMs, and 29 (62%) were intramuscular VMs. The lower limbs intramuscular VMs had a significantly elevated risk of focal VMs (relative risk [RR],1.7; 95% confidence interval [CI], 1.148–2.394).
Conclusion
Intramuscular involvement of the body should be considered in focal VMs. The lower limbs intramuscular VMs had a significantly elevated risk of focal VMs.
Introduction
Venous malformations (VMs) are slow-flow vascular lesions and the most common vascular malformations. VMs can be classified as focal, multifocal, or diffuse types. 1 Common VMs are mostly sporadic and unifocal and account for more than 90% of VMs. 2 Focal VMs are solitary, localized, and predominantly nonfamilial. 3 VMs are usually noted at birth, but they grow proportionally with the child and exhibit progressive ectasia with age. 4
Fewer than 1% of all venous malformations are intramuscular. 5 Intramuscular VMs are generally not evident at birth but manifest themselves later in life. 6 The intramuscular VMs may be highly symptomatic and show a progressive enlargement which induces a gradual worsening of the symptoms. They typically present with swelling and pain and cause significant functional limitations. 7
The purpose of our study was to describe the clinical characteristics of focal VMs in children and the risk of muscle involvement. When the doctors discover focal VM in a specific area or in the skin/subcutaneous area, it is important to be vigilant that there may also be lesions in the muscles. Such patients may also have focal VMs when experiencing muscle pain or swelling in the future, in order to prevent missed diagnosis or misdiagnosis.
Methods
This study was reviewed and approved by the Children’s Hospital Affiliated to Shandong University institutional review board. The Shandong Provincial Clinical Research Center for Children’s Health and Disease database was queried for all patients with a diagnosis of VMs from February 2021 to February 2022. Patients were included in the study if all three of the following criteria were met: (1) a vascular anomalies specialist (general surgeon, interventional radiologist, and pediatrician)-diagnosed focal VMs, (2) diagnostic MRI (magnetic resonance imaging) (Figure 1) or ultrasonic was available, and (3) there were clinical photographs of focus. Diagnostic DSA (Digital Subtraction Angiography) was obtained in cases with equivocal imaging and for therapeutic purposes. According to the number of lesions, focal VMs can be divided into three types: unifocal, dual-focal, and multifocal. We excluded multifocal VMs associated with BRBNS (blue rubber bleb nevus syndrome) and CMVM (cutaneo-mucosal venous malformation). Diagnostic images. MRI showed that the lesions are isolated, with smooth edges and clear boundaries. The lesions to be isointense or hypointense to surrounding muscle on T1-weighted sequences (a) and hyperintense on T2-weighted images (b). The presence of punctate low signal in hyperintense lesions of fat compression T2 weighted images (c). A, B, and C are the same lesions.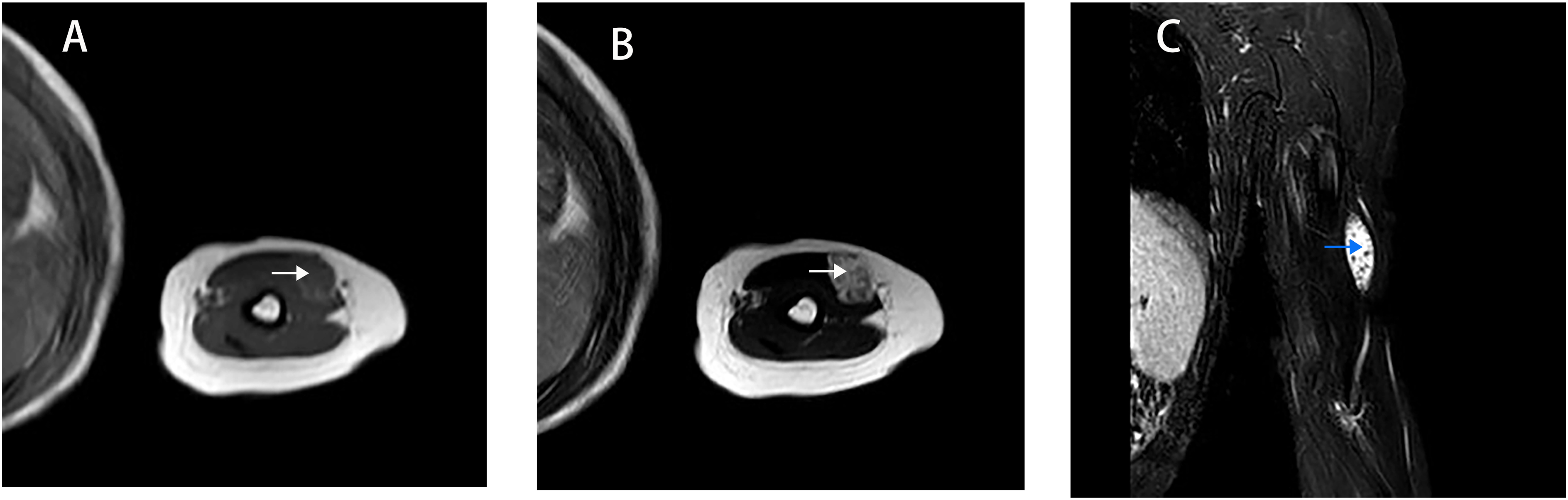
Clinical data including name, inpatient number, sex, age at presentation to our center, diagnostic imaging or ultrasonic, and combined focal VMs were collected from medical records by using standardized data abstraction forms by two reviewers (JZ and ZL).
Clinical photographs of focal VMs were reviewed by one pediatrician (JZ), one interventional radiologist (JL), and one general surgeon (LW) blinded to patient outcomes and categorized by subtype into unifocal, dual-focal, or multifocal VMs. Focal VMs were solitary and localized. Multifocal VMs were noncontiguous. Intramuscular VMs were determined by the presence of venous malformation on MRI and ultrasonic by two interventional radiologists (JL and ZL). A radiologist specialized in vascular malformations (LG) was blinded to clinical data and reviewed all focal VM MRI studies that did not include a comment on intramuscular VMs.
Statistical analysis
Descriptive characteristics were compiled according to lesion type of VMs. Interquartile ranges and medians were reported for nonparametric data. Bivariate comparisons were performed with chi-square or Fisher’s exact tests for categorical variables, and relative risks (RRs) were generated when appropriate. All tests were two-sided, with p-values less than or equal to 0.05 considered to be statistically significant. All statistical analyses were performed with IBM SPSS statistics 21.
Results
Cohort characteristics
Characteristics of 26 patients with focal VMs according to the type.
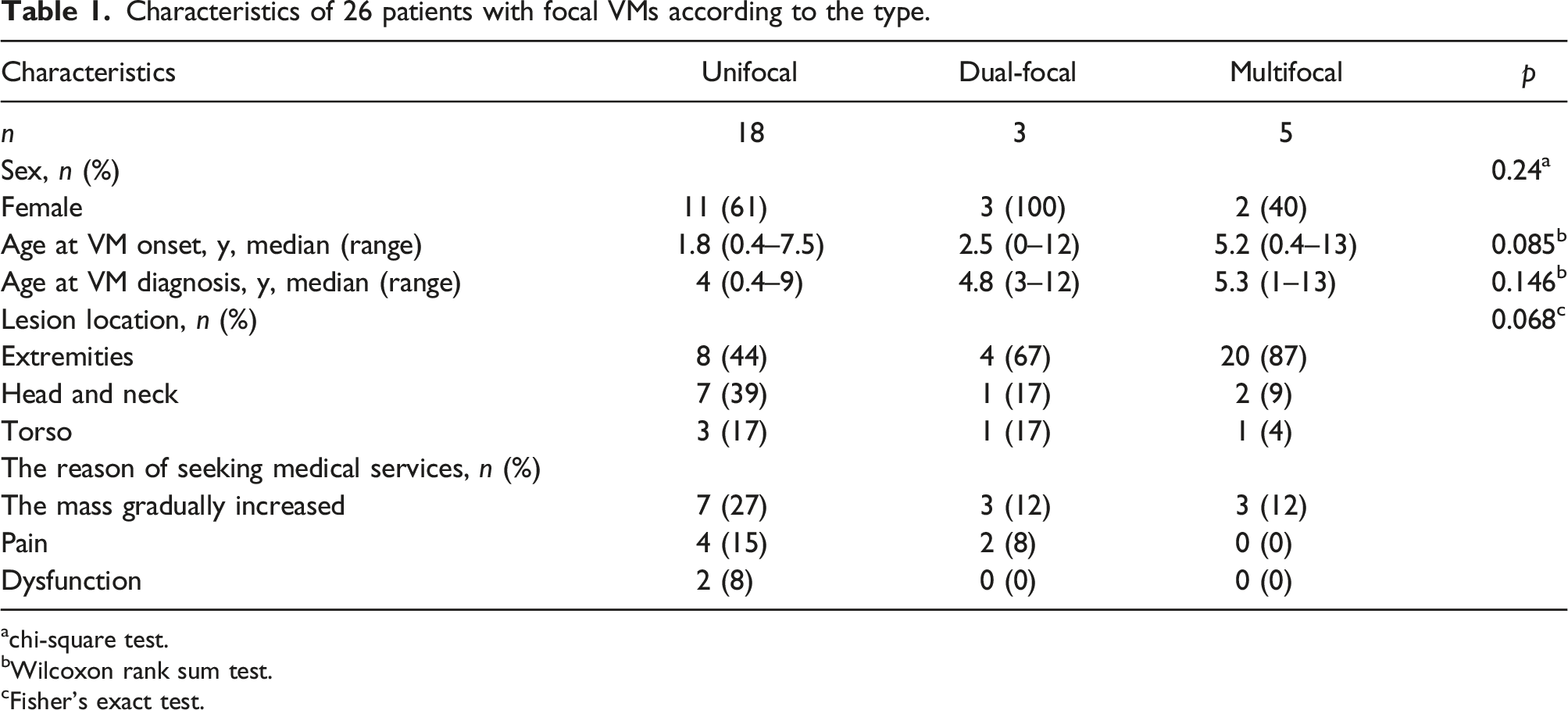
achi-square test.
bWilcoxon rank sum test.
cFisher’s exact test.
The lesions were noted before 1 year old in 36% of the patients, 60% presented at 0 to 5 years, and 40% at 6 to 13 years. The most common presenting symptoms were swelling or mass (100%), pain (n = 6, 23%), and functional limitations (n = 2, 8%), which were often because of pain or the location of the mass. Thirteen patients (50%) had a growing gradually mass at presentation, occurring especially at motion or crying.
There was no significant difference in sex, age at diagnosis, or lesion location based on VM subtype. The median age at diagnosis of VM was 4 years for unifocal and younger than 1.3 years for multifocal. Intramuscular VMs were diagnosed later than extramuscular VMs in focal VMs; the median age of intramuscular is 5.3 years and 4 years for extramuscular tissue.
Risk of intramuscular venous malformation
Characteristics of 45 lesions with focal VMs according to lesion location.
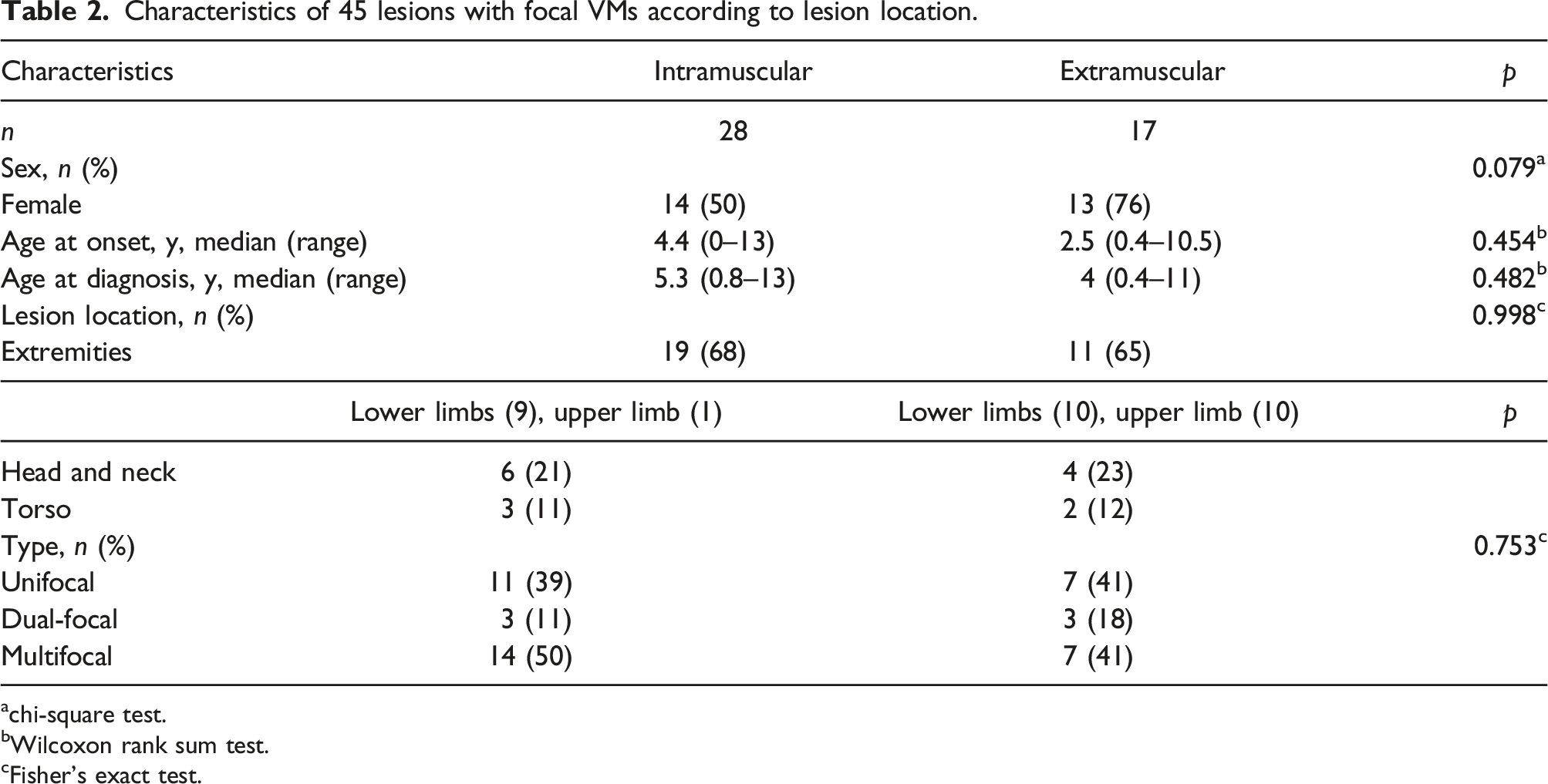
achi-square test.
bWilcoxon rank sum test.
cFisher’s exact test.
Risk of intramuscular involvement.
Discussion
Here, we found that individuals with distinctive focal VMs, who have unifocal and multifocal, do not satisfy the clinical criteria for BRBN and VMCM. Because there is less attention to focal VMs, few papers specifically analyze focal VMs, while many papers merge together focal and diffuse VMs. In this study, we exclusively considered focal VMs and intramuscular VMs.
Venous malformations occurred in every muscle group, most often in the head and neck and extremities. VMs have a higher incidence in muscle than skin, subcutaneous tissue, viscera, or intracranial vasculature. VMs tend to be in contiguous muscle groups, perhaps because they evolved during embryonic development along neurovascular pathways.8,9 The focal VMs we studied are the same as their results, but more common in the extremities, 28 (62%) lesions in muscle. The partial lesions of five multifocal VMs are in contiguous muscle groups; other remaining lesions are distant. The most common intramuscular VM locations were in the lower leg, upper leg, and upper arm. 10 But in focal VMs, the lower limbs intramuscular VMs had a significantly elevated risk. Unlike skin VMs, intramuscular VMs are generally not evident at birth but manifest themselves later in life. 6 As the dysmorphological features of VMs predispose to stagnant blood flow, these lesions can spontaneously thrombose and thus present with swelling and pain.
BRBN is a rare, sporadically occurring disorder characterized by multiple widely distributed cutaneous and internal VMs.11,13 Patients have tens to hundreds of lesions that often increase in size and number with age. Cutaneous lesions are generally small, measuring less than 1–2 cm, blue to purple in color, with a predilection for the skin, mucosae, and gastrointestinal tract. 12 As our study suggests, the multifocal of focal VMs, measuring more than 1–2 cm, involves the muscle, skin, subcutaneous, and spaces between bone and muscles tissue, without viscera or intracranial vasculature.
The condition of multiple CMVM is characterized by the presence of small, multifocal bluish cutaneous and/or mucosal venous malformations. 4 They are usually present at birth and also increase in size and number with age. The malformations range in size from 1 mm to 1 cm. Larger lesions can invade subcutaneous muscles and cause pain. Family inspection is essential in this autosomal dominant disease, with an estimated penetrance of 90% by the age of 20 years. 14 As our study suggests, the multifocal of focal VMs involves the muscle, skin, subcutaneous tissue, and spaces between the bone and muscles, without viscera or intracranial vasculature. Only 19% are multifocal type VMs and are different from VMCM and BRBN.
Given that a large number of patients at our institution, as such, the risk of muscle involvement may not be representative enough in this study. But “the incidence rate of focal veins in the muscles of the lower limbs is increasing” can alert doctors and parents that the focal VMs may affect muscle strength or lower limb movement. When doctors discover lesions in other locations, they should be alert to the possibility of lower limb lesions and actively examine and treat to avoid irreparable damage. Because of the shorter follow-up and only a single evaluation in many patients, we cannot exclude the possibility of some patients developing more lesions later. Patients who are initially successfully managed medically must be followed closely, however, because they may develop new focus or symptoms that then warrant re-evaluation and procedural intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Contributorship
LG is responsible for the project design. JZ is responsible for the article drafting and data collation. LW, JL, and ZL are responsible for the verification of clinical enrolled cases, image data collection, clinical photo case screening, etc. JS is responsible for data analysis.