
Abstract
Venous and arteriovenous malformations of the tongue can cause haemorrhage, airway obstruction, difficulties in chewing and swallowing, speech problems as well as orthodontic abnormalities. The purpose of the present study was to evaluate their exact topography, clinical features, morphologic aspects and management. A retrospective review on all patients with venous and arteriovenous malformations of the tongue who presented between 1998 and 2010 was performed. Medical records were analysed with respect to age and sex distribution, exact localization, symptoms and clinical presentation, management and treatment outcome. Forty-four patients with tongue malformations were analysed. The malformations affected all areas of the tongue as well as the base of the tongue without predilection areas. Nd:YAG laser and CO2 laser therapy provided good results primarily in localized malformations, while in advanced malformations the management was multi-modal since a complete surgical excision was often impossible. The hypothesis that vascular malformations of the tongue occur more frequently along the course of the feeding vessels cannot be confirmed. The therapeutic approach is determined by the exact topography, haemodynamic properties, morphologic aspects and related clinical symptoms as well as patient-specific features.
Introduction
Vascular malformations are anomalies of the vascular system that typically occur at birth; however, sometimes they are visible only later in life.1,2 Normally, they show a size-proportional growth without regression. Vascular malformations can be differentiated into high-flow lesions that include arterial and arteriovenous malformations and low-flow lesions which include lymphatic, venous and capillary malformations. 3 Beneath microcystic lymphatic malformations, venous and arteriovenous malformations are the most common types of lingual vascular malformations. The overall incidence of congenital vascular malformations in the general population is 1.5%. 4 Typical symptoms of venous and arteriovenous malformations of the tongue are bleeding, pain and swelling as well as impairments of speaking, swallowing or even breathing. 5
To precisely determine the location and extent of vascular malformations, imaging has to be performed in most cases. Duplex sonography can be useful to analyse the flow characteristics of the malformation. Sonography can also be easily used intraoperatively to determine the extent of the malformation or the optimal place of injection of a sclerotherapeutic agent. Magnetic resonance imaging (MRI) and computed tomography (CT) can be carried out to estimate the size of the malformations. MRI is superior in determining the extent and the lesion type in complex lesions that have mixed components based on signal characteristics, while a CT scan reveals deformities of the mandibular and maxillary bone, especially in large malformations. In selected cases, angiography should be performed to evaluate the blood supply, existing anastomoses and to plan embolization.
As spontaneous regression of vascular malformations cannot be expected, therapeutic decisions have to be made. Treatment options are surgical excision, laser therapy, embolization and sclerotherapy. Despite the diversity of treatment methods, lingual venous and arteriovenous malformations still represent functional and, in the case of large malformations, also aesthetic problems for the patients. The aim of the present study was to analyse venous and arteriovenous malformations of the tongue regarding symptoms, treatment and outcome, and especially to analyse if there are sites of predilection for venous and arteriovenous malformations of the tongue.
Methods
All patients with venous and arteriovenous malformations of the tongue who presented to the Department of Otolaryngology, Head and Neck Surgery between 1998 and 2010 were included. The diagnosis was made when imaging and clinical features were both consistent with the diagnosis. In some patients, the diagnosis was confirmed by histopathologic examination. Patients with other lingual vascular malformations were excluded. Based on these criteria, 44 patients were identified. Patients’ charts were examined retrospectively for sex, age at diagnosis and age at presentation, therapeutic modalities, residual disease after therapy and outcome. The localization of the malformations was analysed using photographs, MRI and CT scans.
Results
A total of 44 patients with venous and arteriovenous malformations of the tongue were analysed. The sex distribution was equal (23 women and 21 men). The mean age at presentation was 40.1 years. In 36 patients (81.8%), the tongue was affected by the malformation but not the base of the tongue. The tongue and the base of the tongue were affected in four patients (9.1%). The base of the tongue but not the tongue itself was affected in four patients (9.1%). Symptoms depended on the size and localization of the malformations. Typical symptoms in small malformations were recurrent bleeding episodes. In larger lesions the symptoms were haemorrhage, difficulties in chewing and swallowing, speech problems as well as orthodontic abnormalities and airway obstruction. Previous treatments at other hospitals were performed in 13 patients before presentation. The treatment methods included laser therapy in eight patients, surgical reduction in three patients and embolization in three patients. According to the size of the malformations, different groups could be analysed.
Small punctual lingual malformations were observed in 14 patients. The average age at diagnosis was 37.5 years in this patient group. The malformations were equally distributed on both sides of the tongue but most of the punctual malformations were located on the lateral border of the tongue (Figure 1). Laser therapy was performed in nine patients (64.3%) from this group. In three cases the Nd:YAG laser was used and in six cases an excision with the CO2 laser was performed (Figure 2). A conventional surgical excision of the vascular malformation (VM) was performed in one patient. The other patients from this group opted for a watch-and-wait strategy due to asymptomatic small lesions.
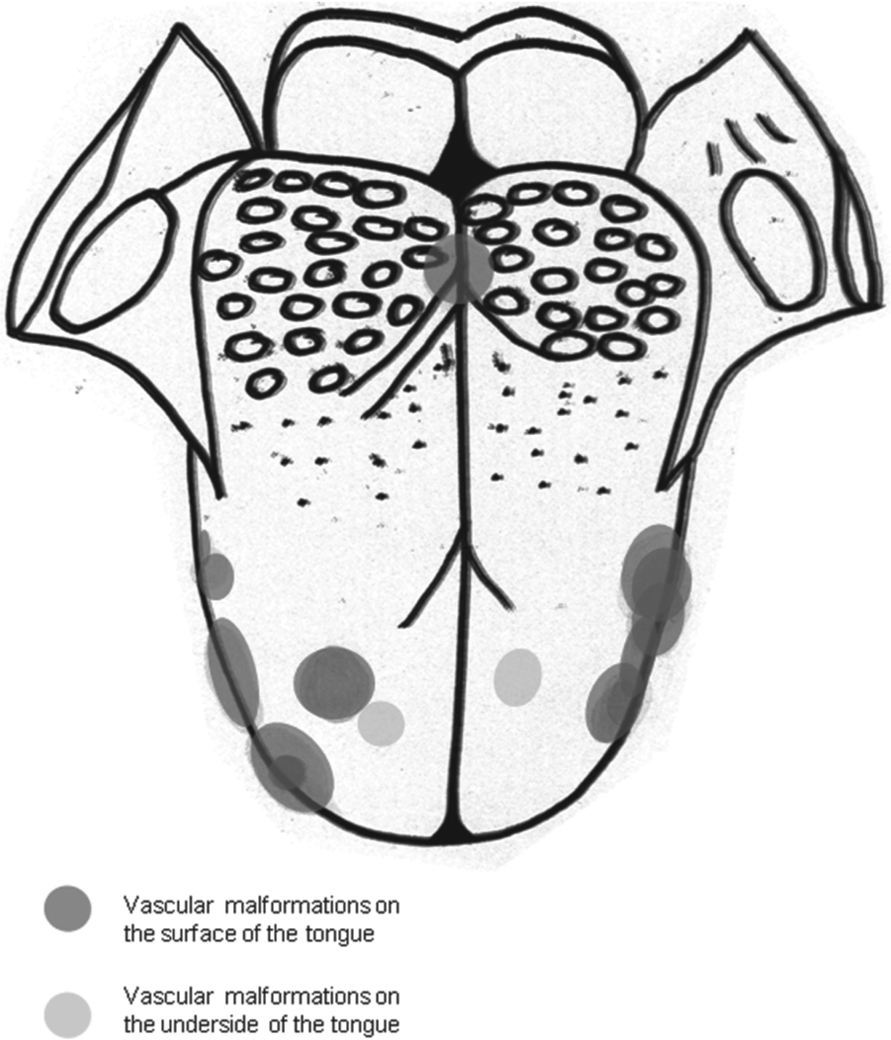
Distribution of small punctual lingual venous and arteriovenous malformations.
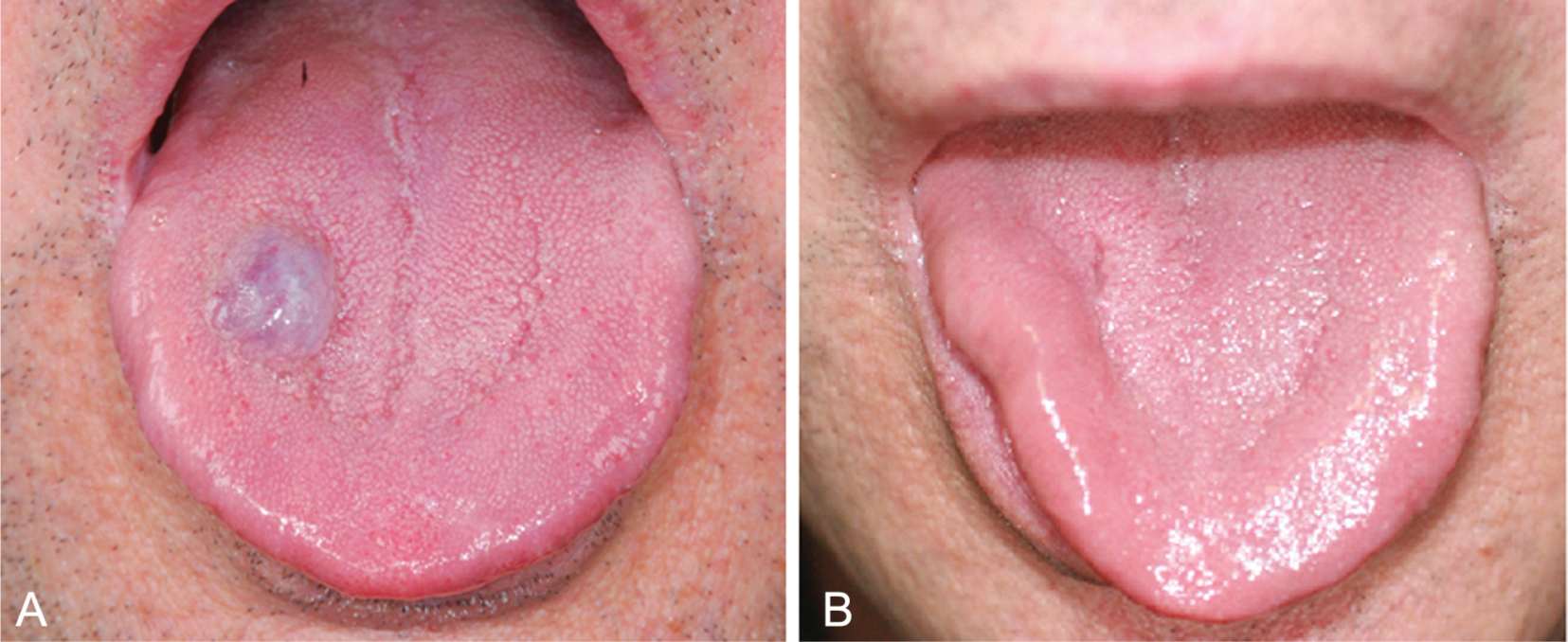
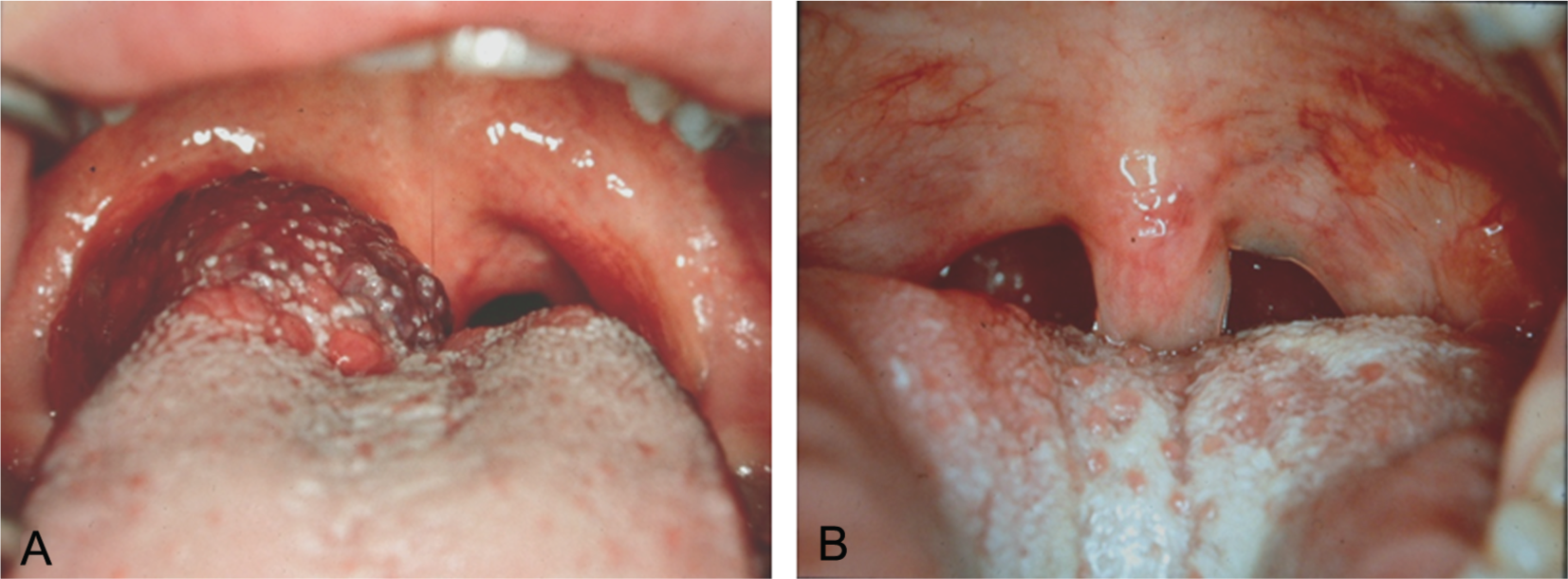
Punctual venous malformation before (A) and 6 weeks after CO2 laser surgical excision (B).
Lingual malformations that were bigger than punctual malformations but smaller than three-quarters of the tongue were observed in 21 patients. The average age at diagnosis in this group was 12.2 years. The malformations were fairly equally distributed on both sides of the tongue. Pretreatment at other hospitals was performed in eight patients. A treatment with the Nd:YAG laser was performed in 11 patients from this group (Figure 3). In seven of these, there was residual disease after therapy. One patient had residual disease after surgical partial resection. The other patients did not want any treatment due to the absence of severe symptoms and therefore were closely followed-up.
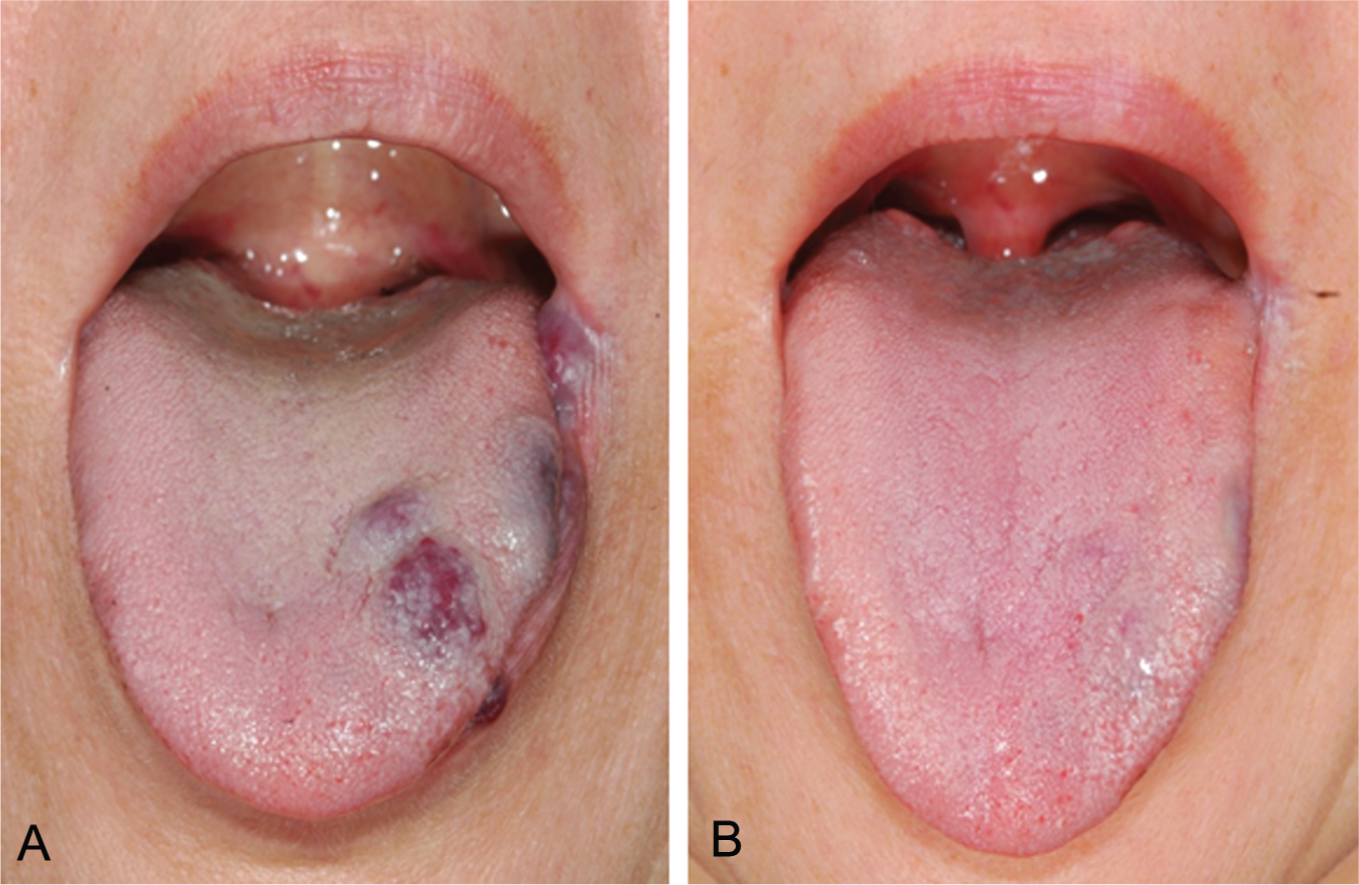
Venous malformation of the tongue in a 40-year-old female patient before (A) and 4 months after Nd:YAG laser treatment (B).
In five patients, the malformations affected more than three-quarters of the tongue. There were no predilection areas. In all these patients the lingual malformations had been diagnosed at birth. Three patients had already been treated at other hospitals. In two patients, sclerotherapy with bleomycin was performed without complications. One of these patients was treated additionally by surgery (Figure 4). Both patients had residual disease. The other patients opted for watchful waiting.
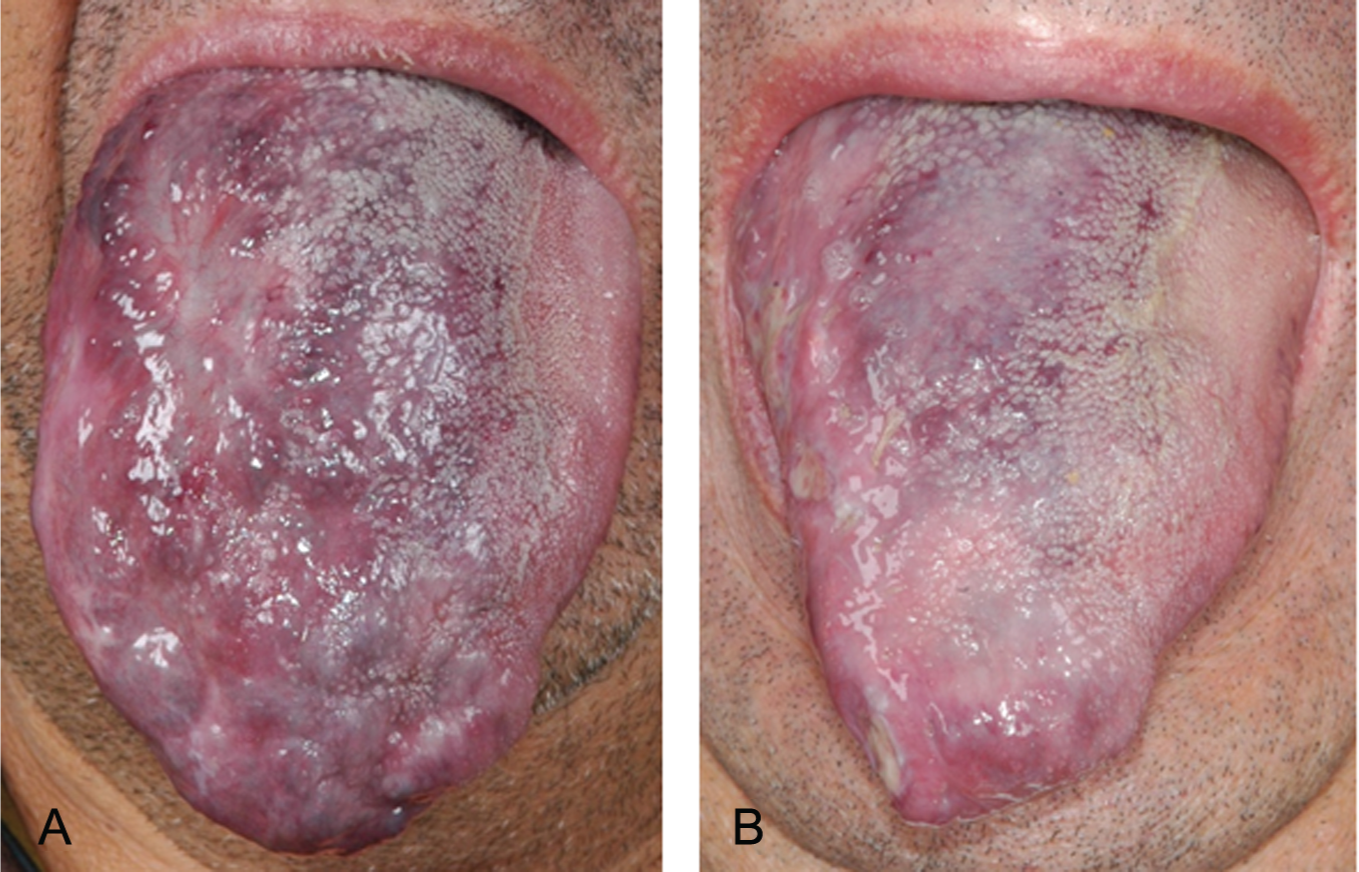
Arteriovenous malformation of the tongue in a 64-year-old man treated with Nd:YAG laser and Ethibloc and who has been tracheotomized previously (A). The same patient after surgery and sclerotherapy with bleomycin (B).
Venous and arteriovenous malformations of the base of the tongue without affecting the tongue were observed in four patients. Nd:YAG laser therapy was performed in two patients (Figure 5); in the other two patients a wait-and-see strategy was indicated.
Venous malformation of the base of the tongue before (A) and 4 months after Nd:YAG laser therapy (B).
Discussion
The tongue is a common site of venous and arteriovenous malformations of the head and neck region. One goal of this study was to assess whether there are predilection sites for the occurrence of vascular malformations of the tongue. It has to be expected that vascular malformations appear along the course of the vessels supplying the tongue (Figure 6). Since vascular malformations of the tongue occur at birth, it is speculated that their development is associated with the genesis of the tongue vessels. The embryology of the tongue vessels is still not analysed in detail and there are contradictory reports regarding the presence of transverse anastomoses between both sides of the tongue. In some studies a complex vascular system with submucosal vascular plexus and perivascular plexus as well as transverse anastomoses of the tongue vessels is reported. 6 Others have described venous interconnections in the subpapillary networks and arterial crosslinks or strong anastomoses of the deep lingual artery at the tongue tip. 7 In contrast, the presence of such anastomoses is neglected by other study groups. 7 However, in the human tongue a significant reduction of the blood supply can be achieved by unilateral ligation of the lingual artery or external carotid artery, which is an argument against strong anastomoses between both sides. However, in the present study, the vascular malformations were fairly equally distributed and no predilection sites at the tongue with accumulation of vascular malformations could be found. The small punctual venous and arteriovenous malformations analysed in this study were mostly located on the lateral border of the tongue. Moreover, in this group the average age at diagnosis of the vascular malformation was 37.5 years. This suggests that some of these lesions may be mechanically caused by a tongue bite. This would fit with the high age of the patients at diagnosis that contradicts a typical vascular malformation.
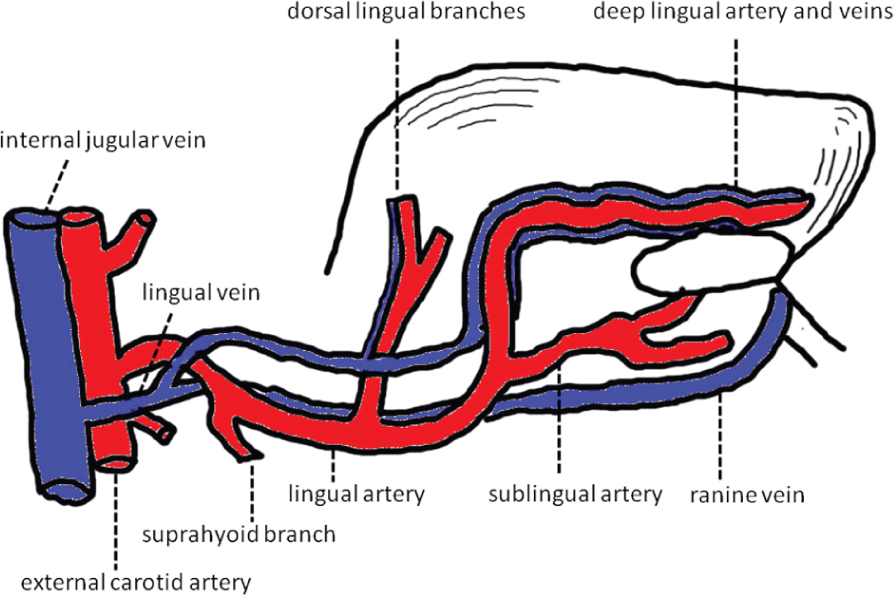
Arterial and venous supply to the tongue.
Despite various treatment options, vascular malformations of the tongue often are associated with functional and aesthetic impairments, depending on the location and extent of the malformation. The choice of the therapeutic approach is particularly dependent on the anatomic location, depth and extent of the malformation. Surgical interventions include conventional surgery, laser therapy and sclerotherapy.
Small malformations could be treated excellently. In contrast, the large lesions were more difficult to treat and residual disease was more common than in small vascular malformations. A correlation between the exact location of the malformation on the tongue and the postoperative result could not be established.
It can be stated that the CO2 laser and the Nd:YAG laser are good modalities in small vascular malformations but can also be used in larger lesions. 8 Surgery of large masses is often associated with functional limitations and impairments. Therefore, it must be weighed up in each individual case whether surgery should be performed in spite of the expected functional limitations.
Cure of arteriovenous malformations can be achieved only by a complete surgical excision with the removal of the nidus. 9 Embolization represents an alternative treatment in cases of surgical inaccessibility or when surgery would cause an unacceptable deformity. Embolization as a sole treatment for arteriovenous malformations can result in the recruitment of new vessels and collateralization, making further embolization or surgical resection impossible. Therefore, embolization provides temporary control of disease, but recurrence is high and the outcome is usually palliation rather than cure for large lesions. 10 In a combined approach, embolization can be performed 1–2 days prior to surgery to control intraoperative bleeding.
Sclerotherapy can be performed as an alternative or in addition to surgery. 11 In many patients, multiple injections have to be performed. However, a significant size reduction makes subsequent surgical excision easier. Owing to the delayed response after treatment, sclerotherapy cannot be used in patients with suspected airway obstruction or these patients have to be tracheotomized. Many different sclerosants can be used in the treatment of venous malformations and the advantages of one over the other are still not completely clear. Ethanol is the most effective sclerosing agent but sclerotherapy can be associated with adverse side effects that include nerve injury, skin necrosis, and severe systemic effects. There are less aggressive sclerosants such as polidocanol and sodium tetradecyl sulphate. Polidocanol acts as an endothelial irritant that induces thrombosis and subsequent fibrosis around the vascular spaces into which it is injected. Owing to its anaesthetic effect, the injection is almost painless. Sodium tetradecyl sulphate is a surface-active substance. It is one of the most widely used and most effective solutions for destroying unwanted veins and can be used as a sclerosant in vascular malformations. Rare complications of these sclerosants are skin necrosis, the development of deep vein thrombosis, and systemic allergic reaction. 12 Nowadays, an increasing number of lesions are treated by direct intralesional application of bleomycin. 9 In the present study, bleomycin sclerotherapy was successful and no complications occurred. Therefore, it seems to be a reliable treatment method for the treatment of vascular malformations of the tongue. However, surgeons should be aware of the possible side effects of bleomycin such as erythema, oedema, transient hair loss and the risk of pulmonary fibrosis, 13 and therefore sclerotherapy should be performed by experienced personnel.
Moreover, it has to be kept in mind that the blood supply of the tongue can cause massive blood loss during surgery, especially in children. When performing conventional surgery we recommend the use of a cell saver which can minimize or avoid the need for blood transfusion. 14 Nevertheless, blood products should be provided in these cases.
Conclusion
Venous and arteriovenous malformations of the tongue do not occur more frequently along the course of the feeding vessels. Their haemodynamic properties, extent and topography define the therapeutic approach.
Footnotes
Declaration of conflicting interest
The authors declare there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.