
Abstract
Objectives
We evaluate the rates and limitations of women’s adherence to low molecular weight heparin (LMWH) after cesarean section (CS) in the Gaza Strip.
Methods
Women who underwent CS were recruited consecutively. Communication offered to women, adherence to Venous thromboembolism (VTE), and its limiting factors were surveyed.
Results
281 women participated (mean age 27.9 years). 51.95% fully adhered to VTE prophylaxis. Causes of suboptimal adherence were: 51.1% did not feel VTE prophylaxis was important, 37.8% due to high drug cost, and 11.1% didn’t receive a prescription for LMWH at discharge. Poor communication was evident as 48.8% of the sample did not receive any instructions about the technical method of LMWH injection, 45.6% did not receive any information about the clinical significance of heparin, and 74.7% were unaware of LMWH side effects.
Conclusion
There is inadequate adherence to VTE prophylaxis after CS among Gaza women, mostly due to a lack of appropriate communication but also due to drug costs.
Keywords
Introduction
Venous thromboembolism (VTE) is a major contributor to maternal mortality which accounts for 3–14% of maternal deaths.1,2 In 2020, VTE was the third commonest cause of maternal mortality in Gaza (12.5%), and West Bank (30.8%).3,4 Pregnancy and the postpartum period are hypercoagulable states. In comparison to non-pregnant women, the risk of VTE is five times greater during pregnancy and 60 times during the postpartum period. 5 Risk factors include cesarean delivery, maternal age above 35, higher (three or more) parity, smoking, preeclampsia, antepartum immobilization, postpartum hemorrhage, infection, blood transfusion, and thrombophilia, among others. 2 Further, the risk of VTE was found to be greater after cesarean section (CS) than after vaginal delivery and was greater after emergency CS than elective CS. 6 Between 20 and 25% of deliveries in the Gaza Strip are Cesarean. 7
Several risk scores were developed to facilitate the estimation of VTE risk during pregnancy and the postpartum period, thus permitting the adoption of an individualized, risk-adapted thromboprophylaxis strategy to mitigate this potentially preventable complication. 8 In terms of CS, international guidelines, such as the guidelines of the Royal College of Obstetricians and Gynecologists (RCOG) and the American College of Chest Physicians (ACCP), advise a short (10 days) postnatal VTE prophylaxis with low molecular weight heparin (LMWH) after emergency CS or following elective CS in women who have additional risk factors. 8 The national guideline in Palestine adopted the recommendations of the RCOG in this regard.
Although the effectiveness of DVT prophylaxis in preventing venous thromboembolism is universally acknowledged, variations in the appropriateness of prescription by physicians and in the adequacy of teaching and communication offered to patients may limit the effectiveness of this intervention. Also, cultural and financial factors may limit women’s adherence to thromboprophylaxis and influence their perceptions of it. Owing to these different factors, studies from different regions have revealed varying degrees of adherence to VTE prophylaxis. For instance, in a study from the UK in 2015, 83% of 111 participating women reported complete adherence to VTE prophylaxis. 9 Meanwhile, a study from Saudi Arabia in 2022 reported a 78.8% rate of adherence to VTE prophylaxis after CS, while the percentage dropped to 67.2% in a third study.10,11
Identifying the gaps in prescription, education, and barriers to patient compliance is essential to avoid potentially preventable VTE events and to formulate interventions and strategies that are appropriate to the local context. This study is the first to assess the prescription patterns and barriers to women’s adherence to VTE prophylaxis after CS in the Gaza Strip.
Methods
Study design, setting, and ethical considerations
This is a descriptive, cross-sectional study conducted at the Obstetrics and Gynecology Hospital, which is government-run and represents the largest provider of secondary and tertiary health services in the Gaza Strip. The study was approved by the ethics committee at the Ministry of Health, and administrative approval was obtained from the Human Resources Development Department at the Ministry. Written informed consent was obtained from participants, and confidentiality was maintained throughout the data collection and data analysis stages.
Study population and case identification
This study extended from January 1st to February 28th, 2023. It consecutively recruited women who reported no previous therapeutic anticoagulant use and underwent elective or emergency CS during the study period. Exclusion criteria included having a prior therapeutic anticoagulant use, having a contraindication to LMWH, or refusing to participate.
Key measures and data collection
For this study, a data collection sheet was developed in accordance with previous literature and in cooperation with experts in the field who confirmed its validity. The data collection sheet comprised three subsections: 1 socio-demographic data, 2 obstetric data, and 3 an assessment of the use of anticoagulants (prescription, communication, and women’s adherence). Demographic data included age, education, employment, economic status, smoking, body mass index (BMI), and comorbid conditions. Obstetric data included parity, history of abortion, previous CS, indication and type of present CS (elective vs emergent), obstetric complications, and current medications. In the third section, the research team checked the correct VTE score based on the national protocol, the calculated VTE scores from medical files, the dose and duration of VTE prophylaxis, patient-perceived appropriateness of communication and teaching, adherence to VTE prophylaxis, factors limiting the adherence, patient-reported complications from LMWH, attitudes towards future LMWH prescription, and others. Inadequate adherence was defined as missing two or more injections. Demographic and clinical data were collected during admission via face-to-face interviews and from medical files. Follow-up phone interviews 10 days after the first interview evaluate each participant’s adherence and drug-related complications.
Statistical analysis
Continuous variables were presented as mean and standard deviation. Categorical variables were presented as frequency and percentages. Logistic regression analysis was performed to investigate the factors predicting suboptimal adherence to VTE prophylaxis. Dependent variables included in the model were younger age, type of CS, poor technical explanation regarding LMWH injection, poor counseling regarding the indication of LMWH, poor explanation of LMWH adverse events, poor income, employment, parity, using LMWH for the first time, education, and the number of comorbid conditions. Statistical significance was set at p-values under .05. Data were analyzed using the statistical package for social sciences (SPSS) version 25 (SPSS Inc., Chicago, IL, USA).
Results
Cohort socio-demographic characteristics
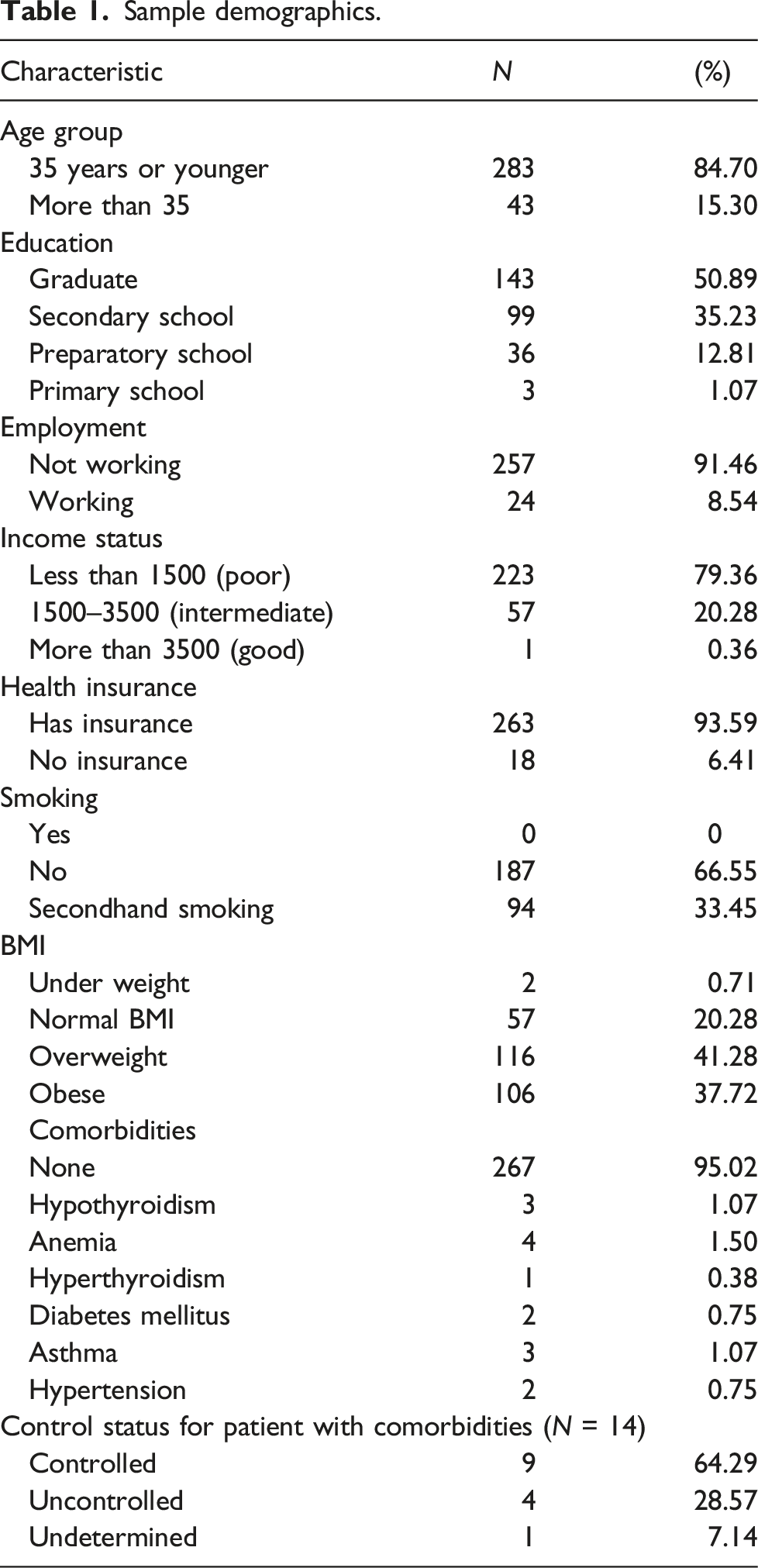
Sample demographics.
Obstetric history assessment
Obstetric history of participants.
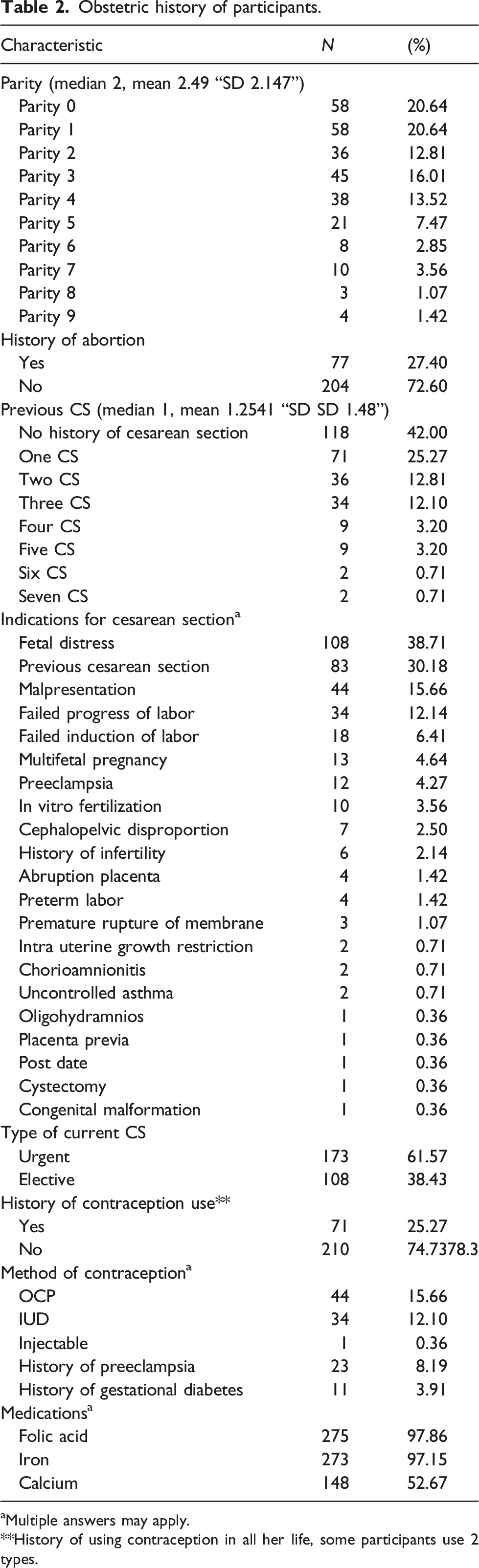
aMultiple answers may apply.
**History of using contraception in all her life, some participants use 2 types.
Anticoagulant use
Anticoagulant use.
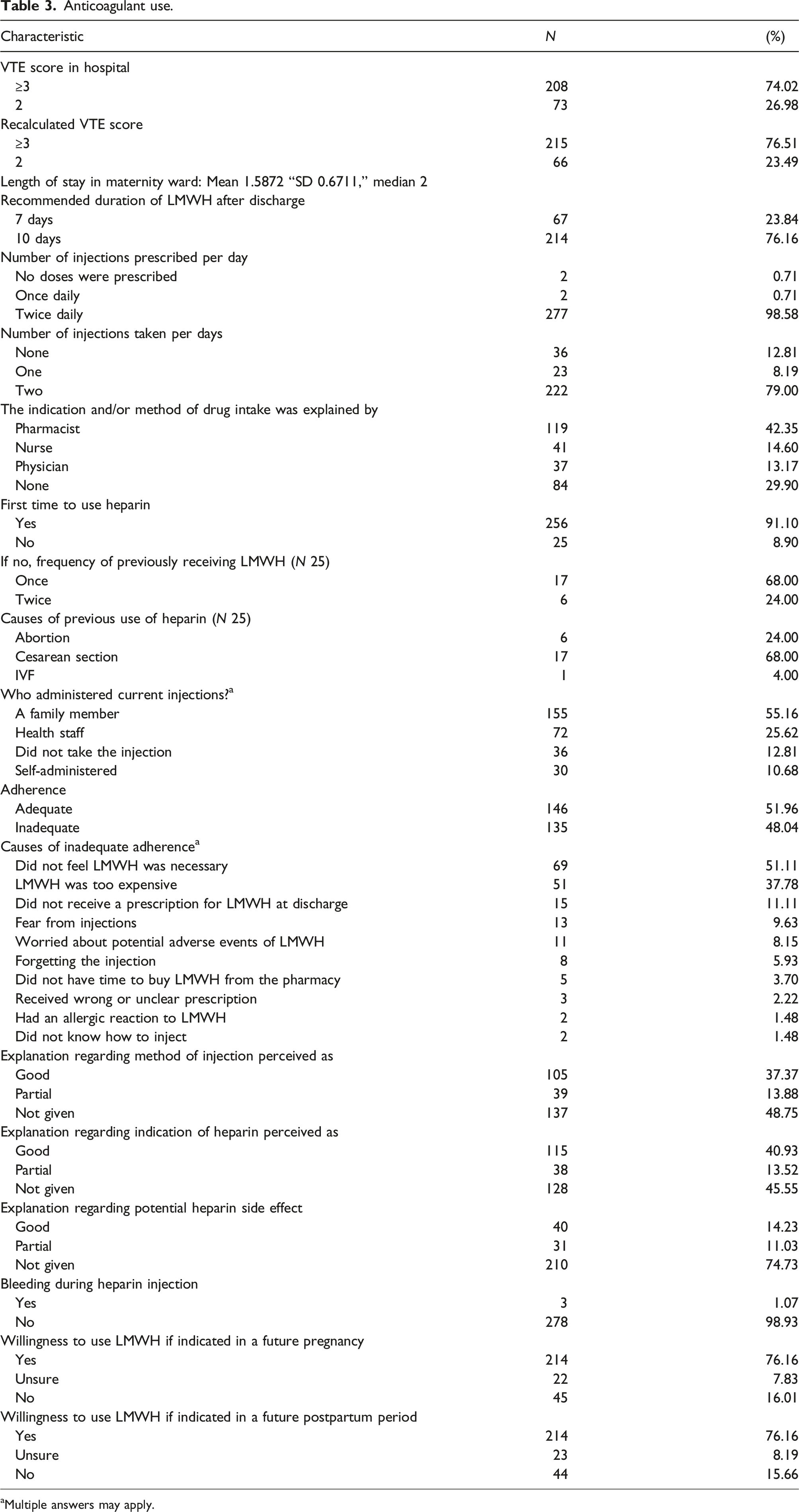
aMultiple answers may apply.
From the 277 (98.58%) participants who received a prescription to use heparin twice per day, only 222 (79%) used the same as prescribed; the remaining either did not use it at all or used it once a day. This could be related to poor education and counseling since 29.90% of patients did not receive counseling on the indications and method of LMWH administration, while those who did receive such counseling were mostly educated by the pharmacist (42.35%) or a nurse (14.60%) (Table 3). This is especially important since 91.1% had never received prophylactic LMWH before.
Regarding the current heparin injection, it was administered by a family member in 55.16% of the cases and by health staff in 25.62%. Adequate adherence was found in 51.96% of participants. The reasons behind inadequate adherence to VTE prophylaxis were diverse. A lack of perceived necessity of the medication was the commonest reported reason (51.11%), followed by the medication’s high cost (37.78%) and not receiving an appropriate prescription at discharge (11.11%). The majority of the participants demonstrated a positive attitude towards a possible future use of LMWH if indicated (Table 3).
Predictors of inadequate adherence
Predictors of inadequate adherence.
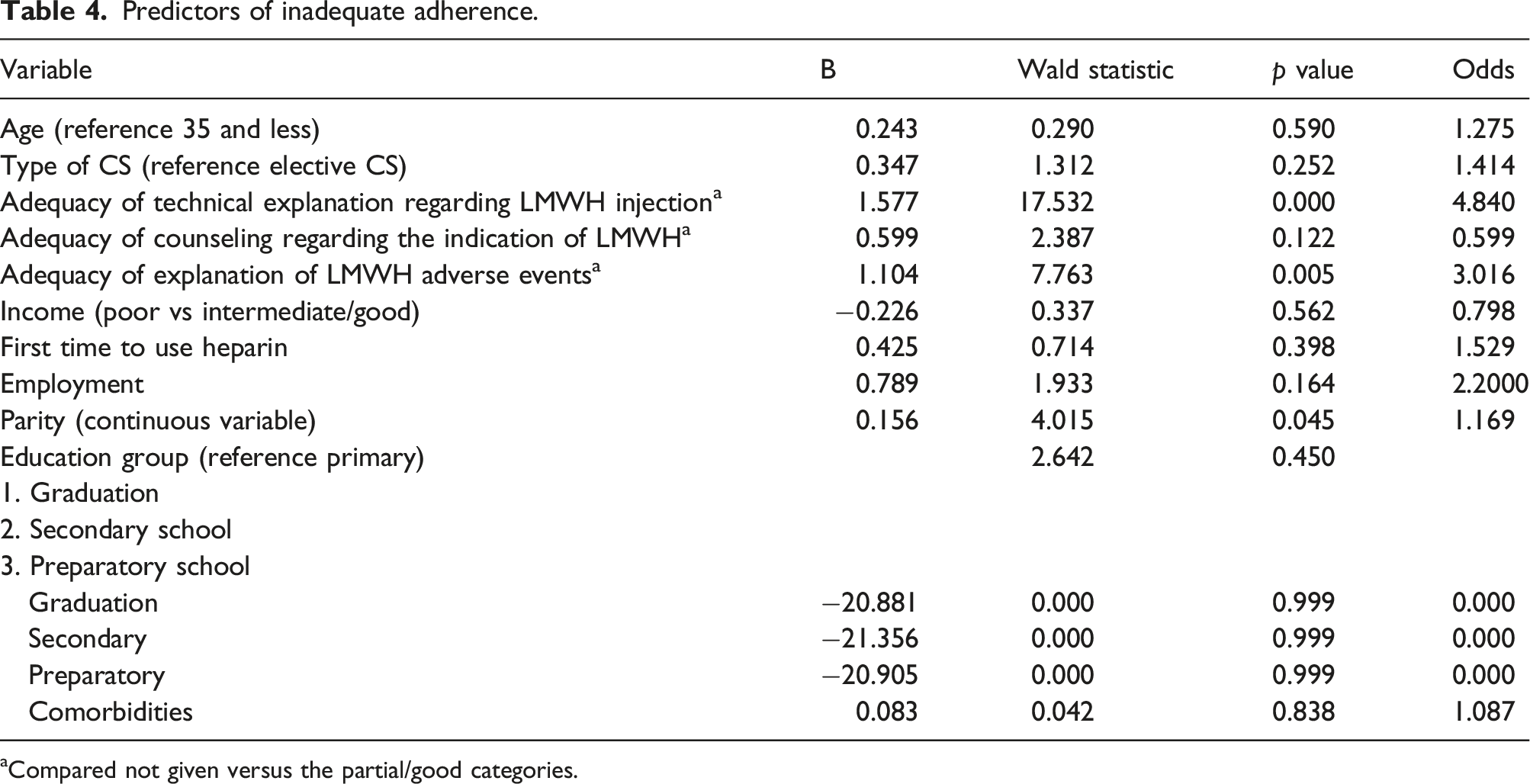
aCompared not given versus the partial/good categories.
Discussion
In this study, we evaluated the prescription patterns of VTE prophylaxis, and the adequacy of counseling and communication offered to women after CS at the largest hospital in the Gaza Strip. We also assessed the rates and factors limiting the adherence of women to VTE prophylaxis in a bid to pinpoint the gaps and limitations hindering optimal prevention of this important complication. The rate of adequate adherence found in our cohort was low (51.96%) compared to some other similar studies. For instance, Rottenstreich and colleagues reported a higher rate of adherence (67.2%), while Elmaghraby and colleagues found that optimal adherence was seen in (78.8%), and Hordern and colleagues reported an even higher percentage (83.3%).9–11 However, abstract numbers should be interpreted with caution since those studies had different populations and varying definitions of adequate adherence. In this regard, the Saudi study by Elmaghraby and colleagues examined a similar cohort of post-CS women and strictly defined inadequate adherence as missing one or more doses of LMWH, permitting further comparisons to be drawn. 10
Concerning the causes of inadequate adherence to VTE prophylaxis, the most reported reason in our cohort was the lack of perceived necessity to use LMWH (51.11%). The percentage is similar to the study by Rottenstreich, where 50.5% cited the same reason. A lack of perceived necessity may be directly linked to inappropriate communication and counseling in relation to the method and the indication of administration of the injections (not given to 45.55% and 48.75% of our participants, respectively). In contrast, 75% and 83.8% of participants in the Saudi and English cohorts felt that they received enough information about the VTE prophylaxis.9,10 Further, there are differences in who gives the education and counseling to patients. Nearly 70% of participants in the Saudi study were educated by their physicians, while in our cohort this percentage dropped to 13.17%.
On the other hand, 37.78% could not purchase the medication from the pharmacy due to high costs. This limiting factor was not reported by the participants of the previously discussed studies, who hail from high-income countries, countries with universal health insurance, or both. For instance, Rottenstreich et al and Hordern et al did not mention drug cost or availability as a possible limitation for their patients. Meanwhile, Elmaghraby et al explicitly stated that drug cost (nearly 10 US dollars per injection) was not a limiting factor for their patients’ adherence since all patients are covered by Saudi public insurance. The Gaza health system has, on the other hand, been under blockade for decades and degraded by repeated wars and chronic shortages in medications, infrastructure, and finances. 12 Thus, patients bear a big share of the costs of their treatment, and many are forced to choose between buying food or medication such as LMWH. In this regard, early mobilization is cheap and has generally been demonstrated to promote recovery and reduce the incidence of VTE in the post-surgical and post-delivery settings.13–15 Also, unfractionated heparin (UH) might be a cheaper alternative to LMWH in some areas. 16
Conversely, other causes for nonadherence can be more easily and promptly addressed than cost limitations. For example, 11.11% and 2.22%, respectively, did not receive a prescription on discharge or received a wrong prescription. Such shortcomings should be avoidable with better documentation and protocol adaptation by the staff. Nonetheless, we found a low incidence of erroneous VTE score calculations, and the vast majority of our patients were appropriately prescribed VTE prophylaxis with the correct dose and duration. In comparison, the pre-intervention arm of a study from Iraq found that only 56.9% and 18.6% of post-CS women, respectively, were prescribed incorrect doses and durations of treatment. 17
Regarding heparin administration, only 10.68% of our participants reported self-injection, which is very low compared to other studies. Rottenstreich, Hordern, and Elmaghraby reported self-injection rates of 82.9%, 54%, and 30%, respectively.9–11 Rottenstreich and colleagues also found a positive correlation between the perception of adequate communication regarding the technical injection of LMWH and the rates of adequate adherence. 11 The low rates of self-injection in our cohort are likely related to the poor education and communication offered to patients. It is safe to assume that appropriate counseling and education foster healthy perceptions about the medication and the confidence to self-inject, while reliance on a family member or healthcare staff incurs unnecessary physical and social burdens on parturient mothers.
In our study, 1.07% of the respondents complained of bleeding events during heparin administration. Similarly, Rottenstreich and colleagues reported bleeding in 3.4% of their cohort. 11 Meanwhile, Elmaghraby and colleagues reported that 10% had side effects of LMWH, but the definition of the side effects was not explained. 10 Therefore, our findings are not dissimilar to other cohorts. However, 74.73% of our participants did not receive an explanation regarding heparin side effects, which reveals another gap in communicating with the patients. Still, despite the poor education, most participants (76.16%) demonstrated a willingness to use LMWH if indicated in a future pregnancy or future postpartum period, which reflects a healthy attitude among Palestinian women. Rottenstreich and Hordern reported a willingness to use LMWH in a future pregnancy in 74.8% and 94% of their cohorts, respectively.
Pregnant women need appropriate communication, education, and sufficient clinician support in order to make shared, informed decisions regarding VTE prophylaxis and their health in general. 18 In our study, adequate technical explanation of the LMWH side effects and injection method were significant predictors of adequate adherence to the treatment, while higher parity was inversely related to adherence. A positive correlation between technical explanation and adherence was also noted by Rottenstreich et al. 11 On the other hand, having previous uncomplicated deliveries might predispose women to undervalue or even disregard VTE prophylaxis as unnecessary, leading to lower adherence rates.
Conclusion
This study reveals that VTE prophylaxis prescription in Gaza is mostly adequate in terms of risk assessment, dose, and duration. However, very high rates of poor communication limit the benefits of prophylaxis and predispose to the high rates of poor adherence demonstrated by our cohort. Thus, physicians should be educated and encouraged to provide proper education to their patients. Additionally, poor economic conditions significantly complicate the efforts to prevent VTE among post-CS women in Gaza, which invites securing funds to provide LMWH injections to parturient women free of charge.
This study has several limitations. Despite a good cohort size, it is based on a single center and remains susceptible to recall and interviewer bias. Selection bias was minimized by the large sample, the recruitment of all patients who were admitted during the study period, and the high response rate, but it also remains possible.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Guarantor
BA.
Contributorship
All authors contributed to the literature review and study design. BA and SA performed the statistical analysis. OA, IH, EJ, SA, and SI contributed to data collection and entry. All authors contributed to writing the manuscript. All authors read and approved the final manuscript. Each author has participated sufficiently in the work to take public responsibility for the content.